Article Text

Abstract
Aim To investigate pain, activities of daily living (ADL) function, sport function, quality of life and satisfaction at different time points after hip arthroscopy in patients with femoroacetabular impingement (FAI).
Design Systematic review with meta-analysis. Weighted mean differences between preoperative and postoperative outcomes were calculated and used for meta-analysis.
Data sources EMBASE, MEDLINE, SportsDiscus, CINAHL, Cochrane Library, and PEDro.
Eligibility criteria for selecting studies Studies that evaluated hip pain, ADL function, sport function and quality of life before and after hip arthroscopy and postoperative satisfaction in patients with symptomatic FAI.
Results Twenty-six studies (22 case series, 3 cohort studies, 1 randomised controlled trial (RCT)) were included in the systematic review and 19 in the meta-analysis. Clinically relevant pain and ADL function improvements were first reported between 3 and 6 months, and sport function improvements between 6 months and 1 year after surgery. It is not clear when quality of life improvements were first achieved. On average, residual mild pain and ADL and sport function scores lower than their healthy counterparts were reported by patients following surgery. Postoperative patient satisfaction ranged from 68% to 100%.
Conclusions On average, patients reported earlier pain and ADL function improvements, and slower sport function improvements after hip arthroscopy for FAI. However, average scores from patients indicate residual mild hip pain and/or hip function lower than their healthy counterparts after surgery. Owing to the current low level of evidence, future RCTs and cohort studies should investigate the effectiveness of hip arthroscopy in patients with FAI.
Trial registration number CRD42015019649.
- Hip
- Arthroscopic surgery
- Functional
- Quality of life
Statistics from Altmetric.com
Introduction
Patients with symptomatic femoroacetabular impingement (FAI) experience hip pain, functional limitations during activities of daily living (ADL) and sport and reduced quality of life.1 In addition, they are exposed to an increased risk of developing hip osteoarthritis (OA) and progressing to total hip arthroplasty (THA).2 Patients with FAI may be offered hip preservation surgery, either arthroscopically or open, to decrease hip pain, improve their functional performance and, in a long-term perspective, to possibly prevent or postpone the development of hip OA.3
In the past decade, the number of hip arthroscopies performed in the USA has continuously increased.4 Mostly low level of evidence case series with broad patient inclusion criteria indicate that the arthroscopic treatment of intra-articular pathologies and correction of bony deformities related to FAI seem to reduce hip pain and improve hip function, with the majority of patients being satisfied with the surgical outcome.5 However, to the best of our knowledge, no published study has compared hip arthroscopy with other non-surgical interventions to establish the true effectiveness of hip arthroscopy for the management of FAI.6 ,7 Currently, several matched cohort studies and randomised controlled trials (RCT), aimed at comparing hip arthroscopy with other interventions, are registered in international clinical research databases. Therefore, the existing knowledge on the effectiveness of hip arthroscopy in patients with FAI may be expanded in the coming years.
Some systematic reviews have already summarised the current knowledge on patient-reported outcomes after hip arthroscopy in patients with FAI.5 ,8–12 The large majority of studies included in previous systematic reviews reported hip arthroscopy outcomes with composite scores (eg, Harris Hip Score and Non-Arthritic Hip Scale).5 ,8–12 However, such scores do not enable evaluation of changes in specific domains, such as hip pain, hip function during ADL and sport, quality of life and satisfaction. In contrast, other scores used to evaluate hip arthroscopy outcome, such as the Hip Outcome Score (HOS)13 and the Copenhagen Hip and Groin Outcome Score (HAGOS),14 quantify improvements in specific domains by means of outcome subscores. Additionally, no systematic review to date has reported domain-specific outcomes at different time points after hip arthroscopy. Despite the methodological limitations of the available studies, knowledge about the timely recovery of the aforementioned specific domains is of particular interest for hip surgeons and therapists in order to provide specific and realistic postoperative expectations to patients with FAI undergoing hip arthroscopy.
The aim of this systematic review was to investigate hip pain, ADL function, sport function, quality of life and satisfaction reported by patients with FAI at different time points before and after hip arthroscopy.
Methods
Study selection
This systematic review was performed in accordance with the PRISMA statement.15 The study protocol was registered at the “International prospective register of systematic reviews” (PROSPERO) database (CRD42015019649). Electronic searches were performed by two authors (SK and ML-C) in the EMBASE, MEDLINE, SportsDiscus, CINAHL, Cochrane Library and PEDro databases to identify studies published before 20 September 2015. Key search terms were combined using three main filters: (1) Femoroacetabular/Hip, (2) Impingement and (3) Arthroscopy, and applying relevant MeSH terms. The specific search terms used for the different databases are shown in online supplementary table S1. Systematic reviews were additionally screened to detect eligible studies that were not identified by the electronic search. To be included in the systematic review, the studies had to satisfy the following criteria:
Supplementary tables
– Study design: Studies had to be RCTs, cohort studies, case–control studies or case series including >10 cases.
– Patients: Patients had to be >16 years old with a diagnosis of symptomatic FAI according to pain history, clinical and radiological evaluation. Patients without a diagnosis of FAI but treated with hip arthroscopy, patients with hip dysplasia, slipped capital femoral epiphysis or the Legg–Calve–Perthes disease, patients with previous hip arthroscopic or open surgery (revision surgery) and patients undergoing periacetabular osteotomy were all excluded.
– Intervention: Patients had to be treated with hip arthroscopic surgery, and the surgical procedure had to be described. Studies with combined arthroscopic and open surgical techniques were excluded.
– Outcomes: Preoperative and postoperative hip pain and/or hip function during ADL and sport and/or quality of life and/or postoperative satisfaction absolute scores had to be reported. Studies with composite scores were enrolled only if authors also separately reported the single subscores.
In order to assist the reviewers to evaluate the inclusion criteria, the following PICO (Population, Intervention, Comparison, Outcome) question16 was formulated: “How are the domains pain, ADL function, sport function, quality of life and satisfaction after surgery compared to before surgery, in patients with FAI who underwent primary hip arthroscopy?” No restrictions were imposed for language, publication date and publication status. All studies resulting from the electronic search were imported into a systematic review software (Covidence, Melbourne, Victoria, Australia) that automatically removed duplicates. SK and ML-C first independently screened titles and abstracts and then assessed study eligibility by reading the full text of the studies. Disagreement was resolved by consensus.
Methodological quality assessment
The methodological quality of the studies was independently assessed by two authors (SK and ML-C) using the tool developed by Yang et al,17 with disagreement resolved by consensus. This tool evaluates (1) study aims and design, (2) description of the study treatment protocol, (3) description of the study methods and therapeutic/side effects, and (4) study conduction. Each criterion was rated either as 1 (if the criterion was met) or 0 (if criterion was not met). The total score was the sum of all satisfied criteria and ranged from 0 to 13 (13=highest methodological quality).17 Studies with total scores <5 were considered to be of low methodological quality, 5–8 with moderate methodological quality and >8 with high methodological quality.17 ,18
Data extraction
Data were independently extracted by SK and ML-C with the exception of surgical procedure data, which were extracted by SK and BL. Disagreement was resolved by consensus. The extracted data included the country where the study was performed, study design, number of patients at recruitment and at final follow-up, number of patients who underwent revision surgery or THA, patient characteristics (age, gender), criteria for the diagnosis of FAI, included FAI types, presence and degree of coexisting hip joint disease, and description of the surgical procedure. Preoperative and postoperative hip pain, ADL function, sport function, quality of life scores and postoperative satisfaction scores were extracted. Postoperative scores were grouped by follow-up times: <3 months, 3 to <6 months, 6 months to <1 year, 1 to <2 years, 2 to <3 years, 3 to <4 years, 4 to <5 years and ≥5 years. The scores, which were used to assess hip arthroscopy outcomes in the included studies, are listed in table 1 grouped by domain. All scores were converted to a 100-point scale, where 100 indicated the best possible score, except for visual analogue scale (VAS) and numeric rating scale (NRS) where 0 indicated no pain.
Domain-specific outcome scores
Statistical analysis
Percentage agreement and Cohen k statistics (mean and 95% CI) were calculated to provide an estimate of the level of agreement between raters when scoring the methodological quality of the included studies. Weighted mean scores were calculated for all scores at the different follow-up times adjusted to the number of patients. Weighted mean differences (WMD) were calculated for pain, ADL function, sport function and quality of life at the different follow-up times by subtracting the preoperative to the postoperative scores and adjusting to the number of patients. Positive WMD indicated a score improvement. The meta-analysis of WMD was performed with random effects meta-analysis. Hedges’ g was applied adjusting for differences in sample size. Between-study variance and heterogeneity among studies were calculated.20 ,21 Between-study variance was evaluated using χ2 tests and τ2. The degree of heterogeneity was interpreted as follows: I2 <30% ‘might not be important’, 30–75% ‘moderate’ and >75% ‘considerable’.20 Sensitivity analyses were performed analysing the WMDs of studies with high methodological quality only. Minimal important changes (MIC), which were calculated by previous studies in different patient populations (pain)22 and specifically in young hip patients (ADL function, sport function, quality of life),23 ,24 were used to evaluate the clinical relevance of the calculated WMD. MIC was 30 points for pain assessed with VAS and NRS;22 9 points for pain and ADL function measured with HAGOS, HOOS, and HOS ADL;23 ,24 10 points for sport function assessed with HAGOS and HOOS;23 6 points for sport function measured with HOS sport;24 and 11 points for hip-related quality of life measured with HAGOS and HOOS.23 The significance of WMD was defined by the lower bound of the WMD 95% CI being higher than the respective MIC. The statistical analyses were performed with Stata 13 (StataCorp, College Station, Texas, USA). Significance level was set at p<0.05.
Results
Study selection and methodological quality
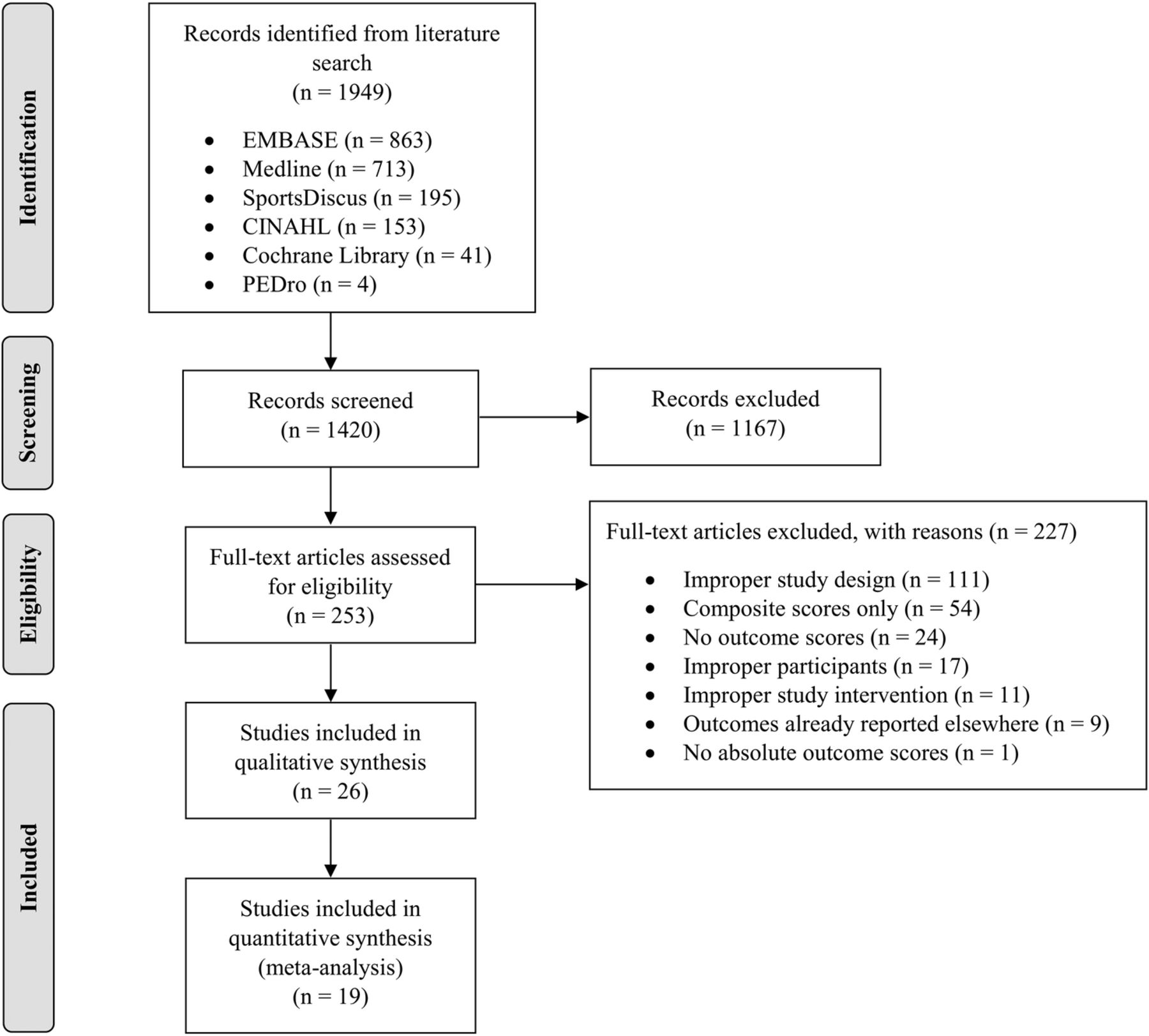
A total of 1949 studies were identified by the electronic search (figure 1). After duplicate removal and title and abstract screening, 253 full-text articles were evaluated for eligibility, of which 26 were included in the systematic review. A total of 19 studies reporting preoperative and postoperative pain and/or ADL function and/or sport function and/or quality of life scores were included into the meta-analysis. The remaining seven studies only reported postoperative satisfaction scores. These studies could only be qualitatively evaluated. The methodological quality of the single studies is reported in online supplementary table S2. Inter-rater agreement for methodological quality of the studies was 83% (Cohen's k: 0.34 (0.19 to 0.50)). Some studies reported scores of patient subgroups already included in previous studies. In these cases, studies with the highest number of patients and with the longest follow-up were used for analyses.25–28

Flow chart of the study selection process.
Study characteristics
Individual study characteristics are presented in table 2. The 19 studies considered for meta-analysis (15 case series, 3 cohort studies, 1 RCT) included 2322 patients (42% women) with a mean±SD age of 36±8 years (range: 18–57). The 3 cohort studies and 1 RCT considered for meta-analysis compared outcomes between 2 groups of patients who underwent different surgical techniques. A total of 175 patients (7%) had revision surgery or THA, and 319 patients (14%) were lost at follow-up. The 7 studies considered for the qualitative analysis (7 case series) included 494 patients (29% women) with a mean±SD age of 37±14 years (range: 22–65). A total of 25 patients (5%) had revision surgery or THA, and 8 patients (2%) were lost at follow-up. The criteria for symptomatic FAI diagnosis generally included (i) hip pain and functional limitations, (ii) physical examinations and (iii) imaging (ie, radiographs, magnetic resonance images and/or CT scans) (see online supplementary table S3). A total of 19 studies included patients with all FAI types, 3 studies patients with cam FAI only, 2 studies patients with cam and mixed FAI, and 2 studies patients with pincer and mixed FAI. Patients presenting with different grades of hip articular cartilage lesions according to preoperative and/or intraoperative evaluations were included. Acetabulum labral lesions were addressed with labrum debridement or repair, articular cartilage lesions with chondroplasty or microfracture, and femoral and acetabular bony deformities with osteoplasty.
Study characteristics
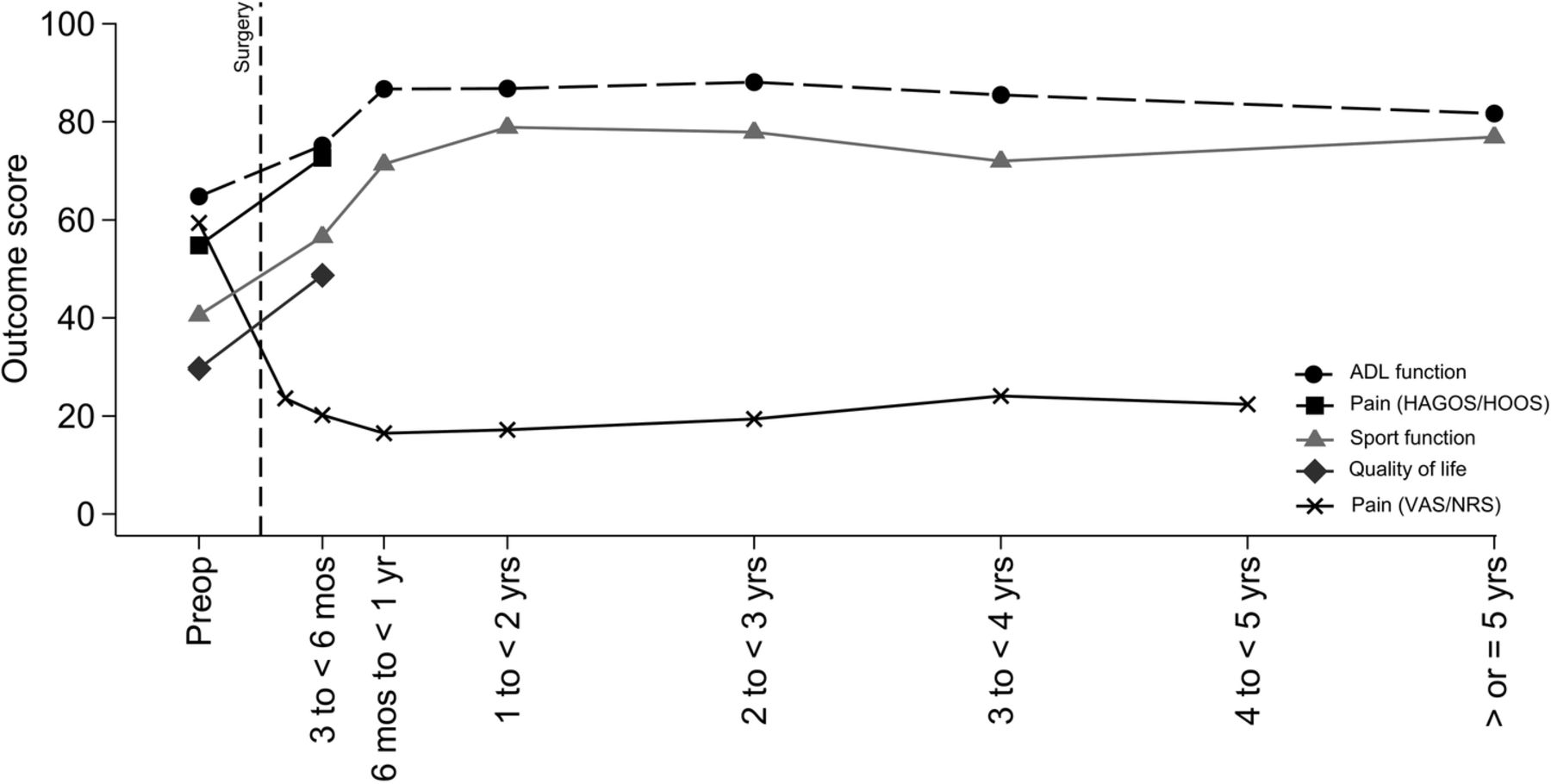
Preoperative and postoperative absolute scores for pain, ADL function, sport function and quality of life are reported in table 3 and postoperative satisfaction scores in online supplementary table S4. Preoperative and postoperative weighted mean scores are reported in figure 2.
Hip pain, ADL function, sport function and quality of life preoperative and postoperative scores

{kind=link}
{kind=link}
Hip pain, ADL function, sport function and quality of life weighted mean scores. ADL, activities of daily living; HAGOS, Copenhagen Hip and Groin Outcome Score; HOOS, Hip Dysfunction and Osteoarthritis Outcome Score; VAS, visual analogue scale; NRS, numeric rating scale.
Quantitative analysis
Pain
Pain WMD assessed using VAS was significantly larger than the respective MIC at 6 months to <1 year, 2 to <3 years and 4 to <5 years follow-ups, while pain WMD assessed using HAGOS/HOOS questionnaires was significantly larger than the respective MIC at 3 to <6 months follow-up (table 4). Between-study variance and moderate to considerable heterogeneity (I2: 56–97) was observed at all follow-ups, except at 4 to <5 years if pain was assessed using VAS and 3 to <6 months if pain was assessed using HAGOS/HOOS questionnaires. Following sensitivity analysis, no between-study variance was observed and heterogeneity was small to moderate (I2: 0–38). The sensitivity analysis confirmed that pain WMD assessed using a VAS was significantly larger than the respective MIC at 6 months to <1 year and 2 to <3 years follow-ups (1 single study), and pain WMD assessed using HAGOS/HOOS questionnaires was significantly larger than the respective MIC at 3 to <6 months follow-up (1 single study).
Hip pain, ADL function, sport function and quality of life outcomes meta-analysis and sensitivity analysis
ADL function
ADL function WMD was significantly larger than the respective MIC at 3 to <6 months, 6 months to <1 year (1 single study), 1 to <2 years and 2 to <3 years follow-ups, but not at 3 to <4 years and ≥5 years follow-ups (table 4). Between-study variance and moderate to considerable heterogeneity (I2: 64–85) were observed from 1 to <2 years to 3 to <4 years follow-ups. Following sensitivity analysis, no between-study variance was observed and heterogeneity was small to moderate (I2: 0–30). In addition, ADL function WMD was significantly larger than the respective MIC at 3 to <6 months (1 single study), 6 months to <1 year (1 single study), 1 to <2 years and 2 to <3 years follow-ups.
Sport function
Sport function WMD was significantly larger than the respective MIC at 3 to <6 months, 6 months to <1-year (one single study), 1 to <2 years, 2 to <3 years, 3 to <4 years (one single study) and ≥5 years follow-ups (one single study) (table 4). Small to considerable heterogeneity were overall observed (I2: 0–93) and between-study variance was significant at 2 to <3 years follow-up. Following sensitivity analysis, sport function WMD was significantly larger than the respective MIC at 6 months to <1 year (1 single study), 1 to <2 years and 2 to <3 years follow-ups. Small to considerable heterogeneity were overall observed (I2: 23–80), and significant between-study variance was observed at 2 to <3 years follow-up.
Quality of life
Only 2 studies evaluated quality of life and only at 3 to <6 months follow-up. Quality of life WMD was significantly larger than the respective MIC at 3 to <6 months follow-up (table 4). No between-study variance and heterogeneity were observed. Following sensitivity analysis, clinically relevant quality of life improvement was not significant at 3 to <6 months follow-up (1 single study).
Qualitative analysis
Satisfaction
Patient satisfaction ranged from 68% to 100% when patients were asked if they were satisfied or dissatisfied with the hip arthroscopy outcome. Patient satisfaction ranged from 71 to 100 points when asked to indicate their satisfaction level either on a 0–100 or 1–10 scale. No clear pattern for increase or decrease in satisfaction scores was observed from <3 months after surgery to more than 5 years after surgery.
Discussion
A total of 26 studies, predominantly reporting low level of evidence (22 case series, 3 cohort studies, 1 RCT), were included in the systematic review, which evaluated hip pain, ADL function, sport function, quality of life and satisfaction at different time points after hip arthroscopy in patients with FAI. The methodological quality of the included studies was moderate to high. Hip pain, ADL function and sport function improved after hip arthroscopy compared with preoperatively. The first clinically relevant hip pain decrease was observed at 3 to <6 months after surgery according to disease-specific questionnaires pain subscores, but at 6 months to <1 year after surgery according to generic pain scales. The first clinically relevant ADL and sport function improvements were observed at 3 to <6 months and 6 months to <1 year after surgery, respectively. Pain, ADL and sport function improvements were evident up to 2 to <3 years after surgery.
To the best of our knowledge, this is the first study investigating patient-reported domain-specific outcomes at different follow-up time points after hip arthroscopy in patients with FAI. This systematic review was performed using a reproducible search strategy and a validated tool for methodological quality evaluation. PRISMA guidelines were followed, with two reviewers involved during study and data selection. WMD’s between preoperative and postoperative outcomes were included in the meta-analysis using MIC as cut-offs when evaluating the clinical relevance of the observed changes.13 This systematic review is limited by the generally low level of evidence of all included studies. Accordingly, our results need to be interpreted with caution. Since hip arthroscopy was not compared to an alternative treatment for FAI (eg, non-surgical treatment or sham surgery), our results are subjected to non-specific, placebo or natural history effects. In addition, large between- and within-study variability in patient inclusion criteria (eg, age, grade of articular cartilage damage) and surgical techniques (eg, acetabular labrum and cartilage treatment) were observed. Nevertheless, all the included studies evaluated patients who underwent hip arthroscopy for the treatment of symptomatic FAI. Last, most of the outcomes presented at the different follow-ups did not include the data of patients who underwent revision surgery or THA. Accordingly, this may have potentially underestimated pain and overestimated ADL and sport function as well as quality of life and satisfaction of patients at follow-ups. Hence, the results of this review should be interpreted also considering the reported rates of revision surgery and THA conversion (7% in the 26 studies), and that 12% of the patients were lost to follow-up.
The strongest and most consistent findings from our sensitivity analysis indicated that the first clinically relevant pain reduction was achieved between 3 and <6 months after surgery according to studies that assessed pain subscores using disease-specific questionnaires (ie, HAGOS pain and HOOS pain). In contrast, the first clinically significant pain reduction using general unidimensional pain scales (ie, VAS and NRS) was observed between 6 months and <1 year after surgery. Disease-specific questionnaires were developed in order to assess pain frequency and intensity under standard conditions and time intervals. In our meta-analysis, disease-specific questionnaires were used to evaluate pain by only 2 studies and at a single time point (3 to <6 months), while general unidimensional scales were otherwise used. Disease-specific questionnaires are generally preferred to unidimensional scales to evaluate outcomes following hip arthroscopy for FAI.5 ,8–12 Nevertheless, studies that used disease-specific questionnaires to assess pain at follow-ups longer than 6 months could not be included in our meta-analysis, since they provided composite scores. In contrast, general unidimensional scales only allow measurement of pain intensity22 under conditions and time intervals arbitrarily defined by the investigators. As an example, some studies might investigate pain at rest during the past 24 hours, while others might ask about pain during activity over the past month. This may lead to large variability of pain levels, and it reduces the ability of general unidimensional scales to detect significant pain changes when they actually occur. For these reasons, we decided to interpret the first clinically relevant pain decrease according to disease-specific questionnaire pain subscores, that is, between 3 and <6 months, even if they were used by only 2 studies included in the meta-analysis.
Of note, some pain (on average around 20 points on a 0–100 scale, where 0 points correspond to no pain at all) was reported by patients after hip arthroscopy until the last available follow-up (4 to <5 years). This suggests that a number of patients might present with residual pain after hip arthroscopy. The origin of postoperative residual pain may be intra-articular (eg, scar tissue, remaining impingement problems, cartilage lesions), extra-articular (eg, muscles, other soft tissues) or a combination of these. Persisting muscle strength impairments after surgery have been demonstrated in patients with FAI,51 ,52 and hip muscle imbalance has been linked to groin pain in some athletic populations.53 Hence, residual pain could be related to persistent postoperative hip muscle impairments in patients with FAI. This relation between hip pain and muscle function after hip arthroscopy is worth to be investigated by future studies.
Improvements in ADL function were smaller (range: 10–24 points) compared to those observed for sport function (range: 19–41 points). This might be related to the relatively high ADL scores reported preoperatively,30 ,38 reflecting less difficulties with ADL than during sport activities. There appears to be a larger window for improvement in sport than ADL function following surgery. ADL, sport function and quality of life all showed the first clinical relevant improvement between 3 and <6 months after surgery, if all the included studies were considered. Of note, however, high-quality studies only confirmed these results for ADL function. In contrast, the first clinically relevant improvement for sport function could be only confirmed between 6 months and 1 year after surgery, and quality of life improvement could not be confirmed at any later follow-up. The slow recovery of sport function may be related to the failure of increasing the quality of life of patients early after surgery. Indeed, it has been reported that the ability to return to sport is—together with pain reduction—the main postoperative expectation of patients with FAI.54 Therefore, the inability of patients to regain their sport function in the first months after surgery may substantially and negatively influence their early postoperative quality of life.
Our analyses showed that improvements in ADL and sport function are seen at all time points up to 2 to <3 years after hip arthroscopy based on high-quality studies (table 4). Only one study of moderate quality showed clinically relevant sport function improvements compared with preoperatively at >5 years after surgery.27 These results need, however, to be confirmed by high-quality studies. Regardless of follow-up time, a considerable number of studies did not report postoperative hip function scores comparable to healthy controls, neither during ADL (<90 vs 99–100, respectively) nor during sport (<80 vs 98–100, respectively) (figure 2).23 These findings are in line with those reported by patients with hip dysplasia, who also underwent hip preservation surgery.55
The dissatisfaction rates reported by patients after hip arthroscopy ranged between 0% and 32%. This dissatisfaction rate corresponds with those reported by previous studies.56 The rate of dissatisfaction may, at least in part, be explained by residual hip pain and/or impaired hip function during ADL and sport reported, on average, after surgery. In addition, the fact that patients with progressed hip joint degeneration (eg, Tönnis grade ≥2) at the time of hip arthroscopy were included in the evaluated studies may explain the residual pain and lower hip function compared with healthy counterparts reported by a number of patients after surgery. Indeed, limited articular joint space at the time of hip arthroscopy, indicating progressed hip OA, has been associated with postoperative low ADL and sport function outcomes, high THA conversion rate and low satisfaction of patients at 2 to <3 years,42 3 to <4 years44 and ≥5 years follow-ups.27 Future high-quality studies are needed to investigate hip pain, ADL function and sport function improvements after hip arthroscopy in patients with FAI at follow-ups longer than 3 years. In addition, future research should investigate the effectiveness of hip arthroscopy in patients with FAI in improving pain, ADL and sport function in RCTs or cohort studies, which compare hip arthroscopy to non-surgical treatments for the management of symptomatic FAI.
Conclusion
Studies with low level of evidence (mostly case series) and broad inclusion criteria evaluated hip pain, ADL function, sport function, quality of life and satisfaction at different time points after hip arthroscopy in patients with FAI. On average, patients with symptomatic FAI experience hip pain reduction and ADL function improvement at 3 to <6 months after hip arthroscopy, and improvements in sport function at 6 months to <1 year postoperatively. Compared with preoperatively, reduced hip pain and improved ADL and sport function seem to be maintained up to 2 to <3 years after hip arthroscopy. More than two-thirds of the patients are satisfied after surgery. Nevertheless, average scores from patients indicate residual mild hip pain and/or ADL and sport function lower than their healthy counterparts after hip arthroscopy. Owing to the current low level of evidence, future RCTs and cohort studies should investigate the effectiveness of hip arthroscopy in patients with FAI.
What is already known?
Patients with symptomatic femoroacetabular impingement (FAI) experience hip pain, as well as decreased activities of daily living (ADL) and sport function.
Hip arthroscopy seems to reduce hip pain and improve ADL and sport function mostly based on low level of evidence case series, but the improvements at different time points are not known.
What are the findings?
In patients with FAI, hip pain reduction and ADL function improvements may be achieved between 3 and 6 months after surgery, while sport function improvements occurs between 6 months and 1 year after hip arthroscopy.
Hip pain, ADL and sport function improvements are evident at least up to 3 years after hip arthroscopy in patients with FAI.
Average scores from patients indicate residual mild hip pain and/or hip function during ADL and sport lower than their healthy counterparts after hip arthroscopy.
REFERENCES
Footnotes
Contributors All authors helped design the study. SK and ML-C conducted literature search, data selection, quality assessment and data extraction (BL helped with surgical data). SK wrote the initial draft of the manuscript. All authors contributed the final draft and approved the manuscript before submission.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.