Article Text

Abstract
Objectives The primary objective was to calculate the rate of return to sport (RTS) following anterior cruciate ligament (ACL) reconstruction in elite athletes. Secondary objectives were to estimate the time taken to RTS, calculate rates of ACL graft rupture, evaluate postsurgical athletic performance and identify determinants of RTS.
Design Pooled RTS and graft rupture rates were calculated using random effects proportion meta-analysis. Time to RTS, performance data and determinants of RTS were synthesised descriptively.
Data sources MEDLINE, EMBASE, AMED, CINAHL, AMI, PEDro, SPORTDiscus and The Cochrane Library were searched from inception to 19 January 2016. Hand searching of 10 sports medicine journals and reference checking were also performed.
Eligibility criteria for selecting studies Studies were included if they reported the ratio of elite athletes who returned to their preinjury level of sport following ACL reconstruction. Twenty-four studies were included.
Results The pooled RTS rate was 83% (95% CI 77% to 88%). The mean time to RTS ranged from 6 to 13 months. The pooled graft rupture rate was 5.2% (95% CI 2.8% to 8.3%). Six out of nine studies that included a noninjured control group found no significant deterioration in athletic performance following ACL reconstruction. Indicators of greater athletic skill or value to the team were associated with RTS.
Summary and conclusions Eighty-three per cent of elite athletes returned to sport following ACL reconstruction, while 5.2% sustained a graft rupture. Most athletes who returned to sport performed comparably with matched, uninjured controls. This information may assist in guiding expectations of athletes and clinicians following ACL reconstruction.
- anterior cruciate ligament
- anterior cruciate ligament reconstruction
- sport re-entry
- elite athletes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about the subject?
Athletes who sustain an ACL rupture often undergo surgical reconstruction to facilitate their return to sport.
In recent years, more studies of ACL reconstruction outcomes have reported the rates of return to sport, which are lower than previously assumed, and further studies focused on elite level athletes and their return to sport following ACL reconstruction have been published.
Little is known about why some elite level athletes do not return to sport or about the outcomes of those elite athletes who do return to sport.
What are the new findings?
The return to sport rate among elite athletes following ACL reconstruction was 83%, and the graft rupture rate was 5.2%.
Most elite athletes took between 6 and 13 months to return to sport, which is less time than what has previously been reported among nonelite athletes.
Although athletic performance among elite athletes who returned to sport after ACL reconstruction often deteriorated compared with preinjury levels, their performance generally remained comparable with that of elite athletes who had not sustained an ACL injury.
Introduction
Athletes who sustain an anterior cruciate ligament (ACL) rupture often undergo surgical reconstruction to facilitate their return to sport.1–3 However, a previous systematic review reported that only 60% of nonelite athletes returned to their preinjury level of sport after ACL reconstruction.4 Elite athletes were analysed as a subgroup rather than being the focus of that systematic review, and additional studies of elite athletes who have undergone ACL reconstruction have since been published. Important physical,5–8 psychological9 and social10 differences between elite and nonelite athletes might give elite athletes a greater chance of returning to sport following ACL reconstruction compared with nonelite athletes.
The primary aim of this systematic review and meta-analysis was to determine the rate of return to the preinjury level of sport following ACL reconstruction among elite athletes. The secondary aims were to assess how long elite athletes took to return to sport, determine the rate of ACL graft rupture among the elite athlete cohort, evaluate athletic performance after ACL reconstruction and identify potential determinants of returning to sport. Further understanding of these outcomes may assist athletes and clinicians to form realistic goals and expectations following ACL reconstruction.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines11 were followed in preparing, conducting and reporting this systematic review.
Search strategy
The electronic databases MEDLINE, EMBASE, AMED, CINAHL, AMI, PEDro, SPORTDiscus and The Cochrane Library were searched from inception to 19 January 2016. Search terms were entered under two concepts; terms within each concept were combined with the OR Boolean operator, and the two concepts were combined with the AND Boolean operator. Where possible, terms were mapped to medical subject headings and searched using keywords. Examples of terms in concept 1 included ‘anterior cruciate ligament’, ‘anterior cruciate ligament reconstruction’ and ‘ACL’. Examples of terms in concept 2 included ‘sport’, ‘athlete’, ‘physical activity’, ‘return to sport’ and ‘sport re-entry’. An example of a database search as applied to MEDLINE is provided in Supplementary file 1.
Supplementary file
To supplement the database searches, we hand searched the online contents pages and ‘Articles in Press’ lists of The American Journal of Sports Medicine; British Journal of Sports Medicine; Arthroscopy; The Knee; Knee Surgery, Sports Traumatology, Arthroscopy; The Journal of Orthopaedic and Sports Physical Therapy; Journal of Science and Medicine in Sport; Sports Health; Orthopaedic Journal of Sports Medicine; and Open Access Journal of Sports Medicine. Studies in the reference lists of the included studies were also screened.
Selection criteria
Studies of interventional or observational design were included if they reported, in English language, the number or ratio of participants who returned to their preinjury level of sport, in a consecutively recruited cohort of at least 10 elite athletes who had undergone ACL reconstruction. Elite athletes were defined as people playing sport professionally, or at the highest possible competitive level for their sport, or in Division I of the National Collegiate Athletic Association.
Conference proceedings and review studies were excluded because of the risk of duplicating data. Studies that included only participants who had undergone revision ACL reconstruction or ACL reconstruction combined with high tibial osteotomy were also excluded.
Two reviewers independently applied the selection criteria to the studies. The reviewers first screened the titles and abstracts of studies identified by the search strategy. Studies that either clearly did not meet the inclusion criteria or had at least one exclusion criterion were excluded. The full-text versions of the remaining studies were then retrieved, and the selection criteria were applied independently by the reviewers. Any discrepancies were discussed, and a third reviewer was consulted if consensus could not be reached. If additional information was required to decide whether a study should be included, attempts were made to contact the authors of the study.
Risk of bias assessment
A six-item checklist12 was used to assess the risk of bias in included studies for this systematic review. The items assessed were selection criteria described, representative population selected, participants’ preinjury sports participation level reported, data collected prospectively, demographic data reported and postoperative sports participation level compared with preinjury level. In addition, the level of evidence for each study in addressing the primary aim of this review was graded.13 For each included study, two reviewers independently assessed and recorded the number of checklist items fulfilled and the level of evidence. Any discrepancies were resolved through discussion; a third reviewer was consulted if consensus could not be reached. The risk of bias assessment was not used in weighting for meta-analysis.
Data extraction and synthesis
Two reviewers independently extracted data from each study. Any discrepancies were resolved by consensus. If further clarification of data was required, contact with the authors of the respective studies was attempted.
‘Return to sport’ was treated as a dichotomous outcome and defined as playing at least one match or competing in at least one event following ACL reconstruction at the preinjury or higher level of competition. The return to sport rate was calculated from the number of elite athletes who returned to sport, out of the number of elite athletes who underwent ACL reconstruction, and expressed as a percentage. If a study defined ‘return to sport’ or derived a return to sport rate in a different manner, and if enough data were available, the return to sport rate was recalculated to meet the definition used in this review.
Where available, rates of ACL graft rupture were calculated from the number of elite athletes who sustained ACL graft rupture out of the number of elite athletes who initially underwent ACL reconstruction, and expressed as a percentage.
The sports and competitions played by participants were extracted from each study. Where three or more studies of the same sport reported return to sport rates or graft rupture rates, subgroup analyses were performed for those sports.
Further data that were extracted from each study included the mean time taken for athletes to return to sport following ACL reconstruction, athletic performance measures of elite athletes who had undergone ACL reconstruction and matched control groups of elite athletes without ACL injury, and determinants of returning to sport following ACL reconstruction. These data were synthesised descriptively.
Pooled rates of return to sport and ACL graft rupture were calculated using random effects proportion meta-analysis (StatsDirect, V.2.8; Altrincham, UK). Heterogeneity was assessed using the I2 statistic14 and interpreted according to the guidelines published by The Cochrane Collaboration.15 Funnel plots were used to evaluate bias in the results of the meta-analyses, and funnel plot asymmetry was quantified with the Harbord test.16
Results
Study selection
The literature search identified 2844 potentially eligible studies for screening; 2502 were excluded after reviewing the titles and abstracts. The full-text versions of the remaining 342 studies were obtained, of which 318 were subsequently excluded. The remaining 24 studies, which included 1272 elite athletes, met the inclusion criteria for this systematic review and meta-analysis (figure 1).
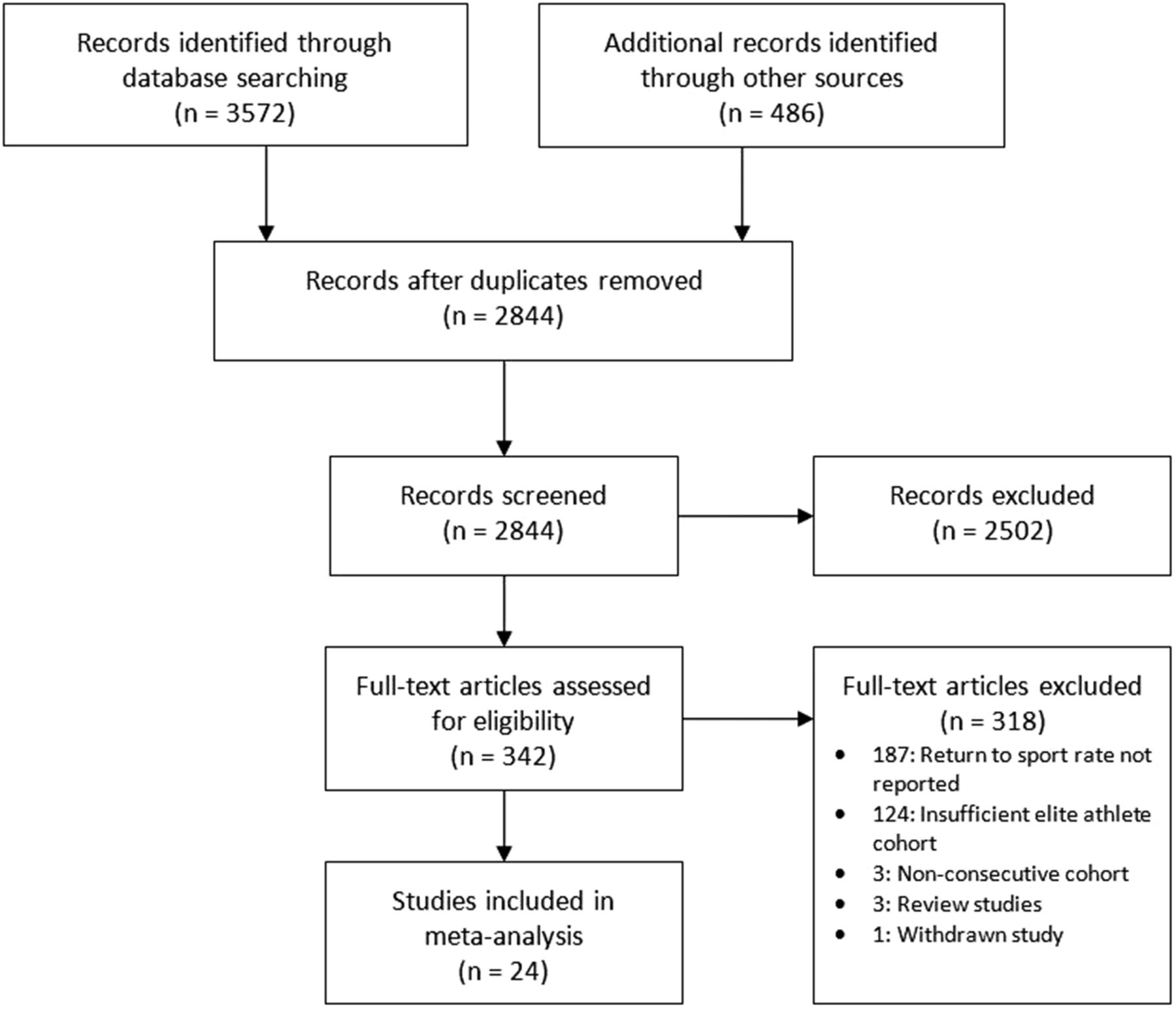
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Risk of bias assessment
Of the 24 studies, 21 (88%) clearly described the selection criteria,17–37 17 (71%) identified the source population,17 18 20 23 25–31 33 34 36–39 and 23 (96%) clearly reported participants’ preinjury level of sports participation.17–25 27–40 Six studies (25%) collected data prospectively,20 26 28 34 35 40 and demographic data were reported in 15 studies (63%).18 19 22–24 27 28 32–39 All of the studies compared postoperative activity levels with preinjury levels. With respect to addressing the primary aim of this systematic review, all of the included studies were graded as level 4 evidence (table 1).
Sports studied
Eighteen studies reported on a cohort of elite athletes from a single sport. Nine of these studies included football players of various codes: four were of soccer players,23 34 35 39 four were of American football players19 21 33 38 and one was of rugby players.40 Three studies were of basketball players,18 27 32 and two studies were of ice hockey players.22 37 Two studies included snow sports athletes: one study was of alpine skiers,36 and one study was of freestyle skiers and snowboarders.24 One study was of baseball players,25 and one study was of handball players.31 Three studies included participants from various sports,17 28 29 while three studies did not report which sports participants played20 26 30 (table 1).
Return to sport rates
The pooled rate of return to sport following ACL reconstruction in elite athletes (n=1272) was 83% (95% CI 77% to 88%; I2=86%; Harbord test=−1.98, 92.5% CI −4.76 to 0.80; figure 2). Among elite soccer players (n=220), the return to sport rate was 85% (95% CI 78% to 90%; I2=36%; Harbord test=1.93, 92.5% CI −9.40 to 13.27; Supplementary file 2). Among elite American football players (n=279), the return to sport rate was 78% (95% CI 67% to 87%; I2=65%; Harbord test=−0.54, 92.5% CI −8.95 to 7.87; Supplementary file 3). Among elite basketball players (n=103), the return to sport rate was 82% (95% CI 74% to 89%; I2=0%; Harbord test=−2.47, 92.5% CI −9.97 to 5.04; Supplementary file 4).
Supplementary file
Supplementary file
Supplementary file

Forest plot of return to sport rates (MLS, Major League Soccer; NFL, National Football League; NHL, National Hockey League).
Time taken to return to sport
Fifteen studies provided data on the duration taken for athletes to return to their preinjury level of sport (table 1). One study reported that all participants returned to sport within 6 months.40 Six studies reported mean times of 6–9 months,20–22 34 35 39 six studies reported mean times of 9–12 months,18 23 27 32 33 37 and two studies reported mean times of 12–13 months.19 38
On average, soccer players returned to sport between 6 and 10.2 months postoperatively,23 34 35 39 American football players returned to sport between 8.2 and 13 months postoperatively19 21 33 38 and rugby players returned to sport within 6 months of ACL reconstruction.40 Basketball players returned to sport, on average, between 10.7 and 11.8 months postoperatively.18 27 32 Ice hockey players returned to sport, on average, between 7.8 and 9.8 months postoperatively.22 37
Graft rupture rates
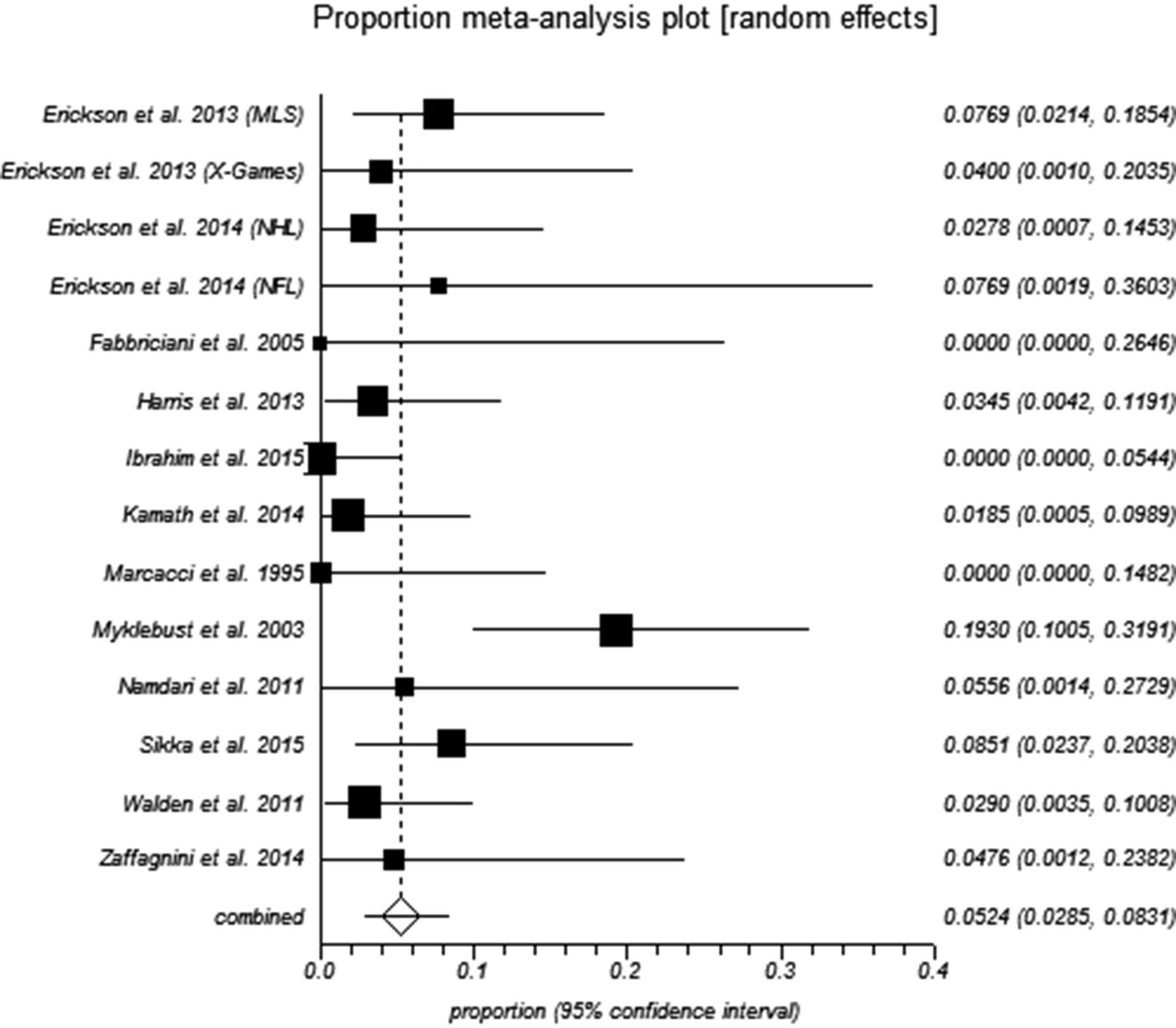
Fourteen of the included studies reported a graft rupture rate (table 1). The pooled graft rupture rate was 5.2% (95% CI 2.8% to 8.3%; I2=51%; Harbord test=0.58, 92.5% CI −3.85 to 2.70; figure 3). Three studies of elite soccer players reported graft rupture rates. The pooled graft rupture rate in elite soccer players was 5.6% (95% CI 2.5% to 9.9%; I2=0%; Harbord test=0.64, 92.5% CI −23.16 to 24.44; Supplementary file 5). Only two studies of American football players and two studies of elite basketball players provided graft rupture rates, so subgroup analyses were not performed.
Supplementary file

{kind=link}
{kind=link}
{kind=link}
Forest plot of graft rupture rates (MLS, Major League Soccer; NFL, National Football League; NHL, National Hockey League).
Characteristics of included studies
Athletic performance on return to sport
Eleven studies compared athletes’ preinjury and postsurgery performances (table 2). Seven of these studies measured overall athletic performance using the following: the number of competition medals won by alpine skiers36 and freestyle skiers and snowboarders,24 International Ski Federation (FIS) rankings and points for alpine skiers,36 the number of All-Star team selections for National Basketball Association (NBA)27 and National Hockey League (NHL)37 players and formulated ratings for players in the NBA18 and the National Football League (NFL).19 38 Eight studies measured performance with various individual statistics, including games played per season,18 22 23 25 27 32 37 38 touchdown passes made by NFL quarterbacks,38 goals scored by soccer23 and ice hockey players,22 37 home runs scored by baseball players25 and shooting percentages among basketball players.18 27 32 Nine of the 11 studies selected a control group of elite athletes who had not sustained an ACL injury but were matched to the ACL reconstruction study group on characteristics, including age, body mass index and amount of playing experience18 22 23 27 32 37 38; national team selection36; preinjury playing performance18 22 23 37 38; and playing position.22 23 27 32 38
Studies comparing athletic performance following ACL reconstruction with preinjury performance and control group performance
Erickson et al 23 reported that the performance of Major League Soccer (MLS) players did not deteriorate significantly following ACL reconstruction, while they attempted more shots at goal and made more assists per season than matched controls. Among NFL players, the study of running backs and wide receivers found that those returning after ACL reconstruction had lower power ratings compared with their preinjury levels and those of matched controls,19 while the study of quarterbacks did not report any significant deterioration in performance postsurgery compared with either their preinjury performance or the performance of matched controls.38
The three studies of elite basketball players each reported that players’ postsurgery performance deteriorated compared with preinjury performance on measures including player efficiency rating,18 number of All-Star selections,27 games played per season,18 27 shooting percentage,18 27 32 points and rebounds per game27 and steals per game.32 However, elite basketball players’ performance did not decline significantly compared with those of matched controls,18 32 except Harris et al 27 reported that players returning from ACL reconstruction played fewer games per season.
The two studies of NHL players had conflicting results. Sikka et al 37 found that forwards and wings who underwent ACL reconstruction did not return to their preinjury level of performance and did not perform as well as players in the control group, while defenders improved their plus-minus rating in their second season after returning to sport and performed comparably with players in the control group. Erickson et al 22 reported that performance did not deteriorate after ACL reconstruction, and some performance measures improved compared with those of the control group.
As a cohort, X-Games freestyle skiers and snowboarders won more medals after surgery than they did preinjury.24 Members of the French national alpine skiing team who underwent ACL reconstruction won more medals per race and improved their FIS rankings and points after surgery.36 After ACL reconstruction, elite baseball players played fewer games per season compared with their preinjury levels.25
Determinants of returning to sport and preinjury performance
Six studies analysed player-related factors possibly associated with a return to sport and preinjury levels of performance. Surrogate measures indicative of greater levels of athletic skill or value to an elite sporting team, including being selected earlier in the NFL draft,33 being on a college sporting scholarship21 39 or having a higher depth chart position (players who started games on field were positioned highest and players who rarely played games were positioned lowest),21 were associated with higher rates of return to sport. NHL players with more goals or assists in the season preceding ACL injury were more likely to return to their previous level of performance.37
Two studies found that more preinjury playing experience was associated with a higher rate of return to sport.21 33 However, college athletes injured during their fourth or fifth years at college were less likely to return to sport,21 39 and NHL players injured after turning 30 years of age were less likely to return to play at least one full season.37 French alpine skiers who were younger at the time of injury were more likely to improve their performance after returning to sport.36 Playing position was not a significant determinant of returning to sport in American football,33 women’s basketball32 or women’s college soccer,39 but Sikka et al 37 found that NHL defenders were more likely to return to their previous level of performance than forwards and wings.
Nine studies reported on the influence of surgical factors on return to sport. Concomitant injuries to menisci were associated with shorter careers among NHL players,37 but no other studies found that concomitant injuries significantly affected return to sport rates.18 21 29 39 Daruwalla et al 21 found that autografts were associated with higher rates of return to sport than allografts, but two other studies did not find any significant association between graft types and return to sport rates39 or postsurgery performance.37 Among elite baseball players, ACL reconstruction to the rear batting leg was associated with decreased batting average on return to sport.25 The timing of surgery,30 tunnel drilling technique21 26 39 or graft fixation method21 28 39 did not significantly affect return to sport rates among elite athletes.
Discussion
Return to sport rates
In this systematic review and meta-analysis, we found that 83% of elite athletes returned to their preinjury level of sport following ACL reconstruction. This finding is consistent with previously published rates4 and incorporates additional data from 11 recent studies. It confirms that rates of return to the preinjury level of sport following ACL reconstruction are higher among elite athletes (83%, 95% CI 77% to 88%) than among nonelite athletes (60%, 95% CI 53% to 67%).4 A combination of factors, including elite athletes having superior athletic skill,5 levels of physical fitness7 and knee proprioception,6 8 different psychological profiles,9 ready access to high-quality healthcare10 and greater financial incentives to play than nonelite athletes might help to explain why elite athletes have a higher rate of return to sport.
Conversely, nearly one out of every five elite athletes who undergo ACL reconstruction does not return to sport, which remains below the expectations of patients undergoing ACL reconstruction41 and their clinicians.42 Our results may help elite athletes who undergo ACL reconstruction, and clinicians who work with elite athletes, to have realistic expectations and goals for surgery and rehabilitation.
Time taken to return to sport
Rehabilitation following ACL reconstruction surgery is a complicated process, and the time from surgery should not be the only factor used to determine when a return to sport should be allowed.43 44 The average time between ACL reconstruction and return to sport may, however, help to guide goal setting for elite athletes and clinicians. Among the 15 studies that reported these data, only two studies of American football players19 38 reported that elite athletes took longer than 12 months on average to return to sport. Two other studies of American football players included in this review reported mean times of 8.2 months21 and 10.8 months21 to return to sport. There are currently insufficient data to confirm whether or not elite athletes from different sports take substantially different amounts of time to return to sport.
The majority of studies in this review reported that elite athletes returned to sport on average within 12 months. This is considerably shorter than what has previously been reported in the nonelite population.45 In our review, it was not possible to determine whether there was any correlation between the amount of time taken to return to sport and graft rupture rates. Although elite athletes appear to return to sport earlier than nonelite athletes,45 whether this approach is safe remains uncertain.
Graft rupture rates
ACL graft rupture is a traumatic and career-threatening event for elite athletes. Elite athletes and clinicians should be aware of the rate of ACL graft rupture when considering the risks and benefits of returning to sport. The pooled graft rupture rate was 5.2% (95% CI 2.8% to 8.3%), which is comparable with a previous meta-analysis of six primary studies of nonelite athletes that reported a graft rupture rate of 5.8%.46 It is important to recognise that the graft rupture rate in this review may be underestimated though, as six of the 14 studies that reported graft rupture rates gathered data from the public domain,22–24 27 32 38 and not all athletes were followed up for the duration of their careers. This graft rupture rate was calculated from studies that met the inclusion criteria for this systematic review, so there may be studies of elite athletes following ACL reconstruction that did not report return to sport rates but did report graft rupture rates. Any such studies have not been included in this meta-analysis. In addition, we were not able to calculate an annualised graft rupture rate because the majority of included studies that reported graft rupture rates did not report the average duration of follow-up.
Athletic performance on return to sport
Feucht et al reported that 94% of patients who were about to undergo primary ACL reconstruction expected to return to sport with only slight or no restrictions.41 It is reasonable to speculate that most elite athletes who undergo ACL reconstruction would expect to return not only to their preinjury level of sport but also to their preinjury level of performance. Returning to preinjury levels of performance can be considered as a further stage of progress following a return to playing at the preinjury level of sport.47 The concept of studying athletic performance on returning to sport from ACL reconstruction is relatively new and under-researched. Eleven studies in this systematic review attempted to compare preinjury and postsurgery athletic performance, and all of them have been published since 2006.
We found conflicting results regarding elite athletes’ performance on their return to sport. Five studies reported that postsurgery performance was unchanged22 23 38 or improved24 36 compared with preinjury performance, while six studies reported that performance deteriorated after surgery.18 19 25 27 32 37 Differing methods of identifying participants might account for some of these discrepancies: for example, Erickson et al 22 used data that were available in the public domain, while Sikka et al 37 accessed a competition-wide injury surveillance system. Even though the studies that used data available in the public domain described thorough search strategies for identifying elite athletes who underwent ACL reconstruction, accessing a database of injuries prospectively collated and maintained by the sporting organisation is likely to be a more reliable source of injury data.
To control for the dynamic nature of elite sport and the progression of time, nine studies used a matched control group with which to compare the study groups’ performances. Encouragingly, six of the nine studies did not demonstrate any significant deterioration in postsurgery performances when compared with the control groups’ performances.18 22 23 32 34 38 In many cases, deterioration in athletic performance following ACL reconstruction may be explained by the progression of time, rather than the result of ACL reconstruction.
Due to the limited number of studies available for each sport, the wide variety of methods used to measure athletic performance and the conflicting results between some studies, the synthesis of athletic performance data was challenging. As further studies explore the concept of returning to preinjury performance following ACL reconstruction, it may become possible to reach stronger conclusions to assist athletes and clinicians. It would be useful for future studies to assess the longevity of elite athletes’ careers following ACL reconstruction. In addition, the increasing use of global positioning systems in sport may offer an avenue to measure performance and load in elite athletes following ACL reconstruction.47
Determinants of returning to sport and preinjury performance
Several studies identified that indicators of greater athletic skill or value to an elite sporting team were determinants of returning to sport. The findings on age and experience were less consistent, but it is possible that even if elite athletes with greater experience are more likely to return to sport, younger elite athletes who return to sport may be more likely to sustain improved athletic performance after ACL reconstruction.
While only one of the included studies found that the presence of concomitant injuries was associated with shortened career length, this may be explained by inadequate power contained within each study. The use of autografts was associated with higher rates of return to sport than the use of allografts in one study,21 but no other surgical factors were associated with different rates of return to sport. This corroborates previous systematic reviews that have not found substantial differences in clinical outcomes following the use of autografts compared with allografts.48–50 There does not appear to be enough evidence to suggest that any one graft choice would increase return to sport rates among elite athletes.
Positive psychological responses to injuries,51 including ACL injuries,52 53 are determinants of returning to sport in the general athletic population. None of the studies included in this systematic review focused on the psychological determinants of returning to sport among elite athletes, and this may be an avenue for further research.
General limitations
The overall return to sport rate of 83% should be interpreted with some caution. There was substantial statistical heterogeneity across the studies (I2=86%), which may be explained by several factors. There was a broad time frame covered across the studies, with elite athletes from as early as 1975 through to 2013 being included. Various methods of identifying and recruiting elite athletes were used across studies, and the rate of return to sport may be affected by the type of sport played. The inconsistent lengths of follow-up across studies may have affected the calculations of pooled return to sport and graft rupture rates. Therefore, it is important that future studies specify the duration of follow-up.
There was also a risk of bias identified in several studies. Nine studies did not report the demographic characteristics of included athletes, which may limit the external validity and generalisability of this meta-analysis. Only six of the included studies collected data prospectively, which introduces a risk of recall bias. However, this risk is expected to be low given that return to sport is usually a highly anticipated and memorable event following major injury. Eight studies collected data exclusively from the public domain,19 22–25 27 32 38 and although the described search methods were comprehensive, it is likely that some ACL injury and return to sport data may have been missed. Although the risk of bias assessment checklist used in this study has been used in previous systematic reviews,4 12 it has not been validated as a mechanism to weight studies in meta-analysis.
All of the studies included in this review were level 4 evidence. We expect that that the majority of future studies in the elite athlete population will also be of observational design. While the quality of findings from this review may be weakened by the lack of interventional studies on elite athletes who sustain ACL rupture, this review does address the aims of the study as best as possible in the elite athlete context.
Publication bias54 may have led to overestimation of return to sport rates and underestimation of graft rupture rates. However, none of the Harbord tests performed were statistically significant at the 92.5% CI. This indicates that publication bias may not have been a significant issue in this meta-analysis, although the substantial heterogeneity present between individual studies limits the interpretation of the Harbord tests.15
There is a relative paucity of research on return to sport rates in the elite female athlete population following ACL reconstruction, even though female athletes face a greater risk of ACL rupture when participating in the same sports as male athletes.55 56 Only two studies included in our review reported on a female-only cohort,32 39 while 13 studies reported on a male-only cohort of elite athletes18 19 21–23 25 27 28 33 35 37 38 40 and most of the remaining studies did not detail the number of male and female elite athletes who returned to sport. These factors meant that we could not determine whether outcomes differed between male and female elite athletes who underwent ACL reconstruction. Our results should not be generalised to elite athletes who have had revision ACL reconstruction, as studies of revision ACL reconstruction were excluded from this meta-analysis, and the outcomes of revision ACL reconstruction, including return to sport rates, are generally inferior compared with primary ACL reconstruction.57 58 However, our meta-analysis does represent the best available estimate of return to sport rates in elite athletes who undergo ACL reconstruction, given that it is based on 1272 elite athletes across 24 studies.
Conclusion
The rate of return to preinjury level of sport following ACL reconstruction among elite athletes was 83%, and most of those who returned to sport played their first game between 6 and 13 months after surgery. Elite athletes with greater levels of athletic skill may be more likely to return to their preinjury level of sport. Five per cent of elite athletes who underwent ACL reconstruction sustained a graft rupture. The performance of elite athletes who returned to sport following ACL reconstruction was comparable with the performance of matched cohorts of elite athletes who had not undergone ACL reconstruction. These results may be used by athletes and their treating clinicians to guide realistic expectations regarding return to sport following ACL reconstruction.
References
Footnotes
Publication embargo This work has been presented at the following conferences:
•The 2016 Sports Medicine Australia Conference, 14 October 2016, as a free paper.
•The 17th European Society of Sports Traumatology, Knee Surgery & Arthroscopy (ESSKA) Congress, 4 to 7 May 2016, as an electronic poster.
Return to sport following anterior cruciate ligament reconstruction in elite athletes: a systematic review and meta-analysis
1. Jessica Thompson is a 28-year-old avid netball fan. She ruptured the anterior cruciate ligament of her left knee 10 years ago while playing nonelite netball for her club. Despite undergoing an anterior cruciate ligament reconstruction, Jessica did not return to sport, which she attributes to a significant fear of reinjuring her knee. Which of the following is most likely to be correct?
(a) Elite athletes place greater demands on their knees than nonelite athletes, so it is unlikely that being in an elite sporting environment would have increased Jessica’s odds of returning to sport.
(b) Even though nearly one out of five elite athletes who undergo anterior cruciate ligament reconstruction never return to their previous level of sport, elite athletes have a greater chance of returning to their preinjury level of sport than nonelite athletes.
(c) Physical attributes alone explain the differing return to sport rates between elite and nonelite athletes following anterior cruciate ligament reconstruction.
(d) Jessica would have been more likely to return to sport if she were playing soccer or football instead of netball.
Answer: (b) This meta-analysis found that 83% of elite athletes return to their preinjury level of sport, which is higher than previously reported rates in nonelite athletes.
2. John Smith is a 24-year-old male professional rugby player who plays at the fullback position. He sustained a direct contact injury to his right knee while being tackled in a match and was subsequently diagnosed with a ruptured anterior cruciate ligament and a lateral meniscal tear. Having undergone an anterior cruciate ligament reconstruction with a hamstrings tendon autograft together with a repair of his lateral meniscus, which of the following statements is true?
(a) The presence of a concomitant injury to his medial meniscus will substantially reduce John’s chances of returning to professional rugby.
(b) There is currently strong evidence to suggest that John, being a fullback, John is more likely to return to sport than a forward would be if they were to sustain a similar injury.
(c) The hamstrings tendon autograft is a better choice than the bone-patellar tendon-bone autograft for elite athletes due to the lower incidence of donor site complications.
(d) If John sustained this injury as a 20-year-old, with less professional rugby experience, he would have been less likely to return to professional rugby.
Answer: (d) The majority of studies in this systematic review did not find that concomitant meniscal injuries, playing position or graft choices were strongly associated with different return to sport rates. Two studies of elite football players of various codes found that greater playing experience was associated with a higher rate of return to sport.
3. Jack Watson is a 28-year-old male professional basketball player in the National Basketball Association. He sustained a left anterior cruciate ligament injury while changing direction 12 months ago. Prior to his injury, he was an All-Star guard. His career is about to resume. Which of the following statements regarding his upcoming performances is most likely to be true?
(a) Given that Jack has taken a full 12 months to return to sport, Jack is likely to return to his preinjury levels of performance within one season on measures including games played per season and shooting percentage.
(b) Very few elite basketball players ever regain their preinjury level of form and Jack should learn to play different roles within the team immediately in order to continue his career.
(c) Jack will find it challenging to add to his previous All-Star selection, but if he can remain on the court, his career trajectory is likely to remain comparable to players with similar experience and playing characteristics.
(d) Guards return to their preinjury level of form more frequently than forwards and centres in the National Basketball Association.
Answer: (c) Studies of elite basketball players have reported that players returning to sport following anterior cruciate ligament reconstruction, on average, do not return to preinjury levels of performance, but these declines are not statistically significant compared with matched control groups.
4. Which of the following rates is closest to the risk of a graft rupture across a career for an elite athlete?
(a) One in 50(2%).
(b) One in 20(5%).
(c) One in five (20%).
(d) One in two (50%).
Answer: (b) The pooled graft rupture rate in elite athletes following anterior cruciate ligament reconstruction was 5.2%.
5. The Australian Rules football season is typically between April and September. Peter Wood is a 23-year-old professional Australian Rules football player who sustained an isolated anterior cruciate ligament injury early in April. Mark’s 25-year-old brother, Andrew, who plays in an amateur nonelite competition, sustained a similar injury one week earlier. Both have elected to undergo ACL reconstruction with hamstrings tendon autografts, and they aim to returning to sport. Which of the following statements is most likely to be correct?
(a) Peter is more likely to return to sport, and a realistic goal is to be ready to play early in the next season.
(b) Peter is more likely to return to sport, and he is a good chance of playing in the finals in September if he undergoes surgery immediately.
(c) Peter is more likely to return to sport, but it is unlikely that he will return until late in the following season (ie, approximately 15 months out of sport).
(d) Andrew is likely to return to sport earlier than his brother because the lower demands of amateur Australian football allow athletes to return to sport earlier on average than those in the high-demand elite environment.
Answer: (a) Elite athletes return to sport more frequently than nonelite athletes, and the majority of studies have reported that elite athletes take between 6 and 13 months on average to return to sport.
Contributors All authors contributed to the conception and design of the review. CCHL and CLA applied the search strategy, applied the selection criteria and completed the risk of bias assessment. CCHL and KEW extracted and synthesised the data. All authors contributed to the analysis and interpretation of data. CCHL wrote the manuscript. CLA, JAF and KEW critically revised the manuscript for important intellectual content. CCHL is responsible for the overall content as guarantor. All authors approved of the final version published.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Full outputs of meta-analyses performed using StatsDirect V.2.8 (Altrincham, UK) are available from the corresponding author on reasonable request.