Article Text

Abstract
Mental health symptoms and disorders are common among elite athletes, may have sport related manifestations within this population and impair performance. Mental health cannot be separated from physical health, as evidenced by mental health symptoms and disorders increasing the risk of physical injury and delaying subsequent recovery. There are no evidence or consensus based guidelines for diagnosis and management of mental health symptoms and disorders in elite athletes. Diagnosis must differentiate character traits particular to elite athletes from psychosocial maladaptations.
Management strategies should address all contributors to mental health symptoms and consider biopsychosocial factors relevant to athletes to maximise benefit and minimise harm. Management must involve both treatment of affected individual athletes and optimising environments in which all elite athletes train and compete. To advance a more standardised, evidence based approach to mental health symptoms and disorders in elite athletes, an International Olympic Committee Consensus Work Group critically evaluated the current state of science and provided recommendations.
- elite performance
- consensus statement
- mental
- psychiatry
- psychology
Statistics from Altmetric.com
Background
The International Olympic Committee (IOC) convened a consensus meeting on 12–14 November 2018 in Lausanne, Switzerland, at which experts reviewed the scientific literature addressing mental health symptoms and disorders in elite athletes. The participants analysed the current best evidence to provide a consensus statement for clinical practice and individual and systemic interventions to improve mental health among elite athletes. We define elite athletes as those competing at professional, Olympic or collegiate levels. Collegiate athletes often train and compete at levels similar to professional athletes, and including them expands the research we can draw on for this paper.
The group was charged with the following tasks:
to review the literature describing prevalence, diagnosis and impact on athletic performance of mental health symptoms and disorders within elite athletes
to review the literature describing and establishing recommendations for non-pharmacological and pharmacological management of mental health symptoms and disorders in elite athletes
to provide recommendations on how to minimise negative impacts of the sport environment on mental health symptoms and disorders in elite athletes.
This consensus paper fulfils the IOC charge by addressing the multifaceted aspects of mental health symptoms and disorders in elite athletes. The intended audience includes sport and exercise medicine physicians and other clinicians (including physiotherapists and athletic trainers), psychiatrists and other licensed mental health providers, other mental health and performance professionals who work with elite athletes, researchers in the fields of elite athlete mental health and clinical or institutional leaders/administrators who are stakeholders in sport.
Methods
Planning for the consensus meeting began in June 2017 (figure 1). The initial organising group included IOC leadership (RB and LE) and the meeting co-chairs (CLR and BH). They identified members of an expert panel, comprised of 23 individuals from 13 nations with expertise in the mental health of elite athletes. Panellists were identified based on their publications in the past 5 years, as determined by a literature search, and invited based on their clinical and/or scientific understanding of specific topics concerning mental health symptoms and disorders in elite athletes.

International Olympic Committee (IOC) consensus process for literature review, meeting and publication.
The meeting work group included the invited panel of experts, the organising committee members, four representatives from the IOC Medical and Scientific Department and two elite athlete representatives. Of the expert panel invited, one did not reply to the invitation and thus was not included, and one was removed after initial inclusion due to lack of follow-up. The final work group included psychiatrists, psychologists, primary care and orthopaedic sports medicine physicians, exercise scientists, a neurologist, a neurological surgeon and a social worker, and the work group represented Australia, Brazil, Canada, China, India, Italy, The Netherlands, Norway, South Africa, South Korea, Turkey, the UK and the USA.
The following methods sections describe the steps taken to plan and prepare for the meeting, the conduct of the meeting and the writing of the consensus statement.
Systematic reviews
The organising group initially identified 20 topic areas for the consensus statement (Figure 1). For each, a lead author and sometimes secondary author(s) were identified based on their scientific and clinical expertise.
An experienced librarian conducted a systematic review of each topic area using the PubMed, SportDiscus, PSycINFO, Scopus and Cochrane databases, and any additional databases felt relevant by individual topic leaders, for each topic. Searches were limited to the English language, and all study designs were included. An initial search strategy was developed with input from the expert panel to ensure that all relevant search terms were captured. Searches were revised by the librarian as needed. The expert panel screened 14 689 published articles. Results and input from the expert panel led to revision of research questions asked within the 20 topic areas. Leaders of topics without a recent published systematic review were invited to write separate, more detailed, subspecialty papers on their topics; these will be published separately.
Each topic team was asked to summarise the key information from their review and share it with the expert panel before presenting it at the consensus meeting. A draft of these summaries was circulated to all participants prior to the meeting.
Consensus meeting
The consensus meeting was a 2.5 day series of presentations in which topic leaders presented their systematic review findings. Group discussion followed each presentation, and meeting co-chairs took notes during the discussions to capture all comments.
Writing the consensus statement
The initial draft systematic review summary document was edited based on agreement at the meeting. Key statements agreed on during the meeting were not changed during the drafting of the final document. To ensure inclusion of the most recent literature, the systematic literature reviews were re-conducted 3 months before submission of the manuscript, using the same search strategies as initially used. The updated search results were provided to topic leaders, and additional edits made accordingly. The edited final document was circulated for review and further editing by the full expert panel.
General prevalence of mental health symptoms and disorders in elite athletes
Increasing numbers of epidemiological studies address mental health symptoms and disorders in elite athletes. Reporting prevalence compared with that in the general population is particularly difficult for the following reasons: (a) most studies in elite athletes have lacked reference groups from the general population; (b) different instruments have been used to assess mental health symptoms and disorders in athletes compared with the general population; (c) studies do not necessarily consider cross cultural differences in meanings and manifestations of mental health symptoms and disorders; and (d) studies vary in whether they describe self-reported specific mental health symptoms or physician diagnosed disorders. Regarding the latter, mental health disorders are typically defined as conditions causing clinically significant distress or impairment that meet certain diagnostic criteria, such as in the Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5)1 or the International Classification of Diseases,2 whereas mental health symptoms are more common, may be significant but do not occur in a pattern meeting specific diagnostic criteria and do not necessarily cause significant distress or functional impairment.
The reported prevalence of mental health symptoms and disorders among male elite athletes from team sports (cricket, football, handball, ice hockey and rugby) varies from 5% for burnout and adverse alcohol use to nearly 45% for anxiety and depression.3–13 Prospective studies have reported that mental health disorders occur in 5% to 35% of elite athletes over a follow-up period of up to 12 months.13–19 Among female elite athletes, mental health disorders—especially eating disorders—are also prevalent.20–23 Among collegiate athletes, the prevalence of mental health disorders ranges from 10% to 25% for depression and eating disorders.24–30
During an elite sport career, generic and sport specific factors may combine to increase the risk of mental health symptoms and disorders.31 32 Elite athletes may experience a greater overall risk of mental health symptoms and disorders compared with their athletic counterparts if they suffer severe musculoskeletal injuries, undergo multiple surgeries, suffer from decreased sport performance or tend toward maladaptive perfectionism.7 16 22 33–38 In other circumstances, sport participation might protect against mental health symptoms and disorders,39 since exercise has antidepressant effects.40 Finally, an athlete might have mental health symptoms or suffer with a mental health disorder with no apparent association between elite sport participation and the mental health condition.39
General approaches to management of mental health symptoms and disorders in elite athletes
Management of mental health symptoms and disorders in elite athletes should take a comprehensive, integrative approach that puts the athlete at the centre and addresses the full range of emotional, mental, physical, social, spiritual and environmental influences that may affect a person’s mental health. A personalised management strategy should be used to address mental health symptoms and disorders while striving to maintain optimum well being. The strategy should take into consideration the elite athlete’s particular needs and circumstances, utilise the most appropriate consensus or evidence based interventions from a variety of scientific disciplines, and recognise differences across countries and cultures.
A core challenge in developing this consensus statement was that the evidence comes predominantly from high income countries, which have more health services compared with low and middle income countries41–43 where many athletes reside. There is debate concerning the range of ways in which mental health symptoms and disorders can be managed in culturally appropriate ways, drawing on resources from other health sectors and community carers, for example,44–46 with increasing evidence that intervening in ways that support existing community strengths may be of benefit to people with these conditions.47 48 It is important to consider this global context throughout this statement.
Psychotherapy
Psychotherapy is defined as the treatment of mental health symptoms or disorders or problems of living, and/or facilitation of personal growth, by psychological means; it is often based on therapeutic principles, structure and techniques. Psychotherapy, with or without pharmacologic therapy, is effective for the treatment of mental health symptoms and disorders but is commonly underprescribed.49 Moreover, studies on specific types of psychotherapy in elite athletes are lacking. Individual psychotherapy, especially cognitive behavioural therapy (CBT), is efficacious for treating depression and anxiety disorders in the general population.50 In many situations, psychoeducation and/or counselling (broadly defined) are considered the treatment of choice for athletes.51 Depending on the sport, the athlete and the family dynamics, family therapy may be helpful.52 Further, although substance use may be problematic in elite athletes, little research exists on different psychotherapeutic treatments for substance use disorders in this population.53 54
Compared with non-athletes, elite athletes may present with sport related issues that may pose a challenge in psychotherapy and make it more difficult to tailor therapeutic interventions. These issues can include the following: diagnostic challenges (eg, overtraining syndrome vs major depression); aggression; narcissism; and entitlement.52 Insight oriented therapy, such as time limited psychodynamic psychotherapy, may be indicated for elite athletes with challenging personality and behavioural issues.55 In these situations, therapy should first focus on maladaptive behaviour patterns because personality traits tend to be more resistant to change.55
When engaging elite athletes in the psychotherapeutic process, the clinician must be mindful of how the athlete’s characteristics may impact treatment. For instance, elite athletes may anticipate receiving preferential treatment from their healthcare providers.55 While a degree of flexibility may be needed to maintain patient privacy and accommodate travel schedules, perpetuating a pattern of preferential treatment may lead to unintended boundary violations.49 Box 1 guides clinicians as to how to overcome common obstacles that can interfere with treatment in elite athletes.
Guidelines to overcome common obstacles that can interfere with psychotherapy with elite athletes
Clinicians should:
be flexible about timing of sessions (although without allowance of persistent cancelling of sessions)55
urge couples or family therapy when relational issues impact functioning or performance55
recommend psychotherapy plus pharmacological therapy when indicated for cases of moderate to severe mental health symptoms or disorders
obtain collateral information from close informants, with appropriate consent, for athletes with severe mental health symptoms or disorders55
insist that the athlete undergo substance use disorder treatment if needed55
Clinicians should not:
Clinicians should not compromise on delivering other appropriate treatment, including medications and hospitalisation as necessary, during psychotherapy with elite athletes.55 While barriers exist that may prevent elite athletes from seeking, accepting or effectively using psychotherapy, elite athletes also possess skills and personality characteristics—notably discipline and compliance with recommended regimens—that make them especially good candidates for psychotherapeutic interventions.49
Pharmacological treatment
Although psychotherapy is generally regarded as the firstline treatment for those with mild to moderate symptoms of mental illness,51 medications may be needed in those with more severe psychopathology.56 Box 2 outlines four important considerations particular to elite athletes when prescribing psychiatric medications. Common side effects that may negatively impact athletic performance include: sedation; weight gain; cardiac side effects (including orthostatic hypotension, hypertension, tachycardia, palpitations, arrhythmias and electrocardiographic changes such as QTc prolongation); and tremor.56 57 Other relevant side effects include: impaired concentration; muscle rigidity; motor changes (including akathisia and bradykinesia); weight loss; blurred vision or dizziness; anxiety or agitation; and insomnia.56
Four key considerations relevant for elite athletes when prescribing psychiatric medications57
Potential negative impact on athletic performance
Potential therapeutic performance enhancing effects (ie, based on improvement in the condition the medication is designed to treat)
Potential non-therapeutic performance enhancement effects (ie, ergogenic effects)
Potential safety risks
The distinction between therapeutic and ergogenic performance enhancement that may result from a medication is important for all classes of medication.58 For example, an athlete who is performing poorly because of uncontrolled anxiety may gain a therapeutic performance enhancing effect by taking serotonin selective reuptake inhibitors (SSRIs). However, there is no evidence that they provide ergogenic performance enhancement, and thus they are not prohibited substances in elite sport.57 59 60 Indeed, stimulants are the only class of psychiatric drugs classified as prohibited substances, and they are prohibited only in competition; research suggest they could enhance performance beyond a pharmacological therapeutic effect.59
Finally, safety risks are paramount with certain psychiatric medications, as elite athletes commonly exercise at much higher intensity than the general population.61 For example, medications with blood levels that must be tightly regulated, such as lithium, can be difficult to manage in elite athletes whose levels might be influenced by hydration status.56 57
The four considerations of prescribing medications to elite athletes listed in Box 2 may vary by the particular sport and its demands,56 level of performance required,56 time frame within the athletic training/competition cycle and anticipated duration of treatment. Ultimately, medication choices must be informed by the need to provide effective clinical care for mental health symptoms and disorders.56 Although there are athlete specific considerations within each category of psychiatric medications, there is a paucity of applicable research on the topic.56 60 Available studies have methodological flaws, including small sample sizes; medications are not used in real world dosages or time frames; populations studied are not representative of elite athletes; few female athletes are studied; performance measures used to determine if a medication has a negative impact on athletic performance may not represent actual performance impact; and study subjects often lack the mental health disorder that the medication is intended to treat.60–62 We acknowledge these limitations. Nevertheless, some research is available regarding psychiatric prescribing for athletes, and details are shared as relevant below.
Specific mental health symptoms and disorders in elite athletes
In this section we detail the assessment and management of:
sleep disorders and sleep concerns
major depressive disorder and depression symptoms
suicide
anxiety and related disorders
post-traumatic stress disorder and other trauma-related disorders
eating disorders
attention-deficit/hyperactivity disorder
bipolar and psychotic disorders
sport-related concussion
substance use and substance use disorders
gambling disorder and other behavioural addictions
Note that we have published separate review papers for several of these conditions.
Sleep disorders and sleep concerns
Insufficient sleep is defined as less than 7 hours of sleep for a healthy adult;63–68 adolescents and younger adults need 9–10 hours of sleep.67–70 National Collegiate Athletic Association (NCAA) surveys indicate that over half of collegiate athletes in the USA report regularly getting insufficient sleep; 50% report less than 7 hours of sleep per night in season and 79% report 8 hours or less.71 Data among large samples of elite athletes are sparse, although 49% of Olympic athletes would be classified as 'poor sleepers'4 (a term that includes multiple sleep problems). Elite athletes are particularly unlikely to get sufficient sleep the night prior to competition.72 Sleep deprivation impairs athletic performance across many sports73–96 and sleep improvement leads to improved performance.78 83 97–100 Sufficient sleep is important to avoid overtraining82 87 92 101 102 and maximise training gains by regulating adaptive release of hormones such as testosterone103–106 and growth hormone.107–111 Conversely, sleepiness and fatigue are associated with poor athletic outcomes.83 85
Circadian dysregulation—a misalignment between the individual’s sleep–wake pattern and the desired pattern or the pattern regarded as the norm—is common in athletes, especially those who frequently travel across time zones. Circadian rhythms are important for metabolism,112–114 performance,91 115–121 and psychological function.122–126 Disrupted circadian rhythms decrease athletic performance.127–129 The timing of sport training, especially in the early morning, can impair sleep72 and lead to suboptimal performance outcomes. Because of an athlete’s chronotype (degree to which an individual is naturally a 'morning' or 'evening' person), timing of training or competition may not align with their personal time of peak performance.130–132 Persistent circadian dysregulation may contribute to neurodegeneration and mental health disorders.133–135
Insomnia disorder—a persistent difficulty initiating or maintaining sleep at least 3 nights per week for at least 3 months (in the context of adequate sleep opportunity and accompanied by daytime impairments)—136 is a major risk factor for mood and other mental health disorders137–139 and impaired physical function.140 Insomnia disorder may be very common among athletes; approximately 64% of Olympic athletes reported significant insomnia symptoms.79 Insomnia is associated with impaired athletic performance.141
Sleep apnoea involves periodic reduction or cessation of breathing during sleep.136 Due to its relationship with higher body mass, sleep apnoea is especially common among American football players142–145 and many are at high risk for sleep apnoea.142 146 However, high body mass is not required for sleep apnoea, and many with the disorder remain undiagnosed.147 Additionally, training at altitude can produce central sleep apnoea.148 Untreated sleep apnoea, regardless of aetiology, increases fatigue and dramatically impairs athletic performance149–155 if untreated.
Addressing sleep problems in elite athletes requires screening for primary sleep disorders (such as circadian dysregulation, insomnia disorder or sleep apnoea), since solely treating comorbid mental health symptoms or disorders (such as depression or anxiety) will likely be unhelpful unless any primary sleep disorders are properly treated.156 A questionnaire validated for use in athletes may help identify athletes who need further sleep assessment.157 At the team level, the sports medicine team can promote healthy sleep by: (i) ensuring coaches model healthy sleep and schedule training around sleep and circadian rhythms; (ii) encouraging healthy sleep as part of the training protocol; (iii) promoting sleep health education; and (iv) engaging in proactive tracking and monitoring of sleep.
Non-pharmacological treatments are often recommended to treat sleep disorders in athletes because many medications are associated with increased injury risk and may cause side effects (eg, slowed reaction time, cognitive impairment) that may impair athletic performance.158 159 Non-pharmacological treatments (collectively described as 'behavioural sleep medicine') are available for many sleep disorders.160 The recommended treatment for insomnia is CBT for insomnia (CBTI); its effects are at least as good as those of medications,161 162 without the associated side effects. Further, CBTI is effective in the presence of comorbidities, such as chronic pain, depression and sleep apnoea.163 Sleep hygiene alone is often insufficient for more complex problems.83 164
Athletes taking any sleep aids should be advised of the importance of allowing a full night of restorative sleep.60 Melatonin, which may be prescribed or purchased over the counter, is a preferred choice of sports psychiatrists for insomnia.57 Additionally, it is the best studied sleep aid in athletes.57 Neither immediate release nor extended release melatonin adversely impact performance.56 60 165 166 Rarely, melatonin may cause hypotension.167 However, although melatonin often helps to ameliorate sleep problems, it may have limited utility for those with more extreme sleep difficulties, including insomnia disorder.168 Additionally, over the counter melatonin may contain impurities and unknown quantities of melatonin; athletes should purchase it only from a reputable company.60 If a supplement such as melatonin includes any prohibited substances, and an athlete ingests them unknowingly, the athlete will be held accountable if found to have an adverse analytical finding for a prohibited substance. Ignorance of ingredients or improper labelling of supplements is not excusable under the World Anti-Doping Agency (WADA) code.60
If melatonin does not help an athlete with insomnia, trazodone and gabapentin are sometimes used, although they have not been studied specifically in athletes,57 and there is no evidence base to support their efficacy for insomnia disorder.168 Imidazopyridines (eg, zolpidem and zopiclone) may be options if needed57 and are effective medications for insomnia disorder.168 They have less of an impact on next day physical performance than benzodiazepines.169–173 Among the benzodiazepines, agents with longer half lives have a more detrimental impact on next day physical performance compared with shorter acting agents.174 This finding must be considered alongside the knowledge that benzodiazepines with shorter half lives are more likely to cause physical dependence and substance use disorders.175
For sleep apnoea, the recommended treatment is usually positive airway pressure therapy.176 Oral appliances are also recommended for some individuals,177 and in rare cases, airway surgery may be required.178 For circadian rhythm disturbances, melatonin is the treatment of choice and has established efficacy in many populations,179 although its dose and timing for schedule shifting are different than for sleep promotion. Typically, this involves lower doses timed earlier in the evening (for advancing sleep) or the end of the night (for delaying sleep).180 181 Timed bright light exposure is also routinely used to shift circadian rhythms. Bright light at night can delay sleep onset, and early morning light can advance sleep onset the next night.181 182
Major depressive disorder and depression symptoms
Individuals with major depressive disorder (MDD) experience depressed mood and/or little interest or pleasure from activities on most days over at least a 2 week period, in addition to associated physical, psychological and cognitive symptoms.1 A diagnosis requires at least five symptoms and a negative impact on functioning, but individuals may also experience depressive symptoms without meeting the criteria for MDD (table 1).1 An athlete specific screening tool for depression is reliable and valid (Box 3).183 184
Diagnostic and Statistical Manual of Mental Disorders-5 diagnostic criteria for a major depressive episode1
Baron Depression Screener for Athletes. The instrument is designed for athletes to self-report; if the athlete scores >5 they should be evaluated by a mental health professional183
Please respond to the following questions utilising the following scale:
0-Never
1-Some of the time (over a 2 week period)
2-Most of the time (over a 2 week period)
I feel sad even after a good practice session or successful competition.
I rarely get pleasure from competing anymore and have lost interest in my sport.
I get little or no pleasure from my athletic successes.
I am having problems with my appetite and weight.
I do not feel rested and refreshed when I wake up.
I am having problems maintaining my focus and concentration during training and competition.
I feel like a failure as an athlete and person.
I cannot stop thinking about being a failure and quitting sports.
I am drinking alcohol or taking supplements to improve my mood.
I have thoughts of ending my life.
The prevalence of depressive symptoms in elite athletes ranges from 4%185 to 68%.35 When the research is considered in its entirety, the prevalence of depressive symptoms in elite athletes and the general population appears to be similar.186 However, elite athletes may not recognise or acknowledge depressive symptoms or may not seek support,187 in part related to stigma.188 Female athletes may be twice as likely to report depressive symptoms as male athletes.186 Rates of adjustment disorder with depressed mood (defined as experiencing more depressive symptoms than would normally be expected in response to a stressful life event, but not to the point of those symptoms meeting criteria for MDD)1 and persistent depressive disorder/dysthymic disorder (defined as a chronic course of depression lasting at least 2 years)1 in elite athletes are unknown.
Different sports are associated with different risks for depressive symptoms and MDD. French athletes who took part in aesthetic or fine motor skills sports were at greater risk of experiencing depressive symptoms than those who took part in team ball sports.185 Among North American athletes, track and field athletes had the highest rates of MDD compared with those in other collegiate sports.29 Depressive symptoms may be more prevalent in individual sport athletes compared with team sport athletes.12 29 189
Risk factors associated with depressive symptoms and MDD in elite athletes include: genetic factors (eg, family history); environmental factors (eg, poor quality relationships, lack of social support);61 190 injury;39 competitive failure;39 retirement from sport;191 pain;192 and concussion.193 After athletes retire from elite sport, those with lower levels of physical activity have higher rates of MDD.194
Non-functional overreaching (NFO) and overtraining should be considered as possible relevant factors in athletes who present with depressive symptoms. There are no generally accepted diagnostic criteria for NFO and overtraining. NFO is often defined as the accumulation of training load without compensatory recovery, with resultant performance decrement and the need for more prolonged recovery.195 196 Overtraining is an extreme form of NFO that results in a prolonged performance decrement (usually longer than 2 months) and more severe psychological and/or neuroendocrinological manifestations.197 198 Both are associated with depressed mood.199 Symptoms that overlap with MDD may include fatigue, insomnia, appetite change, weight loss, amotivation and diminished concentration.200 In an 11 year study of 400 competitive collegiate swimmers, mood state disturbance increased with training stimulus during the season, and then fell to baseline as training load diminished.201 One possible difference between NFO/overtraining and MDD in some athletes may be the nature of the dysfunction—athletic performance in NFO/overtraining versus social, cognitive and work performance in MDD.193 Cessation of training in athletes with NFO or overtraining often improves mood and associated symptoms, whereas depressed athletes who do not exercise may experience worsened mood and lose the antidepressant effect of exercise.61
Depressive symptoms and MDD may result in decreased performance, adverse effects on personal life or an exit from sport.192 MDD is also highly associated with suicide and suicidal ideation.202 203 Treatment of depressive symptoms and MDD depends on the severity of symptoms but usually consists of psychotherapy, often with medication.
In an international survey of sports psychiatrists, most of whom treat elite athletes, bupropion was described as a top choice for use in athletes with depression without comorbid anxiety.57 Bupropion’s relatively energising properties and lack of weight gain as a side effect may have contributed to its top selection.57 However, it is not available worldwide,56 and should not be prescribed in athletes with an eating disorder because it increases the risk of seizure—a potential complication of eating disorders.204 Preliminary evidence suggests that bupropion potentially enhanced performance in endurance athletes who used a single, high dose (600 mg) in warm climates.205 Performance enhancement was not observed with longer term therapeutic bupropion treatment.206 Performance enhancement has been noted with 300 mg dosing the night before and morning of a cycling time trial in warm climates, but not at doses less than 300 mg.207 The research on bupropion suggests that it may allow athletes to push themselves to higher core body temperatures and heart rates (thus improving performance) when used at higher doses and in acute rather than chronic doses.205 Bupropion is currently on WADA’s Monitoring Programme list in competition.59 At present, however, it can be prescribed without a therapeutic use exemption (TUE), which is a process that allows athletes to request permission to take a medication that is on the WADA prohibited list.
SSRIs are also often prescribed to treat depression in athletes.56 57 In particular, fluoxetine has no demonstrated negative impact on performance,208 209 and has emerged as an antidepressant of choice for athletes.56 57 210 211 Serotonin and norepinephrine reuptake inhibitors, tricyclic antidepressants (eg, nortriptyline, amitriptyline) and mirtazapine have not been studied in athletes.60 Serotonin and norepinephrine reuptake inhibitors are sometimes regarded as relatively energising,60 but one small study suggested that a norepinephrine reuptake inhibitor may be performance limiting.212 Tricyclic antidepressants and mirtazapine may cause sedation and weight gain.60 Furthermore, supraventricular and ventricular arrhythmias have been described in young, healthy people taking tricyclic antidepressants.213 Blood levels of tricyclic antidepressants could become toxic in athletes who sweat heavily, although this concern has not been confirmed in research among elite exercisers.214 In summary, the evidence suggests that tricyclic antidepressants should be avoided as firstline medications in athletes56 60 and, if prescribed, blood levels should be monitored.60
Suicide
In the largest study of suicide in elite collegiate student athletes in the USA, 7.3% of all deaths were attributed to suicide.215 Overall, the rate of suicide was 0.93/100 000 in collegiate athletes per year. The mean age of suicide was 20 years, and male collegiate athletes who participated in American football were at greatest risk. However, collegiate athletes still had a lower rate of suicide than individuals of the same age in the general US population (11.6/100 000 per year).216
Suicide prevention interventions should be multimodal, evidence based and range from interventions to manage stress and distress to addressing symptoms of MDD and overt suicidal ideation.202 203 Risk factors (table 2) should be assessed and, where possible, mitigated.27 217–219 To promote help seeking behaviours and to potentially reduce the risk of suicide, greater awareness of risk factors for suicide may be needed among coaches, medical professionals and others who work with athletes.27 29 215 Strategies to understand and modify environmental stressors for elite athletes—such as improving social networks, athletic and personal life balance, team cohesion, and coach and team expectations—should be considered in conjunction with treatment for mental health symptoms and disorders.215 With retired athletes, careful consideration must be given to both mental and other medical aspects of health while addressing social isolation and other stressful aspects of transition from sport.217
Risk factors for suicide27 217–219
Anxiety and related disorders
Individuals with generalised anxiety disorder (GAD) experience excessive anxiety and worry, with symptoms noted in table 3. GAD in elite athletes ranges in prevalence from 6.0% for a clinician confirmed diagnosis185 to 14.6% using self-report measures.14 Consistent with the general population, GAD symptom ratings tend to be higher for female athletes than male athletes.20 24 30 190 220–222 Injured athletes appear to report more severe GAD symptoms than their non-injured counterparts.11 20 30 223 224 From the limited data available regarding prevalence of other anxiety disorders and related disorders in elite athletes (table 4), self-reported estimates include 14.7% for social anxiety,11 5.2% for obsessive–compulsive disorder225 and 4.5% for panic disorder.11 Rates of GAD and these other disorders in elite athletes do not appear to differ markedly from those in the general population.226 227 Rates of specific phobia, agoraphobia, obsessive–compulsive personality disorder and adjustment disorder with anxiety (the latter defined as experiencing more anxiety symptoms than would normally be expected in response to a stressful life event, but not to the point that those symptoms meet the criteria for another specific anxiety disorder)1 in elite athletes are unknown. However, adjustment disorder with anxiety may be more common than other anxiety disorders in elite athletes.228
Diagnostic and Statistical Manual of Mental Disorders-5 diagnostic criteria for generalised anxiety disorder1
Diagnostic and Statistical Manual of Mental Disorders-5 diagnostic criteria for selected other anxiety and related disorders1
Among elite athletes, patterns of symptom onset, duration and severity should be used to differentiate anxiety disorders from competition performance anxiety, although state and trait anxiety domains can overlap.229 230 In addition, other mental health symptoms and disorders, most notably those of depression and/or eating disorders, may be coexisting.17 21 39 185 231 232 Pervasive worries or fears that accompany physiological symptoms may qualify for a diagnosis of GAD (if it persists for at least 6 months) or panic disorder (if accompanied by an abrupt surge in panic related symptoms).1 Agoraphobia, social anxiety and specific phobias occur in the context of specific stimuli, whereas obsessive–compulsive disorder is characterised by intrusive and unwanted obsessions and/or compulsions and obsessive–compulsive personality disorder by preoccupation with orderliness, perfectionism and control in the absence of obsessions and compulsions.1 Fear of negative evaluation by others may differentiate aspects of social anxiety from competitive performance anxiety.233 Panic attacks triggered by certain training or competitive situations may indicate a specific phobia; unexpected panic attacks not triggered by a specific fear more likely signal a panic disorder.234 Because habitual behaviours are commonplace for elite athletes,235 236 idiosyncratic mannerisms or repetitive routines alone do not merit a diagnosis of obsessive–compulsive disorder in the absence of distress or impairment.1
Anxiety symptoms are reliably associated with both impaired cognitive performance and overall functioning in general populations,237 238 although scant research exists for elite athletes.39 Higher ratings of self-reported anxiety (relative to moderate ratings) are associated with negative performance outcomes and skill errors in elite athletes.230 239 240 Pre-competitive (ie, state) anxiety is to be expected among elite athletes competing at major events, and the athlete’s interpretation of pre-competitive anxiety may mediate the functional impact of symptoms.241 Facilitative, rather than debilitative, perceptions of anxiety symptoms appear associated with more adaptive coping and behavioural responses.242 243
Anxiety disorders respond well to evidence based psychotherapy (eg, CBT), although treatment mechanisms necessarily vary by disorder.244 In addition to cognitive strategies addressing unhelpful thinking patterns or experiential avoidance, treatment frameworks should emphasise, as needed, graded exposure and behavioural experimentation for cases of social anxiety, response prevention for cases of obsessive–compulsive disorder and arousal reduction for those with GAD or panic disorder.245
Anxiolytic medications may be used to treat anxiety disorders in elite athletes, and there are important considerations, including side effects and performance impairment.61 SSRIs, specifically escitalopram, sertraline and fluoxetine, are sports psychiatrists’ top choices for pharmacological treatment of anxiety in athletes.56 57 Buspirone, an antianxiety medication, has received little study in athletes; one small study suggested it impaired performance among recreational athletes, but only a single 45 mg dose was tested.246
Short acting medications, such as benzodiazepines, are not usually recommended for performance (situational) anxiety because they may impair performance.56 165 174 247 Propranolol and other beta blockers, sometimes used for performance anxiety in non-sport settings, should typically be avoided in sport60 because they may lower blood pressure in athletes who already may have relatively low blood pressure. In endurance sports, beta blockers can problematically decrease cardiopulmonary capacity.248 Because of their effectiveness in reducing tremor and thereby improving fine motor control, beta blockers are prohibited at all times for archery and shooting, and are prohibited in competition for archery, automobile, billiards, darts, golf, shooting, some skiing/snowboarding and some underwater sports.59
Post-traumatic stress disorder and other trauma-related disorders
Trauma-related mental health disorders in elite athletes are common, with potentially serious consequences.249 These disorders include post-traumatic stress disorder (PTSD), defined as exposure to a trauma followed by at least 1 month of mental health symptoms; acute stress disorder (similar to PTSD, but less than 1 month in duration); and adjustment disorder (abnormal reaction to an identifiable life stressor).1 Athletes may encounter traumatic experiences from inside or outside of sport, and such experiences may range from sport injuries to life events independent of a sport injury.250 251
Research on the prevalence of trauma-related disorders in elite athletes is limited. This is particularly true regarding trauma-related disorders stemming from traumas other than sports injuries. Sport-related musculoskeletal injury is associated with elevated levels of PTSD symptomology.249 Athletes may also experience PTSD symptoms shortly after a sport-related concussion.252 Traumatic injuries may pose an even greater risk of progression to a chronic trauma-related mental health disorder in athletes with pre-existing exposure to trauma of any type.253
Diagnosing PTSD and other trauma-related disorders in athletes can be challenging. Trauma-related symptoms may manifest at any time,254 especially during situations reminiscent of a prior inciting event.249 255 Such symptoms include: hyperarousal (commonly experienced as anxiety); avoidance of physical and psychological reminders; re-experiencing symptoms (eg, intrusive thoughts, nightmares or flashbacks); dissociation (feeling detached from one’s surroundings and/or emotions); and non-specific symptoms, including irritability and depressed mood.1 250 Athletes may also develop comorbid substance use disorders or eating disorders.250 Trauma-related disorders may be associated with inconsistent athletic performance and somatic complaints without evident injury.250
Athletes may engage in behaviours that can obscure trauma-related symptoms. For example, elite athletes may compartmentalise to manage emotions, effectively concealing symptoms of trauma-related disorders.256 Further, dissociative strategies (eg, blocking of sensory input, as intentionally utilised by endurance athletes)257 may conceal trauma symptoms. Adaptive perfectionism, defined as deriving satisfaction from achievement from intense effort and tolerating imperfections without self-criticism,258 is a useful tool against symptom manifestation in many sports.259 However, it can evolve into maladaptive perfectionism, characterised by setting consistently unrealistic personal standards.258 This can include manifestations of obsessive–compulsive disorder, which can be a comorbid condition with trauma-related disorders.259
Symptoms of trauma-related disorders may negatively impact athletic performance.249 260 261 Additionally, fear of re-injury increases the risk of subsequent injuries because of avoidance, inhibited effort or risk seeking behaviours.249 262 Injured athletes may hesitate to undergo physical therapy because of avoidance, thus interfering with recovery.260 Psychological distress, commonly seen in trauma-related disorders, reduces immune function and delays healing, thus impeding the athlete’s ability to participate in rehabilitation following an injury.261
Early identification of and intervention for suspected trauma-related disorders may mitigate associated morbidity.263 Screening for mental health disorders following a sport-related traumatic musculoskeletal injury is recommended.264 Although evidence of impact on ultimate development of PTSD is mixed, careful, non-compulsory psychological debriefing with a qualified provider for an individual and/or team, with appropriate follow-up and support, may reduce distress and enhance group cohesion in the immediate aftermath of trauma.250 Trauma informed management of a traumatised athlete’s team also can improve outcomes for the traumatised individual.265 Conversely, blaming the individual for the traumatic situation may perpetuate symptoms of trauma.250 Passive attitudes, non-intervention, denial and silence by those in power may also compound the initial trauma.266 Psychotherapeutic modalities recommended for the treatment of trauma-related disorders include CBT, cognitive processing therapy, cognitive therapy and prolonged exposure therapy.267 If medications are needed, SSRIs such as sertraline and fluoxetine are generally regarded as the agents of choice268 and overall are reasonable choices for athletes.57
Eating disorders
Eating disorders (including anorexia nervosa, bulimia nervosa and binge eating disorder) and disordered eating (abnormal eating behaviours not meeting criteria for an eating disorder) (table 5) among elite male and female athletes are common.25 269–272 The estimated prevalence of eating disorders and/or disordered eating among athletes in general ranges from 0% to 19% in men and from 6% to 45% in women,273 considerably higher than in non-athletes.274 Data on elite athletes are sparser, but also show significantly greater risk in elite athletes than in non-athletes.23 241 Elite athletes more commonly meet criteria for disordered eating than for eating disorders.275 Data have largely relied on self-reports. However, athletes are prone to denial of symptoms, and are more apt to underreport disordered eating than are non-athletes.23
Characteristics of eating disorders versus disordered eating in elite athletes1 274 736
Athletes possess some of the same risk factors for eating disorders as the general population, and some that are sport specific risks (table 6).273 More than 60% of elite female athletes from both leanness focused and non-leanness focused sports have reported body shaming pressure from coaches.276 Eating disorders are common in athletes using performance and image enhancing drugs, including anabolic androgenic steroids, amphetamine-like substances, coffee and caffeine derivatives, synthetic cathinones and ephedrine.277 Dissatisfaction with body image may be the strongest predictor of eating disorders in athletes.278
General and sport specific risk factors for eating disorders273 296
A diagnosis requires obtaining a detailed current and past history (including a corroborative history), a thorough physical examination and laboratory studies.274 Dual energy X-ray absorptiometry and electrocardiography are sometimes needed to assess possible adverse effects on bone and cardiac health.274 Rating scales that have been validated in athletes, such as the Athletic Milieu Direct Questionnaire version 2, the Brief Eating Disorders in Athletes Questionnaire version 2, and the Physiological Screening Test to Detect Eating Disorders Among Female Athletes, may be used.279 However, research suggests that personal interviews may be superior to rating scales in diagnosing eating disorders in athletes.280 The usual DSM-5 diagnostic criteria1 may be difficult to apply in athletes51 because the adaptive nature of a disciplined training diet and preoccupation with body shape and weight in sport may confuse the diagnosis.281 Additionally, athletes may present as normal weight, with very low body fat but high muscle mass.61 Finally, excessive exercise as an eating disorder behaviour often used to compensate for a perceived excess of calories consumed can be challenging to assess in athletes.282
In elite training, athletes may present with low energy availability (LEA), which can occur secondary to inadvertent inadequate intake or from disordered eating. The female athlete triad was historically denoted by LEA, menstrual dysfunction and low bone mineral density.51 283 284 Male athletes may present with an analogous condition characterised by LEA, hypogonadotropic hypogonadism and low bone mineral density.285 The IOC convened and redefined these entities under a broader umbrella: relative energy deficiency in sport (RED-S), which addresses the more global impact of relative energy deficiency on physiological function and its psychological consequences and includes all genders.280 286
The fact that an eating disorder impairs athletic performance is a powerful motivator for treatment.278 While performance may not immediately suffer, typically performance decreases over time, related to factors such as dehydration, electrolyte disturbances, early glycogen depletion, loss of muscle mass and injuries such as stress fractures.274 278 287 288
Among the challenges in bringing an athlete to treatment are concerns about confidentiality,289 finding access to effective treatment, the athlete's acceptance that there is a problem to treat, the ability to relate—as an athlete—in treatment and the possible need to restrict activity on return to play.290 Just as team culture may engender disordered eating, there may be a role for teammates to encourage healthy eating behaviours.291
One of the first decision points in treatment is what level of care is required. Those who are severely nutritionally compromised may need hospitalisation.274 In any setting, an interdisciplinary team is ideal, and may include a psychiatrist, a sports nutritionist/dietitian, a primary care physician, another licensed mental health provider, an athletic trainer and a coach.274 Once a healthy nutritional status is attained, the psychological and sociocultural underpinnings of the disordered eating may be addressed through psychotherapeutic modalities in individual, group or family settings.292 A team may be viewed as a family structure, or a coach–athlete relationship may benefit from therapy.293
While there is little evidence that medication is helpful for anorexia nervosa, the primary pharmacologic treatments in bulimia nervosa are antidepressants, specifically fluoxetine, which has no evident adverse impact on performance.1 208 209 294 Lisdexamfetamine may be helpful for binge eating disorder295 but it is a stimulant and thus is prohibited in competition at elite levels of competition and requires a TUE.59
Although early detection and treatment are critical, prevention of eating disorders is also important.273 296 Overall, the body of research on eating disorder prevention programmes with elite athletes is small but promising.296 Elements common to seemingly successful prevention programmes include involvement of multiple targets for systematic change (eg, athletes, coaches and sport administration),296–298 and utilisation of interactive programmes that encourage multiple modes of communication (eg, with athletes leading some of the session, use of practical skills assignments and provision of a safe space for athletes to express their experiences of body shape and weight).296–298 Athletes should be educated to recognise signs and behaviours that may be associated with eating disorders and RED-S, including overexercise, rigid eating patterns, amenorrhoea, a focus on thinness and a competitive comparison of physiques.299 A strong coach–athlete relationship may protect against eating disorders.300 Coaches need to understand the physiologic importance of proper nutrition and weight management.301–303 Coaches should feel comfortable discussing eating disorders and RED-S with athletes.299 One strategy to decrease stigma is to reframe these disorders as a continuum of sport-related injury and illness.304
Attention-deficit/hyperactivity disorder
The essential features of attention-deficit/hyperactivity disorder (ADHD) are a persistent pattern of inattention and/or hyperactivity–impulsivity causing dysfunction and present in multiple spheres since prior to the age of 12 years (table 7). A formal diagnosis of ADHD may be made based on patient history, using DSM-5 diagnostic criteria.1 Other data, such as those obtained from neurocognitive testing, laboratory results and collateral information, may support a diagnosis, rule out other conditions or both.305
Diagnostic and Statistical Manual of Mental Disorders-5 diagnostic criteria for attention-deficit/hyperactivity disorder1
Using DSM-5 criteria, 30% of those diagnosed with ADHD in childhood continue to meet ADHD criteria as adults.306 307 There are scant data regarding the prevalence of ADHD in elite athletes; however, ADHD may be more common than in the general population, since individuals with ADHD may be drawn to sport due to the positive reinforcing effects of physical activity.306 308 However, the sport-related hyperactivity manifest in some athletes must be distinguished from diagnosable ADHD.309
Athletes with ADHD who suffer concussions should be evaluated for comorbid or persistent concussion symptoms, since there is symptom overlap between concussion and ADHD.310–314 Both conditions affect similar neurocognitive domains, resulting in possible deficits in memory, attention and concentration.315 316 Collegiate athletes with ADHD are more likely to report a past history of concussions than those without ADHD, and ADHD may be associated with prolonged recovery following sport-related concussion in athletes.317 318
ADHD may negatively affect athletic performance.305 Lack of focus and concentration, oppositional behaviour, argumentative attitude, frustration, lowered self-esteem and labile mood may all interfere with performance.305 ADHD may cause academic difficulties that could threaten the academic eligibility of student athletes.305 Additionally, commonly described comorbid conditions such as anxiety, depression and substance use disorders may negatively impact performance.305 However, some individuals with ADHD naturally excel in sport because of quick and reactive decision making due to inherent impulsivity.319
In managing ADHD in elite athletes, psychosocial interventions should be used;57 these interventions may be as effective as—and should be considered an alternative to—stimulant medication in athletes with mild functional impairment.306 309 320–325 Depending on the age of the elite athlete, treatment may include: behaviour therapy or CBT; individual education plans; parent teaching/training and caregiver support; and education for athletes, families and coaches.308 321 326
Stimulants are a primary pharmacological treatment for ADHD.62 211 306 309 321 322 324 325 327 Such medications, including those in the methylphenidate and mixed amphetamine salts classes, may be ergogenic,328 329 and are misused because of the perception of performance enhancement.306 322 324 325 327 330 Like classic stimulants, the psychostimulant modafinil reportedly may mask symptoms of fatigue.331 Stimulants may be misused for weight loss as a performance advantage in leanness sports (eg, distance running) or in sports with weight classes (eg, wrestling).309 327 Stimulants are prohibited by WADA in competition,59 332 so athletes taking them for legitimate medical reasons must receive a TUE.333
Athletes taking stimulants may be able to exercise to higher core body temperatures without perceived thermal stress,212 thereby raising concerns about both performance enhancement and safety.212 Stimulants may cause several side effects, including insomnia, anxiety, increased heart rate and blood pressure, and an undesired decrease in appetite, all of which can negatively impact performance and threaten athlete safety.211 306 309 322 324 325
Given these concerns, if medications are necessary for an athlete with ADHD, non-stimulant medications should be considered.309 324 327 334 The non-stimulant atomoxetine is a medication of choice for ADHD among sports psychiatrists, presumably owing to the regulatory and safety drawbacks of stimulants.57 However, it has not been studied in elite athletes. In addition, prescribers and athletes should be aware that it takes much longer to see full benefit from atomoxetine than from stimulants,309 and gastrointestinal discomfort and sedation are possible side effects.327 Bupropion, an antidepressant with some stimulant properties, is sometimes used off label for ADHD,306 322 335 especially for individuals with comorbid depression. Clonidine and guanfacine in extended release formulations are approved in some countries for use in children under the age of 18 years with ADHD (which could include elite athletes).325 336 These latter two medications have not been studied in elite athletes, but sedation and cardiac side effects such as hypotension, bradycardia and QTc prolongation are possible side effects.336 337 Tricyclic antidepressants may also be used off label for ADHD,325 but side effects such as sedation, weight gain, cardiac arrhythmias and dry mouth may preclude their use in elite athletes.305
If stimulants are prescribed and a TUE is approved, it may be preferable to start with long acting formulations, which are more convenient and less likely to be abused.57 324 An alternative potential stimulant prescribing strategy involves use of formulations and timing that allow use only during school, study and work times—not during practices and competition—thereby decreasing concerns about safety and impact on performance.57 324 327 A final important consideration is that prescribers must use caution in prescribing stimulant medication if the athlete is participating in endurance events in hot temperatures because of the possible increased risk of heat illness.60 306 322 324
Bipolar and psychotic disorders
Bipolar disorders are characterised by major changes in mood with associated functional impairments (Box 4). Mood changes may be depressive, hypomanic, manic or occasionally with mixed symptoms.1 Psychotic symptoms need not be present, but if so are usually consistent with the individual’s mood.1 Psychotic disorders such as schizophrenia and related conditions are usually characterised by hallucinations and delusions. In addition, schizophrenia may involve disturbances in speech, thought, behaviour, affect and cognition, in addition to social deficits and significant functional impairment.1
Diagnostic and Statistical Manual of Mental Disorders 5 diagnostic criteria for bipolar I disorder and bipolar II disorder1
Bipolar I disorder
At least 1 manic episode, defined as a distinct period of abnormally and persistently elevated, expansive or irritable mood, and abnormally and persistently increased activity or energy, present most of each day for at least a week (or any duration if hospitalisation is necessary)
3 additional symptoms (4 if mood is only irritable) are present to a significant degree during the manic episode and represent a noticeable change from usual behaviour:
inflated self-esteem or grandiosity
decreased need for sleep
more talkative than usual
flight of ideas or subjective experience that thoughts are racing
distractibility
increased goal directed activity or psychomotor agitation
excessive involvement in activities that have a high potential for painful consequences
The mood disturbance is sufficiently severe to cause marked impairment in social or occupational functioning or to necessitate hospitalisation to prevent harm to self or others, or there are psychotic features
The symptoms are not better explained by another medical condition, a psychotic disorder or a substance.
Bipolar II disorder
At least 1 hypomanic episode, defined as a distinct period of abnormally and persistently elevated, expansive or irritable mood, and abnormally and persistently increased activity or energy, present most of each day for at least 4 consecutive days
Symptom criteria for a hypomanic episode are the same as for a manic episode (second bullet point above)
The hypomanic episode is associated with an unequivocal change in functioning that is uncharacteristic of the individual when not symptomatic
The disturbance in mood and change in functioning are observable by others
The episode is not severe enough to cause marked impairment in functioning, hospitalisation or psychosis
The symptoms are not better explained by another medical condition or a substance
At least 1 major depressive episode has occurred (see criteria in table 1).
Bipolar and psychotic disorders have not been thoroughly studied in elite athletes;61 although prominent cases have been reported,338 the prevalence is unknown. Both disorders show a peak age of onset coincident with the usual age of peak sporting performance;339 thus it is important for clinicians and other key professionals in the world of sport to be aware of their symptoms. In cases of mania and hypomania, the diagnosis may be obscured if sport provides a functional outlet for excess energy, or if overactivity is normalised.340
It is important to distinguish primary mood and psychotic disorders from the impact of substance use (secondary disorders), as the latter may be self-limiting or require only short term treatment (table 8).341 For example, anabolic–androgenic steroid use may be associated with psychotic, hypomanic or depressive symptoms.342 343 Other substances used by athletes, including stimulants, cannabinoids and glucocorticoids, may also be associated with mood or psychotic symptoms.344 345
Features that may help distinguish between primary bipolar and psychotic disorders and those secondary to substance use341–343 345 508
There are scant data on how bipolar and psychotic disorders affect athletic performance. The long term course of bipolar disorders is variable, and patients may spend a significant amount of time in a symptomatic (often depressed) state.346 347 However, some athletes have achieved sporting success despite this condition.
Cognitive and negative symptoms in schizophrenia cause significant impairment of function348 349 likely to interfere with the demands of elite sport.51 Conversely, physical activity may be beneficial for symptoms of bipolar and psychotic disorders,350–352 although some evidence suggests that vigorous exercise may exacerbate mania in patients with bipolar disorder.351 Supported strategies to exit from an elite sports level, perhaps to a lower level of participation, should be considered if this strategy would allow the individual to continue to benefit from physical activity.
There is limited evidence on the treatment of bipolar disorders and psychosis in athletes,61 and guidance is usually based on expert opinion and individualised prescribing.56 Long term medication is often needed alongside psychotherapy interventions,353–358 including family therapy, CBT and, for bipolar disorder, social rhythms therapy.359
Sports psychiatrists have reported preferences for lamotrigine and lithium in athletes with bipolar disorders.60 Lamotrigine has a favourable side effect profile for elite athletes, but does not always prevent or treat mania.56 57 Lithium is a full spectrum mood stabiliser, but its levels may fluctuate with intense exercise and hydration status,360 361 so close monitoring is advised.56 Apart from lamotrigine, most medications for bipolar disorder can cause sedation, weight gain and tremor.57 60 Among the atypical antipsychotics that may be used for bipolar or psychotic disorders, aripiprazole, lurasidone and ziprasidone may be relatively less likely to cause sedation and weight gain.56 57 Ziprasidone may cause QTc prolongation362 and thus may not be a firstline choice within this class for athletes.57 Aripiprazole may cause akathisia, which could negatively impact motor performance in athletes.56 Typical antipsychotics are an infrequent choice for psychotic disorders in athletes because of sedation, motor side effects and cardiac concerns.57
Sport-related concussion
Sport related concussion (SRC) is a traumatic brain injury induced by biomechanical forces. It may be caused by a direct blow to the head, face or elsewhere in the body with a transmitted impulsive force to the head.363 SRC typically results in short lived impairment of neurological function, but signs and symptoms may evolve over minutes to hours. It largely reflects functional brain disturbances, but also may result in neuropathological changes. SRC manifests in a range of clinical signs and symptoms, with or without loss of consciousness; resolution of signs and symptoms usually follows a sequential course, but may be prolonged.363 Finally, the signs and symptoms cannot be explained by drugs, other injuries or comorbidities.317 364 365 Changes in mood, emotions and behaviour are common following SRC; indeed, in the Sport Concussion Assessment Tool, fifth edition,366 most symptoms overlap with those attributable to anxiety and depression.367–369 Thus SRC may be viewed as a neuropsychiatric syndrome.
Rice and colleagues365 performed a systematic review of mental health outcomes of SRC in elite athletes; of 103 studies, 27 met the inclusion criteria for the final analysis. The most common mental health symptoms following SRC reported in these studies were depression, anxiety and impulsivity, but studies were primarily in male athletes, and most were from North America. Only one paper was judged as meeting sufficient methodological rigour and lack of bias: Vargas et al 370 described depression symptoms in 20% of collegiate athletes following SRC. Vargas et al also reported that predictors of depression symptoms included baseline depression symptoms, baseline post-concussion symptoms, lower estimated premorbid intelligence, non-white ethnicity, increased number of games missed following injury and age of first participation in organised sport (more depression symptoms noted in athletes with fewer years of experience in organised sport).
Although acute mood and behavioural symptoms may be common following SRC, such symptoms must be differentiated from mental health disorders. For example, Kontos et al 371 reported significantly worse depression symptoms following SRC, but not at the level of major depressive disorder. No high quality studies exist of other mental health outcomes, such as alcohol or other substance use disorders, personality disturbance or psychotic symptoms, after SRC in elite athletes.365
Most athletes recover from SRC within 7–10 days.372–374 However, up to 21% of athletes remain symptomatic after 30 days.374 Delayed recovery has often been diagnosed as ‘post-concussion syndrome’. This label assumes the presence of common influencers of delayed recovery, but it lacks consensus criteria or clinical specificity, and subsumes varied presentations not clearly associated with the concussive injury.1 363 375–383 Since SRC is not a homogenous entity, persistent symptoms are increasingly described within specific, but often overlapping, post-concussion subtypes and should be managed as such.384
The development of depression, anxiety or other mental health symptoms or disorders following SRC may adversely impact recovery.385 386 Further, pre-injury mood and/or other mental health disorder, family history of mental health disorder and high life stressors before injury all negatively impact SRC recovery.387 Multiple SRCs may predispose to the development of clinically significant depression. Kerr et al 388 reported a 5.8-fold increased risk of depression after 5–9 concussions in retired professional football players, and Guskiewicz and colleagues389 described a 3-fold increased risk of depression following three or more SRCs among retired football players. Similarly, Kerr et al 390 reported a higher prevalence of moderate/severe depression among former collegiate football players with a history of three or more concussions. Although Fralick and colleagues391 found a twofold higher risk of suicide in individuals who experienced concussion and/or mild traumatic brain injury, this study was not athlete or sport specific, and included the general population. Of note, the risk of suicide in former professional football players is significantly lower than in the general population.392
Diagnosis of SRC and associated mental health symptoms or disorders can be challenging.365 For example, there are no objective imaging or blood biomarkers for SRC.373 Nonetheless, neuropsychological evaluation may help differentiate cognitive from other mental health manifestations.393–397
After an SRC, management of persistent mental health symptoms and/or disorders should first address factors that can contribute to delayed recovery, which may include several biopsychosocial issues.365 398–401 Because many athletes with prolonged concussive symptoms reduce their daily exercise markedly, a progressive increase in exercise often ameliorates mental health and somatic symptoms.399 400 402 Additionally, social activity, including team activities, should not be restricted, as such a restriction has been associated with increased depression following an SRC.403 Psychotherapy may be helpful for both mental health and somatic symptoms.375 404 405 Athletes with pre-existing or post-SRC substance use disorders may be more likely to report more SRC symptoms;406 407 thus ascertaining substance use patterns in elite athletes with SRC is important.
There are no approved pharmacological interventions specific to SRC and its sequelae, and evidence to support use of specific medications is minimal.408 While the majority of concussed athletes recover relatively quickly and thus will probably not need medications,374 when such an approach is warranted, targeted treatment beginning with a lower starting dose and a prolonged titration interval is generally indicated.409 410 Intervention for insomnia following SRC should focus on sleep hygiene;408 however, if a sleep aid is warranted, melatonin may be considered408 411 412 with trazodone as a second option.374 408 413 414 Benzodiazepines should be avoided because of their negative effect on cognition.408 413 414 SSRIs may be helpful to treat depressed mood following SRC,408 410 413 415 416 and may simultaneously improve cognition.415 416 Tricyclic antidepressants, for example amitriptyline, are sometimes used to treat headache, depression, anxiety and/or insomnia in the post-SRC setting374 408 417–419 but side effects may limit their use in elite athletes.60 While some evidence exists for the use of stimulants to manage cognitive dysfunction such as deficits in attention and processing speed associated with SRC,408 413 415 420–423 they carry risks415 and are prohibited in competition by WADA without an approved TUE.59
Substance use and substance use disorders (ergogenic and recreational)
Elite athletes use alcohol, caffeine, cannabis/cannabinoids, nicotine and other substances that can be misused for similar reasons as non-athletes.345 424 These reasons can include experimentation, socialisation, pleasure, boosting confidence and increasing alertness and energy. Elite athletes may also use substances for relief of stress, negative emotions, pain, cravings and withdrawal.345 424 Athletes may use ergogenic substances,425 doping methods such as gene doping426 427 and blood transfusions,428 and neuromodulation (eg, transcranial stimulation).429 430 Further, athletes may unwittingly ingest ergogenic substances by taking dietary substances that contain adulterants.431 These practices seek to enhance performance via hoped for increases in strength, power, endurance, aggression, concentration, oxygen carrying capacity of the blood and lean body mass; reductions in fatigue and percent body fat; and enhanced recovery from exercise and injury.345 424
The prevalence of substance use, misuse (defined as heavy, risky, harmful, hazardous or problem use) or full use disorders as defined in DSM-51 among elite athletes varies significantly by substance class,424 432–439 sport,5 439–445 in season versus out of season,434 age/level of competition,424 432 438 445–448 gender,438 439 445 449 450 country,433 437 445 451–455 sexual orientation,456 ethnicity,439 444 457 reasons for use424 458 and prevalence determination methods.433 459–461 Although self-report surveys and competition day urine drug testing are the most common ways of determining use or misuse, these likely are underestimates.460 461 More reliable measures include: athlete biological passport baselines (obtaining an individual’s profile of biological markers of doping over time); team urine surveillance and post-game testing; repeat testing; hair testing; early out of season testing; attitude scale administration; indirect questioning techniques; and interviews with athletes, teammates and parents or coaches.460–464
A few recent high quality studies have compared substance use among athletes and non-athletes. Using indirect comparisons among US collegiate athletes and non-athletes, athletes across all sports report annual use of alcohol, cigarettes, marijuana, amphetamines, anabolic–androgenic steroids, cocaine, ecstasy and lysergic acid diethylamide (LSD) at lower rates than their non-athlete peers.439 465 466 However, in the recent NCAA study (2018) and older US studies that included comparison groups,432 434 448 467–472 collegiate athletes (especially white males) in lacrosse, ice hockey, swimming, baseball and wrestling use more spit tobacco473 and report higher rates of binge drinking and alcohol related problems than non-athletes. Female collegiate athletes in ice hockey, lacrosse and swimming binge drink at higher rates than non-athletes, while women ice hockey players use spit tobacco far more often than non-athletes.473 Male and female collegiate lacrosse players have higher rates of use for both cannabis and cocaine.439 465 466 Recent studies of professional European football players from five countries6 and professional rugby players from eight countries19 showed rates of adverse alcohol behaviours (regular, heavy drinking and/or binge drinking) ranging from 6% to 17%6 and from 8% to 21%, respectively, while a 2015 study of elite rugby players from Australasia using similar measures showed much higher rates of hazardous alcohol use both before (68.6%) and during (62.8%) the season.14 At the collegiate level, a 2017 study by Zanotti et al using the Psychiatric Diagnostic Survey Questionnaire (N=304) showed rates of DSM IV alcohol abuse/dependence of 7.2% to 10.3%,474 confirming previous reports about collegiate athletes’ relatively high rate of alcohol misuse.432 448 468
The most commonly used substances by elite athletes across countries, sports and genders are alcohol, caffeine, nicotine, cannabis/cannabinoids, stimulants and anabolic–androgenic steroids.425 434 435 437 444 459 475–477 Marijuana (inhaled and/or ingested) has replaced nicotine as the second most widely used drug among some elite adolescent and collegiate athletes; it is more likely to be used in places where it is legal, which are becoming increasingly common.437 439 478 Despite relatively low rates of use, synthetic cannabinoids479 and cocaine439 appear to be a growing problem among collegiate athletes, with uncertain year round trends for athletes worldwide.
The sports with the highest general substance use/misuse rates across all substances for men’s elite sports are lacrosse, ice hockey, football, rugby, baseball, soccer, wrestling, weightlifting, skiing, biathlon, bobsleigh and swimming, and lowest for track, tennis and basketball.439 443 459 480 For women’s elite sports, the highest rates occur in ice hockey, gymnastics, lacrosse, softball, swimming and rowing, and lowest in track, tennis, basketball and golf.439 443 459 480 In general, those who participate in team sports are more likely to use or misuse substances than athletes in individual sports.439 442
Common risk factors for use include: sport context and culture (eg, normative beliefs about heavy peer drinking or illicit drug use); situational temptation (eg, drinking games); permissive attitudes among athletes, coaches and parents; male sex; use of performance enhancing substances or tobacco; identification as lesbian, gay, bisexual, transgender or queer; party lifestyle or drinking game participation; sensation seeking; overestimating peer use; achievement orientation; lower use of protective measures (eg, avoiding serious intoxication, using a designated driver); leadership position; fraternity/sorority membership; problem gambling; and injury.442 443 448 450 452 458 468 481–483 Intrinsic religiosity has been inversely associated with the use of alcohol, marijuana and other drugs.484
Substances most commonly used by elite athletes may cause performance enhancement, decrement or both, and the net impact may vary by sport and athlete. Some athletes may use alcohol before competition to reduce anxiety or tremor and improve subjective self-confidence.54 442 485 Alcohol is no longer a prohibited substance in competition in specified sports.59 Post-competition, alcohol is used by some athletes to reduce stress, boost self-esteem, increase social connectedness, improve team cohesion, strengthen athletic identity and raise subjective happiness.54 442 485 Ergolytic effects of alcohol include dehydration, insomnia, higher injury rates, slower injury healing, impaired psychomotor skills, hangovers, accidents, lateness, missing important obligations, reduced metabolic recovery/glycogen re-synthesis, impaired thermoregulation, weight gain and academic underperformance that can threaten athletic eligibility.424 485 486
Although some elite athletes speculate that cannabis/cannabinoids increase the likelihood of obtaining restorative sleep before a competition, reduce pre-competition stress and anxiety to allow for optimal relaxation, or reduce physical pain, no studies have shown a beneficial effect on performance.486 487 In fact, since cannabis is likely to raise heart rate and blood pressure and impair reaction time and coordination,486 it might be expected to limit performance. Regular or heavy cannabis/cannabinoid use may reduce motivation, activate anxiety, trigger psychosis488 or produce temporary disorientation, delirium or aggression.489 490
Ergogenic effects of anabolic–androgenic steroids include enhanced muscle mass, improved biomechanical efficiency and anti-catabolic effects.491 Potential ergolytic effects include cognitive impairment,492 negative mood symptoms,345 psychosis,345 aggression345 and injury, especially tendon rupture.345 Some individuals who use anabolic–androgenic steroids have muscle dysmorphia, a preoccupation that one’s body is not sufficiently lean and muscular, often with significant body image distortion.493–495 Cycles of using anabolic–androgenic steroids are usually interspersed with drug free periods and are sometimes associated with other drug use (eg, diuretics or benzodiazepines) to mitigate side effects.424 491 These other drugs themselves may have ergolytic effects.56 165 174 247
Stimulants may be attractive to elite athletes because they may improve reaction time and concentration, increase arousal, improve memory, boost energy, trigger relaxation and confidence, and improve energy when fatigued.309 424 475 486 496 497 Their negative effects, however, are more apparent in high doses or when combined ('stacked'), which may be relatively common among male athletes who use performance enhancing substances.424 452 Athletes may knowingly or unknowingly consume large amounts of caffeine in dietary supplements, and larger caffeine doses do not appear to increase performance and indeed are more likely to cause side effects.431 Ergolytic effects of high dose stimulant use or combination stacking may include anxiety, insomnia, gastric irritation, tachycardia and tremors.309 424 476 486
Nicotine, whether smoked (eg, via cigars, cigarettes or hookahs), used orally (eg, via moist snuff, snus or leaf tobacco) or vaped, is also widely used by elite athletes.439 Nicotine is currently being studied by WADA because of its potential ergogenic effects on performance and because it is so widely used in some sports, especially baseball, ice hockey and lacrosse.59 486 Athletes’ perception of nicotine’s ergogenic effects include improved alertness and concentration, increased energy and focus, increased muscular strength and power, enhanced endurance, relaxation/calmness, weight control and reduction of boredom, although the results of higher quality studies generally do not support ergogenesis.424 475 486 Ergolytic effects may include elevated blood pressure, anxiety, insomnia and chronic respiratory infections.424 475 486 Potential performance enhancement and decrement associated with other substances by elite athletes, not described in detail here, are documented elsewhere in the literature.345
Interventions for regular, risky or disordered use of substances in elite athletes are not well studied. Nonetheless, approaches to reducing spit tobacco use among baseball players424 498 499 and newer approaches to service delivery models for mental health and substance use disorders in elite athletes provide some guidance.339 500 For spit tobacco use, two approaches used the pre-season physical and dental examinations as an opportunity to screen for heavy nicotine use and examine players for oral lesions. If screening is positive, then a brief intervention by a dental technician or a substance counsellor experienced in tobacco cessation is delivered. In one study,498 after 10 years of annual oral examinations and dental technician interventions, spit tobacco use dropped from 41.1% to 25.6% of players. In more recent models of service delivery, experienced sports clinicians are onsite with teams to integrate substance screenings and brief interventions with other health screenings and interventions.339 500 One model uses experienced mental health/substance providers, who work with the team all year, to conduct screenings for substance use/misuse at the time of the pre-season physical and carry out follow-up evaluations and treatments for those who screen positive. This approach has led to increasing service utilisation rates and problem identification at earlier stages, when problems are easier to treat.424 500 Finally, drug testing is a known deterrent to substance use among athletes,501 and research suggests that increased frequency of drug testing, including during high risk time periods (eg, immediately after a game when athletes are socialising or early in the post-season), may diminish illicit drug use among elite athletes.462
Brief individual or group interventions delivered by clinicians, sometimes with key family members or members of the athlete’s entourage in attendance, may successfully prevent or diminish binge drinking or other substance use in collegiate athletes.502–505 Similarly, binge drinking may be successfully diminished when athletic trainers and academic advisors screen for and deliver brief motivational interventions.506 Group therapy, as an adjunct to medication treatment, is effective when addressing substance use disorders among professional athletes.14 478 507 No research on the use of self-help groups such as Alcoholics Anonymous or Narcotics Anonymous or intensive outpatient or residential treatment of elite athletes is available. While these treatments are evidence based in other populations, concerns about confidentiality may limit elite athletes’ willingness to participate in self-help groups.508
There are no pharmacological studies on treatment of substance use disorders in elite athletes. Such treatment is generally grounded in psychosocial modalities, and pharmacotherapy is used to manage withdrawal and cravings and to treat comorbid mental health symptoms or disorders, such as insomnia, anxiety or depression.508 There are unique implications for treatment of opioid use disorder in elite athletes because treatment often involves use of opioid agonists (eg, methadone and buprenorphine). Since these are prohibited in competition by WADA,59 elite athletes falling under WADA’s governance require a break from training and competition if such an approach is utilised.53 Because alcohol is the most commonly used substance among elite athletes, alcohol use disorder may occur in this population; naltrexone, acamprosate and disulfiram are treatment options for this disorder when cravings are strong or persistent and when the athlete is unable to stop use on their own.53 Since heavy oral nicotine use is also seen frequently in some sports and can be accompanied by tolerance, physiological dependence and cravings, pharmacological strategies for moderate to severe nicotine use disorders in elite athletes should be considered. These include nicotine replacement therapy with or without bupropion, varenicline or bupropion plus varenicline.509–511 Electronic cigarettes or nicotine vaping devices are not recommended for use in elite athletes since their safety and effects on respiratory function have not been established.512 513
Gambling disorder and other behavioural addictions
Many behavioural addictions may negatively impact an athlete’s functioning, but most studies have focused on gambling disorder.514 Gambling disorder, as described by the DSM-5,1 involves at least 12 months of persistent and recurrent problematic gambling with resultant negative consequences. Individuals with gambling disorder report decreased athletic and academic performance, comorbid mental health symptoms and disorders (eg, anxiety, depression and substance use disorders), interpersonal difficulties and legal concerns (theft or embezzlement to support their gambling).514–516
Along with technological advances, attitudes toward gambling have changed. It is now a socially accepted, easily accessible form of entertainment.517 Gambling disorder is regarded as a 'hidden disorder', and mental health professionals have reported relative lack of awareness and concern about gambling as a potential problem.518 Relatively few studies have examined the impact of gambling disorder. Elite athletes may be particularly at risk for gambling disorder, given their overrepresentation of young males, which is a known high risk group.514 519–521 Additional risk factors for elite athletes include their desire for competition and challenges, high levels of sensation seeking and impulsivity, and increased risk taking behaviours.522–525
Early studies that assessed North American collegiate athletes found prevalence rates of disordered gambling between 5.2%526 and 6.2%.527 Weiss and Loubier521 reported that both former and current athletes had the greatest likelihood of problem gambling (13.0% and 7.0%, respectively) compared with non-athletes (3.0%). In the NCAA’s study of North American collegiate athletes between 2004 and 2016, over 84 000 male collegiate athletes self-reported prevalence rates of disordered gambling of between 0.7% and 2.0%. However, those athletes at risk (not meeting the clinical criteria for gambling disorder, but self-reporting serious gambling related problems) comprised between 1.1% and 2.9% of the sample.522 Thus the results suggest that between 1.8% and 4.0% of respondents have serious gambling related problems. Importantly, assessment measures have differed among studies, as have the availability and accessibility of gambling opportunities. Additionally, the NCAA study assessed athletes where gambling by collegiate athletes was prohibited. In a study among professional athletes from Spain, France, Greece, Ireland, Italy, Sweden and the UK, 56.6% participated in some form of gambling during the past year, and 8.2% had a gambling problem (either current or in the past). In particular, problem gambling was related to wagering on one’s own team, betting online and gambling regularly.520
Several other behavioural disorders, including excessive gaming, Internet and social media use, may be of concern in athletes but are not DSM-5 diagnoses and have received little research attention. In one case study, a professional baseball pitcher experienced an injury after excessively playing a video game.528 Others have argued that Wii Sports software may be helpful for rehabilitation of athletic injuries.529 Some papers describing excessive professional gaming in electronic sports ('e-Sports') have questioned whether professional gamers who spend 10 hours or more a day practising and competing are 'addicted' to gaming or work.530–532
While also not included as a behavioural addiction in the DSM-5, excessive exercise shares behaviours with other addictive behaviours.533 Prevalence rates of 'exercise addiction' among athletes have varied considerably. Szabo and Griffiths534 reported that 6.9% of British sports science students were at risk for an exercise addiction. Blaydon and Linder535 reported that 30.5% of triathletes could be diagnosed with exercise addiction, with another 21.6% approaching an addiction. Allegre et al 536 reported that 3.2% of ultra-marathoners displayed signs of an exercise addiction. Several studies have reported a significantly greater risk for exercise addiction in elite athletes compared with recreational exercisers.537 In the elite population, it may be challenging to distinguish exercise addiction from normative and adaptive high level training, but some characteristics may help with that distinction (table 9).537 538
Features of 'exercise addiction' versus normative/adaptive exercise in elite athletes538 738–741
Eating disorders often are comorbid with exercise addiction in athletes.290 539 Some researchers distinguish primary exercise addiction, in which there is no accompanying eating disorder and exercise is the primary objective, from secondary exercise addiction, in which weight loss is the objective, with excessive exercise being one of the primary means in achieving the objective.540–542
There is a growing body of clinical evidence that behavioural disorders can be successfully treated.514 The most common approaches include motivational interviewing and CBT.514 543 Coaches, trainers and team physicians are in a unique position to identify and address these concerns.522 544
Major stressors and key environmental factors that influence elite athlete mental health
In addition to the specific mental health issues mentioned above, the IOC expert group also considered the larger social environment in which elite athletes operate. We share our consensus findings on: harassment and abuse; how injury, performance and mental health interesect; barriers to seeking care for mental health symptoms and disorders; the athete’s transition out of sport; mental health emergencies; and how it may be possible to create an environment that promotes mental well-being and resilience.
Harassment and abuse (non-accidental violence)
The risk of non-accidental violence in elite sport environments—whether psychological, physical or sexual abuse, or neglect—requires policies and procedures to protect athletes (table 10).266 Non-accidental violence is the term used by the United Nations and the IOC to describe harms experienced by athletes because of an abuse of actual or perceived differentials in power, based in a cultural context of discrimination.266 Psychological abuse is considered the basis for all other forms of non-accidental violence and is the most prevalent in sport.545 The four types of non-accidental violence may occur in isolation or in combination, and may be a one time occurrence, continuous or repetitive. Non-accidental violence can manifest via different mechanisms, including contact, verbal or cyber mechanisms, negligence, bullying or hazing (figure 2).
International Olympic Committee definitions: types of non-accidental violence in sport266
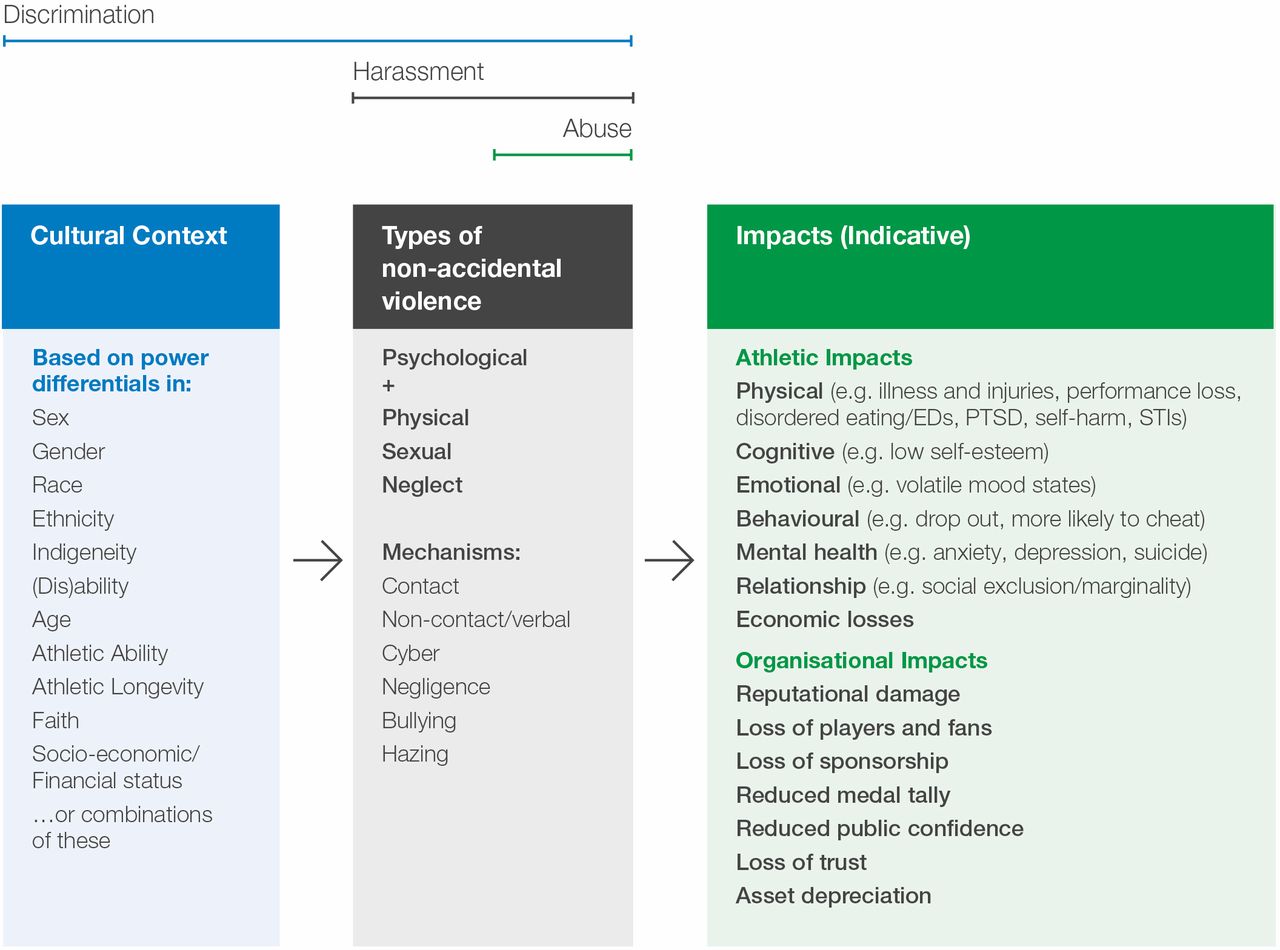
{kind=link}
{kind=link}
Framework of non-accidental violence in sport, as adapted from the International Olympic Committee.266
Non-accidental violence occurs in all sports and at all levels,546–548with a greater risk for psychological, physical and sexual abuse at the elite level.546 549 High risk sport populations for non-accidental violence include: child athletes;550 athletes who identify as lesbian, gay, bisexual,transgender, or queer;551 and athletes with a disability.549 Underreporting is a significant concern and limits conclusions about the prevalence of non-accidental violence of any form among elite athletes.552 Stafford reports that the prevalence of psychological abuse approaches 75% in youth athletes.553 The reported prevalence of sexual abuse in sport ranges from 2% to 49%.554 Although there are few robust prevalence studies on physical abuse and neglect in sport, many public reports outline these forms of non-accidental violence in sport. Male perpetrators of sexual abuse are reportedly more common than female perpetrators, and female athletes are reportedly more often victims of sexual abuse than male athletes.555 Perpetrators of forms of non-accidental violence may be team physicians,556 coaches, other members of the athlete entourage,557 peers or team mates.558
The impact of non-accidental violence in sport can be devastating and long standing,559 including loss of self-esteem, poor academic performance, distorted body image, eating disorders, self-harm, depression, anxiety, substance use disorders and suicide.560 Non-accidental violence is correlated with willingness to cheat or dope in sport.561 Psychological abuse can lead to impaired athletic performance, reduced medal opportunities, loss of sponsorship and early sport dropout.560 Childhood psychological abuse is a correlate of long term post-traumatic and dissociative symptoms in athletes.562
Athletes can also suffer from indirect non-accidental violence when they witness such events experienced by others and not stopped by others, including those in authority.563 This phenomenon compounds the psychological trauma of the victim, and deters disclosure by athletes.564 Non-accidental violence in sport may also affect the victim’s family, and personal, social and work/school relationships outside of sport.565
An athlete presenting with mental health symptoms to a clinician should be asked about a history of non-accidental violence, either within or outside of sport.566 Sports medicine healthcare providers should develop the clinical competence to recognise non-accidental violence, manage athlete disclosures, report cases and treat victims, their families and their teams.556 It is imperative to ensure immediate athlete safety. Multidisciplinary support should be the cornerstone of management.556 Support for teammates, the athlete entourage and family members may also be appropriate.556 Depending on laws where the abuse occurred, reporting to legal authorities may be required, for example if a child has been sexually abused.556
How injury, performance and mental health intersect
The relationship of injury, performance and mental health in elite athletes is complex.322 567–570 Elite sport has specific stressors that potentially increase the likelihood of injury or illness, including mental health disorders.222 571–576 Injury also can potentially unmask or precipitate mental health disorders.574 Finally, mental health disorders can increase the likelihood of, or complicate recovery from, injury.222 572 573 577 Nonetheless, there is minimal prospective research in this area.
Injury risk factors
Psychological and sociocultural factors are potential risk factors for injury in sport.569 574 575 578 Psychological risk factors include anxiety/worry, hypervigilance, poor body image or low self-esteem, perfectionism, limited coping resources, life event stress (ie, perceived strain associated with major life event stressors such as the death of a family member or starting at a new school), risk taking behaviours or low mood state. Sociocultural risk factors include limited social resources, a lifetime history of sexual or physical abuse,579 social pressures, organisational stress (ie, associated with an athlete’s appraisal of the structure and function of their sports organisation),580 stress related to negative self-appraisal of athletic and academic performance, coaching quality (eg, poor athlete–coach relationship and communication) and the culture of sport and teams (eg, a mindset of 'winning at all costs' vs striving for continual improvement).223 569 574 581
Although there are limited prospective studies coupled with conflicting results regarding risk factors related to injury, life event stress and high stress response (ie, negative emotional responses after sport injury or other stressful events) consistently demonstrate a relationship with injury risk.223 572 574 578 581–585 Life event stress and high stress response can cause inattention, distraction and increased self-consciousness while increasing muscle tension and impaired coordination, all of which can impair performance and increase the risk for injury.223 572 578 581–585 When team mates and coaches are sources of life event stress, there is an associated increased risk of both acute and overuse injuries.581 Emotional reactivity (involuntary and overly intense emotional reaction) is also associated with poor on field performance and injury.222 586 587
Response to and recovery from injury and illness
Cognitive, emotional and behavioural responses are important factors associated with outcome following injury.578 The evidence for outcomes following illness is not well evaluated, but the same processes may occur as after injury. Cognitive responses to injury may include concerns about re-injury, doubts about competency, low self-efficacy, loss of identity and concerns about competency of the medical staff.588 Emotional responses to injury may include symptoms of sadness, depression, suicidal ideation, anxiety, isolation, lack of motivation, anger, irritation, frustration, changes in appetite and sleep, low vigour, disengagement and burnout.7 574 Injured athletes report more symptoms of depression and of generalised anxiety disorder compared with non-injured athletes.11 Whereas emotional responses to injury and illness vary, problematic emotional responses are those that do not resolve, worsen over time or in which the symptoms seem excessive.569 Injury (and possibly illness) may trigger or unmask other behavioural responses or underlying mental health disorders, including disordered gambling, disordered eating or eating disorders, and substance use disorders.26 30 35 192 241 389 483 589–595
Athletes with more positive cognitive, emotional and behavioural responses may have improved injury recovery.35 573 596–606 Higher levels of optimism and self-efficacy and lower levels of depression and stress are associated with improved recovery from injury.35 573 596–605 Examples of strategies that support positive return to sport experiences include: (a) reducing re-injury anxieties using modelling techniques, such as watching videos of formerly injured athletes discussing how they overcame their re-injury anxieties, or pairing an injured athlete with another athlete proficient in certain rehabilitation exercises so the less experienced athlete can learn how to execute the exercises correctly; (b) fostering athlete autonomy (eg, by explaining why they are performing rehabilitation exercises); (c) building confidence through functional tests and goal setting; (d) providing social support; (e) keeping athletes involved in their sport but avoiding premature return to sport; and (f) stress inoculation training when injury requires surgical intervention.604 606
Barriers to seeking care for mental health symptoms and disorders
Elite athletes may encounter many barriers to seeking mental healthcare, including stigma.188 607–615 Public stigma and self-stigma predict a significant detrimental impact on seeking treatment for mental health.616 Additionally, many athletes come from countries where there are few, if any, mental health services, and where there may also be ways of understanding and treating mental health symptoms and disorders outside of evidence and biomedically based ones.617 618 Other barriers can include lack of mental health literacy, negative past experiences with mental health help seeking and busy athlete schedules.188 290 609 610
Facilitators to seeking mental healthcare among athletes include: having an established relationship with a mental health provider; positive previous interactions with mental health providers; perception of benefits to seeking help; a sense of self-efficacy to seek treatment; and the positive attitudes of others, especially coaches, regarding seeking mental health treatment.188 619 620 Even for elite athletes with positive attitudes toward mental health help seeking who express a willingness to engage psychological services, many have concerns regarding how they will be perceived by their peers, coaches and sport managers.611 612 621 Brief mental health literacy and de-stigmatisation interventions improve knowledge and may decrease stigma but may not be enough to increase help seeking.289 502 505 622–627
Negative attitudes about mental health services are associated with several factors, including identification as male, younger age, Black (vs Caucasian) race, US (vs European) nationality, lower measures of openness, higher measures of conscientiousness, gender role conflicts and participation in physical contact sports.628–632 Conversely, coaches can be important advocates of promoting positive attitudes about mental health by being mindful of early identification and referral of athletes with possible mental health symptoms and disorders to mental health services.607 Moreover, athletes with stronger positive coping skills generally have attitudes more supportive of seeking mental health help.291 Finally, athletes have strong preferences for counsellor characteristics, such as familiarity with their sport, same gender, older but still close enough in age to understand their lives and geographic proximity to the sports facility.633–636
Cultural issues within sport have broad reaching effects that impact elite athletes differently, depending on their own cultural identities, including gender, gender identity, sex, sexual orientation, race, ethnicity, socioeconomic status and religion.55 Cultural influences and discrimination related to cultural factors may leave some athletes at a performance disadvantage and set the stage for mental health symptoms or disorders.
As women continue to engage in elite sport opportunities, their participation has led to varying degrees of cultural acceptance.637 Women competing in sports traditionally considered 'male' may face being marginalised and stereotyped638 and may experience unequal training opportunities and resources.639 Sexualisation, traditional gender roles, religion and ethnic beliefs all influence opportunities for women.640 For example, women of some religions may experience difficulty combining traditional roles with competition as an elite athlete, as related to religious rules about the body and presentation in public.640 Tension may also exist between what is functionally optimal for women elite athletes to be wearing and what is culturally deemed acceptable.641 642 Gender stereotyping in the media may influence how women athletes view themselves.641 Women athletes may be stereotyped as 'lesbian' to keep them from playing certain sports, or from playing for certain coaches or with certain teams.641 Some professional women athletes must train outside their native countries643 and may struggle to find a support network and cultural understanding from team mates in their new location.644
Sexuality and cultural norms of masculinity in elite sport also impact elite athletes.645 Non-heterosexual athletes face various degrees of acceptance,646 and this may interfere with sports performance.646 647 Transgender athletes often have negative experiences in sports and may struggle to be accepted,648 even after they meet criteria allowing them to participate.649
Racial disparities—including those involving exploitation, player–coach tension, prejudicial treatment and microaggressions—in addition to socioeconomic inequities, form barriers that may prevent equal opportunities.650–654 For example, access to wealth has predicted participation and success at the Olympic Games.655 Importantly, discrimination based on any aspect of cultural identity may come from several sources, including coaches, team mates, agents, universities, leagues, managers, healthcare providers or others.
Transition out of sport
Epidemiological evidence suggests that elite athletes transitioning out of sport are at risk of developing mental health symptoms and disorders. As in current athletes, most studies have relied on self-reported cross sectional data. These reports show that the prevalence of mental health symptoms and disorders in former elite athletes ranges from 5% for adverse alcohol use to around 45% for anxiety and depression.13 16 22 34 590 656–661 Few studies have prospectively explored mental health disorders in former elite athletes; those that have done so reported incidence rates from 5% to 30% over a follow-up period of up to 12 months.13 16 18 662
While transitioning out of elite sport, generic and sport specific factors are likely to interact and increase the risk of mental health symptoms and disorders among athletes.31 32 663 Undesired and involuntary retirement from sport (eg, because of injury or deselection from sport) is especially associated with an increased risk of mental health symptoms and disorders among transitioning athletes.8 661 664–668 Concussion in sport is associated with subsequent mental health symptoms and disorders among retired elite athletes; however, a causal relationship has not been established.16 390 594 669–672 Other factors associated with adjustment difficulties and mental health symptoms and disorders among former elite athletes include high levels of athletic identity, lack of retirement planning, lower educational attainment, adverse life events, post-sport unemployment and chronic pain.9 18 662 668 673 674
Stakeholders in elite sport have considered how to protect and promote the long term health of elite athletes beyond retirement. For example, an ‘exit health examination’ focusing on mental health indicators may promote sustainable health and quality of life.675 676 This could be particularly important for former elite athletes at risk for mental health disorders, especially those retiring from sport involuntarily. Additionally, thorough preparation for post-sport life may help mitigate mental health disorders during transition out of sport.668 Accordingly, education programmes/seminars, practical resource centres, and mental and life skills training for career transition could be offered to elite athletes across their sport career.668 677 Finally, clinicians can help athletes to become aware of, develop and use transferable skills that may provide direction, meaning and motivation in their post-sport life.660
Mental health emergencies
A mental health emergency refers to immediate risk in the context of a disturbed mental state.678 679 Risks are typically to the health and/or safety of the athlete or others.678 Data on prevalence in elite athletes are sparse. Some circumstances within sport may carry an increased risk of mental health emergencies. For example, deselection is linked to acute adverse emotional reactions.680 Sporting injuries are associated with anger and depression,681 which are in turn associated with an increased suicide risk.682 Periods of injury may also necessitate time away from sport and a further increased risk of suicide.683
Substances misused by elite athletes may also contribute to a higher risk of mental health emergencies. Use of anabolic–androgenic steroids is linked to hypomanic or psychotic symptoms, aggression and even suicide.342 343 Longitudinal studies lend support to these links,684 685 and symptoms are more likely with the high doses and multiple agents misused by athletes.341 342 Symptoms can emerge rapidly,686 but may be self-limiting or require only short term treatment.341 Current users may experience mood changes with suicidal thinking and impulsivity; discontinuation leads some to descend into depression with more planned suicidal ideation.687 Both scenarios carry significant risks, and death by suicide is 2–4 times greater in male athletes who may have used anabolic–androgenic steroids compared with the general population.591 Stimulant use may lead to acute mood disturbance, aggression and psychosis.344 345 Marijuana and synthetic cannabinoids are associated with acute psychosis,688 689 but there are no athlete specific data.
Athletes’ patterns of alcohol consumption tend more towards binge drinking;444 thus acute intoxication may be a more likely emergency presentation than physical dependence and/or withdrawal. Retired athletes may also be at greater risk for mental health emergencies associated with heavy alcohol use compared with their non-sporting peers.690 Acute concerns in eating disorders are often medical (eg, fracture risk, electrolyte abnormalities and electrocardiographic changes) and may be severe enough to warrant deselection.274 286 If so, then there is a risk of emotional decompensation, and urgent clinical evaluation may be needed.691 Limited data suggest that borderline (along with obsessive–compulsive) subtypes are the the most common personality disorders found in sport.692 Borderline personality disorder is associated with impulsivity, risk taking, frequent suicidal behaviours, an unstable affect and interpersonal difficulties.1 These features alone, or especially in combination, may promote an emergency mental health presentation.
There is little to guide the choice of pharmacological treatments for mental health emergencies in elite athletes.57 Benzodiazepines and/or antipsychotics by oral or parenteral routes are all used to tranquillise a person with an acutely, severely and dangerously disturbed mental state.679 693 Sports specific treatment concerns include the performance impact of motor symptoms, weight gain or sedation,56 57 but these concerns may be less relevant when only short term treatment is required.
When conducting an emergency mental health assessment, the physical environment should be uncluttered and provide both containment and escape routes.678 However, such environments may be unavailable when assessing an athlete at a training or competition venue.694 Although pathways and available personnel may differ from country to country,339 it is best practice to develop and rehearse a mental health emergency action management plan for all relevant sport stakeholders. This plan should include clarity on what constitutes an emergency, who should be contacted and when, and familiarity with local emergency services and mental health legislation. Plans should be consistent with other emergencies in sport, such as cardiac arrest, heat illness and severe trauma. A review of procedures after any incident can be very helpful.567
Creating an environment that supports mental well-being and resilience
The diagnosis and management of mental health symptoms and disorders is a separate but related continuum with athlete well-being.695 696 Within sport, coaches are often the primary interpersonal interface with the athlete. They can support diagnosis and management of mental health symptoms and disorders by creating a destigmatising environment wherein mental health help seeking is a core function of training and self-care.697 698 Coaches can attend to athlete stressors that may diminish well-being and predispose to mental health symptoms and disorders, including training load and recovery,699 700 injury,22 322 700 burnout701 and retirement.241 Coaches can ensure that training is age and developmentally appropriate.702–704 For younger elite athletes, coaches can communicate the importance of mental healthcare to parents, thereby managing expectations about avoiding stressors and seeking care when appropriate.705
Coaches can foster positive psychosocial development and well-being by helping athletes learn to respond to stressors in healthy ways.698 706 707 This includes helping athletes learn skills that promote resilience,708 psychological flexibility,709 self-compassion710 and adaptation to situational demands while staying consistent with one’s values.709 In day to day training, coaches can de-emphasise achievements and outcomes and instead foster a process oriented mindset, in which effort and improvement are emphasised.711 Such an approach may help mitigate performance related anxiety712 and attrition from sport713 while optimising the positive psychological experiences of sport participation.714
Organisations can support athlete mental health by providing coaching education that is evidence based and efficacious.622 698 715–719 Effective delivery of coaching education is more likely if it falls within the framework of coaching duties and expectations.705 Resource allocation, priorities and outcomes or behaviours that are rewarded (well-being vs win–loss record) show coaches whether mental health is viewed as an organisational priority. Intentional time allocation in the athlete’s normal practice schedule for learning positive psychosocial skills is associated with better developmental outcomes.720 Sport governing bodies can further influence athlete mental health by requiring or recommending that coaches undergo mental health training.291 Ultimately, sport can positively influence society to promote well-being and de-stigmatise mental health help seeking.721
Special considerations: mental health in Paralympic athletes
Paralympic sport is sport for people with disabilities. Paralympic athletes use adapted equipment or rules to make sport accessible to individuals with impairments. In general, sport is often heralded for its ability to promote mental health, and there is a largely unexamined assumption that participation in Paralympic sport improves an athlete’s psychological well being.722 However, research concerning the mental health of athletes with disabilities is minimal.723
Rates of mental health symptoms and disorders, specifically depression, among the general population of people with disabilities are reported to be higher than in non-disabled individuals.724 Nonetheless, a review of 12 studies of Olympic and Paralympic athletes demonstrated that most indices of well-being (eg, physical confidence, physical self-worth, self-regard, self-actualisation, self-acceptance, confidence and self-efficacy) were similar in the two groups.725 Emerging research suggests that athletes making a Paralympic team may have lower rates of depression and anxiety than those trying out for but not making a Paralympic team.723 While eating disorders in Paralympic athletes have received little research attention, those who restrict their food intake may be at greater risk for complications from low energy availability, especially low bone mineral density, because of factors such as altered skeletal loading.280 Finally, athletes with intellectual and physical impairments, as a subset of Paralympic competitors, may have unique mental health challenges, but specific research is particularly sparse.724
Elite athletes with disability experience both sport specific and disability specific stressors that may contribute to mental health symptoms and disorders.724 Stressors that disproportionately and commonly affect elite athletes with disabilities include: chronic pain; overtraining and injury in often complex medical situations (eg, with the need to distinguish sport fatigue, discomfort from the underlying disability and sport injuries); lack of sufficient adaptive sport facilities; logistical difficulties in getting to competition sites; challenging sleep conditions and inferior sleep quality in Paralympic villages; recent rapid escalation of Paralympic sport competitiveness and associated rapid increases in training demands; malfunctioning sports equipment; costs associated with new technology; negative coaching behaviours (eg, demeaning comments); and being ‘misclassified’ or assigned to the wrong disability category for competition.724 726–729
There is little published work on the management of psychosocial stressors or mental health symptoms and disorders in Paralympic athletes. Studies that exist usually had very small sample sizes, did not use standardised measures of psychopathology and relied on unsophisticated statistical analysis. Some attention has been given to the use of psychological skills training to promote peak performance by Paralympic athletes, independent of a history of mental health disorders.724 Psychological skills training entails systematically training athletes to use mental skills—such as regulating anxiety, sustaining motivation, focusing attention and maintaining concentration—to enhance sport performance.724 Addressing insufficient sleep may be particularly relevant, as athletes with disabilities may be at high risk for sleep disorders.730
Given the relative prominence of research regarding social factors among athletes with disabilities, disability exclusion may be an important issue when working with these athletes.731 For example, Paralympic athletes may report feelings of powerlessness and invisibility;732 accordingly, athletes with disabilities benefit from coaches who are trained to be supportive of athletes’ autonomy,733 734 and sport performance may improve as a result.735 Additionally, as with non-disabled athletes, retirement from sport is an important time of transition for Paralympic athletes.724 Many Paralympians start their careers shortly after the onset of disability.724 Consequently, with relatively short lived professional sport careers, some face the challenge of simultaneously needing to adjust to a relatively new disability and preparing for retirement from sport; providers should be aware of these dual transitions.723 724
Future directions
The current state of the science of mental health in elite athletes suggests possible future direction for additional research, change in clinical practice and optimisation of environmental factors. These include:
The relative lack of access to mental health services in some countries and cultures must be considered as research is undertaken and clinical services developed. A rigorous, evidence based approach to mental healthcare should be utilised across countries, but nuanced approaches to provision of that care might be needed, for example by incorporating into the mental healthcare team people such as athletic trainers, physical therapists, coaches and others in the athlete’s entourage and community. If mental healthcare for elite athletes is to be equitably available globally, researchers and practitioners must engage with any emerging evidence and lessons from the global mental health field.
More thorough and reliable mental health epidemiology in elite athletes is needed, with attention to cross cultural differences in manifestations of symptoms and disorders. There are particularly sparse data on bipolar and psychotic disorders, mental health emergencies and athletes with disabilities.
More robust data on pre-existing mental health symptoms and disorders as risk factors for subsequent concussion, and on mental health implications of sub-concussive impact, are needed.
While future research should be clear about whether mental health symptoms versus full disorders are being measured, athletes with symptoms and not full disorders must remain a focus of research attention, as symptoms themselves can be problematic for elite athletes. Increased understanding of risk factors for development of full disorders from earlier symptomatic stages needs clarification within elite athletes.
More research on and subsequent recommendations for expanded mental health screening of elite athletes is needed. Screening is often an important step to ensure that more affected elite athletes ultimately receive the treatment they need. Timing of screening must be carefully considered, given that risks, such as those that occur with injury, may increase at various times throughout an elite athlete’s career. There may be benefit from athlete specific screening tools being developed across diagnostic categories where they do not yet exist, taking into consideration potential unique manifestations of these conditions in this population while also appreciating the limitations to sole reliance on rating scales in the absence of clinical interview. To be able to develop optimal assessment methodologies and screening tools, we need better understanding of the unique symptom manifestations in athletes, which may require both qualitative and quantitative study across countries and cultures.
A better understanding of physiological recovery and optimum readiness—including physical and psychological—to return to play after an injury or illness must be developed. The impact of sleep on recovery and on optimum readiness must be considered in this context.
Additional research is needed on treatments, including psychotherapy and pharmacological treatment, for mental health symptoms and disorders in elite athletes. Methodology should address the limitations that exist in the pharmacologic research to date. Cross cultural considerations include types of therapies and medications/supplements disproportionately used in some countries and cultures, but for which an evidence base may be relatively lacking. Pharmacological intervention for post-concussion mental health symptoms also needs further study, for example addressing duration of recommended treatment for apparent new onset depression and anxiety associated with concussion.
Additional prevention strategies for mental health symptoms and disorders are needed. For example, comprehensive strategies for preventing eating disorders and substance use disorders, especially within high risk elite sports, are needed. Furthermore, more widespread implementation of prevention strategies for non-accidental violence in elite sport is needed.
Strategies that more effectively overcome stigma for elite athlete populations must be developed, such that members of this population come to understand that the 'mental toughness' required for success in sport is compatible with mental health help seeking.
A better understanding of sport as a subculture within society is needed, including which elements of that subculture are particularly conducive to positive mental health outcomes. While much of the research in this area focuses on coaching interventions, roles for other members of the athlete entourage, including parents and other caregivers through their involvement in developmental factors that may lead to ultimate positive adjustment in elite sport, should be studied. Interventions need to distinguish between impact on mental well-being, and on actual mental health symptoms and disorders.
Olympic villages and similar areas should be designed and assessed with sleep hygiene in mind.
Researchers need to better understand the societal and sport specific impact of sport sponsorship by companies that promote alcohol, tobacco and other products associated with adverse mental health outcomes in elite athletes.
Coaches, athletes and stakeholders should be empowered with relevant information so that they recognise the importance of creating an environment that supports mental wellness and mental health help seeking.
Conclusion
The IOC has committed to improve the mental health of elite athletes, recognising that doing so will reduce suffering and improve quality of life in elite athletes and serve as a model for society at large. The IOC hopes that all involved in sport will increasingly recognise that mental health symptoms and disorders should be viewed in a similar light as other medical illnesses and musculoskeletal injuries; all can be severe and disabling, and nearly all can be managed properly by well informed medical providers, coaches and other stakeholders.
Mental health is an integral dimension of elite athlete well-being and performance and cannot be separated from physical health. Mental health assessment and management in elite athletes should be as commonplace and accessible as their other medical care; ideally elite athletes should have access to the best interdisciplinary care. To advance a more unified, evidence informed approach to mental health assessment and management in elite athletes, the IOC Consensus Group has critically evaluated the current state of the science and practice of mental health in elite athletes.
Acknowledgments
The authors acknowledge Mary E Hitchcock, Senior Academic Librarian, Ebling Library for the Health Sciences, University of Wisconsin-Madison, for conducting systematic literature reviews for this manuscript; Sarah E Watkins from Raccoona Editing and Laura Arnett, NCAA Sport Science Institute Coordinator, for manuscript preparation; and Torbjorn Soligard, International Olympic Committee Medical and Scientific Department, for participation in the consensus meeting.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.↵
- 203.↵
- 204.↵
- 205.↵
- 206.↵
- 207.↵
- 208.↵
- 209.↵
- 210.↵
- 211.↵
- 212.↵
- 213.↵
- 214.↵
- 215.↵
- 216.↵
- 217.↵
- 218.↵
- 219.↵
- 220.↵
- 221.↵
- 222.↵
- 223.↵
- 224.↵
- 225.↵
- 226.↵
- 227.↵
- 228.↵
- 229.↵
- 230.↵
- 231.↵
- 232.↵
- 233.↵
- 234.↵
- 235.↵
- 236.↵
- 237.↵
- 238.↵
- 239.↵
- 240.↵
- 241.↵
- 242.↵
- 243.↵
- 244.↵
- 245.↵
- 246.↵
- 247.↵
- 248.↵
- 249.↵
- 250.↵
- 251.↵
- 252.↵
- 253.↵
- 254.↵
- 255.↵
- 256.↵
- 257.↵
- 258.↵
- 259.↵
- 260.↵
- 261.↵
- 262.↵
- 263.↵
- 264.↵
- 265.↵
- 266.↵
- 267.↵
- 268.↵
- 269.↵
- 270.↵
- 271.↵
- 272.↵
- 273.↵
- 274.↵
- 275.↵
- 276.↵
- 277.↵
- 278.↵
- 279.↵
- 280.↵
- 281.↵
- 282.↵
- 283.↵
- 284.↵
- 285.↵
- 286.↵
- 287.↵
- 288.↵
- 289.↵
- 290.↵
- 291.↵
- 292.↵
- 293.↵
- 294.↵
- 295.↵
- 296.↵
- 297.↵
- 298.↵
- 299.↵
- 300.↵
- 301.↵
- 302.↵
- 303.↵
- 304.↵
- 305.↵
- 306.↵
- 307.↵
- 308.↵
- 309.↵
- 310.↵
- 311.↵
- 312.↵
- 313.↵
- 314.↵
- 315.↵
- 316.↵
- 317.↵
- 318.↵
- 319.↵
- 320.↵
- 321.↵
- 322.↵
- 323.↵
- 324.↵
- 325.↵
- 326.↵
- 327.↵
- 328.↵
- 329.↵
- 330.↵
- 331.↵
- 332.↵
- 333.↵
- 334.↵
- 335.↵
- 336.↵
- 337.↵
- 338.↵
- 339.↵
- 340.↵
- 341.↵
- 342.↵
- 343.↵
- 344.↵
- 345.↵
- 346.↵
- 347.↵
- 348.↵
- 349.↵
- 350.↵
- 351.↵
- 352.↵
- 353.↵
- 354.↵
- 355.↵
- 356.↵
- 357.↵
- 358.↵
- 359.↵
- 360.↵
- 361.↵
- 362.↵
- 363.↵
- 364.↵
- 365.↵
- 366.↵
- 367.↵
- 368.↵
- 369.↵
- 370.↵
- 371.↵
- 372.↵
- 373.↵
- 374.↵
- 375.↵
- 376.↵
- 377.↵
- 378.↵
- 379.↵
- 380.↵
- 381.↵
- 382.↵
- 383.↵
- 384.↵
- 385.↵
- 386.↵
- 387.↵
- 388.↵
- 389.↵
- 390.↵
- 391.↵
- 392.↵
- 393.↵
- 394.↵
- 395.↵
- 396.↵
- 397.↵
- 398.↵
- 399.↵
- 400.↵
- 401.↵
- 402.↵
- 403.↵
- 404.↵
- 405.↵
- 406.↵
- 407.↵
- 408.↵
- 409.↵
- 410.↵
- 411.↵
- 412.↵
- 413.↵
- 414.↵
- 415.↵
- 416.↵
- 417.↵
- 418.↵
- 419.↵
- 420.↵
- 421.↵
- 422.↵
- 423.↵
- 424.↵
- 425.↵
- 426.↵
- 427.↵
- 428.↵
- 429.↵
- 430.↵
- 431.↵
- 432.↵
- 433.↵
- 434.↵
- 435.↵
- 436.↵
- 437.↵
- 438.↵
- 439.↵
- 440.↵
- 441.↵
- 442.↵
- 443.↵
- 444.↵
- 445.↵
- 446.↵
- 447.↵
- 448.↵
- 449.↵
- 450.↵
- 451.↵
- 452.↵
- 453.↵
- 454.↵
- 455.↵
- 456.↵
- 457.↵
- 458.↵
- 459.↵
- 460.↵
- 461.↵
- 462.↵
- 463.↵
- 464.↵
- 465.↵
- 466.↵
- 467.↵
- 468.↵
- 469.↵
- 470.↵
- 471.↵
- 472.↵
- 473.↵
- 474.↵
- 475.↵
- 476.↵
- 477.↵
- 478.↵
- 479.↵
- 480.↵
- 481.↵
- 482.↵
- 483.↵
- 484.↵
- 485.↵
- 486.↵
- 487.↵
- 488.↵
- 489.↵
- 490.↵
- 491.↵
- 492.↵
- 493.↵
- 494.↵
- 495.↵
- 496.↵
- 497.↵
- 498.↵
- 499.↵
- 500.↵
- 501.↵
- 502.↵
- 503.↵
- 504.↵
- 505.↵
- 506.↵
- 507.↵
- 508.↵
- 509.↵
- 510.↵
- 511.↵
- 512.↵
- 513.↵
- 514.↵
- 515.↵
- 516.↵
- 517.↵
- 518.↵
- 519.↵
- 520.↵
- 521.↵
- 522.↵
- 523.↵
- 524.↵
- 525.↵
- 526.↵
- 527.↵
- 528.↵
- 529.↵
- 530.↵
- 531.↵
- 532.↵
- 533.↵
- 534.↵
- 535.↵
- 536.↵
- 537.↵
- 538.↵
- 539.↵
- 540.↵
- 541.↵
- 542.↵
- 543.↵
- 544.↵
- 545.↵
- 546.↵
- 547.↵
- 548.↵
- 549.↵
- 550.↵
- 551.↵
- 552.↵
- 553.↵
- 554.↵
- 555.↵
- 556.↵
- 557.↵
- 558.↵
- 559.↵
- 560.↵
- 561.↵
- 562.↵
- 563.↵
- 564.↵
- 565.↵
- 566.↵
- 567.↵
- 568.↵
- 569.↵
- 570.↵
- 571.↵
- 572.↵
- 573.↵
- 574.↵
- 575.↵
- 576.↵
- 577.↵
- 578.↵
- 579.↵
- 580.↵
- 581.↵
- 582.↵
- 583.↵
- 584.↵
- 585.↵
- 586.↵
- 587.↵
- 588.↵
- 589.↵
- 590.↵
- 591.↵
- 592.↵
- 593.↵
- 594.↵
- 595.↵
- 596.↵
- 597.↵
- 598.↵
- 599.↵
- 600.↵
- 601.↵
- 602.↵
- 603.↵
- 604.↵
- 605.↵
- 606.↵
- 607.↵
- 608.↵
- 609.↵
- 610.↵
- 611.↵
- 612.↵
- 613.↵
- 614.↵
- 615.↵
- 616.↵
- 617.↵
- 618.↵
- 619.↵
- 620.↵
- 621.↵
- 622.↵
- 623.↵
- 624.↵
- 625.↵
- 626.↵
- 627.↵
- 628.↵
- 629.↵
- 630.↵
- 631.↵
- 632.↵
- 633.↵
- 634.↵
- 635.↵
- 636.↵
- 637.↵
- 638.↵
- 639.↵
- 640.↵
- 641.↵
- 642.↵
- 643.↵
- 644.↵
- 645.↵
- 646.↵
- 647.↵
- 648.↵
- 649.↵
- 650.↵
- 651.↵
- 652.↵
- 653.↵
- 654.↵
- 655.↵
- 656.↵
- 657.↵
- 658.↵
- 659.↵
- 660.↵
- 661.↵
- 662.↵
- 663.↵
- 664.↵
- 665.↵
- 666.↵
- 667.↵
- 668.↵
- 669.↵
- 670.↵
- 671.↵
- 672.↵
- 673.↵
- 674.↵
- 675.↵
- 676.↵
- 677.↵
- 678.↵
- 679.↵
- 680.↵
- 681.↵
- 682.↵
- 683.↵
- 684.↵
- 685.↵
- 686.↵
- 687.↵
- 688.↵
- 689.↵
- 690.↵
- 691.↵
- 692.↵
- 693.↵
- 694.↵
- 695.↵
- 696.↵
- 697.↵
- 698.↵
- 699.↵
- 700.↵
- 701.↵
- 702.↵
- 703.↵
- 704.↵
- 705.↵
- 706.↵
- 707.↵
- 708.↵
- 709.↵
- 710.↵
- 711.↵
- 712.↵
- 713.↵
- 714.↵
- 715.↵
- 716.↵
- 717.↵
- 718.↵
- 719.↵
- 720.↵
- 721.↵
- 722.↵
- 723.↵
- 724.↵
- 725.↵
- 726.↵
- 727.↵
- 728.↵
- 729.↵
- 730.↵
- 731.↵
- 732.↵
- 733.↵
- 734.↵
- 735.↵
- 736.↵
- 737.
- 738.↵
- 739.↵
- 740.↵
- 741.↵
Supplementary materials
Press release
Footnotes
Contributors All authors meet criteria for authorship, as all have contributed in the following ways: substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of the data; drafting the work or revising it critically for important intellectual content; final approval of the version published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. No one meeting the criteria for authorship has been excluded from authorship.
Disclaimer This consensus paper provides an overview of mental health symptoms and disorders in elite athletes that are important to physicians and other clinicians who treat elite athletes. It is not intended as a clinical practice guideline or legal standard of care and should not be interpreted as such. This consensus paper serves as a guide and, as such, is of a general nature, consistent with the reasonable practice of the healthcare professional. Individual treatment will depend on the facts and circumstances specific to each individual case.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.