Article Text

Statistics from Altmetric.com
What you need to know
We make a strong recommendation against the use of arthroscopy in nearly all patients with degenerative knee disease, based on linked systematic reviews; further research is unlikely to alter this recommendation
This recommendation applies to patients with or without imaging evidence of osteoarthritis, mechanical symptoms, or sudden symptom onset
Healthcare administrators and funders may use the number of arthroscopies performed in patients with degenerative knee disease as an indicator of quality care.
Knee arthroscopy is the most common orthopaedic procedure in countries with available data
This Rapid Recommendation package was triggered by a randomised controlled trial published in The BMJ in June 2016 which found that, among patients with a degenerative medial meniscus tear, knee arthroscopy was no better than exercise therapy
What is the role of arthroscopic surgery in degenerative knee disease? An expert panel produced these recommendations based on a linked systematic review triggered by a randomised trial published in The BMJ in June 2016, which found that, among patients with a degenerative medial meniscus tear, knee arthroscopy was no better than exercise therapy. The panel make a strong recommendation against arthroscopy for degenerative knee disease.


Box 1 shows all of the articles and evidence linked in this Rapid Recommendation package. The infographic provides an overview of the absolute benefits and harms of arthroscopy in standard GRADE format. Table 1 below shows any evidence that has emerged since the publication of this article.
Linked articles in this BMJ Rapid Recommendations cluster
Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ 2017;257:j1982. doi:10.1136/bmj.j1982
Summary of the results from the Rapid Recommendation process
Brignardello-Peterson R, Guyatt GH, Schandelmaier S, et al. Knee arthroscopy versus conservative management in patients with degenerative knee disease: a systematic review. BMJ Open 2017;7:e016114. doi:10.1136/bmjopen-2017-016114
Review of all available randomised trials that assessed the benefits of knee arthroscopy compared with non-operative care and observational studies that assessed risks
Devji T, Guyatt GH, Lytvyn L, et al. Application of minimal important differences in degenerative knee disease outcomes: a systematic review and case study to inform BMJ Rapid Recommendations. BMJ Open 2017;7:e015587. doi:10.1136/bmjopen-2016-015587
Review addressing what level of individual change on a given scale is important to patients (minimally important difference). The study informed sensitivity analyses for the review on net benefit, informed discussions on patient values and preferences, and was key to interpreting the magnitude of effect sizes and the strength of the recommendation
MAGICapp (www.magicapp.org)
Expanded version of the results with multilayered recommendations, evidence summaries, and decision aids for use on all devices
New evidence which has emerged after initial publication
Current practice
Approximately 25% of people older than 50 years experience knee pain from degenerative knee disease (box 2).1 2 Management options include watchful waiting, weight loss if overweight, a variety of interventions led by physical therapists, exercise, oral or topical pain medications such as non-steroidal anti-inflammatory drugs, intra-articular corticosteroid and other injections, arthroscopic knee surgery, and knee replacement or osteotomy. The preferred combination or sequence of these options is not clear and probably varies between patients.
What is degenerative knee disease?
Degenerative knee disease is an inclusive term, which many consider synonymous with osteoarthritis. We use the term degenerative knee disease to explicitly include patients with knee pain, particularly if they are >35 years old, with or without:
Imaging evidence of osteoarthritis
Meniscus tears
Locking, clicking, or other mechanical symptoms except persistent objective locked knee
Acute or subacute onset of symptoms
Most people with degenerative arthritis have at least one of these characteristics.14 The term degenerative knee disease does not include patients having recent debut of their symptoms after a major knee trauma with acute onset of joint swelling (such as haemarthrosis)
Knee replacement is the only definitive therapy, but it is reserved for patients with severe disease after non-operative management has been unsuccessful.3 4 Some believe that arthroscopic debridement, including washout of intra-articular debris, with or without arthroscopic partial meniscectomy to remove damaged meniscus, may improve pain and function.
Current guidelines generally discourage arthroscopy for patients with clear radiographic evidence of osteoarthritis alone, but several support or do not make clear statements regarding arthroscopic surgery in other common groups of patients (table 2).
Support from current guidance for arthroscopic surgery in patients with subgroups of degenerative knee disease
Arthroscopic knee surgery for degenerative knee disease is the most common orthopaedic procedure in countries with available data5 and on a global scale is performed more than two million times each year (figure 1).6–9 Arthroscopic procedures for degenerative knee disease cost more than $3bn per year in the US alone.10 A high prevalence of features advocated to respond positively to arthroscopic surgery (such as meniscal tears, mechanical symptoms, and sudden symptom onset) as well as financial incentives may explain why arthroscopic knee surgery continues to be so common despite recommendations against its use for osteoarthritis. Further, patients may be frustrated with their symptoms, having tried several less invasive management strategies by the time that they see the surgeon, and in many cases this may come with an expectation for surgical management. Moreover, many patients experience important and marked improvements after arthroscopy, which may be erroneously attributed to the effects of the procedure itself instead of the natural course of the disease, co-interventions, or placebo effects.

Population adjusted trends in frequency of knee arthroscopy; percent. Arthroscopic knee surgery remains common despite accumulating evidence suggesting little benefit.
The evidence
The panel requested two systematic reviews to inform the recommendation.11 12
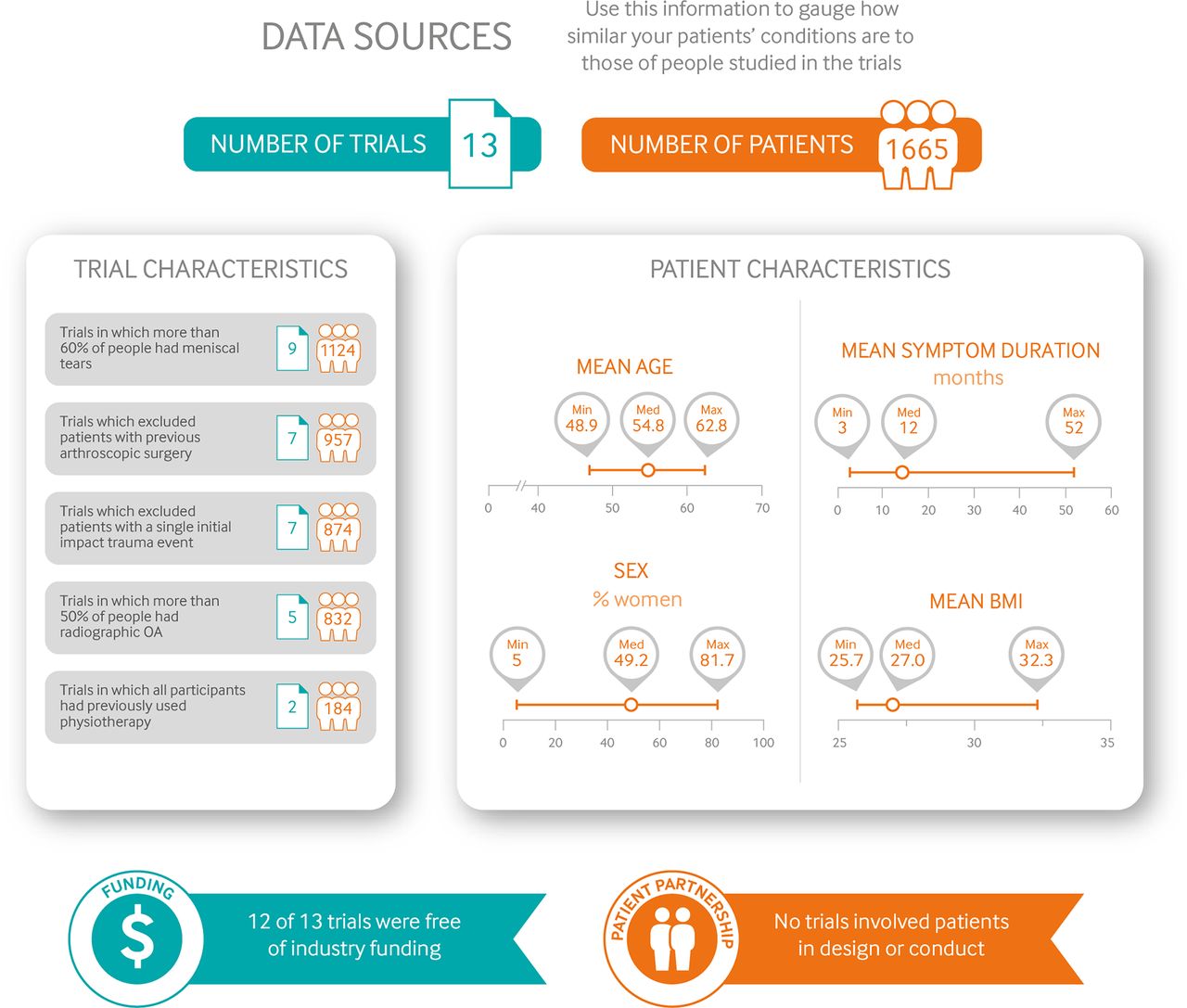
The systematic review on the net benefit of knee arthroscopy compared with non-operative care pools data from 13 randomised trials for benefit outcomes (1668 patients) and an additional 12 observational studies for complications (>1.8 million patients).12 Figure 2 gives an overview of the patients included, the study funding, and patient involvement in the design of the studies.

Characteristics of patients and trials included in systematic review of arthroscopic knee surgery.
Panel members identified three outcomespain, function, and quality of lifeas the most important for patients with degenerative knee disease who are considering surgery. Although the included studies reported these patient-important outcomes, it is difficult to know whether changes recorded on an instrument measuring subjective symptoms are important to those with symptomsfor example, a ch ange of three points might have completely different meanings in two different pain scales.
Therefore, a second team performed a linked systematic review addressing what level of individual change on a given scale is important to patients,11 a characteristic called the minimally important difference (MID).13 The study identified a range of credible MIDs for each key outcome; this range of MID estimates informed sensitivity analyses for the review on net benefit, informed discussions on the patient values and preferences, and was key to interpreting the magnitude of effect sizes as well as the strength of the recommendation.11
Understanding the recommendations
The infographic provides an overview of the benefits and harms of arthroscopy in standard GRADE format. Estimates of baseline risk for effects comes from the control arms of the trials; for complications, comparator risk was assumed to be nil.
The panel is confident that arthroscopic knee surgery does not, on average, result in an improvement in long term pain or function. Most patients will experience an important improvement in pain and function without arthroscopy. However, in <15% of participants, arthroscopic surgery resulted in a small or very small improvement in pain or function at 3 months after surgerythis benefit was not sustained at 1 year. In addition to the burden of undergoing knee arthroscopy (see practical issues below), there are rare but important harms, although the precision in these estimates is uncertain (low quality of evidence).
It is unlikely that new information will change interpretation of the key outcomes of pain, knee function, and quality of life (as implied by high to moderate quality of evidence).
The panel is confident that the randomised controlled trials included adequate representation from groups commonly cited to derive benefit from arthroscopic knee surgery for degenerative knee diseasenotably those with meniscal tears, no or minimal radiographic evidence of osteoarthritis, and those with sudden but non-traumatic symptom onset. Thus the recommendation applies to all or almost all patients with degenerative knee disease. Further, the evidence applies to patients with any severity of mechanical symptoms, with the only possible exception being those who are objectively unable to fully extend their knee (that is, a true locked knee). We did not consider young patients with sports related injuries or patients with major trauma in any age.
Trials that enrolled a majority of patients without radiographic osteoarthritis showed similar effect sizes to trials enrolling patients with radiographic evidence of osteoarthritis. Most of these trials exclusively included patients with meniscus tears. Meniscus tears are common, usually incidental findings, and unlikely to be the cause of knee pain, aching, or stiffness.14 Mechanical symptoms were also a prominent feature for most trial participants, and many had sudden or subacute onset of symptoms.15–18 Given that there is evidence of harm and no evidence of important lasting benefit in any subgroup, the panel believes that the burden of proof rests with those who suggest benefit for any other particular subgroup before arthroscopic surgery is routinely performed in any subgroup of patients.
Practical issues
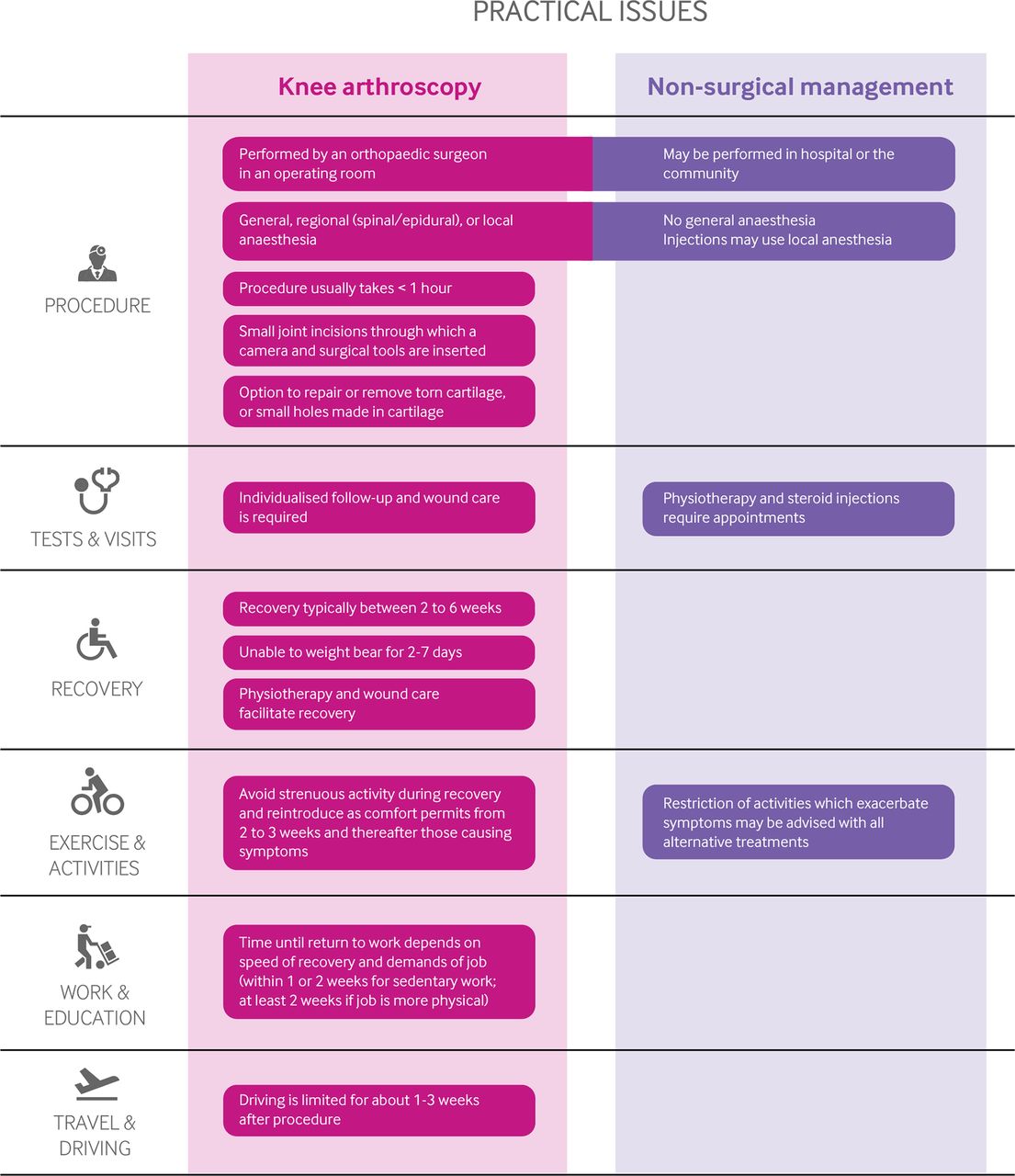
It takes between two and 6 weeks to recover from arthroscopy, during which time patients may experience pain, swelling, and limited function.19 20 Most patients cannot bear full weight on the leg (that is, they may need crutches) in the first week after surgery, and driving or physical activity is limited during the recovery period.19 Figure 3 outlines the key practical issues for those considering arthroscopic knee surgery versus non-surgical management for degenerative knee disease.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Practical issues about use of arthroscopic knee surgery versus non-surgical management for degenerative knee disease.
Degenerative knee disease is a chronic condition in which symptoms fluctuate. On average, pain tends to improve over time after seeing a physician for pain,12 21 and delaying knee replacement is encouraged when possible.3
Values and preferences
Our strong recommendation against arthroscopy reflects a low value on a modest probability (<15%) of small or very small improvement in short term pain and function that does not persist to 1 year, and a higher value on avoiding the burden, postoperative limitations, and rare serious adverse effects associated with knee arthroscopy. The panel, including the patient participants, felt that almost all patients would share these values. The recommendation is not applicable to patients who do not share these values (that is, those who place a high value on a small, uncertain, and transient reduction in pain and function, and a low value on avoiding the burden and postoperative limitation associated with arthroscopy).
Costs and resources
The panel focused on the patient perspective rather than that of society when formulating the recommendation. However, implementation of this recommendation will almost certainly result in considerable cost savings for health funders. A rigorous economic analysis found that knee arthroscopy for degenerative knee disease is not close to cost effective by traditional standards, even in extreme scenarios that assume a benefit with arthroscopy.22 The panel made a strong recommendation against arthroscopy, which applies to almost all patients with degenerative knee disease, implying that non-use of knee arthroscopy can be used as a performance measure or tied to health funding.23
Future research
Key research questions to inform decision makers and future guidelines are:
Randomised trials—Does arthroscopic knee surgery benefit patients who are objectively unable to fully extend their knee or who have persistent, severe, and frequent mechanical symptoms?
Implementation studies—What are the most effective ways to reduce the overuse of arthroscopic surgery for degenerative knee disease?
Updates to this article
Table 1 shows evidence which has emerged since the publication of this article. As new evidence is published, a group will assess the new evidence and make a judgement on to what extent it is expected to alter the recommendation.
How patients were involved in the creation of this article
Three people with lived experience of osteoarthritis, one of whom had arthroscopic knee surgery, were full panel members. These panel members identified important outcomes and led the discussion on values and preferences. Pain was weighed as higher importance for most patients: for example, the patient panel members felt that a possible small benefit to function without a reduction in pain would be unimportant to almost all patients. Those with lived experience identified key practical issues including concerns with cost and accessibility for both arthroscopy and interventions provided by physiotherapists. The members participated in the teleconferences and email discussions and met all authorship criteria.
How the recommendation was created
A randomised controlled trial published in The BMJ in June 2016 found that, among patients with a degenerative medial meniscus tear, knee arthroscopy was no better than exercise therapy.32 This study adds to the body of evidence suggesting that the benefits of arthroscopy may not outweigh the burden and risks.33 34 The RapidRecs executive felt that the study, when considered in context of the full body of evidence, might change practice.35
Our international panel including orthopaedic surgeons, a rheumatologist, physiotherapists, a general practitioner, general internists, epidemiologists, methodologists, and people with lived experience of degenerative knee disease (including those who had undergone and those who had not undergone arthroscopy) met to discuss the evidence. No person had financial conflicts of interest; intellectual and professional conflicts were minimised and managed (see online appendix 1 on bmj.com).
The panel followed the BMJ Rapid Recommendations procedures for creating a trustworthy recommendation35 36 and used the GRADE approach to critically appraise the evidence and create recommendations (see online appendix 2).37 The panel considered the balance of benefits, harms, and burdens of the procedure, the quality of evidence for each outcome, typical and expected variations in patient values and preferences, and acceptability. Recommendations can be strong or weak, for or against a course of action.
Supplementary Appendix 1
Education into practice
Project: how many arthroscopic procedures are scheduled in your organisation for degenerative knee disease?
Based on the information you have read in this article or in this package of Rapid Recommendation articles, is there anything which you might alter your practice?
To what extent might you use information in this article to alter the conversations you have with patients with degenerative knee disease, or those considering arthroscopic surgery?
Acknowledgments
We thank Alison Hoens for critical review of the recommendation and manuscript. We also thank Tahira Devji for expertly leading the systematic review of minimally important differences.
References
Footnotes
Disclaimer This infographic is not a validated clinical decision aid. This information is provided without any representations, conditions or warranties that it is accurate or up to date. BMJ and its licensors assume no responsibility for any aspect of treatment administered with the aid of this information. Any reliance placed on this information is strictly at the user’s own risk. For the full disclaimer wording see BMJ’s terms and conditions.
Competing interests All authors have completed the BMJ Rapid Recommendations interests disclosure form, and a detailed, contextualised description of all disclosures is reported in appendix 1. As with all BMJ Rapid Recommendations, the executive team and The BMJ judged that no panel member had any financial conflict of interest. Professional and academic interests are minimised as much as possible, while maintaining necessary expertise on the panel to make fully informed decisions.
Provenance and peer review Not commissioned; externally peer reviewed.