Article Text

Statistics from Altmetric.com
- relative energy deficiency in sport (RED-S)
- low energy availability
- female athlete triad
- disordered eating
- amenorrhea
- low testosterone
- low bone mineral density
Introduction
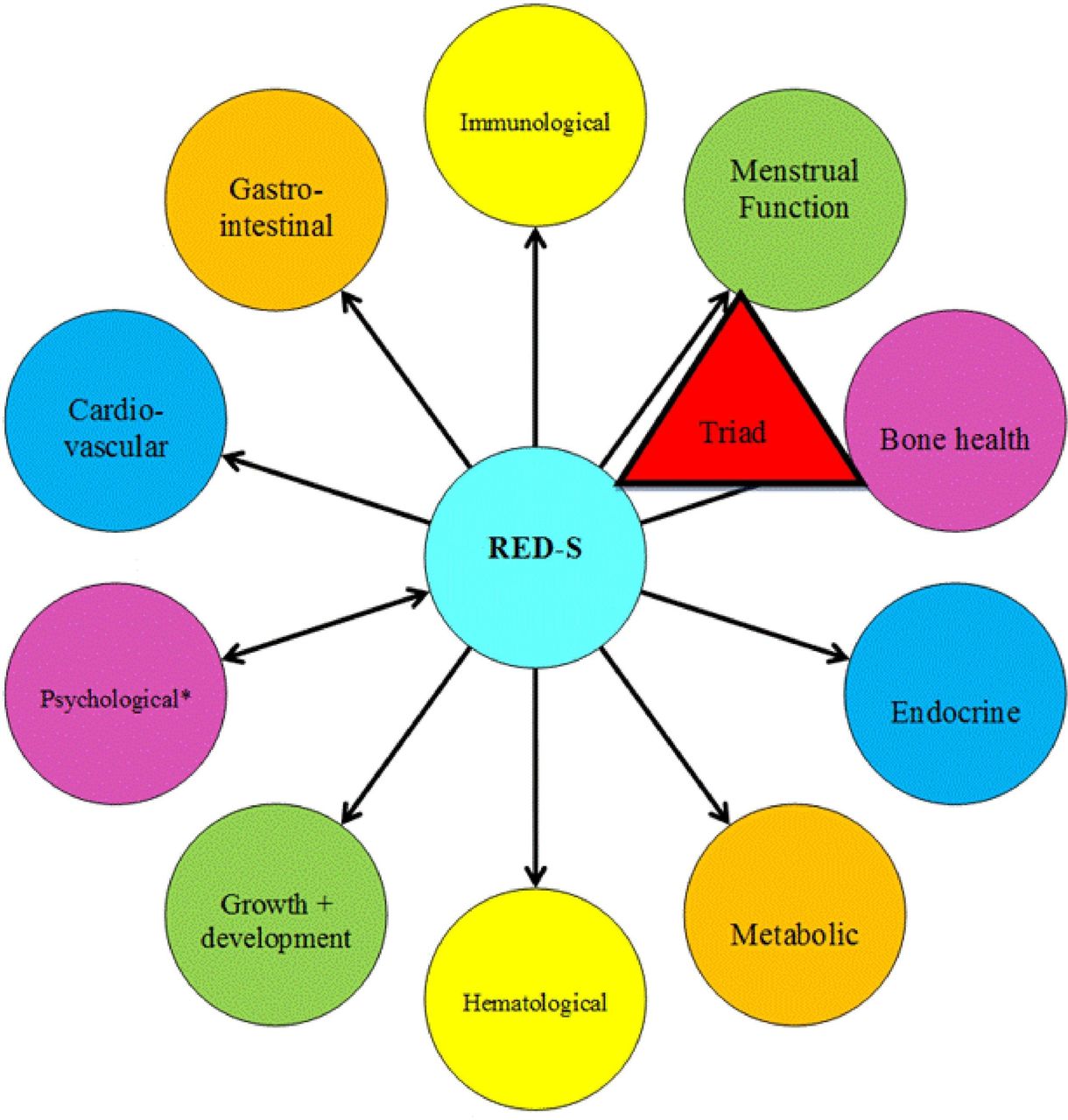
In 2014, the IOC published a consensus statement entitled ‘Beyond the Female Athlete Triad: Relative Energy Deficiency in Sport (RED-S)’. The syndrome of RED-S refers to ‘impaired physiological functioning caused by relative energy deficiency and includes, but is not limited to, impairments of metabolic rate, menstrual function, bone health, immunity, protein synthesis and cardiovascular health’. The aetiological factor of this syndrome is low energy availability (LEA).1
The publication of the RED-S consensus statement stimulated activity in the field of Female Athlete Triad science, including some initial controversy2 3 followed by numerous scientific publications addressing:
The health parameters identified in the RED-S conceptual model (figure 1).1 4
Relative energy deficiency in male athletes.
The measurement of LEA.
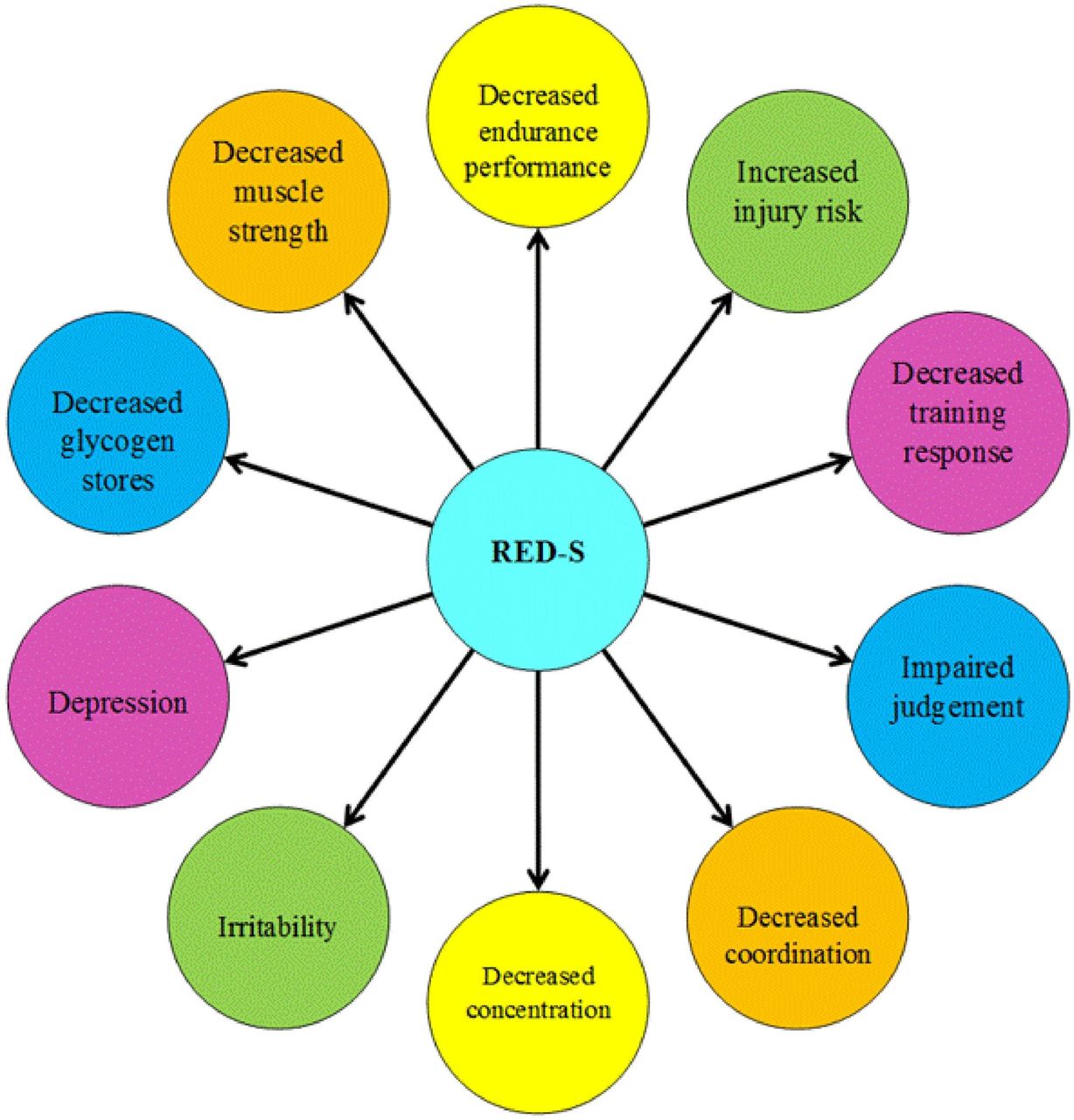
The performance parameters identified in the RED-S conceptual model (figure 2).1 4
The IOC RED-S consensus authors have reconvened to provide an update summary of the interim scientific progress in the field of relative energy deficiency with the ultimate goal of stimulating advances in RED-S awareness, clinical application and scientific research to address current gaps in knowledge.

Health consequences of Relative Energy Deficiency in Sport (RED-S) showing an expanded concept of the Female Athlete Triad to acknowledge a wider range of outcomes and the application to male athletes (*Psychological consequences can either precede RED-S or be the result of RED-S).1 4

{kind=link}
{kind=link}
Potential Performance consequences of Relative Energy Deficiency in Sport (*Aerobic and anerobic performance).1 4
Low energy availability
LEA, which underpins the concept of RED-S, is a mismatch between an athlete’s energy intake (diet) and the energy expended in exercise, leaving inadequate energy to support the functions required by the body to maintain optimal health and performance. Operationally, energy availability (EA) is defined as:

where exercise energy expenditure (EEE) is calculated as the additional energy expended above that of daily living during the exercise bout, and the overall result is expressed relative to fat-free mass (FFM), reflecting the body’s most metabolically active tissues.5 6 Rigorously controlled laboratory trials in women have shown that optimal EA for healthy physiological function is typically achieved at an EA of 45 kcal/kg FFM/day (188 kJ/kg FFM/day).7 8 Meanwhile, although some caveats are noted in relation to differential responses of various body systems,9 many of these systems are substantially perturbed at an EA <30 kcal/kg FFM/day (125 kJ/kg FFM/day), making it historically a targeted threshold for LEA. However, recent evidence suggests that this cut-off does not predict amenorrhoea in all women.10 11 In addition, and not withstanding differences across body sizes and pubertal age, it is noted that an EA of 30 kcal/kg/FFM roughly equates to the average resting metabolic rate (RMR).5 Because LEA has proven robust in explaining markers of suboptimal health and function in both laboratory7 8 and field settings,12 13 it seems logical that an EA assessment could serve as a diagnostic tool in the prevention or management of RED-S.
Measurement of EA
Despite the primary importance of determining whether an athlete has adequate EA, several barriers prohibit the direct measurement of EA from being a practical and reliable option. First, there is no standardised or reference protocol for undertaking an EA assessment (eg, the number of collection days, methodologies for assessing energy intake, exercise energy expenditure or FFM). Furthermore, there are significant concerns over the reliability and validity of each of these metrics. The greatest challenge is to gain an accurate record of usual energy intake from self-reported sources.9 14 Other challenges include the measuring of exercise energy expenditure during many of the training/competition activities performed by athletes and accounting for their additional recreational/lifestyle activity.9 15 These problems may partially explain why many field studies report considerable discrepancies between EA calculations and symptoms associated with LEA.9 14 16–18 However, other explanations for these observations include: (1) the temporal dissociation between the period of mismatched eating and exercise behaviour that created the LEA problems and the occasion on which the EA assessment was undertaken and (2) the interaction of other dietary characteristics that often co-exist with LEA and may exacerbate its effects (eg, high intake of fibre, stimulants and artificial sweeteners; low energy density foods; high dietary restraint and poor spread of energy within a day).19–23 Even if these problems could be solved, EA calculations would likely involve specialised equipment and expertise (eg, dual energy X-ray absorptiometry measurement of body composition), good motivation and compliance of the athlete (eg, keeping a food record or comprehensive activity diary) and considerable time and expertise to process the information. Additionally, LEA states may develop at different stages of training and competition due to varying physiological demands. An EA assessment may achieve some valuable outcomes, such as strengthening the interaction between the practitioner and athlete, which can create rapport, trust and an appreciation of EA needs. However, the considerable effort needed to assess EA and its frailties as a stand-alone diagnostic tool prevent expert bodies from instituting it as a universally recommended measurement.
Low energy availability in male athletes
Similar to female athletes, there is growing evidence that males may experience LEA in situations when there is a mismatch between energy intake and the exercise energy expenditure of training or competition. Populations of male athletes at increased risk for LEA and resulting health consequences of RED-S include cyclists, rowers, runners, jockeys and athletes in weight class combat sports.24–30 Factors that contribute to LEA in male athletes are varied and often unique to the sport. They include the cyclical changes in body mass and composition (‘making weight’), prolonged inadequate energy intake to meet high exercise energy expenditure of endurance sport, punctuated changes in training volume/intensity and participation in strenuous endurance events without accompanied changes in nutrition.26 Inadequate food availability, including food insecurity from cultural practices or lack of financial resources may also contribute risk for LEA in some male athletes, even among high calibre athletes, as it undoubtedly also does in female athletes.26
While RED-S may occur in both sexes, there are likely differences in biological responses to LEA in male athletes compared with their female counterparts. The prevalence of LEA has been suggested to be higher in females than in males, although precise differences are unknown.31 The threshold and duration of the LEA state required to induce RED-S in men is unknown. Reduction in the sex hormone testosterone is likely to be of greater health concern in male athletes.28 32 33
Low energy availability in para-athletes
The prevalence of LEA in para-athletes is incompletely characterised.34 When extrapolating from trends noted in general populations of individuals with disability, it can be assumed that athletes who use a wheelchair for daily mobility are likely to have reduced baseline energy needs.35 36 Despite this, male and female athletes with spinal cord injury (SCI) may monitor or restrict body weight for sport and are at risk for nutrient deficiencies.37 38 Athletes with central neurological injury, such as cerebral palsy, who demonstrate aberrant movement patterns that include dyskinesis or athetosis, may have higher energy expenditures than similar athletes without such non-purposeful movements.39 Additionally, the presence of central neurological injury may result in alterations of the hypothalamic–pituitary axis and baseline menstrual function, regardless of energy status.40–42 Amputee athletes may have higher energy needs in the setting of prosthetic use and resultant gait asymmetry.43
Para-athletes are at high risk for impaired bone health and bone-related injury secondary to many factors, including altered skeletal loading. For example, in unilateral amputees, the affected limb may exhibit reduced bone mineral density (BMD).44 Athletes with SCI have disuse osteopenia/osteoporosis affecting the lower extremities; however, positive adaptive changes in upper body BMD values have been reported in wheelchair basketball players compared with non-athletes (greater radial BMD and trend towards increased lumbar BMD).45Characterising effects of LEA on bone in para-athletes requires consideration of baseline effects of each individual’s underlying disability. More work is needed in this area.
Given rising participation in para sport from grass roots to elite levels, further research is needed to investigate the impact of LEA in athletes with a disability. The para-athlete population requires screening for LEA to reduce complications of RED-S, including low BMD.
Race and low energy availability
Whether race plays a role in the incidence and underlying aetiology of RED-S remains speculative. Research shows a lower risk of disordered eating (DE) in African-American, but not Latino female high-school athletes compared with Caucasians.46 47 It is currently unknown whether the prevalence of menstrual disorders differs among racially diverse athletic groups. Stress fractures in African-American military recruits are lower than in Caucasian recruits.48 Meanwhile, male Kenyan runners have been observed to have greater BMD at weight-bearing sites (eg, proximal femur) than healthy controls, but not at the lumbar spine, where Z scores were reported to be below −2.0 in 40% of study subjects.49 Such runners may have LEA resulting from low energy intake and high exercise energy expenditure associated with heavy training loads,49 as has been previously shown.50 51 In another study of young Kenyan female athletes, middle-distance and long-distance runners were found to exhibit one or more subclinical and/or clinical components of the RED-S, including a greater risk for LEA and menstrual dysfunction than controls.52 A study of sport nutrition knowledge, behaviours and beliefs across sex, race/ethnicity and socioeconomic status in high school soccer players identified that general sports nutrition knowledge is lower in adolescent soccer players compared with prior reports in adolescent athletes and that specifically females and Latinos may benefit from sport nutrition education.53 Published research is greatly lacking on RED-S in African-American, Hispanic and Asian athletes, with a few exceptions.54 55 Thus, there is a need to include more diverse athlete populations in RED-S research and to integrate race/ethnicity in the prevention and treatment of RED-S.
Health effects of low energy availability
Endocrine
Effects of LEA on the endocrine system have been described predominantly in female athletes and only recently in male athletes. Findings in some female athletes in LEA states (measured EA and/or athletes with amenorrhoea) include disruption of the hypothalamic–pituitary–gonadal axis, alterations in thyroid function, changes in appetite-regulating hormones (eg, decreased leptin and oxytocin, increased ghrelin, peptide YY and adiponectin), decreases in insulin and insulin-like growth factor 1 (IGF-1), increased growth hormone (GH) resistance and elevations in cortisol.8 56–59 Many of these hormonal changes likely occur to conserve energy for more important bodily functions or to use the body’s energy reserves for vital processes.60 61
Specific changes in men are not completely understood; however, reduced leutinizing hormone (LH) pulsatility and amplitude have been described in a case series of male marathon runners, a population at high risk for LEA.62 Other studies, primarily in endurance male athlete populations, have shown reductions in testosterone and inconsistent findings in differences in basal LH parameters.63 64 Koehler et al assessed the effects of short-term EA manipulation through diet and exercise on various hormonal parameters in six male habitual exercisers.65 Each male experienced four separate 4-day conditions: LEA (15 kcal/kg FFM/day with and without exercise) and adequate EA (40 kcal/kg FFM/day with and without exercise). Following both LEA conditions, regardless of exercise, leptin and insulin were reduced compared with baseline (−53% to −56% and −34% to −38%, respectively). LEA did not significantly affect ghrelin, triiodothyronine (T3), testosterone or IGF-1 levels. Thus, the LEA state, often in combination with disruptions to endocrine function in women and possibly men, may contribute to multiple physiological disease states described by RED-S. However, the relationship is likely to be subject to a large degree of within-participant and between-participant variability; more research is needed, particularly in men.11 66 67
Menstrual function
The effects of LEA on reproductive hormones and menstrual function in female athletes have been well described,8 68 69 although the complex hormonal signalling pathways underpinning these effects are still being fully elucidated. Current evidence supports a LEA-associated disruption of gonadotropin releasing hormone (GnRH) pulsatility at the hypothalamus, followed by alterations of LH and follicle stimulating hormone release from the pituitary and decreased oestradiol and progesterone levels; this is considered a form of functional hypothalamic amenorrhoea (FHA).68 70 The duration and severity of LEA needed to create such disturbances are also unclear, reflecting both the complex nature of the problem and discrepancies associated with the different methodologies used to study it. For example, Loucks and Thuma studied previously sedentary women in a laboratory setting and identified that well-controlled interventions reducing EA below 30 kcal/kg FFM/day via the short-term (5 day) manipulation of exercise energy expenditure and energy intake were associated with a dose–response decrease in LH pulsatility.8 More recently, Williams et al reduced EA via manipulation of energy intake and exercise energy expenditure over several menstrual cycles in untrained, previously eumenorrhoeic subjects.11 The researchers found that the frequency of menstrual disturbances (including luteal phase defects, anovulation and oligomenorrhoea) was affected by the magnitude of energy deficit compared with baseline needs,11 but a specific threshold of EA below which menstrual disturbances occurred was not identified.10
Meanwhile, Reed et al performed a cross-sectional analysis of EA (measured using 3-day diet logs to determine energy intake and a combination of exercise logs and heart rate monitoring to measure estimated exercise energy expenditure) in female athletes with eumenorrhoea and various menstrual disturbances.71 These investigators reported mean EA was >30.0 kcal/kg FFM/day in all the groups (amenorrhoeic, oligomenorrhoeic, ovulatory eumenorrhoeic, inconsistent subclinical menstrual dysfunction eumenorrhoeic and anovulatory eumenorrhoeic athletes) and EA did not discriminate subclinical forms of menstrual disturbance; however, EA was lower in amenorrhoeic athletes compared with eumenorrhoeic athletes (mean 30.9 vs 36.9 kcal/kg FFM/day).71 Thus, severe energy deficiency is known to lead to amenorrhoea, but more work is needed to better understand the interplay of change in short-term and long-term EA and more subtle menstrual disruption.
Bone health
It is established that LEA contributes to impaired bone health in athletes, particularly women. Cross-sectional studies of physically active female athletes with oligomenorrhoea/amenorrhoea or measured LEA have demonstrated decreased BMD, altered bone microarchitecture and bone turnover markers, decreased estimates of bone strength and increased risk for bone stress injuries compared with eumenorrhoeic athletes and those who are energy replete.66 69 72–74 Short-term LEA (via diet and exercise) has prospectively been shown to negatively affect bone turnover markers in women and some men.57 67 Specific female and male sport populations are at increased risk for lower BMD, including jockeys, runners, swimmers and cyclists.24 29 30 75–83 Anatomical sites with less bone loading and/or greater trabecular versus cortical bone content (lumbar spine and radius vs total hip) are at greater risk for low BMD and impaired microarchitecture in populations susceptible to LEA.72 73 77 78 84
Low body mass index (BMI) is an imperfect surrogate marker for LEA. However, BMI ≤17.5 kg/m2, <85% expected body weight for adolescents or ≥10% weight loss in 1 month are proposed indicators of LEA,85 and indeed both BMI and expected body weight cut-offs are associated with increased risk for low BMD in both sexes.24 82 86 LEA may be accompanied by DE/eating disorders (EDs), menstrual dysfunction and low BMD, and the combination of factors places athletes at higher risk for bone stress injury.87–89
Metabolic
LEA has been correlated with decreased RMR in female endurance athletes.90 Prospectively, increasing training load while maintaining constant EI over 4 weeks in male and female elite rowers led to a significant reduction in RMR.91 In normal weight women with induced energy deficits via exercise and dietary manipulation, measured weight loss over 3 months was less than predicted.92 Subjects who were moderately energy deficient had a significant decrease in RMR, and those who were severely energy deficient demonstrated significant decreases in leptin, T3, IGF-1 and an increase in ghrelin.92
Haematological
Iron is essential for haematopoiesis and subsequent oxygen carrying capacity. Iron deficiency, often seen in female athletes, can contribute directly and indirectly to energy deficiency. This is due to a potential reduction in appetite, decreased metabolic fuel availability and impaired metabolic efficiency, leading to an increase in energy expenditure during exercise and rest.93 Iron deficiency may also interact with bone health via dysregulation of the GH/IGF-1 axis, hypoxia and hypothyroidism, in addition to playing an important role in thyroid function, fertility and even psychological well-being.93 Thus, LEA may be partially induced by, and may contribute to, iron deficiency.93 Surrogates for LEA have been correlated with haematological dysfunction, including low ferritin and iron deficiency anaemia, in adolescent and young adult female athletes.94
Growth and development
Linear growth retardation has been reported in various studies of male and female adolescents with severe anorexia nervosa, with studies demonstrating partial, but not always complete, catch-up growth after recovery.95–97 Decreases in IGF-1, increases in GH and increased GH resistance are consistently noted in those with anorexia nervosa.98 Studies in amenorrhoeic athletes have demonstrated disorderly GH secretory patterns, decreased GH and IGF-1 secretory response to exercise accompanied by increased interpulse GH levels and decreased IGF-1/IGFBP-1 ratios, with more research needed to understand training and growth implications.99 100
Cardiovascular
Early atherosclerosis may be associated with hypoestrogenism and FHA in young athletes.101 Endothelial dysfunction and unfavourable lipid profiles have been reported in amenorrhoeic athletes,102 with resumption of menses leading to improvements in vascular endothelial function.103 In one study, amenorrhoeic athletes demonstrated lower heart rates and systolic blood pressure compared with eumenorrhoeic athletes, in addition to disruptions of the normal renin–angiotensin–aldosterone response to an orthostatic challenge.104 In the more severe LEA state of anorexia nervosa, significant cardiovascular changes can occur, including valve abnormalities, pericardial effusion, severe bradycardia, hypotension and arrhythmias.105
Gastrointestinal
In the severe LEA state of AN, negative health influences on the full gastrointestinal tract such as altered sphincter function, delayed gastric emptying, constipation and increased intestinal transit time, have been described.106 Melin et al measured EA and developed the Low Energy Availability among Female Athletes Questionnaire (LEAF-Q), both of which found a negative correlation with EA and gastrointestinal symptoms in elite Swedish and Danish athletes.12 These findings were supported in a survey of adolescent American female athletes with surrogate markers of LEA, who also reported a higher incidence of stool leakage and constipation than those considered to have adequate EA.94
Immunological
The immune system may be altered by LEA. A study of 21 Japanese elite, collegiate runners reported more upper respiratory symptoms and lower immunoglobulin A secretion rates in the amenorrhoeic versus eumenorrhoeic athletes.107 Meanwhile, in observational studies of elite Australian athletes in preparation for the 2016 Rio Olympic Games, LEA, as measured by the LEAF-Q in female athletes, was associated with increased likelihood of illnesses (including those of the upper respiratory tract and gastrointestinal tract), bodily aches and head-related symptoms in the previous month.108 109
Psychological
Psychological problems can precede or be caused by LEA.1 LEA in athletes has been shown to have negative correlates with various aspects of psychological well-being. Higher drive for thinness may be a proxy for LEA, as higher drive for thinness scores on the Eating Disorder Inventory have been associated with reduced resting energy expenditure, lower T3 levels, and higher ghrelin levels in female athletes.110 Athletes who scored higher on DT also scored higher in domains of ineffectiveness, cognitive restraint, and bulimic tendencies.110 Adolescent females with FHA have been found to have a higher incidence of mild depressive traits, psychosomatic disorders, and a decreased ability to manage stress.111 112 A separate study found overlap in adolescents with anorexia nervosa and those with FHA: both groups demonstrated increased depression, social insecurity and introversion and fears of weight gain compared with healthy controls.113 More profound psychological disturbances were seen in the presumably more restricted EA (anorexia nervosa) group versus the FHA group.113 Results from a study with male athletes indicated that dietary restraint and muscle building behaviours were associated with bulimic symptomatology.114 Additionally, studies of male body builders indicate that a prolonged EA of approximately 20–25 kcal/kg FFM/day, as seen in the final stage of contest diets, might be pathological and have negative psychological effects for males.27 The restrictive diet patterns observed resulted in a reduction in muscle mass and a loss of strength, with reports of endocrine dysfunction and mood disturbances in those athletes with body composition measurements of approximately 4% total body fat.27
Disordered eating and eating disorders
Disordered eating and eating disorders are more prevalent among female and male athletes in weight-sensitive sports in comparison to athletes representing sports in which leanness is a less important performance variable.115–119 In a Norwegian study of adolescent elite male and female athletes, a higher prevalence of disordered eating in non-athletes as compared with athletes was found when using questionnaires,120 but when using a clinical interview, the prevalence of eating disorders was higher in athletes versus controls.121 These findings suggest the need for personal interviews to diagnose eating disorders in athletes.117 121 122 It should be noted that the revised diagnostic criteria for eating disorders (Diagnostic and Statistical Manual, fifth edition) may influence the prevalence of the different diagnoses among athletes.123 124
The pathogenesis of eating disorders is multifactorial with cultural, familial, individual and genetic/biochemical factors playing roles.125 Weight pressure and unique eating disorder risk and trigger factors have been reported and include performance pressure, sudden increase in training volume, injury, teammate modelling of eating disorder behaviours and team weigh-ins.126–128 A desire to be leaner to enhance performance seems to predict later disordered eating127 and the risk of eating pathology increases when the coach–athlete relationship is characterised by high conflict and low support.129 Disordered eating seems to be influenced by perfectionism, competitiveness, pain tolerance and the perceived performance advantage of weight loss.130 These suggested risk factors need to be validated to demonstrate a causal relationship. However, these findings serve as a call to action for enhanced screening for eating disorder risk among athletes who experience weight pressure, are injured, or who have teammates with known disordered eating/eating disorders.126
Performance consequences of low energy availability
Associations between various surrogates of LEA (eg, hormonal aberrations, oligomenorrhoea/amenorrhoea, leanness sport participation and increased scores on ED/DE/LEA screening tools) and factors negatively influencing performance (eg, illness, injury, iron deficiency, impaired cognition and mood) have been reported.87 93 94 131–137 Intervention studies on long-term energy restriction and sport performance are lacking.138 However, it has been postulated that persistent LEA could impair sport performance through a variety of different indirect mechanisms (eg, impaired recovery leading to premature reduction in physical, psychological and mental capacity and impairment of optimal muscle mass and function).139 Indeed, LEA could be expected to impair performance or interfere with optimal performance gains via acute impairment of key processes such as glycogen storage140 or protein synthesis,141 or by preventing consistent and high quality training due to the increased risk of injury and illness.108 109
Despite the importance of these associations, it is only recently that studies have tried to measure the direct impact of LEA on sports performance. For example, Silva and Paiva reported that athletic performance, measured as competition ranking, negatively correlated with EA in elite rhythmic gymnasts.142 Furthermore, Tornberg et al found no difference in aerobic capacity (VO2, O2 (mL/min/kg)) between elite eumenorrhoeic endurance athletes and elite endurance athletes with secondary FHA, despite lower body weight and fat mass in the athletes with FHA.143 However, subjects with FHA had decreased neuromuscular performance (measured as knee muscular strength and endurance) and reaction time compared with the eumenorrhoeic athletes.143 Overall, lower neuromuscular performance was associated with higher cortisol levels, and lower blood glucose, T3, oestrogen and FFM in the tested leg.143 Although striving for a greater power to mass ratio is commonly regarded as important for running performance, this study suggests that achieving an idealised body weight or body composition through severe and persistent energy restriction is likely to negatively affect performance and health.143 This finding is supported in a study of East African runners.144 Woods et al followed male and female national team rowers through a 4-week intensified training period, which was accompanied by a lack of increase in energy intake despite a 21% increase in training load.91 It was concluded that inadequate EA likely negatively affected training recovery, at least partially explaining the alterations in 5 km time trial pacing strategy and reduced performance.91
Considering the reported high prevalence of menstrual dysfunction caused by energy deficiency,145 surprisingly, only one study has investigated the direct impact of LEA on sport performance. Vanheest et al reported a 10% decline in swimming velocity over a 400 m time trial (after 12 weeks of training) among young elite swimmers with ovarian suppression secondary to energy deficiency compared with an 8% improvement in their eumenorrhoeic teammates.13 Clearly, more investigations, including robust protocols involving random allocation of athletes to intervention groups, are needed to provide further evidence and explanation of the effects of LEA on training adaptations and sport performance.
Prevention of relative energy deficiency in sport
The prevention of RED-S requires increased awareness among athletes and their entourage. Current evidence suggests that there is much work to be done. Surveys have reported that less than 50% of physicians, coaches, physiotherapists and athletic trainers could identify the triad components (LEA with or without an eating disorder, menstrual dysfunction and low BMD),70 146–152 and only 19% of 370 US high school nurses could identify all three triad components.153 In a survey of 931 multispecialty physicians, only 37% were aware of the triad, and only one-half of these were comfortable treating or referring a patient.70 In a group of exercising Australian women, one-third believed irregular periods were ‘normal’ for active females, and approximately half reported knowing that menstrual dysfunction was a risk factor for poor bone health.154 Educational programmes typically identify their target audiences as health professionals, coaches, athletic trainers, teachers, school administrators, athletes and parents.155 However, a survey of International Sport Federations (IFs) identified that only 2 of 28 Olympic IFs had programmes on RED-S, indicating the need to also involve a top-down approach.156 Peer-based eating disorder/body image/triad education and cognitive-dissonance based programmes have shown promise,157–160 and similar RED-S peer-led programmes should be developed.
Effective eating disorder prevention programmes should be multimodal, interactive and target athletes and coaching staff.161 One successful intervention is a peer-led educational programme for female athletes that resulted in improved bulimic pathology 1 year postintervention.162 A Norwegian school-based controlled intervention programme, including elite male and female athletes163 and coaches,164 resulted in no new cases of eating disorders among females in the intervention schools as opposed to eight (13%) in females at the control schools.163 There was only one new eating disorder case in a male at a control school and none in males from the intervention schools.163 These results suggest that effective disordered eating and eating disorder prevention should target individuals beyond athletes and coaches, be gender specific, involve significant others and include changes to sport regulations, policy measures and the healthcare system.165
Screening for relative energy deficiency in sport
Early detection of athletes at risk for energy deficiency is critical to prevent long-term health sequelae.1 69 85 There are several disordered eating/eating disorder screening tools intended for general population.166–169 Some tools have been developed to target athletes, although none are validated for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria.170–172 Additionally, due to stigma associated with eating disorders, athletes may be motivated to hide their illness. An elevated Eating Disorder Inventory—drive for thinness score168 has been reported to indicate energy deficiency in exercising women,173 and amenorrhoeic athletes seem more likely to have an elevated drive for thinness score compared with eumenorrhoeic athletes.173 In order to diagnose an eating disorder, additional in-depth personal interviews must be performed.117 121 122 166 However, the prevalence of energy deficiency is reported to be high in some athletes even without the presence of disordered eating/eating disorders.90 145
Although coaches are in an ideal situation to identify athletes with disordered eating/eating disorders, they sometimes have difficulty distinguishing between athletes whose appearance or body composition metrics meets their sport-type expectations (eg, thin) from those with an eating disorder, especially if the athlete’s performance is good.174 Even if disordered eating is identified, coaches may have difficulty convincing athletes to seek treatment.175
The Periodic Health Examination176 and the Preparticipation Physical Evaluation177 include relevant questions that may be helpful for early detection. Recently, the LEAF-Q was developed12 as a brief questionnaire on physiological symptoms linked to energy deficiency, and the Low Energy Availability in Males Questionnaire is in development. Expanded testing of these questionnaires in various athletic populations is needed. There is limited evidence for the efficacy of self-reported questionnaires, and additional individual evaluation is recommended.1 85 The RED-S Clinical Assessment Tool (RED-S CAT) can assist clinicians in screening for RED-S and the management of return to play decisions,178 although validation is needed.
Treatment of relative energy deficiency in sport
Non-pharmacological management
If LEA is due to unintentional under eating, then simple nutritional education may suffice. Regardless of the severity of the eating pathology, early involvement of an accredited or appropriately trained expert (eg, sports dietitian) is recommended to enhance the athlete’s nutritional practices. Optimising EA can improve function of the hypothalamic–pituitary–gonadal axis, as well as other systems negatively affected by LEA in females.15 179–181 Energy deficits should be addressed via modification of exercise and nutrition practices68 182 in both female and male athletes and energy needs may be even higher in growing adolescents. Treatment is typically based on increased food intake but may also require changes in food choices, energy spread and other dietary characteristics; these changes must be individualised and periodised according to the athlete’s energy expenditure and exercise goals. A reduction or cessation of exercise may be necessary, depending on the severity of the energy deficit, symptoms and compliance level.
Adequate bone-building nutrients are critical; for example, serum 25-hydroxy vitamin D levels <30 ng/mL are associated with increased incidence of bone stress injury.183 184 Vitamin D intake of 600–800 IU daily is recommended by USDA dietary guidelines,185 but greater intake may be needed temporarily to reach goal serum 25-hydroxy vitamin D levels of >30 ng/mL.186–188 Improving 25-hydroxy vitamin D levels may also reduce healing time and facilitate earlier return to play for bone stress injury.189 Additionally, adequate consumption of calcium may help decrease the incidence of bone stress injury.190 191 The current recommendation for daily calcium intake is 1000 mg/day of calcium for men and women aged 19–50 years, and 1300 mg/day for children and adolescents aged 9–18 years.192
Cognitive behavioural therapy is another non-pharmacological treatment for RED-S that has been shown to contribute to the resumption of menses in some women with FHA.193 194 Initial non-pharmacological management of RED-S may restore menstrual function over months,181 195 while improvements in bone health take longer and may never reach optimal levels.15 Non-compliance with therapy may require removal of the athlete from training/competition. Examples of treatment contracts and clearance categories for return to play can be found in other publications.1 85 196 Current recommendations need further validation and may lead to the eventual inclusion of other progress parameters, such as RMR and blood biomarkers.
Pharmacological interventions
The use of combined oral contraceptives for the intention of regaining menses or improving BMD in those with RED-S is not recommended. Data regarding the effects of combined oral contraceptives on BMD and fracture risk are inconsistent.68 197–200 If using combined oral contraceptives for contraception, the athlete should understand that combined oral contraceptives may mask the return of spontaneous menses, and bone loss may continue if the energy deficit is not corrected. If menstrual cycles do not return after a reasonable trial of nutritional, psychological and/or modified exercise interventions, transdermal oestradiol (E2) therapy with cyclic oral progestin can be considered for short-term use.68 Notably, transdermal E2 is not a reliable form of hormonal contraception and an athlete should be counselled to avoid unintended pregnancy if she receives transdermal E2 for bone health. Transdermal oestrogen does not affect IGF-1 secretion, a bone-trophic hormone that combined oral contraceptives downregulate, and has been shown to improve BMD in anorexia nervosa201 and BMD and bone microarchitecture in oligo-amenorrhoeic athletes.202 Recombinant parathyroid hormone 1–34 (rPTH) has been shown to improve BMD in AN203 and rare, short-term use may be considered in adults with LEA, FHA or RED-S in the setting of delayed fracture healing or very low BMD.68 Transdermal oestrogen or rPTH should only be prescribed in conjunction with a metabolic bone expert and it is important to note that rPTH is contraindicated in adolescents and young adults with open growth plates.68
Treatment strategies for disordered eating/eating disorders
Apparent disordered eating/eating disorders should be treated with a multidisciplinary team including medical, dietary and mental health support. Inpatient treatment should be considered for patients with severe bradycardia, hypotension, orthostasis and/or electrolyte imbalance.85 196 204 Athletes’ resistance to treatment usually increases with the severity of the problem.205 Because many patients with eating disorders see their disorders as purposeful and necessary,206 motivation to recover is a critical factor in treatment. With sport participation as leverage for athletes, the desire to be healthy enough to return to sport most often facilitates recovery for athletes with eating disorders.207
As higher levels of depression and anxiety are observed in athletes with eating pathology,208 there is a need to treat these pathologies in athletes with disordered eating/eating disorders. Additionally, comorbid disorders of depression, anxiety and substance abuse complicate eating disorder treatment and require treatment modifications.165 209 Ideally, treatment should be provided by a mental health professional experienced in treating eating problems in athletes.205 For athletes, meeting the diagnostic criteria for severe eating disorders (eg, anorexia nervosa and bulimia nervosa), participation in competition is not recommended.1
Conclusions
Since the original publication of the IOC consensus statement on RED-S in 2014, there have been many scientific advances to improve our understanding of the health and performance effects of LEA in both female and male athletes. To address remaining gaps, the IOC RED-S consensus authors encourage scientific activity in the following domains:
Identification of athletes at risk for RED-S: it is evident that there is no practical tool for the measurement of EA; therefore, there is a recognised need to develop a methodology to screen and identify athletes at risk for RED-S that is both scientifically validated and relevant and applicable in clinical sport practice.
Prevention of RED-S: improved awareness of RED-S is required through educational initiatives for athletes, coaches, members of the entourage and sport organisations. The development of scientifically validated prevention interventions is encouraged.
Male athletes: despite the improvement in the knowledge base of RED-S in male athletes, there remains a gap in our understanding of RED-S in specific sports with differing energy demands, performance criteria, ethnicities and cultural perspectives.
Health and performance consequences of RED-S: there is still much to be learned about the psychological and physiological health risks and long-term consequences of RED-S in all athletes, particularly male athletes, para-athletes and athletes of various races. To best engage the attention of athletes and coaches, it is imperative to further increase our understanding of the performance effects of RED-S.
Treatment and ‘return to play’: practical guidelines for the treatment and safe return to play for athletes with RED-S need to be further developed to improve athletes’ health and performance.
Acknowledgments
The authors would like to gratefully acknowledge the work of Barbara Drinkwater in the field of the Female Athlete Triad and for her ongoing support of the advancement of science in this domain. A special thanks to Allyson L Parziale and Bryan Holtzman for their logistical and editorial assistance.
References
Footnotes
Contributors MM, JKS-B, LMB substantially contributed to the conception and design and are the co-coordinators of IOC Expert Group. MM, JKS-B, LMB and KEA substantially contributed to drafting and revising the manuscript. CB, NC, CL, BL, AKM, NLM, RTS, AST, MKT and RB are the members of IOC Expert Group and substantially contributed to drafting the manuscript. RB is the Director IOC Medical and Scientific Department and contributed to revising the manuscript. All authors confirmed the final version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There is no unpublished data.
Presented at This article has been copublished in the International Journal of Sport Nutrition and Exercise Metabolism; doi: 10.1123/IJSNEM.2018-0136.