Article Text

Abstract
Objective To evaluate extracorporeal shockwave therapy (ESWT) in treating Achilles tendinopathy (AT), greater trochanteric pain syndrome (GTPS), medial tibial stress syndrome (MTSS), patellar tendinopathy (PT) and proximal hamstring tendinopathy (PHT).
Design Systematic review.
Eligibility criteria Randomised and non-randomised studies assessing ESWT in patients with AT, GTPS, MTSS, PT and PHT were included. Risk of bias and quality of studies were evaluated.
Results Moderate-level evidence suggests (1) no difference between focused ESWT and placebo ESWT at short and mid-term in PT and (2) radial ESWT is superior to conservative treatment at short, mid and long term in PHT. Low-level evidence suggests that ESWT (1) is comparable to eccentric training, but superior to wait-and-see policy at 4 months in mid-portion AT; (2) is superior to eccentric training at 4 months in insertional AT; (3) less effective than corticosteroid injection at short term, but ESWT produced superior results at mid and long term in GTPS; (4) produced comparable results to control treatment at long term in GTPS; and (5) is superior to control conservative treatment at long term in PT. Regarding the rest of the results, there was only very low or no level of evidence. 13 studies showed high risk of bias largely due to methodology, blinding and reporting.
Conclusion Low level of evidence suggests that ESWT may be effective for some lower limb conditions in all phases of the rehabilitation.
- Tendinopathy
- Shockwave
- Shin Splints
- Review
- Intervention effectiveness
Statistics from Altmetric.com
Introduction
Extracorporeal shockwave therapy (ESWT) is often used in the management of common lower limb conditions. These include Achilles tendinopathy1–15 (AT), greater trochanteric pain syndrome16 17 (GTPS), medial tibial stress syndrome18–20 (MTSS), patellar tendinopathy10 21–30 (PT) and proximal hamstring tendinopathy31 (PHT).
As with primary research studies, systematic reviews vary greatly in quality and clarity of reporting. With the aim to address suboptimal reporting and improve the quality of systematic reviews, guidelines have been published, such as the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) statement.32 Recently, several systematic reviews of the effectiveness of ESWT have been published which did not adhere to these recommendations.33–35 In addition, in systematic reviews evaluating ESWT effectiveness several types of biases can be identified. Selective reporting of complete studies (eg, publication bias) and inclusion of only studies in English language (eg, language bias) are the most frequent types of bias36 found in the majority of these reviews33–35 37–39 while a minority of them meet these quality requirements.40 It is also noted that a relatively large body of evidence is mainly driven and established by the quality assessment tools. The arbitrary selection of quality assessment tools (ie, risk of bias tool, Downs and Black checklist, Jadad score), along with poor reporting41 and differences in inclusion and exclusion criteria, leads systematic reviews to inconsistent conclusions and recommendations.34 37 42
Taking this into account, this review intended to evaluate the short term (≤3 months), mid-term (3 to <12 months) and long term (≥12 months) effectiveness of ESWT in the treatment of AT, GTPS, MTSS, PT and PHT by following published guidelines, robust quality assessment criteria, well-described measures of treatment effect and an established approach for quality of evidence and recommendations. A secondary objective was to document, where possible, the specifics of successful ESWT parameters in the conditions under investigation.
Materials and methods
We adhered to the PRISMA guidelines32 in search strategy and reporting, and followed guidance of Cochrane Handbook for Systematic Reviews 36 for the preparation of this intervention review.
Eligibility criteria
Types of studies
We included randomised and non-randomised studies at the initial selection. Criteria for qualitative and quantitative synthesis are stated below. No limit on language or publication year was imposed to minimise language and publication bias. No minimal duration of follow-up was considered for inclusion.
Type of participants
The population consists of patients suffering from AT, GTPS, MTSS, PT and PHT. We included adult patients of both sexes, involved in all types of activities, and we set no limit for duration of symptoms.
Types of intervention
We included studies on radial or focused ESWT, high or low energy, or studies where ESWT was used as a monotherapy or as an additive intervention.
Types of outcome measures
The effectiveness of ESWT was evaluated in terms of improvement in function, patient-perceived recovery and pain reduction. Follow-up was categorised into short term (≤3 months), mid-term (3 to <12 months) and long term (≥12 months), as recommended by the 2009 updated Method Guidelines for Systematic Reviews of Cochrane group.36
Eligible studies evaluated at least one of the main clinically relevant outcome measures using a valid instrument. The only secondary outcome that was used was time to recovery where non-condition-specific scales were available (ie, MTSS) and the predefined primary outcome measures were compared, as mentioned below.
Previous systematic reviews34 35 37 42 43 of ESWT in the management of lower limb conditions have typically reported treatment effects in terms of standardised mean differences (SMDs) or were unable to pool data due to heterogeneity of studies. In addition, we suggest that treatment effects need to be presented in with reference to the patient’s perspective, and as such we propose that outcomes should be also reported in patient-specific terms44 (rather than statistically derived outcomes which may or may not be associated with the patient’s experience). The patient’s experience of change in pain (‘improvement’ or ‘worsening’) is seen to vary according to their baseline levels of pain such that a reduction of one point on a pain scale is perceived differently if your baseline level is 9 or 3, for example. Two approaches are documented attempting to overcome these limitations. Some researchers advocate using a percentage reduction as denoting clinically meaningful change in pain as, for example, Ostelo et al.45 Alternately Farrar et al 44 examined both the numeric rating scale (NRS) pain change and the individual patient’s rating of the change in pain on a seven-point Likert scale. This scale ranged from ‘very much improved’ to ‘very much worsened’. They showed that the patient rating was not distributed equally across the categorisations when adjusting for the baseline level of pain.
Accordingly, this systematic review also aims to document the outcomes of ESWT and evaluate the effect in terms of the patient-reported benefit. To accomplish that, we considered absolute change in pain when adjusting for baseline levels of pain (see measures of treatment effect section).44 It should be recalled that in the presence of high enough sample size and/or low enough variance, even a reduction in pain of 0.5/10 can be considered statistically significant when this is clearly clinically meaningless. Further in the presence of a high baseline level of pain, such a reduction is actually perceived by the patient as a clinical worsening after an intervention,44 hence reporting these changes according to patient rating is seen as more clinically applicable.
Primary outcomes
functional disability (eg, Victorian Institute of Sports Assessment–achilles questionnaire (VISA-A),46 Victorian Institute of Sports Assessment–patella questionnaire (VISA-P)47)
self-perceived recovery
pain reduction in visual analogue scale (VAS) or NRS
Information sources and search methods
A systematic search was undertaken on 15 August 2016 adhering to the PRISMA guidelines32 using the following databases: MEDLINE, CINAHL Plus, EMBASE, Web of Science and the Cochrane Library. Grey literature was searched via OpenGrey as were the following clinical trial registries: EU Clinical trials Register, Clinical Trials.gov, WHO International Clinical Trials Registry Platform and Australian New Zealand Clinical Trials registry. The basic search strategy is presented in online supplementary appendix 1.
Supplementary_Appendix_1
Additionally, reference lists and citation tracking results were also reviewed. Systematic reviews were not included or assessed for quality, but were examined for possible references.
Study selection
Two reviewers independently identified relevant titles and abstracts in two different search sessions. A third reviewer was consulted if consensus was not reached and full text was obtained if necessary.
Data collection, extraction and analysis
We categorised retrieved studies into three groups: randomised controlled trials (RCTs), non-randomised controlled studies (both used in quantitative synthesis) and prospective/retrospective non-controlled trials (used only in qualitative evaluation).
All data describing study characteristics such as study design, quality and risk of bias assessment, demographics and numbers of participants, interventions and co-interventions, treatment protocol, primary and secondary outcomes, follow-up time and main results were extracted and presented.
Data were entered into and analysed using Review Manager V.5.3 statistical software of the Nordic Cochrane Collaboration.48
Assessment of quality and risk of bias
Two independent reviewers assessed risk of bias using the criteria advised by the Cochrane Review Group for evaluation of RCTs.36 As this list is not suitable for assessment of non-randomised studies, in agreement with the recommendations provided by the Cochrane non-randomised studies methods group,49 we selected a modified Downs and Black checklist50 to evaluate the non-randomised studies. Both lists are designed to assess the internal validity of the studies. Justification for each selection/scoring in both risk of bias tool and Downs and Black checklist is presented in supplementary appendices 2 and 3. An estimate of correlation between these tools in terms of study quality was calculated.
Risk of bias was assessed with a modification of the Cochrane Risk of Bias tool. The tool used expanded the 7 main domains and comprises 13 items; however for ESWT, it is currently impractical to expect blinding of participants or care providers. Accordingly, arbitrarily the review authors rated studies as having low risk of bias if at least seven of the criteria were met and the study had no serious flaws (ie, excessive drop-out rate, extremely small sample size—<15 per group). Descriptions of the scoring and reasons are available in online supplementary appendix 2.
Supplementary Appendix 2
The modified Downs and Black checklist consists of 27 items, with a total possible score of 28 for randomised and 25 for non-randomised studies and has been proven valid and consistent among reviewers.50 In the present version of the checklist, we modified the scoring of item 27 that refers to the power of the study. Instead of rating according to an available range of study powers, we rated whether the study or not performed power calculation. Accordingly, the maximum score for item 27 was 1 (a power analysis was conducted) instead of 5 and thus the highest possible score for the checklist was 28 (instead of 32). Downs and Black score ranges were given corresponding quality levels as previously reported51: excellent (26–28), good (20–25), fair (15–19) and poor (≤14) (see online supplementary appendix 3).
Supplementary Appendix 3
In non-randomised trials, the use of allocation mechanism predisposes outcomes to be subject to confounding. The characteristics considered for confounding such as age, gender, duration of symptoms and baseline symptoms were taken into consideration in heterogeneity assessment in order to pool data.49
The review authors discussed differences in scoring of the risk of bias and Downs and Black assessment during consensus meeting and consulted a third reviewer when necessary.
Measures of treatment effect, assessment of heterogeneity and data synthesis
Differences on the primary outcome measures between the ESWT and control groups and the patient rating of clinical effectiveness were defined as treatment effects.
We presented comparisons of continuous data as mean differences (MDs) with corresponding CIs. Continuous data were compared directly or by calculation of SMDs if outcome measures were not directly comparable due to different measurement scales used. For dichotomous data , the effect measure calculated was ORs with 95% CIs.
We assessed the included studies first for the more important clinical heterogeneity and then for statistical heterogeneity.52 Clinical heterogeneity was evaluated for variability in duration of symptoms, patient age and baseline pain and/or functional characteristics with individual assessments examining group means and variance to decide for a combined quantitative analysis. When we judged studies to be clinically homogenous, we tested statistical homogeneity. If there were >10 studies available, a meta-regression was performed.36
Evaluation of heterogeneity in order to pool data was not judged only by the value of I2 statistic, as thresholds for the interpretation can be misleading.53 Since clinical and methodological diversity always occur in quantitative synthesis, statistical heterogeneity is inevitable.52 Statistical heterogeneity was assessed as follows: (1) overlap (poor or adequate) of CIs presented in forest plots36; (2) magnitude and direction of effects36; (3) sample sizes and number of studies included (as small number of participants and/or studies included in analysis results in low power of heterogeneity test)53; and (4) strength of evidence for heterogeneity (p value from χ2 test or CI for I2).36
We aimed to use minimal clinically important difference (MCID) in order to measure clinically relevant treatment effect. Unfortunately, to date there is no consensus on MCID in pain and functional outcomes in AT and PT. Finally, there is no consistent use of condition-specific outcome measures among studies, and no available condition-specific outcome measures for GTPS, MTSS and PHT at the time that these studies were conducted. The treatment effects, therefore, were measured as follows:
We defined MCID for VISA-P a mean 15-point change and for Harris hip score (HHS) a mean 10-point change based on studies assessing clinimetric properties of the scales.54–56
MCID for VISA-A has been reported57 to be 6.5 points; based on available data,58 59 we arbitrary increased this cut-off point to 12 points.
We employed the methods of Overdevest et al 60 in setting the MCID to a 30% improvement from the mean of the baseline level of pain. This corresponded to 1.5 points on a VAS and 2.0 points on an NRS for the data examined here.
To estimate the patient-rated clinical effectiveness, previously described thresholds for change in pain scores were used, with appropriate adjustment for baseline levels of pain (6, 7 and 8/10 baseline pain).44 Since the data from the study of Farrar et al 44 were not normally distributed, the appropriate group estimator was the median. Accordingly, treatment outcomes were classified in line with the closest median for each category. Specifically, the median values for the six categorisations of change in pain were as follows: ‘much worse’≥+0.32/10; ‘minimally worse’≤−0.08/10; ‘no change’≤−0.20/10; ‘minimally improved’≤−1.07/10; ‘much improved’≤−2.69/10; and ‘very much improved’≤−4.15/10. We pooled results if they were judged to be sufficiently homogenous (methodologically and statistically).
We evaluated the quality of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.61 The adapted following criteria were used: (1) 75% of studies have low risk of bias (≥7 items of risk of bias tool met); (2) included studies have relatively consistent findings; (3) included population adequately reflects selection criteria of the review; (4) results are based on direct and indirect comparison, as usually ESWT is not used as a monotherapy in clinical practice (studies with indirect comparison were automatically downgraded); (5) estimate of effect is sufficiently precise (CI is narrow and conclusive); and (6) analysis is free of publication bias.
Additionally, regarding non-randomised trials,49 we selected only prospective controlled studies and a priori their level of evidence was set as ‘low’. All the following criteria49 were used for non-randomised studies in order to be included in quantitative synthesis: (1) reasonably resistant to biases (selection bias—within-study and between-study differences between patients in different groups, sample representative of population, which parts of the study were prospectively designed, potential confounders; detection bias—patient-reported outcomes; attrition bias); (2) Downs and Black score >20 (good quality); (3) relatively homogeneous with included RCTs (confounders, population, intervention, outcomes); (4) intervention and control group matched for at least age, duration of symptoms and pain and/or functional status; and (5) investigating long-term outcomes.
We used guidelines from Cochrane Collaboration Group36 to assess levels of quality of evidence (table 1). We a priori graded an outcome with only one trial as low quality, and if it also had high risk of bias the evidence was graded as very low quality.61
Guidelines used from Cochrane Collaboration Group and Grading of Recommendations Assessment, Development and Evaluation (GRADE) system of evaluation
Results were presented as summary tables and forest plots with total and subtotal values where applicable (see online supplementary appendix 4). Forest plots are presented only if aggregate, pooled estimates meet the predefined homogeneity criteria. If only one study with low risk of bias was found, we depicted the effect in a singular forest plot of the outcome parameter. A suggested protocol was presented where possible, based on ESWT parameters used and extracted form high-quality studies with favourable outcomes for ESWT.
Supplementary Appendix 4
Additional analyses
The robustness of our results was tested through a sensitivity analysis. We performed analyses to investigate various aspects of trial and review methodology. These included assessing the impact of (1) using solely high-quality studies with using studies of low, medium and high quality combined; (2) using fixed-effects versus random-effects models; and (3) using SMD instead of MD for pooling (see online supplementary appendix 5).
Supplementary appendix 5
Results
Results of the search
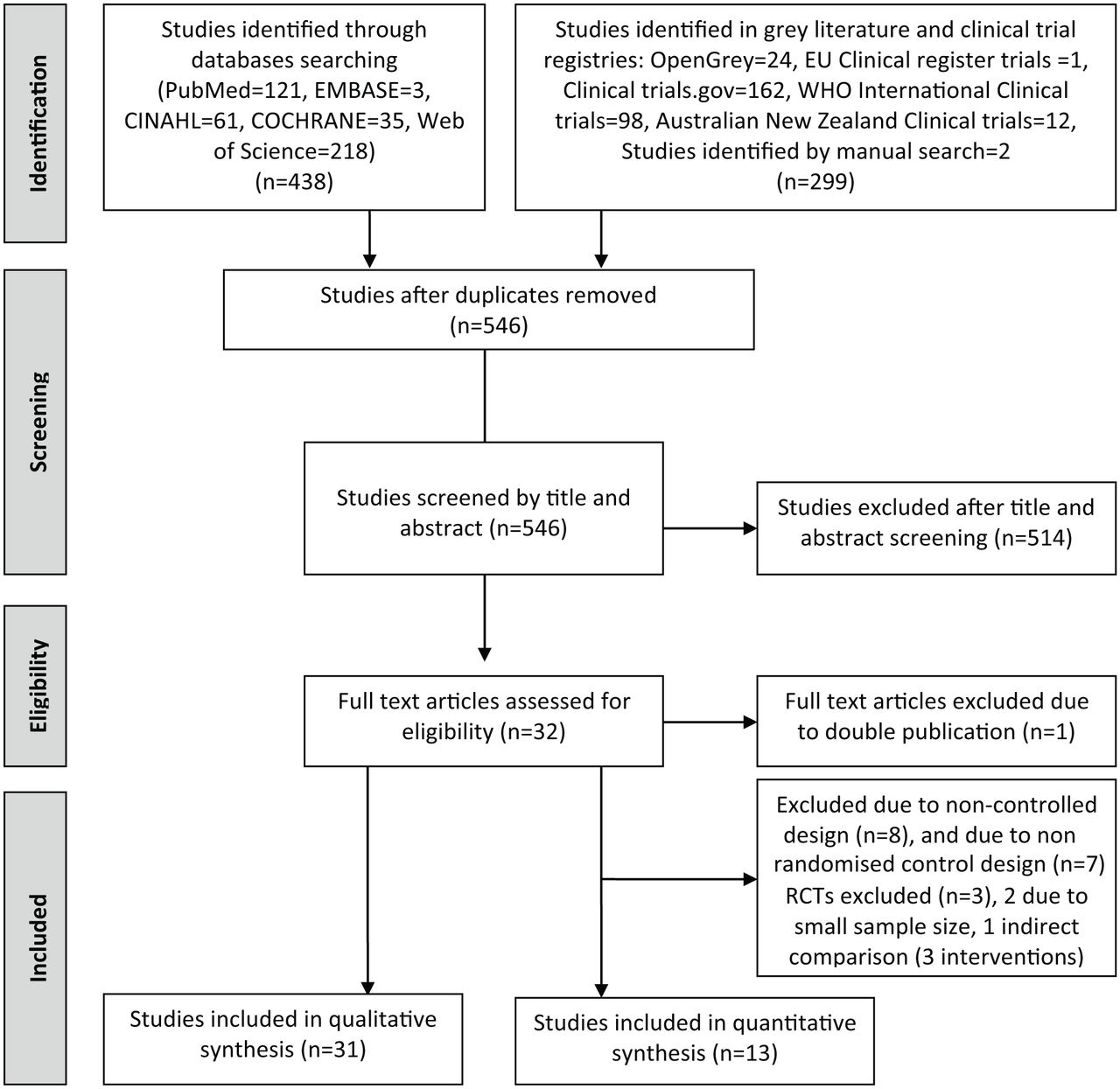
The literature search up to 15 August 2016 yielded 736 articles and manual search added 2 studies. Once duplicates were removed, 546 studies were assessed for eligibility from the title and abstract, which revealed 32 suitable studies for quality assessment (figure 1). One study62 was excluded after full-text assessment as double publication. Agreement on article eligibility between the two reviewers was 100% (n=31).

The Preferred Reporting Items for Systematic reviews and Meta-analyses flow diagram of study selection process.
An overview network representation of all the primary controlled studies is presented in figure 2. The diagram depicts the results of all the studies before assessment of quality and evaluation for inclusion in quantitative synthesis. The network diagram stands as an overview of all available studies that have investigated the effects of ESWT compared with other interventions in patients with lower limb pathologies.

Network comparisons of extracorporeal shockwave therapy (ESWT) interventions for common low limb pathologies. The size of pie part represents the total number of participants having received ESWT as a primary intervention. The direction of the arrowhead on the lines (solid or dashed) indicates the intervention with known superior effect over the comparator. The different size and type of the line represent the time of follow-up (short term, mid-term and long term) as depicted in the legend of the figure. The dotted line without arrowhead represents head-to-head comparisons reported in the literature but with no clear benefit of one intervention over another. AT, Achilles tendinopathy; Ecc, eccentric training; GTPS, greater trochanteric pain syndrome; HT, home training; MTSS, medial tibial stress syndrome; PHT, proximal hamstring tendinopathy; PRP, platelet-rich plasma; PT, patellar tendinopathy; Running, graded running programme; Suppl, dietary supplements; Wait, wait-and-see policy.
Characteristics, quality and risk of bias of included and excluded studies
Study design, study level of evidence, risk of bias, total Downs and Black scores, sample size, age of the participants, interventions, ESWT protocol, length of follow-up, outcome measures and main results of the studies meeting the eligibility criteria for qualitative synthesis are presented inonline supplementary table 2. Thirty-one studies1–31 published between 2002 and 2016 involving a total of 1847 participants were included in qualitative analysis. Quality assessment, risk of bias and justification for selection/scoring of each individual study are presented in online supplementary appendices 2 and 3. Out of the 31 studies assessed, only 12 RCTs4 6 7 14 15 17 25–27 29–31 and 1 non-randomised controlled study16 met the inclusion criteria for quantitative synthesis.
Supplementary Table
Risk of bias and quality assessment of included studies
All included studies had low risk of bias, having met at least seven of the risk of bias criteria. Poor performance on the risk of bias assessment (figure 3) was the result of methodology, blinding and reporting. Assessment of the tools used showed a poor correlation between risk of bias and Downs and Black checklist (r=0.5).

Summary of risk of bias for 151 4 6 7 14 15 17 20 22 25–27 29–31 eligible studies for bias assessment. Note that eight studies8–13 23 24 without a comparator intervention were not assessed with the risk of bias tool, as well as eight case–control studies.2 3 5 16 18 19 21 28
Synthesis of results
Patient-rated pain reduction for clinical effectiveness
To estimate the patient-rated clinical effectiveness, previously described thresholds for change in pain scores were used, with appropriate adjustment for baseline levels of pain (6, 7 and 8/10 baseline pain).44 For a clinically meaningful interpretation of results, a graphical representation of change in pain scores for ESWT and control groups for different pathologies is presented in figure 4. The cut-off points for the six categorisations of change in pain were as follows: ‘much worse’≥+0.32/10; ‘minimally worse’≤−0.08/10; ‘no change’≤−0.20/10; ‘minimally improved’≤−1.07/10; ‘much improved’≤−2.69/10; and ‘very much improved’≤−4.15/10.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graphical representation of clinically meaningful patient-rated change in pain for extracorporeal shockwave therapy (ESWT) (black shapes) and control groups (white shapes) at different time points of follow-up. Time points are categorised as short term: ≤3 months; mid-term: 3–12 months; long term:≥12 months. Change in pain is represented on the left vertical axis with negative values indicating an improvement in pain, that is, a reduction in visual analogue scale (VAS)/numeric rating scale (NRS). The right vertical axis depicts the patient-reported descriptors associated with these changes in pain.
Mid-portion AT
Studies assessing the effectiveness of ESWT in AT were subgrouped into three categories according to the diagnosis patients received during inclusion in each study: mid-portion tendinopathy, insertional tendinopathy or mixed/non-specified.63
Included and excluded studies
Four studies5–7 9 assessed the effectiveness of ESWT in mid-portion AT (see online supplementary table 2). One fair quality prospective study9 reporting favourable pain and functional outcomes with ESWT was excluded due to non-controlled design. One non-randomised controlled study5 of good quality comparing focused ESWT with traditional non-operative therapy did not meet the inclusion criteria. We excluded this study because of the use of regional block with or without sedation (as this does not reflect standard clinical practice) and possible selection bias in the control group (financial or insurance coverage). This study compared ESWT with traditional non-operative therapy up to 12-month follow-up. Scores in VISA-A, perceived recovery and pain reduction favoured participants in the ESWT group at all follow-up assessments.
Two RCTs6 7 with low risk of bias—one7 of excellent and one6 of good quality assessing the effectiveness of radial ESWT (used same protocol)—met the inclusion criteria for quantitative synthesis. Both studies performed analyses according to the intention-to-treat principle. The duration of follow-up for both was 4 months, the mean age of the participants ranged from 46.2 to 53.1 years and the mean duration of symptoms varied from 9.2 months to 16 months (online supplementary table 2). The definition of mid-portion AT was pain over the main body of Achilles tendon 2–6 cm proximal to its insertion, swelling and impaired function. Both studies included patients with a history of AT for at least 6 months and failure of non-operative management.6 7 A total number of 143 patients were randomised into ESWT, ESWT additive to eccentric loading, eccentric loading or wait-and-see policy groups.
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 2. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
Mid-portion Achilles tendinopathy summary of evidence
Conclusion and recommendations
Low level of evidence:
Radial ESWT is comparable to eccentric training at mid-term follow-up (4 months) for VISA-A, pain scores, self-perceived recovery and patient rating of pain reduction (both much improved).
Radial ESWT is superior to a wait-and-see policy at mid-term follow-up (4 months) for disability scores, pain, self-perceived recovery and patient rating of pain reduction (much improved compared with minimally improved).
Very low level of evidence:
Radial ESWT combined with eccentric training is superior to eccentric training alone at mid-term follow-up (4 months) for VISA-A scores, self-perceived recovery and patient-rated pain reduction (very much improved compared with much improved).
Suggested protocol:
By using radial ESWT, deliver 2000 impulses at three bars (energy flux density 0.1 mJ/mm2) at 8 Hz for three sessions at weekly intervals.
Insertional AT
Included and excluded studies
Four studies1–4 evaluated focused or radial ESWT in patients with insertional AT. Two non-randomised controlled studies2 3 (see online supplementary table 2) were excluded: one2 assessing focused ESWT compared with surgery due to poor quality, and the other3 evaluating effectiveness of focused ESWT compared with orthoses, non-steroidal anti-inflammatory drugs (NSAID), massage, physiotherapy, stretching, strengthening, ultrasound, ice, iontophoresis, contrast baths and immobilisation because of fair quality, selection bias of the control group (insurance coverage) and the possibility of author’s conflict of interest. Finally, we excluded an RCT1 with low risk of bias due to indirectness of comparison (three domains of intervention; ESWT, eccentric loading and dietary supplements).
Only one RCT4 with low risk of bias, assessing the effectiveness of radial ESWT compared with eccentric loading in a total of 50 patients, met the inclusion criteria. The study was performed on an intention-to-treat basis. The duration of follow-up was 4 months, the mean age of the participants ranged from 39.2 to 40.4 years and the mean duration of symptoms varied from 24.8 months to 26.3 months (see online supplementary table 2). The definition of insertional AT was localised pain over the distal part of Achilles tendon at its insertion onto the calcaneus, with local tenderness, and reduced levels of activity. The study included patients with a history of AT for at least 6 months and failure of non-operative management.4
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 3. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
Insertional Achilles tendinopathy summary of evidence
Conclusion and recommendations
Low level of evidence:
Radial ESWT is superior to eccentric training at mid-term follow-up (4 months) for disability scores, pain, self-perceived recovery and patient rating of pain reduction (much improved compared with minimally improved).
Suggested protocol:
By using radial ESWT deliver 2000 impulses at 2.5 bars (energy flux density 0.12 mJ/mm2) at 8 Hz for three sessions at weekly intervals.
Mixed/non-specified AT
Included and excluded studies
Five prospective non-controlled studies8 10–13 of fair and poor quality (online supplementary table 2) were excluded from quantitative synthesis. Most non-controlled studies reported significant improvement at pain and/or functional scores at the long-term follow-up (≥12 months).8 10–12 Only one study13 reported pain reduction in favour of ESWT at 12 month follow-up, better results in non-insertional AT compared with insertional, but no significant improvement at 2-year follow-up.
Two RCTs14 15 with low risk of bias assessing the effectiveness of ESWT in mixed/non-specified groups of patients with AT were included for quantitative synthesis. Both studies used as an inclusion criterion tenderness exacerbated by dorsiflexion of the ankle, but the definition of AT was broad in both reflecting the mixed group of patients included. Both studies performed analyses according to the intention-to-treat principle. The studies enrolled 97 patients, their mean age ranged from 46 to 58.7 years; the follow-up assessment was performed in both at 3 months, but the mean duration of symptoms is reported only in one study14 (varied from 17.8 to 20.8 months). Costa et al 14 compared ESWT with placebo shock wave, while Rasmussen et al 15 used ESWT or placebo additive to stretching and eccentric training.
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 4. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
Mixed/non-specified Achilles tendinopathy summary of evidence
Conclusion and recommendations
Very low level of evidence:
Both radial and focused ESWT are superior to placebo ESWT at short-term follow-up (3 months) for disability scores, but in non-condition-specific outcome measures.
No difference between focused and placebo ESWT in pain reduction, and activities of daily living.
Suggested protocol:
Not applicable due to substantial heterogeneity in studies’ protocols.
Greater trochanteric pain syndrome
Included and excluded studies
One RCT17 with low risk of bias and a good quality non-randomised controlled study16 that met all the predefined criteria were included in quantitative synthesis. Both studies included four comparison groups with a total number of 295 patients with GTPS, of which 111 received radial ESWT, 75 corticosteroid injections, 75 home training programme consisted of strengthening and stretching, and 33 traditional non-operative treatment (ie, stretching and strengthening, physical therapy modalities, iontophoresis, rest). The duration of follow-up for both was ≥12 months, the mean age of the participants ranged from 46 to 51 years and the mean duration of symptoms varied from 11 to 14 months (see online supplementary table 2). In general, definition of GTPS was pain located over and around the greater trochanter area with or without tenderness. Rompe et al 17 in the definition also included positive resisted external hip rotation test, pain while lying on the affected side, and no radiological evidence at hip imaging. Conversely, Furia et al 16 included in the definition pain with resisted hip abduction and impaired function, but for confirmation of diagnosis they used local anaesthetic injection.
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 5. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
Greater trochanteric pain syndrome summary of evidence
Conclusion and recommendations
Very low level of evidence:
Radial ESWT is superior to control treatment (physiotherapy, stretching and strengthening) at short (3 months) and long-term follow-up (12 months) for disability scores (HHS).
Low level of evidence:
Radial ESWT is superior to control treatment (physiotherapy, stretching and strengthening) at short (1–3 months) and mid-term follow-up (4 months) in self-perceived recovery.
Corticosteroid injection is superior to radial ESWT at short-term (1 month) follow-up in self-perceived recovery, pain scores and patient-rated pain reduction.
Radial ESWT is superior to corticosteroid injection at mid-term (4 months) and long-term follow-up (>12 months) in self-perceived recovery, pain scores and patient-rated pain reduction.
Radial ESWT produces comparable results to control treatment (physiotherapy, stretching and strengthening) at long-term follow-up (>12 months) in self-perceived recovery, pain scores and patient-rated pain reduction.
Suggested protocol:
Not applicable due to substantial heterogeneity in studies’ protocols.
Medial tibial stress syndrome
Included and excluded studies
Small sample size in one RCT,20 and study design, methodological limitations and reporting of data in two non-randomised studies18 19 did not allow for a quantitative comparison. Moen et al 18 reported that five sessions of focused ESWT added to a graded running programme reduced significantly the time to full recovery (mean 32 days) compared with the running programme in isolation, as assessed by a treadmill running test. On the contrary, a high-quality, low risk of bias RCT20 that used the same ESWT protocol without additive controlled intervention reported no significant differences at 10-week follow-up between ESWT and sham dose ESWT groups in pain during muscle pressure (patient-rated improvement of ‘no change’ and ‘minimally improved’, respectively), pain-limited distance run and self-perception of change. Interestingly, pain during bone pressure was significantly reduced at the control group compared with the ESWT group at 10-week follow-up (patient-rated improvement of ‘minimally improved’ and ‘no change’, respectively). On the other hand, Rompe et al 19 reported that radial ESWT additive to a standardised home training programme comprising lower limb active range of motion, stretching and strengthening exercises, provided significant benefit in reducing pain and self-perceived global improvement in patients with MTSS. Estimation of patients’ rating showed that adjunct ESWT group and home training group were both ‘minimally improved’ at 1 month.44 Regarding 4 and 15 months follow-up, the reduction of pain was seen to be 4.3 and 5.4 points for the ESWT group compared with 1.6 and 3.2 for the home training group, which were both a patient rating of ‘very much improved’ compared with ‘minimally improved’ and ‘much improved’, respectively.44
Conclusion and recommendations
No evidence for the effectiveness of ESWT in patients with MTSS.
Suggested protocol:
Not applicable.
Patellar tendinopathy
Included and excluded studies
Eleven studies were evaluated for inclusion in quantitative synthesis (see online supplementary table 2). We pooled data from five RCTs25–27 29 30 of low risk of bias by grouping studies with relatively similar comparisons in order to draw clinically meaningful conclusions and evidence. Three prospective non-controlled studies10 23 24 of poor and fair quality presenting positive results from ESWT were excluded from quantitative synthesis. Two fair quality non-randomised controlled studies21 28 were excluded due to retrospective design. One study28 reported favourable results for ESWT compared with conservative treatment at long-term follow-up, and the other21 comparable results between ESWT and surgery at >20 months follow-up. Moreover, an RCT22 with low risk of bias reporting superior results of ESWT compared with placebo shock wave at short term was excluded due to small sample size.
Focused ESWT compared with placebo shock wave
Included and excluded studies
Two multicentre double-blinded RCTs with low risk of bias compared ESWT with placebo shock wave with30 or without25 additive eccentric training. Both studies included a total number of 114 patients with PT, of which 53 received focused ESWT and 61 placebo ESWT with or without eccentric training. Both studies performed analyses according to the intention-to-treat principle. The duration of follow-up for both was >5 months, the mean age of the participants ranged from 24.2 to 30.5 years and the mean duration of symptoms varied from 32 to 99.4 weeks (online supplementary table 2). Definition of PT consisted of localised knee in the patellar tendon related to activity, present for >2 months, palpation tenderness at the corresponding painful area and VISA-P score <80 at baseline.
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 6. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
ESWT compared with placebo shock wave in patellar tendinopathy summary of evidence
Conclusion and recommendations
Moderate level of evidence:
No difference between focused ESWT and placebo ESWT at short (3 months) and mid-term (5–6 months) follow-up in VISA-P, pain scores and patient-rated pain reduction.
Low level of evidence:
No difference between focused ESWT and placebo ESWT in self-perceived recovery.
Suggested protocol:
Not applicable.
Focused ESWT compared with conservative management
Included and excluded studies
Only one RCT26 with low risk of bias met the criteria for qualitative analysis. Wang et al 26 evaluated the effectiveness of focused ESWT compared with conservative treatment consisting of NSAIDs, physiotherapy, exercise programme and the use of knee strap in patients with PT and assessed the functional improvement by using VISA-P questionnaire at 2–3-year follow-up (mean 32.7 months for the ESWT group and 28.6 months for the control group). PT was defined as recurrent pain and tenderness attributable to degenerative changes of the patellar tendon for at least 6 months. The study enrolled 50 patients (54 knees), their mean age ranged from 29.4 to 30.2 years (—online supplementary table 2).
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 7. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
ESWT compared with control conservative management in patellar tendinopathy summary of evidence
Conclusion and recommendations
Low level of evidence:
Focused ESWT is superior to control conservative treatment (NSAID, physiotherapy, exercise, knee strap, modification of activity levels) at long-term follow-up (2–3 years) in VISA-P, self-perceived recovery, pain scores and patient-rated pain reduction.
Suggested protocol:
Not applicable due to substantial heterogeneity in PT studies’ protocols.
Focused ESWT compared with platelet-rich plasma (PRP)
Included and excluded studies
Only one RCT27 with low risk of bias evaluated the effectiveness of focused ESWT compared with PRP injection up to 12-month follow-up. The comparison was indirect as both groups additionally received a standardised stretching and strengthening protocol for 2 weeks post treatment. The study did not provide information regarding the clinical diagnosis of PT, but they used ultrasound to identify proximal tendon anterior–posterior thickening with focal area of hypoechoic change and fibril discontinuity. Forty-six patients were enrolled with a mean age of 27 years, and mean duration of symptoms ranging from 17.6 to 18.9 months (table 2—see online supplementary table 2).
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 8. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
ESWT compared with PRP injection in patellar tendinopathy summary of evidence
Conclusion and recommendations
Very low level of evidence:
Focused ESWT produced comparable results to PRP injection at short-term follow-up (2 months) in VISA-P, self-perceived recovery and pain reduction.
PRP is more effective than focused ESWT at mid-term follow-up (6 months) in VISA-P, pain scores and patient-rated pain reduction.
PRP is more effective than focused ESWT at long-term follow-up (12 months) in VISA-P, self-perceived recovery, pain scores and patient-rated pain reduction.
Suggested protocol:
Not applicable due to substantial heterogeneity in PT studies’ protocols.
Focused ESWT compared with radial ESWT
Included and excluded studies
Only one high-quality study with low risk of bias RCT29 evaluated the effectiveness of focused ESWT compared with radial ESWT at mid-term follow-up. The comparison was indirect as both groups additionally received a standardised eccentric exercise programme that started 2 weeks after the final ESWT session. The study performed analyses according to the intention-to-treat principle. Definition of PT was localised knee pain in the patellar tendon or its insertions related to activity, present for at least 3 months, palpation tenderness at the corresponding painful area and VISA-P score <80 at baseline. In case of doubt in diagnosis, ultrasound and MRI were used to rule out other knee pathologies. The study included 43 patients with PT, with a mean age of 31.1 years, and the mean duration of symptoms was 35.2 months (see online supplementary table 2).
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 9. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
Focused ESWT compared with radial ESWT in patellar tendinopathy summary of evidence
Conclusion and recommendations
Very low level of evidence:
Focused ESWT produces comparable results to radial ESWT in patients with PT that received additive eccentric training at short-term and mid-term follow-up (up to 14 weeks) in VISA-P and pain scores.
Suggested protocol:
Not applicable.
Proximal hamstring tendinopathy
Included and excluded studies
Only one high-quality study with low risk of bias RCT31 evaluated the effectiveness of radial ESWT compared with traditional conservative treatment at 12-month follow-up. The control treatment consisted of rest, NSAIDs, physiotherapy and exercise programme for the last three weeks. The study was based on intention-to-treat principle, enrolled 40 patients with PHT with a mean age range from 23.7 to 24.2 years and mean duration of symptoms ranging from 19.6 to 21 months (online supplementary table 2). The diagnosis was based on relevant pain-provoking clinical testing and MRI. Pathology was defined as abnormalities at the proximal hamstring tendon substance, ill-defined pain, especially while performing sports activities or when sitting, in the ischial tuberosity that radiates distally towards the popliteal fossa.
Effects of interventions
Effects of interventions regarding functional disability, pain reduction, self-perceived recovery and patient-rated pain reduction are presented in table 10. Comparison parameters, forest plots and criteria for quantitative synthesis are presented in detail in online supplementary appendix 4.
ESWT compared with traditional conservative treatment in proximal hamstring tendinopathy summary of evidence
Conclusion and recommendations
Moderate level of evidence:
Radial ESWT produces superior results to conservative treatment (consisted of rest, NSAIDs, physiotherapy, and exercise programme) in patients with PHT at short-term, mid-term and long-term follow-up (up to 12 months) in Nirschl rating scale, self-perceived recovery, pain scores and patient-rated pain reduction.
Conservative treatment consisting of rest, NSAIDs, physiotherapy and exercise programme is not effective for patients with PHT.
Suggested protocol:
Using radial ESWT deliver 2500 impulses at four bars (energy flux density 0.18 mJ/mm2) at 10 Hz for four sessions at weekly intervals.
Additional analyses
Sensitivity analyses did not reveal any significant differences with the results of the present systematic review. None of the approaches examined resulted in a change in direction of the effect in any condition evaluated. Inclusion of low-quality and/or non-randomised controlled studies affected only the magnitude of effect (overestimation). One of these analyses is presented in online supplementary appendix 5.
Discussion
Summary of main findings and clinical interpretation
To date, 31 studies have been published assessing ESWT in lower limb conditions assessed, among which 15 were RCTs.
Mid-portion AT
Low and very low level of evidence suggests that radial ESWT produces equal results with eccentric loading, superior results compared with wait-and-see policy and superior results when combined with eccentric training compared with eccentric training alone, at mid-term follow-up.
Clinically eccentric loading is considered the gold-standard non-operative treatment for mid-portion AT,64 but here it is seen that low-energy ESWT showed equal results in the short term. It is noted however that there are conflicting outcomes when compared with wait-and-see policy outcomes.7 Further, despite ESWT in combination with eccentric loading showing superior results in pain and function compared with eccentric training alone,6 the significance was seen only in functional scores but not in pain reduction.
Insertional AT
Low-level evidence suggests that three sessions of radial ESWT is more effective in functional outcome and pain reduction than eccentric training at mid-term follow-up.
The clinical significance of these results is further supported by the patient-rated improvement in pain reduction.
Mixed non-specified AT
Very low level of evidence suggests that ESWT is no better than placebo shockwave at short-term follow-up in self-perceived recovery and pain reduction. It is noted that effect size calculation was not possible from one study15 due to insufficient data.
Conversely, inconsistent findings were found in function between patients treated with ESWT or placebo ESWT as indicated by American Orthopaedic Foot and Ankle Society score14 and functional index of lower limb activity.15 Two possible confounding factors may explain these inconsistent results: the groups’ age and the treatment protocols. The mean age of ESWT group in the Costa et al 14 study was significantly older than their control group and both groups of the Rasmussen et al 15 study. Furthermore, Costa et al 14 used lower total energy flux density, less sessions and longer (monthly) intervals compared with the treatment protocol used by Rasmussen et al.15 The differences in treatment protocols, along with the use of generic outcome measures for function assessment, may partially explain these results and the inconsistencies in patient-rated pain reduction. We suggest that the sample configuration in these studies raises several considerations that will be discussed below.
Greater trochanteric pain syndrome
Low level of evidence suggests that corticosteroid injection is superior to therapeutic intervention in the short term. Low level of evidence showed that at mid-term and long-term follow-up radial ESWT is more effective than corticosteroid injection and produced comparable results to physiotherapy, stretching and strengthening.
Conflicting evidence exists regarding the short-term effectiveness of ESWT (1 month). Interestingly in the study of Rompe et al,17 in contrast to the study of Furia et al,16 the ESWT group did not present statistically or clinically significant pain reduction at 1 month with a patient rating of ‘no change’.44 By reviewing the demographic data in both studies, there were no significant differences in age and symptom duration among ESWT groups. The difference in ESWT protocol probably could partially explain the differences between the groups, with the major difference being the number of sessions (one compared with three). Furthermore, the lack of clarity in the reporting of the non-operative conservative treatments prevented a meaningful interpretation of the findings between the studies.16 17
The short-term effect of corticosteroid injection disappeared with time providing no benefit in reducing pain or improving function in GTPS at mid-term and long-term follow-up.17 This result was in accordance with several studies demonstrating only the short-term effect of corticosteroid injections in a number of musculoskeletal conditions.65–67 Accordingly, ESWT can be an effective mid-term and a feasible long-term treatment option for patients with GTPS. Inconsistencies between studies limit the external validity of the results regarding the short-term effectiveness of ESWT.
Medial tibial stress syndrome
No evidence for ESWT due to extremely small sample size in one study20 and non-randomised controlled study design in two studies.18 19
Both non-randomised studies18 19 reported favourable results for the ESWT group. The most striking difference between studies was the ESWT protocol used in terms of total energy flux. One study19 used the same low-energy protocol of radial ESWT for three sessions (energy flux density 0.1mJ/mm2), while the other18 used a graded energy protocol of focused ESWT for five sessions (energy flux density from 0.1 to 0.3 mJ/mm2), resulting in more than the double total energy flux. Contradictory results at short-term follow-up were presented by the only RCT20 that used the same ESWT protocol as a non-randomised study.18 Several considerations are raised regarding the effectiveness of ESWT as well as the dose of the mechanical energy to be transferred. According to the data presented in this probably underpowered study, the sham group had better results in terms of pressure-induced pain and distance of pain-free running compared with the ESWT group. Data from these three studies suggest that the types of regimens and the configuration of the sample used can significantly influence outcome. The utility for ESWT in MTSS remains to be seen. Future randomised controlled studies with sufficient sample sizes are needed to clearly assess the effectiveness of ESWT and define the parameters of the most effective protocol.
Patellar tendinopathy
Moderate-level evidence suggests no difference between focused ESWT and placebo ESWT at short-term and mid-term (5–6 months) follow-up in pain and function. On the contrary, low-level evidence suggests that focused ESWT is superior to control conservative treatment (NSAID, physiotherapy, exercise, knee strap, modification of activity levels) at long-term follow-up (2–3 years) in functional and pain outcomes. Very low-level evidence suggests that focused ESWT produces comparable results to PRP injection along with stretching and strengthening at short-term follow-up, but PRP is more effective than ESWT at mid-term and long-term follow-up on VISA-P, pain scores and patient-rated pain reduction. Very low level of evidence suggests that focused ESWT produces comparable results to radial ESWT in patients with PT that received additive eccentric training at short-term and mid-term follow-up.
From the clinical perspective, conflicting evidence from two RCTs25 26 with comparison of ESWT and another RCT30 that used additive eccentric training was drawn for the effectiveness of ESWT compared with control/placebo. Zwerver et al 25 argued that the inconsistent findings could be attributed to patient characteristics. The athletes in the Zwerver et al 25 study had a mean VISA-P score of 60 and mean duration of symptoms of 8 months compared with the recreational athletes of Wang et al,26 which had a mean VISA-P score of 40 and mean duration of symptoms of >12 months. If interpreted according to the continuum model of tendon pathology,68 the athletes in one study were probably suffering from reactive tendinopathy or early tendon disrepair in contrast to athletes in a more degenerative stage of tendinopathy. Additionally, it is possible that these results could be attributed to the ESWT protocol used and the fact that the athletes continued participating in their sport activities in the Zwerver et al 25 study.
We suggest that these results may demonstrate preliminary evidence for a non-linear dose–response relationship for ESWT with both the lowest and highest levels of total energy flux resulting in less improvement. Specifically, the placebo group in Zwerver et al 25 (lowest total energy flux: 180 mJ/mm2) and the active group in the same study (highest total energy flux: estimated between 600 and 3480 mJ/mm2) had the lowest patient-rated improvements. The highest improvement (long-term follow-up) was seen in the study of Wang et al, 26 who applied approximately 270 mJ/mm2. While we cannot draw direct evidence from the results of Thijs et al 30 due to indirect comparison, the minimum and maximum energy flux they used was in accordance with the study of Zwerver et al.25 In this study, the placebo ESWT group received approximately 180 mJ/mm2 while the ESWT group received >600 mJ/mm2 similar to the Zwerver et al 25 study.
Limited evidence suggests no difference in the effectiveness between radial and focused ESWT along with an adjunct eccentric training programme in functional and pain scores at mid term.29 There are only two studies29 30 (one being one arm of Thijs et al 30) combining eccentric loading and ESWT in patients with PT and both reported significant improvement. However, van der Worp et al 29 questioned the significance of these results because the difference in VISA-P scores did not reach the cut-off point for MCID (15 points).55 69 Interestingly, the VISA-P scores in the focused ESWT arm of both studies were comparable. Clinically it is of importance to ascertain if ESWT (focused or radial) may mitigate the positive effects of eccentric training in PT. Studies that assessed eccentric training alone70–72 and included PT patients with similar duration of symptoms and follow-up reported consistent improvements in VISA-P scores that exceeded 20 points. Further studies are needed to assess different protocols of ESWT (energy and sessions) as an adjunct to eccentric load, as a specific single application low-energy treatment scheme was found to be effective.26
Given these data, the most effective ESWT protocol (sessions, dose, duration) is likely yet to be elucidated.
Proximal hamstring tendinopathy
Moderate-level evidence suggests that radial ESWT produces superior results to conservative treatment up to long-term follow-up (up to 12 months) in both functional and pain outcomes.
Using a protocol of four sessions over 4 weeks with medium energy, ESWT significantly decreased pain at 1 week follow-up.31 The reduction of pain persisted for 3 months and then remained stable up to 12 months follow-up (‘very much improved’). In contrast, the control group’s condition according to patients’ estimation44 deteriorated in each follow-up assessment, suggesting that the traditional conservative therapy used was ineffective. The high effect sizes calculated probably overestimated the effect due to the small numbers included in the study or probably because of the ineffectiveness of control treatment regimen. The overestimation was more evident in the OR calculation as 35% of the control group reported worsening in symptoms at 3 months, 45% at 6 months and 40% at 12 months, resulting in 25% loss at long-term follow-up. Based on these data, moderate evidence suggests that rest, NSAIDs, ultrasound, transverse friction massage, stretching and strengthening are not recommended in patients with chronic PHT.
Despite this study indicating that ESWT is an effective and promising treatment option for chronic PHT, the external validity of these results is limited by the relatively small sample size. Future studies are needed not only to evaluate further its effectiveness, but to compare ESWT with other more appropriate treatments for chronic PHT.
Strengths and limitations
This systematic review has documented the outcomes for a relatively large number of subjects (1847) included in relatively high-quality trials spread across conditions assessed and we suggest that the inclusion of the interpretation of effect sizes for pain reduction in patient-centred terms is a strength. Unfortunately, there are no occasions where multiple high-quality studies exist for a single pathology, hence for any individual pathology there are low and very low levels of evidence. We acknowledge the following as limitations: the study was not registered on the International prospective register of systematic reviews, and a funnel plot for assessment of publication bias was not created due to the small number of included studies for each individual pathology.
The poor correlation of the two different quality assessment tools used probably can explain the inconsistent results between the present and a recent systematic review,34 at least for AT, PT and GTPS. This highlights the importance of a research consensus in terms of methodological standardisation, guidelines in reporting and applicability/suitability of selected quality assessment tools in terms of study design. It is noted that our use of the GRADE ranking for level of evidence has likely contributed to the marked difference in overall conclusions drawn.
A limitation of research in this area and a possible bias is that a relatively small number of research groups account for the majority of research (approximately half of the studies included in quantitative analysis here) in this area. Another limitation relates to the inclusion criteria of studies which are seen to be variable and somewhat arbitrary. Increasingly it is noted that there is a poor association between radiologically identified abnormalities and pathology.63 64 Similarly, the variability and inaccuracy associated with clinical examination make for potentially insurmountable difficulties in the standardisation of treatment groups. Finally, the variability of the treatment protocols (in terms of energy delivered and total number of sessions) as well as the included patients makes generalisability difficult.
Future research suggestions and recommendations
Research to date has provided preliminary evidence for the effectiveness or not of ESWT; however, there is still a need for high-quality RCTs to discover the exact dose–response relation and its efficacy in larger sample sizes. It is also noted that clinicians would rarely provide ESWT as a monotherapy; rather it is often recommended that an individualised intervention should be provided depending both on the individual pathology (eg, insertional AT compared with non-insertional, reactive compared with degenerative) and the individual patient (non-athlete compared with high-level athlete, in-season compared with out of season, presence of comorbidities or not). It remains to be seen which factors in the patient’s presentation are truly confounding and what aspects of the intervention need to be modified to maximise the outcomes. We recommend, as a starting point, that minimum reporting standards be developed in terms of diagnostic classification criteria, outcomes, baseline measures, confounding factors (subject-specific) and aspects of the treatment applied. A future research suggestion is a network meta-analysis that would allow comparison of different treatment options to ESWT, once sufficient studies are available for a reasonable analysis.
Evidence suggests that exercise interventions are effective in lower limb conditions such as tendinopathy,73 74 but their effectiveness is limited to a subgroup of patients. Given the conflicting, low level of evidence or no evidence for more aggressive treatment approaches, such as PRP or corticosteroid injections,73 75 we suggest that ESWT is a suitable alternative option in lower limb conditions under investigation unresponsive to other conservative interventions.
Conclusion
There is a relatively large body of evidence spread across individual conditions assessed providing mainly low-level evidence for the efficacy of ESWT in lower limb conditions at short-term, mid-term and long-term follow-up. Caution needs to be exercised however in the clinical interpretation of these findings as it is likely that patient-specific individual confounding factors may have a significant effect on ultimate treatment outcomes, and these confounding aspects have not been fully examined.
What is the evidence of shockwave therapy in lower limb conditions?
Moderate-level evidence suggests that shockwave therapy is no better than placebo shockwave in patellar tendinopathy. This needs to be further investigated as preliminary evidence exists for a non-linear dose–response relationship for extracorporeal shockwave therapy with both the lowest and highest levels of total energy flux.
Moderate-level evidence suggests that shock wave is an effective intervention with large effect size in proximal hamstring tendinopathy.
Low-level evidence suggests that shockwave therapy is an effective intervention for Achilles tendinopathy, as well as for greater trochanteric pain syndrome.
There is no evidence for the effectiveness of shockwave therapy in medial tibial stress syndrome.
Future research
We suggest that future systematic reviews include the interpretation of effect sizes for pain reduction in patient-centered terms.
Shockwave therapy is rarely used as a monotherapy. Future studies should evaluate more clinically oriented, as well as individualised protocols, in terms of clinical effectiveness.
A research consensus in terms of methodological standardisation, guidelines in reporting and applicability/suitability of selected quality assessment tools in terms of study design is essential.
References
Footnotes
Contributors All authors contributed to this work and the authorship of this manuscript. VK planned, coordinated the idea, conducted the search, analysed results, wrote and reviewed the manuscript. RW coordinated the idea, analysed the results, provided writing content and reviewed. AT conducted the search, wrote and reviewed the manuscript. NM provided writing and review support.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.