Article Text

Statistics from Altmetric.com
Introduction
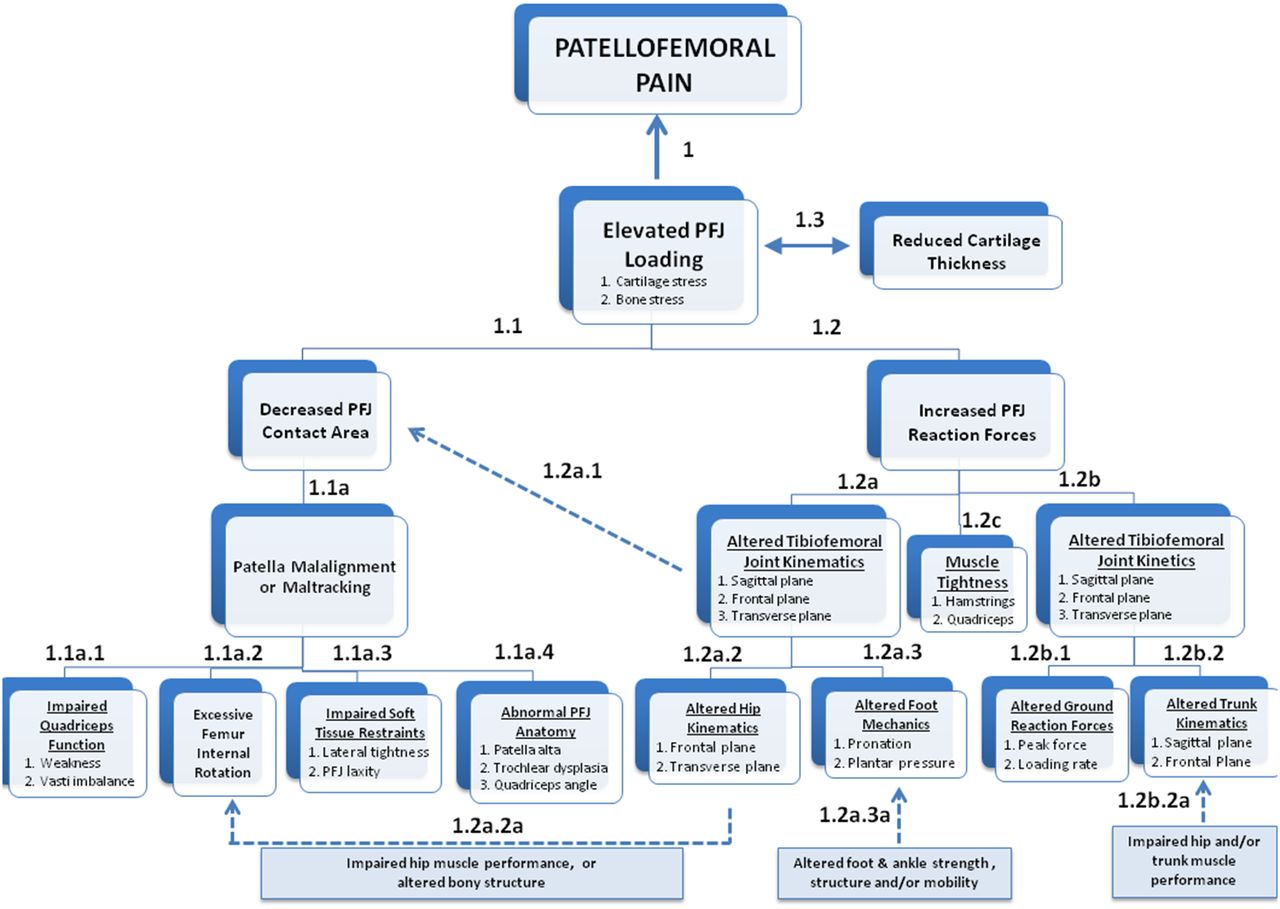
The aetiology of patellofemoral pain (PFP) is a complex interplay among various anatomical, biomechanical, psychological, social and behavioural influences. Numerous factors associated with PFP have been reported in the literature, but the interaction between these proposed risk factors and the clinical entity of PFP remains unclear (figure 1).

{kind=link}
Schematic overview of potential pathways to elevated patellofemoral joint (PFJ) stress, a proposed contributor to patellofemoral pain.
The goal of this consensus document is to place known associated factors within the context of a pathomechanical model of PFP. An underlying assumption of the proposed pathomechanical model is that PFP is associated with abnormal loading of the patellofemoral joint (elevated joint stress). In this model, abnormal loading could affect the various patellofemoral structures that can contribute to nociception (ie, subchondral bone, infrapatellar fat pad, retinaculum and ligamentous structures); however, the specific tissue sources related to PFP are not known.
The experience of PFP is not just nociception.1 Persons with persistent PFP exhibit abnormal nociceptive processing (ie, widespread mechanical hyperalgesia, impaired pain modulation),2–5 altered somatosensory processing (implying neuropathic pain),6 impaired sensorimotor function (ie, proprioception and balance)7–10 and certain psychological factors (ie, catastrophising and kinesiophobia).11 The amount and quality of research in the non-‘patho-mechanical’ pathways to PFP are evolving, and will be included in future consensus statements emanating from the International Patellofemoral Pain Research Retreats.
At the 4th International Patellofemoral Pain Research Retreat,12 Dr Christopher Powers presented a draft framework of the pathomechanical model, which was based on prior consensus statements from the three previous Patellofemoral Pain Research Retreats.13–15 At the meeting, all attendees (clinician-researchers and research scientists) participated in a comprehensive discussion of the draft model, and agreed on the overall framework (Figure 1). Following the retreat, the authors conducted a thorough review of pertinent literature related to the specific pathways specified within the pathomechanical model.
The current document does not include risk factors for patellofemoral osteoarthritis. It also should be noted that the associated factors and statements in the current document pertain only to PFP, and not patellar instability. Although it is likely that many of the factors associate with PFP also play a role in patellar instability (particularly anatomical and biomechanical factors), the research that has formed the basis of this document primarily has focused on persons with pain.
The current consensus document should be viewed as a ‘living document’ and will be reviewed and edited as necessary at future retreats based on new research findings. In the interim, it is anticipated that this document will provide the basis from which to frame research questions related to PFP and provide clinicians with a contemporary synthesis of current evidence.
1. Maclachlan LR, Collins NJ, Matthews MLG, Hodges PW, Vicenzino B. The psychological features of patellofemoral pain: a systematic review. Br J Sports Med 2017;51(9):732–42
2. Rathleff MS, Petersen KK, Arendt-Nielsen L, et al. Impaired conditioned pain modulation in young female adults with long-standing patellofemoral pain: a Single Blinded Cross-Sectional Study. Pain Med 2016;17(5):980–8.
3. Noehren B, Shuping L, Jones A, et al. Somatosensory and biomechanical abnormalities in females with patellofemoral pain. Clin J Pain. 2015;32(10):915–9.
4. Rathleff MS, Roos EM, Olesen JL, et al. Lower mechanical pressure pain thresholds in female adolescents with patellofemoral pain syndrome. J Orthop Sports Phys Ther 2013;43(6):414–21.
5. Fingleton C, Smart K, Moloney N, et al. Pain sensitization in people with knee osteoarthritis: a systematic review and meta-analysis. Osteoarthritis Cartilage 2015;23(7):1043–56.
6. Jensen R, Kvale A, Baerheim A. Is pain in patellofemoral pain syndrome neuropathic? Clin J Pain 2008;24(5):384–94.
7. Yosmaoglu HB, Kaya D, Guney H, et al. Is there a relationship between tracking ability, joint position sense, and functional level in patellofemoral pain syndrome? Knee Surg Sports Traumatol Arthrosc 2013;21(11):2564–71.
8. Naseri N, Pourkazemi F. Difference in knee joint position sense in athletes with and without patellofemoral pain syndrome. Knee Surg Sports Traumatol Arthrosc 2012;20(10):2071–76.
9. Yilmaz Yelvar GD, Cirak Y, Dalkilinc M, et al. Impairments of postural stability, core endurance, fall index and functional mobility skills in patients with patello femoral pain syndrome. J Back Musculoskelet Rehabil 2016; Epub ahead of print.
10. Lee SP, Souza RB, Powers CM. The influence of hip abductor muscle performance on dynamic postural stability in females with patellofemoral pain. Gait Posture 2012;36(3):425–9.
11. Domenech J, Sanchis-Alfonso V, Espejo B. Changes in catastrophizing and kinesiophobia are predictive of changes in disability and pain after treatment in patients with anterior knee pain. Knee Surg Sports Traumatol Arthrosc 2014;22(10):2295–300.
12. Crossley KM, Stefanik JJ, Selfe J, Collines NJ, David IS, Powers CM, McConnell J, Vicenzino B, Bazett-Jones DM, Esculier JF, Morrisey D, Callaghan MJ. 2016 patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: terminology. Definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br J Sports Med 2016;50(14):839–843.
13. Davis IS, Powers CM. Patellofemoral pain syndrome: proximal, distal and local factors. consensus statements from the 2009 International Patellofemoral Research Retreat. J Orthop Sports Phys Ther 2010;40(3):A1-A48.
14. Powers CM, Bolgla LA, Callaghan M, et al. Patellofemoral pain: proximal, distal and local factors, 2nd International Research Retreat. J Orthop Sports Phys Ther 2012;42(6):A1-A54.
15. Witrouw E, Callaghan MJ, Stefanik JJ, et al. Patellofemoral pain: Consensus statement from the 3rd International Patellofemoral Pain Research Retreat held in Vancouver, September 2013. Br J Sports Med 2014;48(6):411–414.
Statement 1. Persons with PFP exhibit elevated patellofemoral joint, cartilage and bone stress during functional tasks; however, this finding is not consistent across studies. Currently, no prospective studies have linked elevated mechanical stress to the development of PFP.
Persons with PFP exhibit greater patellofemoral jiont (PFJ) stress during walking,1 as well as patellar cartilage stress and bone strain during squatting (45° knee flexion).2–3 However, studies that evaluated PFJ and patellar cartilage stress during tasks with relatively higher knee flexion angles (ie, stair ambulation, running and squatting to 60°) have not reported differences between persons with and without PFP.4–6 Similarly, braced-induced reductions in PFJ stress during walking resulted in an immediate decrease in PFP symptoms,7 but the same stress–pain relationship was not reported during stair ambulation.8
The exact mechanism by which elevated joint loading may contribute to PFP is not clear. Repetitive overloading of the PFJ may increase patellar subchondral bone metabolic activity9,10 and/or elevate patellar bone water content.11 Elevated water content could increase the intraosseous pressure within the patella, thus stimulating pressure-sensitive mechanical nociceptors.11,12 In support of this premise, it has been reported that runners with PFP exhibit elevated bone water content,10 and that running-induced PFP fluctuates with changes in patellar water content.12
1. Heino BJ, Powers CM. Patellofemoral stress during walking in persons with and without patellofemoral pain. Med Sci Sports Exerc 2002;34(10):1582–93.
2. Farrokhi S, Keyak JH, Powers CM. Individuals with patellofemoral pain exhibit greater patellofemoral joint stress: a finite element analysis study. Osteoarthritis Cartilage 2011;19(3):287–94.
3. Ho KY, Keyak JH, Powers CM. Comparison of patella bone strain between females with and without patellofemoral pain: A finite element analysis study. J Biomech 2014;47(1):230–36.
4. Brechter JH, Powers CM. Patellofemoral joint stress during stair ascent and descent in persons with and without patellofemoral pain. Gait Posture 2002;16(2):115–23.
5. Besier TF, Pal S, Draper CE, et al. The role of cartilage stress in patellofemoral pain. Med Sci Sports Exerc 2015;47(11):2416–2.
6. Wirtz AD, Willson JD, Kernozek TW, et al. Patellofemoral joint stress during running in females with and without patellofemoral pain. Knee 2012;19(5):703–08.
7. Powers CM, Ward SR, Chen YJ, et al. The effect of bracing on patellofemoral joint stress during free and fast walking. Am J Sports Med 2004;32(1):224–31.
8. Powers CM, Ward SR, Chan LD, et al. The effect of bracing on patella alignment and patellofemoral joint contact area. Med Sci Sports Exerc 2004;36(7):1226–32.
9. Dye SF. The pathophysiology of patellofemoral pain: a tissue homeostasis perspective. Clin Orthop Relat Res 2005;436:100–10.
10. Draper CE, Fredericson M, Gold GE, et al. Patients with patellofemoral pain exhibit elevated bone metabolic activity at the patellofemoral joint. J Orthop Res 2012;30(2):209–13.
11. Ho KY, Hu HH, Colletti PM, et al. Recreational runners with patellofemoral pain exhibit elevated patella water content. Magn Reson Imaging 2014;32(7):965–68.
12. Ho KY, Hu HH, Colletti PM, et al. Running-induced patellofemoral pain fluctuates with changes in patella water content. Eur J Sport Sci 2014;14(6):628–34.
Statement 1.1. Elevated patellofemoral joint stress can result from diminished contact area in persons with PFP, but this is variable and likely dependent on knee flexion angle.
Elevated patellofemoral joint stress during walking in persons with PFP is the result of diminished contact area.1 However, diminished contact area in this population appears to be dependent on the knee flexion angle evaluated. For example, some studies found a difference in available contact area during relatively higher knee flexion angles between persons with and without PFP,2 while others did not.3–5 The premise that lower contact area in persons with PFP may be knee flexion-dependent is supported by research reporting diminished contact area in this population at 20°, but not 40° of knee flexion.4 Contact area differences between persons with and without PFP are minimised once the patella moves deeper within the femoral trochlea.4
1. Heino BJ, Powers CM. Patellofemoral stress during walking in persons with and without patellofemoral pain. Med Sci Sports Exerc 2002;34(10):1582–93.
2. Hinterwimmer S, Gotthardt M, von Eisenhart-Rothe R, et al. In vivo contact areas of the knee in patients with patellar subluxation. J Biomech 2005;38(10):2095–101.
3. Brechter JH, Powers CM. Patellofemoral joint stress during stair ascent and descent in persons with and without patellofemoral pain. Gait Posture 2002;16(2):115–23.
4. Besier TF, Pal S, Draper CE, et al. The role of cartilage stress in patellofemoral pain. Med Sci Sports Exerc 2015;47(11):2416–2.
5. Salsich GB, Perman WH. Tibiofemoral and patellofemoral mechanics are altered at small knee flexion angles in people with patellofemoral pain. J Sci Med Sport 2013;16(1):13–17.
Statement 1.1a. Patellar malalignment and/or maltracking in persons with PFP can contribute to diminished contact area, but only in a subset of persons with PFP.
Patellar malalignment and/or maltracking in persons with PFP can result in diminished contact area.1–3 A systematic review of 40 studies reported that lateral patellar displacement in persons with PFP is more pronounced in knee extension, regardless of weightbearing status.4
Although persons with PFP exhibit patellar malalignment,5–9 and/or altered patellar kinematics,10–15 this finding is not consistent across all studies.16–18 This suggests that altered patellar alignment or tracking may not be a universal finding in this population. In addition, conflicting findings may be attributed to differences in the methods used to quantify patellar tracking (ie, dynamic MRI, CT and others), the conditions under which patellar alignment/tracking was quantified (static vs dynamic; weightbearing vs non-weightbearing), and the specific measurements and frames of reference used (two-dimensional (2D) vs three-dimensional).
1. Salsich GB, Perman WH. Tibiofemoral and patellofemoral mechanics are altered at small knee flexion angles in people with patellofemoral pain. J Sci Med Sport 2013;16(1):13–17.
2. Powers CM, Ward SR, Chan LD, et al. The effect of bracing on patella alignment and patellofemoral joint contact area. Med Sci Sports Exerc 2004;36(7):1226–32.
3. Ward SR, Terk MR, Powers CM. Patella alta: association with patellofemoral alignment and changes in contact area during weight-bearing. J Bone Joint Surg Am 2007;89(8):1749–55.
4. Drew BT, Redmond AC, Smith TO, et al. Which patellofemoral joint imaging features are associated with patellofemoral pain? Systematic review and meta-analysis. Osteoarthritis Cartilage 2016;24(2):224–36.
5. Salsich GB, Perman WH. Patellofemoral joint contact area is influenced by tibiofemoral rotation alignment in individuals who have patellofemoral pain. J Orthop Sports Phys Ther 2007;37(9):521–28.
6. Aglietti P, Insall JN, Cerulli G. Patellar pain and incongruence. I: Measurements of incongruence. Clin Orthop Relat Res 1983(176):217–24.
7. Biedert R, Gruhl C. Axial computed tomography of the patellofemoral joint with and without quadriceps contraction. Arch Orthop Trauma Surg 1997;116(1-2):77–82.
8. Taskiran E, Dinedurga Z, Yagiz A, et al. Effect of the vastus medialis obliquus on the patellofemoral joint. Knee Surg Sports Traumatol Arthrosc 1998;6 (3):173–80.
9. Witonski D, Goraj B. Patellar motion analyzed by kinematic and dynamic axial magnetic resonance imaging in patients with anterior knee pain syndrome. Arch Orthop Trauma Surg 1999;119(1-2):46–9.
10. Draper CE, Besier TF, Santos JM, et al. Using real-time MRI to quantify altered joint kinematics in subjects with patellofemoral pain and to evaluate the effects of a patellar brace or sleeve on joint motion. J Orthop Res 2009;27(5):571–77.
11. Wilson NA, Press JM, Koh JL, et al. In vivo noninvasive evaluation of abnormal patellar tracking during squatting in patients with patellofemoral pain. J Bone Joint Surg Am 2009;91(3):558–66.
12. Souza RB, Draper CE, Fredericson M, et al. Femur rotation and patellofemoral joint kinematics: a weight-bearing magnetic resonance imaging analysis. J Orthop Sports Phys Ther 2010;40(5):277–85.
13. Haim A, Yaniv M, Dekel S, et al. Patellofemoral pain syndrome: validity of clinical and radiological features. Clin Orthop Relat Res 2006;451:223–28.
14. MacIntyre N, Hill N, Fellows R, et al. Patellofemoral joint kinematics in individuals with and without patellofemoral pain syndrome. J Bone Joint Surg Am 2006;88(12):2596–605.
15. Powers CM. Patellar kinematics, part I: the influence of vastus muscle activity in subjects with and without patellofemoral pain. Phys Ther 2000;80(10):956–64.
16. Laprade J, Culham E. Radiographic measures in subjects who are asymptomatic and subjects with patellofemoral pain syndrome. Clin Orthop Relat Res 2003;414:172–82.
17. Powers CM, Ward SR, Fredericson M, et al. Patellofemoral kinematics during weight-bearing and non-weight-bearing knee extension in persons with lateral subluxation of the patella: a preliminary study. J Orthop Sports Phys Ther 2003;33(11):677–85.
18. Draper CE, Besier TF, Fredericson M, et al. Differences in patellofemoral kinematics between weight-bearing and non-weight-bearing conditions in patients with patellofemoral pain. J Orthop Res 2011;29(3):312–17.
Statement 1.1a.1. Impaired quadriceps function is a common finding in persons with PFP, but its role in patellar malalignment and/or maltracking is unclear.
Generalised quadriceps weakness and/or atrophy is evident in idiopathic PFP1–3; however, isolated atrophy of the vastus medialis (VM) has not been consistently reported.4,5 Similarly, altered magnitude and/or timing of VM activation (determined using electromyography) relative to the vastus lateralis (VL) is not consistently implicated in PFP.6–11 Nonetheless, quadriceps weakness,1,12 as well as delayed onset of VM relative to VL,13,14 is associated with the development of PFP.
Cadaveric studies demonstrate that simulated muscle force imbalance of the VM relative to the VL results in lateral patellar displacement and tilt,15,16 and increased contact pressures on the lateral patellar facet.17 However, diminished force generation of the VM following a motor branch block in vivo explained some, but not all, of the expected changes in lateral patellar displacement and tilt.18
Reduced activation and/or delayed onset timing of the VM relative to the VL is associated with increased lateral patellar tilt and displacement.19,20 The inverse association between lateral patellar displacement and VM activation21 suggests that increased motor unit activity may be a response to meet the increased demand of providing medial patellar stability. While activation of the synergistic medial and lateral components of the vasti may be altered in a subgroup/proportion of persons with PFP, the implication of this altered activation in relationship to patellar kinematics is unclear.
1. Lankhorst NE, Bierma-Zeinstra SM, van Middelkoop M. Risk factors for patellofemoral pain syndrome: a systematic review. J Orthop Sports Phys Ther 2012;42(2):81–94.
2. Kaya D, Citaker S, Kerimoglu U, et al. Women with patellofemoral pain syndrome have quadriceps femoris volume and strength deficiency. Knee Surg Sports Traumatol Arthrosc 2011;19(2):242–7.
3. Werner S. An evaluation of knee extensor and knee flexor torques and EMGs in patients with patellofemoral pain syndrome in comparison with matched controls. Knee Surg Sports Traumatol Arthrosc 1995;3(2):89–94.
4. Pattyn E, Verdonk P, Steyaert A, et al. Vastus medialis obliquus atrophy: does it exist in patellofemoral pain syndrome? Am J Sports Med 2011;39(7):1450–5.
5. Giles LS, Webster KE, McClelland JA, et al. Atrophy of the Quadriceps is not isolated to the vastus medialis oblique in individuals with patellofemoral pain. J Orthop Sports Phys Ther 2015;45(8):613–9.
6. Cowan SM, Bennell KL, Hodges PW, et al. Delayed onset of electromyographic activity of vastus medialis obliquus relative to vastus lateralis in subjects with patellofemoral pain syndrome. Arch Phys Med Rehabil 2001;82(2):183–9.
7. Cowan SM, Hodges PW, Bennell KL, et al. Altered vastii recruitment when people with patellofemoral pain syndrome complete a postural task. Arch Phys Med Rehabil 2002;83(7):989–95.
8. Cowan SM, Bennell KL, Crossley KM, et al. Physical therapy alters recruitment of the vasti in patellofemoral pain syndrome. Med Sci Sports Exerc 2002;34(12):1879–85.
9. Cavazzuti L, Merlo A, Orlandi F, et al. Delayed onset of electromyographic activity of vastus medialis obliquus relative to vastus lateralis in subjects with patellofemoral pain syndrome. Gait Posture 2010;32(3):290–5.
10. Karst GM, Willett GM. Onset timing of electromyographic activity in the vastus medialis oblique and vastus lateralis muscles in subjects with and without patellofemoral pain syndrome. Phys Ther 1995;75(9):813–23.
11. Powers CM, Landel R, Perry J. Timing and intensity of vastus muscle activity during functional activities in subjects with and without patellofemoral pain. Phys Ther 1996;76(9):946–55.
12. Pappas E, Wong-Tom WM. Prospective predictors of patellofemoral pain syndrome: a systematic review with meta-analysis. Sports Health 2012;4(2):115–20.
13. Witvrouw E, Lysens R, Bellemans J, et al. Intrinsic risk factors for the development of anterior knee pain in an athletic population. A two year prospective study. Am J Sports Med 2000;28(4):480–9.
14. Van Tiggelen D, Cowan S, Coorevits P, et al. Delayed vastus medialis obliquus to vastus lateralis onset timing contributes to the development of patellofemoral pain in previously healthy men: a prospective study. Am J Sports Med 2009;37(6):1099–105.
15. Amis AA. Current concepts on anatomy and biomechanics of patellar stability. Sports Med Arthrosc 2007;15.
16. Lorenz A, Muller O, Kohler P, et al. The influence of asymmetric quadriceps loading on patellar tracking--an in vitro study. Knee 2012;19(6):818–22.
17. Goh JC, Lee PY, Bose K. A cadaver study of the function of the oblique part of vastus medialis. J Bone Joint Surg Br 1995;77(2):225–31.
18. Sheehan FT, Borotikar BS, Behnam AJ, et al. Alterations in in vivo knee joint kinematics following a femoral nerve branch block of the vastus medialis: Implications for patellofemoral pain syndrome. Clin Biomech (Bristol, Avon) 2012;27(6):525–31.
19. Pal S, Draper CE, Fredericson M, et al. Patellar maltracking correlates with vastus medialis activation delay in patellofemoral pain patients. Am J Sports Med 2011;39(3):590–8.
20. Pal S, Besier TF, Draper CE, et al. Patellar tilt correlates with vastus lateralis: vastus medialis activation ratio in maltracking patellofemoral pain patients. J Orthop Res 2012;30(6):927–33.
21. Powers CM. Patellar kinematics, part I: the influence of vastus muscle activity in subjects with and without patellofemoral pain. Phys Ther 2000;80(10):956–64.
Statement 1.1a.2. Internal rotation of the femur can contribute to patellar malalignment and maltracking.
During weightbearing, internal rotation of the femur underneath the patella is an important contributor to lateral patellar tilt and displacement.1 Altered patellofemoral joint kinematics in women with PFP is associated with excessive internal rotation of the femur during a single leg squat task as measured using weightbearing MRI.2
1. Powers CM, Ward SR, Fredericson M, et al. Patellofemoral kinematics during weight-bearing and non-weight-bearing knee extension in persons with lateral subluxation of the patella: a preliminary study. J Orthop Sports Phys Ther 2003;33(11):677–85.
2. Souza RB, Draper CE, Fredericson M, et al. Femur rotation and patellofemoral joint kinematics: a weight-bearing magnetic resonance imaging analysis. J Orthop Sports Phys Ther 2010;40(5):277–85.
Statement 1.1a.3. There is evidence that persons with PFP exhibit impairments related to soft tissue restraints, and that these impairments may contribute to patellar malalignment and/or maltracking.
Persons with PFP have a tighter1 and thicker2 iliotibial band compared with pain-free individuals. Based on in vivo and cadaveric studies, iliotibial band tension has a substantial effect on patellar alignment and lateral patellar translation.3–5 Currently, it is not known whether iliotibial band tightness and thickening is an adaptation to or a cause of lateral tilt/translation of the patella.
Ligamentous injury or laxity (particularly the medial patellofemoral ligament) can contribute to altered patellar tracking.6 Although ligamentous laxity has been proposed to be a risk factor for patellar instability,7 increased passive mobility of the patella has not been reported in persons with PFP.8 However, generalised ligamentous laxity is associated with PFP development.9
1. Hudson Z, Darthuy E. Iliotibial band tightness and patellofemoral pain syndrome: a case-control study. Man Ther 2009;14(2):147–51.
2. Schoots EJ, Tak IJ, Veenstra BJ, et al. Ultrasound characteristics of the lateral retinaculum in 10 patients with patellofemoral pain syndrome compared to healthy controls. J Bodyw Mov Ther 2013;17(4):523–9.
3. Kang SY, Choung SD, Park JH, et al. The relationship between length of the iliotibial band and patellar position in Asians. Knee 2014;21(6):1135–38.
4. Merican AM, Amis AA. Iliotibial band tension affects patellofemoral and tibiofemoral kinematics. J Biomech 2009;42(10):1539–46.
5. Kwak SD, Ahmad CS, Gardner TR, et al. Hamstrings and iliotibial band forces affect knee kinematics and contact pattern. J Orthop Res 2000;18(1):101–08.
6. Stephen JM, Kader D, Lumpaopong P, et al. Sectioning the medial patellofemoral ligament alters patellofemoral joint kinematics and contact mechanics. J Orthop Res 2013;31(9):1423–9.
7. Koh JL, Stewart C. Patellar instability. Clin Sports Med 2014;33(3):461–76.
8. Ota S, Nakashima T, Morisaka A, et al. Comparison of patellar mobility in female adults with and without patellofemoral pain. J Orthop Sports Phys Ther 2008;38(7):396–402.
9. Witvrouw E, Lysens R, Bellemans J, et al. Intrinsic risk factors for the development of anterior knee pain in an athletic population. A two year prospective study. Am J Sports Med 2000;28(4):480–9.
Statement 1.1a.4. Patellar alignment and patellofemoral joint kinematics are influenced by the bony geometry of the distal femur, patellar height, but not the static quadriceps angle (Q-angle).
The sulcus angle and inclination of the lateral anterior femoral condyle are important determinants of patellar malalignment and maltracking.1–4 However, the inclination of the lateral anterior femoral condyle is a better predictor of mediolateral tracking of the patella than the sulcus angle.3,4
The height of the patella within the trochlear groove is an important contributor to malalignment and maltracking of the patella. For example, lateral patellar tilt and displacement is more prevalent in persons with patellar alta than persons with normal patellar height.5,6 In addition, patellar height is the best structural predictor of lateral patellar tilt at 0° of knee flexion.4 Persons with patellar alta exhibit lower contact area for a given knee flexion angle5 and higher patellofemoral stress during fast walking.7
A systematic review of prospective studies indicates the Q-angle as a static measure is not a risk factor for PFP.8 Based on MRI measurements, the static Q-angle does not represent the quadriceps line-of-action, and this measurement should not be used to infer patellofemoral kinematics.9
1. Powers CM. Patellar kinematics, part II: the influence of the depth of the trochlear groove in subjects with and without patellofemoral pain. Phys Ther 2000;80(10):965–78.
2. Varadarajan KM, Freiberg AA, Gill TJ, et al. Relationship between three-dimensional geometry of the trochlear groove and in vivo patellar tracking during weight-bearing knee flexion. J Biomech Eng 2010;132(6):061008.
3. Harbaugh CM, Wilson NA, Sheehan FT. Correlating femoral shape with patellar kinematics in patients with patellofemoral pain. J Orthop Res 2010;28(7):865–72.
4. Teng HL, Chen YJ, Powers CM. Predictors of patellar alignment during weight bearing: An examination of patellar height and trochlear geometry. Knee 2014;21(1):142–46.
5. Ward SR, Terk MR, Powers CM. Patella alta: association with patellofemoral alignment and changes in contact area during weight-bearing. J Bone Joint Surg Am 2007;89(8):1749–55.
6. Pal S, Besier TF, Beaupre GS, et al. Patellar maltracking is prevalent among patellofemoral pain subjects with patella alta: An upright, weightbearing MRI study. J Orthop Res 2013;31(3):448–57.
7. Ward SR, Powers CM. The influence of patella alta on patellofemoral joint stress during normal and fast walking. Clin Biomech (Bristol, Avon) 2004;19(10):1040–47.
8. Lankhorst NE, Bierma-Zeinstra SM, van Middelkoop M. Risk factors for patellofemoral pain syndrome: a systematic review. J Orthop Sports Phys Ther 2012;42(2):81–94.
9. Freedman BR, Brindle TJ, Sheehan FT. Re-evaluating the functional implications of the Q-angle and its relationship to in-vivo patellofemoral kinematics. Clin Biomech (Bristol, Avon) 2014;29(10):1139–45.
Statement 1.2. Patellofemoral (PF) joint reaction forces in persons with PFP differ from those in pain-free individuals.
Persons with PFP exhibit lower peak resultant PF joint reaction forces compared with healthy controls during walking,1,2 running1 and stair ambulation.1,3 However, persons with PFP have a higher lateral component of the PF joint reaction force than do pain-free individuals.1 The lower resultant PF joint reaction forces in persons with PFP may represent a compensatory strategy to minimise patellofemoral joint loading during functional tasks.
1. Chen YJ, Powers CM. Comparison of three-dimensional patellofemoral joint reaction forces in persons with and without patellofemoral pain. J Appl Biomech 2014;30(4):493–500.
2. Heino BJ, Powers CM. Patellofemoral stress during walking in persons with and without patellofemoral pain. Med Sci Sports Exerc 2002;34(10):1582–93.
3. Brechter JH, Powers CM. Patellofemoral joint stress during stair ascent and descent in persons with and without patellofemoral pain. Gait Posture 2002;16(2):115–23.
Statement 1.2a. Persons with PFP exhibit differences in tibiofemoral kinematics in all three planes of motion compared with pain-free individuals, but not consistently.
Altered tibiofemoral joint kinematics in the sagittal, frontal and transverse planes can influence the magnitude and direction of the resultant PF joint reaction force vector.1 In the sagittal plane, greater knee flexion would be expected to increase the posterior (compression) component of the PF joint reaction force vector. However, persons with PFP exhibit lower knee flexion during walking,2 stair ambulation3–5 and running.6 Although reduced knee flexion in persons with PFP may represent a compensatory strategy to minimise patellofemoral joint loading during functional tasks (statement 1.2), the finding of reduced knee flexion during ambulatory tasks is not consistent across all studies.7–11 Interestingly, it has reported that lower knee flexion during a jump-landing task is a risk factor for the development of PFP.12
Increased frontal plane motion of the knee (ie, abduction or valgus) can increase the laterally directed component of the patellofemoral joint reaction force (PFJRF) vector.1 Although persons with PFP exhibit increased knee abduction during gait,13 and single tasks such as squatting,14–17 stepping18 and hop landing,17 higher knee abduction has not been reported during stair descent19 or running.20 Furthermore, 2D measures of knee valgus can predict the development of PFP.21 Knee abduction also is correlated with self-reported pain in men and women with PFP.22
Transverse plane tibiofemoral rotation also can affect the laterally directed component of the PFJRF vector, with the influence dependent on relative segmental motion. For example, internal rotation of the femur relative to the tibia can increase the laterally directed forces acting on the patella, while tibia internal rotation relative to the femur would result in a reduction of the laterally directed forces acting on the patella.1 While women with PFP exhibit higher degrees of knee external rotation during single leg squats, jumps and running,23 greater degrees of knee internal rotation have been reported in persons with PFP during stair descent.24 It should be noted that the finding of abnormal tibiofemoral rotation during stair descent is not consistent across studies.19
1. Powers CM. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther 2003;33(11):639–46.
2. Powers CM, Heino JG, Rao S, et al. The influence of patellofemoral pain on lower limb loading during gait. Clin Biomech (Bristol, Avon) 1999;14(10):722–8.
3. Silva Dde O, Briani RV, Pazzinatto MF, et al. Reduced knee flexion is a possible cause of increased loading rates in individuals with patellofemoral pain. Clin Biomech (Bristol, Avon) 2015;30(9):971–5.
4. de Oliveira Silva D, Barton CJ, Pazzinatto MF, et al. Proximal mechanics during stair ascent are more discriminate of females with patellofemoral pain than distal mechanics. Clin Biomech (Bristol, Avon) 2016;35:56–61.
5. Crossley KM, Cowan SM, Bennell KL, et al. Knee flexion during stair ambulation is altered in individuals with patellofemoral pain. J Orthop Res 2004;22(2):267–74.
6. Dierks TA, Manal KT, Hamill J, et al. Lower extremity kinematics in runners with patellofemoral pain during a prolonged run. Med Sci Sports Exerc 2011;43(4):693–700.
7. Powers CM, Landel R, Perry J. Timing and intensity of vastus muscle activity during functional activities in subjects with and without patellofemoral pain. Phys Ther 1996;76(9):946–55.
8. Powers CM, Perry J, Hsu A, et al. Are patellofemoral pain and quadriceps femoris muscle torque associated with locomotor function? Phys Ther 1997;77(10):1063–75.
9. Heino BJ, Powers CM. Patellofemoral stress during walking in persons with and without patellofemoral pain. Med Sci Sports Exerc 2002;34(10):1582–93.
10. Brechter JH, Powers CM. Patellofemoral joint stress during stair ascent and descent in persons with and without patellofemoral pain. Gait Posture 2002;16(2):115–23.
11. Wirtz AD, Willson JD, Kernozek TW, et al. Patellofemoral joint stress during running in females with and without patellofemoral pain. Knee 2012;19(5):703–08.
12. Boling MC, Padua DA, Marshall SW, et al. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am J Sports Med 2009;37(11):2108–16.
13. Salsich GB, Long-Rossi F. Do females with patellofemoral pain have abnormal hip and knee kinematics during gait? Physiother Theory Pract 2010;26(3):150–9.
14. Willson JD, Davis IS. Utility of the frontal plane projection angle in females with patellofemoral pain. J Orthop Sports Phys Ther 2008;38(10):606–15.
15. Nakagawa TH, Maciel CD, Serrao FV. Trunk biomechanics and its association with hip and knee kinematics in patients with and without patellofemoral pain. Man Ther 2015;20(1):189–93.
16. Nakagawa TH, Moriya ET, Maciel CD, et al. Trunk, pelvis, hip, and knee kinematics, hip strength, and gluteal muscle activation during a single-leg squat in males and females with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther 2012;42(6):491–501.
17. Herrington L. Knee valgus angle during single leg squat and landing in patellofemoral pain patients and controls. Knee 2014;21(2):514–7.
18. Nakagawa TH, Moriya ET, Maciel CD, et al. Frontal plane biomechanics in males and females with and without patellofemoral pain. Med Sci Sports Exerc 2012;44(9):1747–55.
19. Bolgla LA, Malone TR, Umberger BR, et al. Hip strength and hip and knee kinematics during stair descent in females with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther 2008;38(1):12–8.
20. Noehren B, Sanchez Z, Cunningham T, et al. The effect of pain on hip and knee kinematics during running in females with chronic patellofemoral pain. Gait Posture 2012;36(3):596–9.
21. Holden S, Boreham C, Doherty C, et al. Two-dimensional knee valgus displacement as a predictor of patellofemoral pain in adolescent females. Scand J Med Sci Sports 2015.
22. Nakagawa TH, Serrao FV, Maciel CD, et al. Hip and knee kinematics are associated with pain and self-reported functional status in males and females with patellofemoral pain. Int J Sports Med 2013;34(11):997–1002.
23. Willson JD, Davis IS. Lower extremity mechanics of females with and without patellofemoral pain across activities with progressively greater task demands. Clin Biomech (Bristol, Avon) 2008;23(2):203–11.
24. Schwane BG, Goerger BM, Goto S, et al. Trunk and lower extremity kinematics during stair descent in women with or without patellofemoral pain. J Athl Train 2015;50(7):704–12.
Statement 1.2a.1. Altered tibiofemoral joint kinematics in the sagittal, frontal and transverse planes can influence available contact area to distribute PF joint reaction forces.
Patellofemoral joint contact area increases with knee flexion,1,2 and lower knee flexion during dynamic tasks such as gait and running could result in less available contact area to distribute PF joint reaction forces.
Tibiofemoral rotation is associated with contact area in persons with PFP.3 For example, internal rotation of the femur relative to the tibia is associated with reduced contact area and elevated patellar cartilage stress at 15° and 45° knee flexion.4 However, this association has not been observed at 60°,5 suggesting that the influence of tibiofemoral rotation on contact area is less pronounced at larger knee flexion angles. External rotation of the tibia relative to the femur can reduce contact area and increase PFJ stress, while internal rotation of the tibia relative to the femur has little impact on PFJ contact areas and pressures.6
Small degrees of simulated knee valgus (5°) do not affect patellofemoral contact mechnanics7; however, a 10° change in the frontal plane alignment of the extensor mechanism increases patellofemoral joint pressures by 45%.8 Interestingly, the elevated contact pressures observed in this study occurred without a change in contact area, suggesting that the finding of elevated patellofemoral stress was likely a function of increase in the laterally directed PFJRF.8
1. Besier TF, Draper CE, Gold GE, et al. Patellofemoral joint contact area increases with knee flexion and weight-bearing. J Orthop Res 2005;23(2):345–50.
2. Salsich GB, Ward SR, Terk MR, et al. In vivo assessment of patellofemoral joint contact area in individuals who are pain free. Clin Orthop Relat Res 2003(417):277–84.
3. Salsich GB, Perman WH. Patellofemoral joint contact area is influenced by tibiofemoral rotation alignment in individuals who have patellofemoral pain. J Orthop Sports Phys Ther 2007;37(9):521–28.
4. Liao TC, Yang N, Ho KY, et al. Femur rotation increases patella cartilage stress in females with patellofemoral pain. Med Sci Sports Exerc 2015;47(9):1775–80.
5. Besier TF, Gold GE, Delp SL, et al. The influence of femoral internal and external rotation on cartilage stresses within the patellofemoral joint. J Orthop Res 2008;26(12):1627–35.
6. Lee TQ, Yang BY, Sandusky MD, et al. The effects of tibial rotation on the patellofemoral joint: assessment of the changes in in situ strain in the peripatellar retinaculum and the patellofemoral contact pressures and areas. J Rehabil Res Dev 2001;38(5):463–9.
7. Bryant BJ, Tilan JU, McGarry MH, et al. The biomechanical effect of increased valgus on total knee arthroplasty: a cadaveric study. J Arthroplasty 2014;29(4):722–6.
8. Huberti HH, Hayes WC. Patellofemoral contact pressures. The influence of q-angle and tendofemoral contact. J Bone Joint Surg Am 1984;66(5):715–24.
Statement 1.2a.2. Persons with PFP exhibit altered hip kinematics; however, findings are not consistent among all studies.
Given that the hip joint shares a common segment with the tibiofemoral joint (ie, femur), abnormal hip kinematics could contribute to the altered tibiofemoral kinematics described above (statement 1.2a).1 The motions of hip adduction and knee abduction are significantly correlated, resulting in medial displacement of the knee.2 With respect to tibiofemoral rotation, internal rotation of the femur relative to the tibia (ie, hip internal rotation) could result in relative tibiofemoral external rotation and vice versa. Hip internal rotation was also correlated with knee abduction during single limb squats3; however, the opposite was evident during running, where greater hip external rotation was associated with greater knee abduction angles.4
Persons with PFP exhibit excessive hip adduction during a wide range of functional tasks including running, stepping and landing from a jump. The results of two systematic reviews have concluded that there is a moderate association between hip adduction and PFP.5,6 Furthermore, excessive hip adduction predicts self-reported PFP and function during a stepdown task.7 Additionally, a prospective study reported that hip adduction was significantly greater in runners who later went on to develop PFP.8
Similarly, persons with PFP exhibit excessive hip internal rotation during running, stepping and landing from a jump,9 although this finding has not been consistent across all studies.10 A systematic review also identified a moderate association between hip internal rotation during running and PFP.6 Furthermore, hip internal rotation can predict self-reported pain and function during a stepdown task,7 and the development of PFP in Naval Academy cadets.11 Interestingly, lower than normal hip internal rotation has been observed during gait in persons with PFP,12 13 which may represent a compensatory strategy to avoid pain.
1. Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther 2010;40(2):42–51.
2. Willson JD, Davis IS. Utility of the frontal plane projection angle in females with patellofemoral pain. J Orthop Sports Phys Ther 2008;38(10):606–15.
3. Hollman JH, Galardi CM, Lin IH, et al. Frontal and transverse plane hip kinematics and gluteus maximus recruitment correlate with frontal plane knee kinematics during single-leg squat tests in women. Clin Biomech (Bristol, Avon) 2014;29(4):468–74.
4. Sakaguchi M, Shimizu N, Yanai T, et al. Hip rotation angle is associated with frontal plane knee joint mechanics during running. Gait Posture 2015;41(2):557–61.
5. Meira EP, Brumitt J. Influence of the hip on patients with patellofemoral pain syndrome: a systematic review. Sports Health 2011;3(5):455–65.
6. Neal BS, Barton CJ, Gallie R, et al. Runners with patellofemoral pain have altered biomechanics which targeted interventions can modify: A systematic review and meta-analysis. Gait Posture 2016;45:69–82.
7. Nakagawa TH, Serrao FV, Maciel CD, et al. Hip and knee kinematics are associated with pain and self-reported functional status in males and females with patellofemoral pain. Int J Sports Med 2013;34(11):997–1002.
8. Noehren B, Hamill J, Davis I. Prospective evidence for a hip etiology in patellofemoral pain. Med Sci Sports Exerc 2013;45(6):1120–4.
9. Souza RB, Powers CM. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J Orthop Sports Phys Ther 2009;39(1):12–9.
10. Willson JD, Davis IS. Lower extremity mechanics of females with and without patellofemoral pain across activities with progressively greater task demands. Clin Biomech (Bristol, Avon) 2008;23(2):203–11.
11. Boling MC, Padua DA, Marshall SW, et al. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am J Sports Med 2009;37(11):2108–16.
12. Powers CM, Chen PY, Reischl SF, et al. Comparison of foot pronation and lower extremity rotation in persons with and without patellofemoral pain. Foot Ankle Int 2002;23(7):634–40.
13. Barton CJ, Levinger P, Webster KE, et al. Walking kinematics in individuals with patellofemoral pain syndrome: a case-control study. Gait Posture 2011;33(2):286–91.
Statement 1.2a.2a. Although impaired hip muscle performance is consistently reported in persons with PFP, evidence of abnormal hip/femur structure in persons with PFP is lacking.
Two separate systematic reviews indicated that persons with PFP exhibit strength deficits in hip extension, abduction and external rotation,1,2 but hip strength and the risk of developing PFP were not associated.3 In fact, hip abduction strength4 and external rotator strength5 were reported to be higher in persons who subsequently developed PFP. This discrepancy might reflect the imprecise relationship between hip strength and hip and knee kinematics.6–11 It is possible that hip weakness develops as a consequence of PFP.
Two bony abnormalities may influence altered hip kinematics in the context of PFP: (1) excessive femoral anteversion and (2) increased femoral neck inclination (ie, coxa valga).7 Although excessive femoral anteversion can contribute to excessive hip rotation during gait,12 excessive femoral anteversion is not apparent in persons with PFP.7,13 In addition, coxa valga can contribute to diminished the lever arm for the gluteus medius.14 Although women with PFP exhibit greater degrees of coxa valga compared with healthy controls,7 the reported difference was quite small (4.4°) and likely of little clinical relevance.
1. Van Cant J, Pineux C, Pitance L, et al. Hip muscle strength and endurance in females with patellofemoral pain: a systematic review with meta-analysis. Int J Sports Phys Ther 2014;9(5):564–82.
2. Prins MR, van der Wurff P. Females with patellofemoral pain syndrome have weak hip muscles: a systematic review. Aust J Physiother 2009;55(1):9–15.
3. Rathleff MS, Rathleff CR, Crossley KM, et al. Is hip strength a risk factor for patellofemoral pain? A systematic review and meta-analysis. Br J Sports Med 2014;48(14):1088.
4. Herbst KA, Barber Foss KD, Fader L, et al. Hip strength is greater in athletes who subsequently develop patellofemoral pain. Am J Sports Med 2015;43(11):2747–52.
5. Boling MC, Padua DA, Marshall SW, et al. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am J Sports Med 2009;37(11):2108–16.
6. Boling M, Padua D. Relationship between hip strength and trunk, hip, and knee kinematics during a jump-landing task in individuals with patellofemoral pain. Int J Sports Phys Ther 2013;8(5):661–9.
7. Souza RB, Powers CM. Predictors of hip internal rotation during running: an evaluation of hip strength and femoral structure in women with and without patellofemoral pain. Am J Sports Med 2009;37(3):579–87.
8. Willson JD, Davis IS. Lower extremity mechanics of females with and without patellofemoral pain across activities with progressively greater task demands. Clin Biomech (Bristol, Avon) 2008;23(2):203–11.
9. Dierks TA, Manal KT, Hamill J, et al. Proximal and distal influences on hip and knee kinematics in runners with patellofemoral pain during a prolonged run. J Orthop Sports Phys Ther 2008;38(8):448–56.
10. Bazett-Jones DM, Cobb SC, Huddleston WE, et al. Effect of patellofemoral pain on strength and mechanics after an exhaustive run. Med Sci Sports Exerc 2013;45(7):1331–9.
11. Cronstrom A, Creaby MW, Nae J, et al. Modifiable factors associated with knee abduction during weight-bearing activities: a systematic review and meta-analysis. Sports Med 2016.
12. O’Sullivan R, Walsh M, Hewart P, et al. Factors associated with internal hip rotation gait in patients with cerebral palsy. J Pediatr Orthop 2006;26(4):537–41.
13. Erkocak OF, Altan E, Altintas M, et al. Lower extremity rotational deformities and patellofemoral alignment parameters in patients with anterior knee pain. Knee Surg Sports Traumatol Arthrosc 2015.
14. Arnold AS, Komattu AV, Delp SL. Internal rotation gait: a compensatory mechanism to restore abduction capacity decreased by bone deformity. Dev Med Child Neurol 1997;39(1):40–4.
Statement 1.2a.3. Excessive rotation of the tibia accompanies subtalar joint pronation, and may be a contributor to patellofemoral dysfunction. While a subset of persons with PFP may exhibit altered foot kinematics and plantar pressures, measures of dynamic foot function are not consistently associated with PFP.
Excessive subtalar joint pronation may result in greater tibia and femur rotation through coupling mechanisms.1,2 A systematic review of 24 case–control studies reported that persons with PFP exhibit tendencies towards excessive and delayed rearfoot eversion during walking and running.3 However, dynamic foot function did not emerge as a risk factor for the development of PFP.4,5 The discrepancy between the cross-sectional and prospective studies may relate to the quantification of pronation (ie, mid-foot vs rearfoot motion), and the variable coupling actions of the mid-foot, rearfoot, tibia and femur among individuals.6 To date, only one study found a correlation between rearfoot eversion and lower extremity kinematics in persons with PFP (hip adduction)7; however, the reported relationship was moderate (r=0.48).
Altered plantar pressures may be found in persons with PFP; however, findings among studies are variable.8–11 A prospective study reported that persons who developed PFP had significantly greater lateral pressure at the rearfoot during walking, suggestive of a less pronated foot.12
1. Tiberio D. The effect of excessive subtalar joint pronation on patellofemoral mechanics: a theoretical model. J Orthop Sports Phys Ther 1987;9(4):160–5.
2. Powers CM. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther 2003;33(11):639–46.
3. Barton CJ, Levinger P, Menz HB, et al. Kinematic gait characteristics associated with patellofemoral pain syndrome: a systematic review. Gait Posture 2009;30(4):405–16.
4. Dowling GJ, Murley GS, Munteanu SE, et al. Dynamic foot function as a risk factor for lower limb overuse injury: a systematic review. J Foot Ankle Res 2014;7(1):53.
5. Noehren B, Hamill J, Davis I. Prospective evidence for a hip etiology in patellofemoral pain. Med Sci Sports Exerc 2013;45(6):1120–4.
6. Reischl SF, Powers CM, Rao S, et al. Relationship between foot pronation and rotation of the tibia and femur during walking. Foot Ankle Int 1999;20(8):513–20.
7. Barton CJ, Levinger P, Crossley KM, et al. The relationship between rearfoot, tibial and hip kinematics in individuals with patellofemoral pain syndrome. Clin Biomech (Bristol, Avon) 2012;27(7):702–5.
8. Willson JD, Ellis ED, Kernozek TW. Plantar loading characteristics during walking in females with and without patellofemoral pain. J Am Podiatr Med Assoc 2015;105(1):1–7.
9. Rathleff MS, Richter C, Brushoj C, et al. Increased medial foot loading during drop jump in subjects with patellofemoral pain. Knee Surg Sports Traumatol Arthrosc 2014;22(10):2301–7.
10. Aliberti S, Costa Mde S, Passaro Ade C, et al. Influence of patellofemoral pain syndrome on plantar pressure in the foot rollover process during gait. Clinics (Sao Paulo) 2011;66(3):367–72.
11. Aliberti S, Costa MS, Passaro AC, et al. Medial contact and smaller plantar loads characterize individuals with patellofemoral pain syndrome during stair descent. Phys Ther Sport 2010;11(1):30–4.
12. Thijs Y, Van Tiggelen D, Roosen P, et al. A prospective study on gait-related intrinsic risk factors for patellofemoral pain. Clin J Sport Med 2007;17(6):437–45.
Statement 1.2a.3a. Persons with PFP exhibit physical impairments at the foot and ankle that are consistent with excessive foot pronation, but these findings are not universal.
Persons with PFP exhibit rearfoot and forefoot varus,1 2 navicular drop,3 4 and calf tightness5; however, this is not a universal finding across all studies.6 Similarly, static measures of foot posture (ie, foot arch height index, foot posture index) are not associated with PFP across all studies. While some authors report differences in foot posture in persons with PFP,4 others do not.7 8 Although there is some indication that foot posture may be associated with certain measures of dynamic foot function,9 there is limited evidence that a pronated foot posture is associated with PFP development.10 In contrast, navicular drop is associated with PFP development.11
Foot and ankle mobility (ie, limited ankle dorsiflexion, increased mid-foot mobility) is associated with 2D measures of knee valgus12 and diminished quality of movement during a lateral stepdown task.13
1. Powers CM, Maffucci R, Hampton S. Rearfoot posture in subjects with patellofemoral pain. J Orthop Sports Phys Ther 1995;22(4):155–60.
2. Levinger P, Gilleard W. An evaluation of the rearfoot posture in individuals with patellofemoral pain syndrome. J Sports Sci Med 2004;3(Yisi 1):8–14.
3. Molgaard C, Rathleff MS, Simonsen O. Patellofemoral pain syndrome and its association with hip, ankle, and foot function in 16- to 18-year-old high school students: a single-blind case-control study. J Am Podiatr Med Assoc 2011;101(3):215–22.
4. Barton CJ, Bonanno D, Levinger P, et al. Foot and ankle characteristics in patellofemoral pain syndrome: a case control and reliability study. J Orthop Sports Phys Ther 2010;40(5):286–96.
5. Piva SR, Goodnite EA, Childs JD. Strength around the hip and flexibility of soft tissues in individuals with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther 2005;35(12):793–801.
6. de Moura Campos Carvalho ESAP, Magalhaes E, Bryk FF, et al. Comparison of isometric ankle strength between females with and without patellofemoral pain syndrome. Int J Sports Phys Ther 2014;9(5):628–34.
7. Lankhorst NE, Bierma-Zeinstra SM, van Middelkoop M. Risk factors for patellofemoral pain syndrome: a systematic review. J Orthop Sports Phys Ther 2012;42(2):81–94.
8. McPoil TG, Warren M, Vicenzino B, et al. Variations in foot posture and mobility between individuals with patellofemoral pain and those in a control group. J Am Podiatr Med Assoc 2011;101(4):289–96.
9. Barton CJ, Levinger P, Crossley KM, et al. Relationships between the Foot Posture Index and foot kinematics during gait in individuals with and without patellofemoral pain syndrome. J Foot Ankle Res 2011;4:10.
10. Neal BS, Griffiths IB, Dowling GJ, et al. Foot posture as a risk factor for lower limb overuse injury: a systematic review and meta-analysis. J Foot Ankle Res 2014;7(1):55.
11. Boling MC, Padua DA, Marshall SW, et al. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am J Sports Med 2009;37(11):2108–16.
12. Wyndow N, De Jong A, Rial K, et al. The relationship of foot and ankle mobility to the frontal plane projection angle in asymptomatic adults. J Foot Ankle Res 2016;9:3.
13. Rabin A, Kozol Z, Moran U, et al. Factors associated with visually assessed quality of movement during a lateral step-down test among individuals with patellofemoral pain. J Orthop Sports Phys Ther 2014;44(12):937–46.
Statement 1.2b. Persons with PFP exhibit differences in tibiofemoral kinetics in all three planes of motion compared with pain-free individuals; however, there are inconsistencies among studies.
Altered tibiofemoral joint kinetics in the sagittal plane can influence the magnitude of the PFJRF. Consistent with the finding of lower PFJRFs in this population, persons with PFP exhibit lower knee extensor moments during walking,1–3 stair climbing1,4,5 and running.1 Other studies report no differences in knee extensor moments between persons with PFP and healthy controls during walking,6 stair climbing7 and running.6,8 Persons with PFP exhibit higher muscle co-contraction at the knee (quadriceps-hamstrings), which may lower the net joint moments at the knee.6
With respect to knee kinetics in the frontal plane, persons with PFP have elevated knee abductor moments during walking3,8 and stair ambulation,9 as well as higher knee abduction impulses during running.10 In the transverse plane, persons with PFP exhibit increased knee external rotator moments during loading response, when compared with age-matched and sex-matched controls.3
Increased knee abduction moments during a drop jump task can predict PFP development in young female athletes.11,12 Furthermore, the knee abduction impulse can predict PFP in runners.10 The kinetic tendencies displayed by persons with PFP may be accompanied by abnormal kinematics described in statement 1.2a.
1. Chen YJ, Powers CM. Comparison of three-dimensional patellofemoral joint reaction forces in persons with and without patellofemoral pain. J Appl Biomech 2014;30(4):493–500.
2. Heino BJ, Powers CM. Patellofemoral stress during walking in persons with and without patellofemoral pain. Med Sci Sports Exerc 2002;34(10):1582–93.
3. Paoloni M, Mangone M, Fratocchi G, et al. Kinematic and kinetic features of normal level walking in patellofemoral pain syndrome: more than a sagittal plane alteration. J Biomech 2010;43(9):1794–8.
4. Brechter JH, Powers CM. Patellofemoral joint stress during stair ascent and descent in persons with and without patellofemoral pain. Gait Posture 2002;16(2):115–23.
5. Salsich GB, Brechter JH, Powers CM. Lower extremity kinetics during stair ambulation in patients with and without patellofemoral pain. Clin Biomech (Bristol, Avon) 2001;16(10):906–12.
6. Besier TF, Fredericson M, Gold GE, et al. Knee muscle forces during walking and running in patellofemoral pain patients and pain-free controls. J Biomech 2009;42(7):898–905.
7. Besier TF, Pal S, Draper CE, et al. The role of cartilage stress in patellofemoral pain. Med Sci Sports Exerc 2015;47(11):2416–2.
8. Wirtz AD, Willson JD, Kernozek TW, et al. Patellofemoral joint stress during running in females with and without patellofemoral pain. Knee 2012;19(5):703–08.
9. Aminaka N, Pietrosimone BG, Armstrong CW, et al. Patellofemoral pain syndrome alters neuromuscular control and kinetics during stair ambulation. J Electromyogr Kinesiol 2011;21(4):645–51.
10. Stefanyshyn DJ, Stergiou P, Lun VM, et al. Knee angular impulse as a predictor of patellofemoral pain in runners. Am J Sports Med 2006;34(11):1844–51.
11. Myer GD, Ford KR, Barber Foss KD, et al. The incidence and potential pathomechanics of patellofemoral pain in female athletes. Clin Biomech (Bristol, Avon) 2010;25(7):700–7.
12. Myer GD, Ford KR, Di Stasi SL, et al. High knee abduction moments are common risk factors for patellofemoral pain (PFP) and anterior cruciate ligament (ACL) injury in girls: is PFP itself a predictor for subsequent ACL injury? Br J Sports Med 2015;49(2):118–22.
Statement 1.2b.1. Persons with PFP exhibit differences in ground reaction forces compared with pain-free individuals, but study results are inconsistent.
When compared with healthy controls, persons with PFP have lower ground reaction forces and loading rates during free and fast walking,1 higher than normal loading rates during stair ambulation,2 and no differences in vertical force loading rate during running.3 Although higher ground reaction and loading rates during stair ambulation were associated with pain and functional status,4 the influence of vertical force loading rate on patellofemoral joint loading has not been established.
1. Powers CM, Heino JG, Rao S, et al. The influence of patellofemoral pain on lower limb loading during gait. Clin Biomech (Bristol, Avon) 1999;14(10):722–8.
2. de Oliveira Silva D, Briani R, Pazzinatto M, et al. Vertical Ground Reaction Forces are Associated with Pain and Self-Reported Functional Status in Recreational Athletes with Patellofemoral Pain. J Appl Biomech 2015;31(6):409–14.
3. Esculier JF, Roy JS, Bouyer LJ. Lower limb control and strength in runners with and without patellofemoral pain syndrome. Gait Posture 2015;41(3):813–9.
4. Silva Dde O, Briani RV, Pazzinatto MF, et al. Reduced knee flexion is a possible cause of increased loading rates in individuals with patellofemoral pain. Clin Biomech (Bristol, Avon) 2015;30(9):971–5.
Statement 1.2b.2. Persons with PFP exhibit differences in trunk kinematics compared with pain-free individuals, but findings are not consistent.
Sagittal plane trunk posture has the potential to influence the knee extensor moment and therefore the PFJRF. For example, running with a more upright trunk posture is associated with higher knee extensor moments, PFJRFs and higher PFJ stress when compared with running with a more flexed trunk.1 Running-induced fatigue can result in a compensatory forward trunk lean, which was hypothesised to minimise PFJ loading and pain.2 In contrast to running, however, persons with PFP do not exhibit altered sagittal plane trunk kinematics during stair descent.3
Persons with PFP also exhibit altered trunk kinematics in the frontal plane. Specifically, persons with PFP exhibit an ipsilateral trunk lean during single limb tasks (ie, single leg squatting, jumping/landing).4–6 An ipsilateral trunk lean would shift the centre of mass of the body towards the stance limb, thereby increasing the potential for a knee abductor moment.7
1. Teng HL, Powers CM. Sagittal plane trunk posture influences patellofemoral joint stress during running. J Orthop Sports Phys Ther 2014;44(10):785–92.
2. Bazett-Jones DM, Cobb SC, Huddleston WE, et al. Effect of patellofemoral pain on strength and mechanics after an exhaustive run. Med Sci Sports Exerc 2013;45(7):1331–9.
3. Schwane BG, Goerger BM, Goto S, et al. Trunk and lower extremity kinematics during stair descent in women with or without patellofemoral pain. J Athl Train 2015;50(7):704–12.
4. dos Reis AC, Correa JC, Bley AS, et al. Kinematic and kinetic analysis of the single-leg triple hop test in women with and without patellofemoral pain. J Orthop Sports Phys Ther 2015;45(10):799–807.
5. Nakagawa TH, Maciel CD, Serrao FV. Trunk biomechanics and its association with hip and knee kinematics in patients with and without patellofemoral pain. Man Ther 2015;20(1):189–93.
6. Boling M, Padua D. Relationship between hip strength and trunk, hip, and knee kinematics during a jump-landing task in individuals with patellofemoral pain. Int J Sports Phys Ther 2013;8(5):661–9.
7. Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther 2010;40(2):42–51.
Statement 1.2b.2a. Impaired hip and trunk muscle performance may contribute to altered trunk kinematics in persons with PFP; however, there is inconsistency among studies.
Abnormal motions/postures of the trunk in the frontal and sagittal planes may be compensatory strategies related to diminished hip strength.1 Runners with hip extensor weakness tend to adopt a more upright trunk posture to reduce the demand on the hip extensors, while runners with greater hip extensor strength run with a more forward trunk.2 In addition, ipsilateral trunk lean in persons with PFP has been reported to be a compensation for stance limb hip abductor weakness.3
Persons with PFP have been reported to exhibit reduced trunk strength4; however, this impairment has not been shown to be associated with faulty trunk kinematics. Nonetheless trunk strength has been shown to be correlated with knee abduction during weightbearing,5 as well as with self-reported function in persons with PFP.6
1. Popovich JM, Jr, Kulig K. Lumbopelvic landing kinematics and EMG in women with contrasting hip strength. Med Sci Sports Exerc 2012;44(1):146–53.
2. Teng HL, Powers CM. Individuals with weak hip extensors exhibit an upright trunk posture and greater reliance on the knee extensors during running: Implications for knee injury. J Athl Train.
3. Boling M, Padua D. Relationship between hip strength and trunk, hip, and knee kinematics during a jump-landing task in individuals with patellofemoral pain. Int J Sports Phys Ther 2013;8(5):661–9.
4. Cowan SM, Crossley KM, Bennell KL. Altered hip and trunk muscle function in individuals with patellofemoral pain. Br J Sports Med 2009;43(8):584–8.
5. Cronstrom A, Creaby MW, Nae J, et al. Modifiable Factors Associated with Knee Abduction During Weight-Bearing Activities: A Systematic Review and Meta-Analysis. Sports Med 2016.
6. Almeida GP, Carvalho ESAP, Franca FJ, et al. Does anterior knee pain severity and function relate to the frontal plane projection angle and trunk and hip strength in women with patellofemoral pain? J Bodyw Mov Ther 2015;19(3):558–64.
Statement 1.2c. Persons with PFP exhibit tightness of the quadriceps and hamstring muscle groups. However, prospective studies linking muscle tightness to the development of PFP are inconsistent.
Shorter hamstring length was associated with greater PFJRFs and stress during squatting in healthy persons.1 Although persons with PFP have shorter hamstring muscles compared with asymptomatic controls,2–4 hamstring tightness was not a predictor of PFP development in a prospective study.5
Tightness of the quadriceps muscles can increase PFJRFs. Several studies report that persons with PFP exhibit tightness of the quadriceps muscles compared with those without PF,3,4,6,7 and a shortened quadriceps muscle has been shown to be a predictor of PFP development.5
1. Whyte EF, Moran K, Shortt CP, et al. The influence of reduced hamstring length on patellofemoral joint stress during squatting in healthy male adults. Gait Posture 2010;31(1):47–51.
2. White LC, Dolphin P, Dixon J. Hamstring length in patellofemoral pain syndrome. Physiotherapy 2009;95(1):24–8.
3. Smith AD, Stroud L, McQueen C. Flexibility and anterior knee pain in adolescent elite figure skaters. J Pediatr Orthop 1991;11(1):77–82.
4. Piva SR, Goodnite EA, Childs JD. Strength around the hip and flexibility of soft tissues in individuals with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther 2005;35(12):793–801.
5. Witvrouw E, Lysens R, Bellemans J, et al. Intrinsic risk factors for the development of anterior knee pain in an athletic population. A 2 year prospective study. Am J Sports Med 2000;28(4):480–9.
All6. Kibler W. Strength and flexibility findings in anterior knee pain syndrome in athletes. Am J Sports Med 1987;15(410):49.
7. Duffey MJ, Martin DF, Cannon DW, et al. Etiologic factors associated with anterior knee pain in distance runners. Med Sci Sports Exerc 2000;32(11):1825–32.
Statement 1.3. Reduced patellar cartilage thickness can contribute to elevated patellofemoral joint loading.
Reduced patellar cartilage thickness has been reported to be associated with higher patellar bone strain1 and diminished deformational behaviour of patellar cartilage.2 Reduced cartilage thickness also has been shown to result in elevated cartilage stress for a given load.3 As such, decreased patellar cartilage thickness may contribute to a vicious cycle of patellofemoral joint pathology (reduced cartilage thickness → elevated cartilage stress → further reduction in cartilage thickness → patellofemoral osteoarthritis (PFJOA)).2
It has been reported that persons with elevated patellofemoral joint loading exhibit decreased thickness and diminished deformational behaviour of patellar cartilage when compared with age-matched and activity-matched controls.4,5 However, the finding of decreased cartilage thickness in this population is not consistent across studies.6
1. Ho KY, Keyak JH, Powers CM. Comparison of patella bone strain between females with and without patellofemoral pain: A finite element analysis study. J Biomech 2014;47(1):230–36.
2. Farrokhi S, Colletti PM, Powers CM. Differences in patellar cartilage thickness, transverse relaxation time, and deformational behavior: a comparison of young women with and without patellofemoral pain. Am J Sports Med 2011;39(2):384–91.
3. Li G, Lopez O, Rubash H. Variability of a three-dimensional finite element model constructed using magnetic resonance images of a knee for joint contact stress analysis. J Biomech Eng 2001;123(4):341–6.
4. Ho KY, Keyak JH, Powers CM. Comparison of patella bone strain between females with and without patellofemoral pain: A finite element analysis study. J Biomech 2014;47(1):230–36.
5. Farrokhi S, Colletti PM, Powers CM. Differences in patellar cartilage thickness, transverse relaxation time, and deformational behavior: a comparison of young women with and without patellofemoral pain. Am J Sports Med 2011;39(2):384–91.
6. Draper CE, Besier TF, Gold GE, et al. Is cartilage thickness different in young subjects with and without patellofemoral pain? Osteoarthritis Cartilage 2006;14(9):931–7.
Acknowledgments
The authors would like to acknowledge the attendees at the 2015 consensus meeting in Manchester, UK . All attendees contributed to the discussion of the pathways in the pathomechanical framework.
Footnotes
Funding The British Journal of Sports Medicine provided £2000 to support the 4th International Patellofemoral Pain Research Retreat, in Manchester, UK.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.