Article Text

Statistics from Altmetric.com
Coronary artery disease pathogenesis and treatment urgently requires a paradigm shift. Despite popular belief among doctors and the public, the conceptual model of dietary saturated fat clogging a pipe is just plain wrong. A landmark systematic review and meta-analysis of observational studies showed no association between saturated fat consumption and (1) all-cause mortality, (2) coronary heart disease (CHD), (3) CHD mortality, (4) ischaemic stroke or (5) type 2 diabetes in healthy adults.1 Similarly in the secondary prevention of CHD there is no benefit from reduced fat, including saturated fat, on myocardial infarction, cardiovascular or all-cause mortality.2 It is instructive to note that in an angiographic study of postmenopausal women with CHD, greater intake of saturated fat was associated with less progression of atherosclerosis whereas carbohydrate and polyunsaturated fat intake were associated with greater progression.3
Preventing the development of atherosclerosis is important but it is atherothrombosis that is the real killer
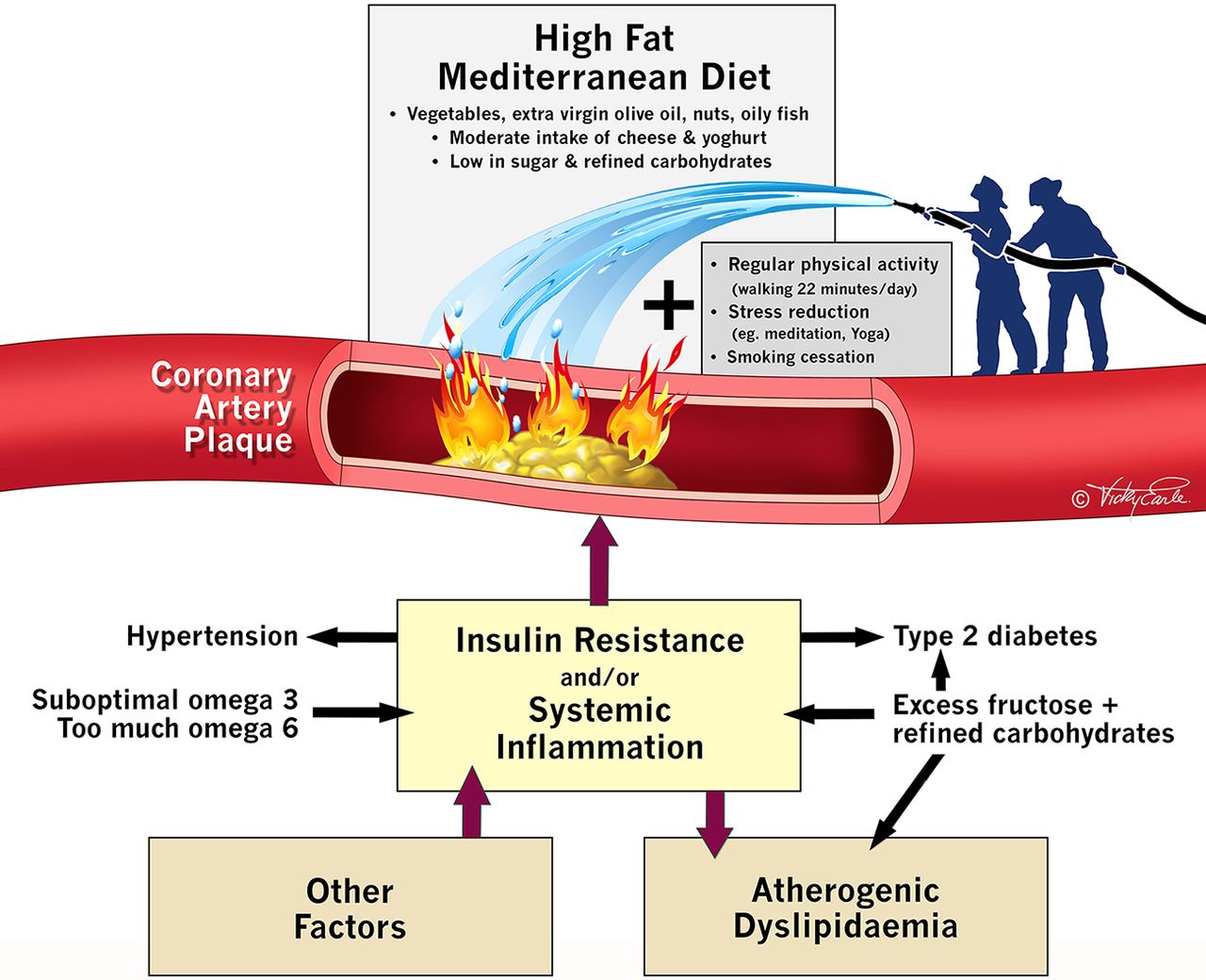
The inflammatory processes that contribute to cholesterol deposition within the artery wall and subsequent plaque formation (atherosclerosis), more closely resembles a ‘pimple’ (figure 1). Most cardiac events occur at sites with <70% coronary artery obstruction and these do not generate ischaemia on stress testing.4 When plaques rupture (analogous to a pimple bursting), coronary thrombosis and myocardial infarction can occur within minutes. The limitation of the current plumbing approach (‘unclogging a pipe’) to the management of coronary disease is revealed by a series of randomised controlled trials (RCTs) which prove that stenting significantly obstructive stable lesions fail to prevent myocardial infarction or to reduce mortality.5
{kind=link}
Lifestyle interventions for the prevention and treatment of coronary disease.
Dietary RCTs with outcome benefit in primary and secondary prevention
In comparison with advice to follow a ‘low fat’ diet (37% fat), an energy-unrestricted Mediterranean diet (41% fat) supplemented with at least four tablespoons of extra virgin olive oil or a handful of nuts (PREDIMED) achieved a significant 30% (number needed to treat (NNT)=61) reduction in cardiovascular events in over 7500 high-risk patients. Furthermore, the Lyon Heart study showed that adopting a Mediterranean diet in secondary prevention improved hard outcomes for both recurrent myocardial infarction (NNT=18) and all-cause mortality (NNT=30), despite there being no significant difference in plasma low-density lipoprotein (LDL) cholesterol between the two groups. It is the alpha linoleic acid, polyphenols and omega-3 fatty acids present in nuts, extra virgin olive oil, vegetables and oily fish that rapidly attenuate inflammation and coronary thrombosis.6 Both control diets in these studies were relatively healthy, which make it highly likely that even larger benefits would be observed if the Mediterranean diets discussed above were compared with a typical western diet.
LDL cholesterol risk has been exaggerated
Decades of emphasis on the primacy of lowering plasma cholesterol, as if this was an end in itself and driving a market of ‘proven to lower cholesterol’ and ‘low-fat’ foods and medications, has been misguided. Selective reporting may partly explain this misconception. Reanalysis of unpublished data from the Sydney Diet Heart Study and the Minnesota coronary experiment reveal replacing saturated fat with linoleic acid containing vegetable oils increased mortality risk despite significant reductions in LDL and total cholesterol (TC).7
A high TC to high-density lipoprotein (HDL) ratio is the best predictor of cardiovascular risk (hence this calculation, not LDL, is used in recognised cardiovascular risk calculators such as that from Framingham). A high TC to HDL ratio is also a surrogate marker for insulin resistance (ie, chronically elevated serum insulin at the root of heart disease, type 2 diabetes and obesity). And in those over 60 years, a recent systematic review concluded that LDL cholesterol is not associated with cardiovascular disease and is inversely associated with all-cause mortality.8 A high TC to HDL ratio drops rapidly with dietary changes such as replacing refined carbohydrates with healthy high fat foods.
A simple way to combat insulin resistance (chronically high levels of serum insulin) and inflammation
Compared with physically inactive individuals, those who walk briskly at or above 150 min/week can increase life expectancy by 3.4–4.5 years independent of body weight.9 Regular brisk walking may also be more effective than running in preventing coronary disease. And just 30 min of moderate activity a day more than three times/week significantly improves insulin sensitivity and helps reverse insulin resistance (ie, lowers the chronically elevated levels of insulin that are associated with obesity) within months in sedentary middle-aged adults. This occurs independent of weight loss and suggests even a little activity goes a long way.
Another risk factor for CHD is environmental stress. Childhood trauma can lead to an average decrease in life expectancy of 20 years. Chronic stress increases glucocorticoid receptor resistance, which results in failure to down regulate the inflammatory response. Combining a complete lifestyle approach of a healthful diet, regular movement and stress reduction will improve quality of life, reduce cardiovascular and all-cause mortality.10 It is time to shift the public health message in the prevention and treatment of coronary artery disease away from measuring serum lipids and reducing dietary saturated fat. Coronary artery disease is a chronic inflammatory disease and it can be reduced effectively by walking 22 min a day and eating real food. There is no business model or market to help spread this simple yet powerful intervention.
Footnotes
Contributors AM wrote the initial draft with further revisions and edits from RFR and PM.
Competing interests RFR served as a consultant for one day in May 2015 for Amgen. AM is a co-producer of the documentary The Big Fat Fix.
Provenance and peer review Not commissioned; externally peer reviewed.