Article Text

Abstract
Objective To estimate the incidence proportion (IP) and incidence rate (IR) for ACL injury in athletes.
Design Systematic review with meta-analysis
Data sources The PubMed, CINAHL and SPORTDiscus electronic databases were searched from inception to 20 January 2017.
Eligibility criteria for selecting studies Studies were included if they reported total number of participants/population by sex, total number of ACL injuries by sex and total person-time by sex.
Results Fifty-eight studies were included. The IP and IR of ACL injury in female athletes were 3.5% (1 out of every 29 athletes) and 1.5/10 000 athlete-exposures over a period of 1 season-25 years. The IP and IR of ACL injury in male athletes were 2.0% (1 out of every 50 athletes) and 0.9/10 000 athlete-exposures over a period of 1–25 years. Female athletes had a higher relative risk (RR) for ACL injury compared with males (RR=1.5; 95% CI 1.2 to 1.9; P<0.01) and a higher incidence rate ratio (IRR) of ACL injury compared with males over 1 season–25 years (IRR=1.7; 95% CI 1.4 to 2.2; P<0.010). When accounting for participation level, the disparity in the IR between female and male athletes was highest for amateur athletes compared with intermediate and elite athletes (IRR=2.1; 95% CI 1.3 to 3.4; P<0.01; I²=82%). Amateur female athletes remained at higher risk of ACL injury than did with amateur male athletes. In studies where follow-up length was <1 year, female athletes had a higher IR of ACL injury than did to males (IRR=1.7; 95% CI 1.3 to 2.2; P<0.01). Where follow-up was 1 year and beyond, there was no sex difference in the IR of ACL injury (IRR=2.1; 95% CI 0.9 to 4.8; P=0.06; I²=65%).
Summary/conclusions One in 29 female athletes and 1 in 50 male athletes ruptured their ACL in a window that spanned from 1season to 25 years. The IR of ACL injury among female athletes in a season was 1.7 times higher than the IR of ACL injury among male athletes and the IP of ACL injury among female athletes was 1.5 times higher than the IP of ACL injury among male athletes. The reported sex disparity in ACL injury rates is independent of participation level and length of follow-up.
- ACL
- knee
- athlete
- epidemiology
Statistics from Altmetric.com
Studies that control for athletic exposure and population size suggest that female athletes may be at greater risk than male athletes for ACL injury.1 2 These findings have underscored the substantial research focus on injury mechanisms and injury prevention approaches for female athletes.3–7 ACL injuries present a significant healthcare burden. In addition to the financial burden, ACL injury can have significant personal costs and may result in the loss of a sport season, the loss of sport scholarships, reduced academic performance, long-term disability and increased risk of developing knee osteoarthritis.8 9
Estimates for the increased risk of injury in females relative to males exist for certain sex-comparable sports.1 2 This information is useful for those sports; however, the same information is not available for all sports. To compare the rates of injury in male and female athletes in a research study, the conditions for data collection must be identical. If the data collection methods of two studies investigating sex-comparable sports differ, it is not possible to compare the risk of injury. Therefore, meta-analysis may be a useful tool for estimating ACL injury rates. While previous meta-analyses comparing the rates on ACL injury incidence in male and female athletes have been conducted, they were either specific to one participation level (eg, high school only) or did not include all sports for which information was available.10 11 Therefore, the purpose of this systematic review was to estimate and compare the incidence proportions and incidence rates of ACL injury in male and female athletes.
Method
A systematic review was conducted using the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines. We searched the PubMed and EBSCO host (CINAHL, SPORTDiscus) electronic databases from database inception to 20 January 2017. The following phrase was used in the search: anterior cruciate ligament AND (injury OR tear OR rupture) AND (incidence OR prevalence OR epidemiology). We limited the search to peer-reviewed articles published in English language. Experts in the field were contacted for further study suggestions, and references from review papers were examined to identify any further relevant articles for potential inclusion. Publication details from all studies identified in the literature search were exported to bibliographic software (EndNote V.X7, Thomson Reuters, USA).
Selection criteria
One assessor screened articles for inclusion. Any grey areas of inclusion were brought to discussion with a second assessor and any disagreements were arbitrated by a third assessor. Articles were screened first by title, then by abstract and finally by full text according to the inclusion and exclusion criteria (box 1). We defined organised sport as a school-based, organised recreational or professional sport. Full texts were retrieved when the title or abstract met the selection criteria, or when the status (include or exclude) could not be determined from the title and/or abstract alone.
Inclusion and exclusion criteria
Inclusion criteria
Research conducted in athletes playing organised sports
Total number of ACL injuries and total number of individuals in the population by sex reported
Reported data such that the number of ACL injuries by sex could be calculated
Exclusion criteria
Further analyses on previously reported prospective studies
Studies published in languages other than English
Review articles
Data extraction and management
The primary variables extracted were the number of ACL injuries, the person-time for each sex, type of exposure, length of follow-up (<1 year, 1 year or >1 year), participation level (amateur, intermediate and elite). Participation level was defined as follows: amateur included recreational, high school and intramural athletes; intermediate included collegiate and semi-professional athletes and elite included elite and professional athletes. One author extracted data from all included articles (AMM) and another author independently reviewed these data for accuracy and completeness (DKS). Studies used for incidence proportion and incidence rate analyses are listed in online supplementary file 1.
Supplemental material
The reported person-time unit was not uniform across studies. To establish a common metric, we calculated athlete-exposures (AE). When the number of player-hours were reported, AEs were estimated by multiplying the number of player-hours by 2. This was to estimate the average length of training sessions and games with warm-ups included.12–30 Player-days were treated as AEs as athletes typically participate in one practice or game per day. This unit was only used in studies that investigated high school and college athletes.12 For studies that reported incidence rate by sex, the number of AEs and the reported incidence rates were used to calculate the number of ACL injuries by sex (number ACL injuries by sex=total AE by sex×rate numerator by sex/rate denominator by sex).15 31 32
Whenever possible, the incidence proportion and incidence rate were calculated. The incidence proportion was calculated by dividing the number of new ACL injuries by the total number of participants over the given time period specified in each study. The denominator for incidence proportion ranged from 1 season to 25 years. The incidence rate was calculated by dividing the total number of new ACL injuries by the total number of exposures. We emailed the authors of studies where the number of ACL injuries by sex could not be estimated. If the study authors did not have access to the information or did not respond to our email, the study was excluded from the meta-analysis.33–40
Risk of bias assessment
Risk of bias was assessed by two authors independently (AMM, DKS) using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.41 This tool dichotomously assesses criteria including participation rate, whether exposure data were collected prospectively, whether the timeframe was sufficient to allow for the outcome to occur, number of participants lost to follow-up after baseline, etc. If the criterion was present, the item was given a ‘Y’. If the criterion was absent or was not reported, the item was given an ‘N’. Any discrepancies in assessment were discussed. For discrepancies that could not be resolved, a third author was consulted for arbitration (GDM). Studies where interventions were administered were treated as cohort studies in our analyses, and assessed using the same tool.
Statistical analysis
Injury data were analysed using R (V.3.3.2, the R Foundation for Statistical Computing). We used the packages meta and metafor with the functions metarate for incidence rate, metaprop for incidence proportion single ratio, metainc for incidence rate ratio (IRR) and metabin for incidence proportion binary data ratio (weighted for individual study size). For calculating incidence proportion and incidence rate for the total population, female athletes only and male athletes only, all studies that presented data were included in the respective analyses. When calculating the relative risks (RRs) and IRRs only studies that presented both females and males in the same study were used. For example, studies that included only females were used to calculate female incidence proportion and incidence rate, but were not used to calculate RR or IRR.
Injury risk proportions for individual studies and pooled estimates were summarised in forest plots for the following subgroups: female, male, combined. A pooled estimate for the RR of ACL injury in females versus males was calculated and summarised a forest plot. Raw injury incidence rates for individual studies and pooled estimates were summarised in forest plots for the following groups and subgroups: female, male, combined. Pooled IRRs for females versus males were calculated and summarised in forest plots. Heterogeneity was assessed using the I2 statistic,42 which estimates the variation resulting from heterogeneity and not chance.42 I2 values over 75% were considered high.42 Publication bias was assessed using funnel plots with SE as the measure of the study size on the y-axis and the ratio on the x-axis. A P value of ≤0.05 was considered to be significant for all statistical analyses.
Sensitivity analyses
To account for heterogeneity among studies, we used sensitivity analysis to assess the effect of each individual study on the overall rate of ACL injury. This was done by removing one study, performing the analysis, investigating the effect of the removal on heterogeneity, adding the study back to the analysis and repeating the procedure. This was repeated for each individual analysis included.
To account for bias, we attempted to perform separate analyses on studies that met the criteria for item 11 (reliability and validity of measurement of the dependent variable) and item 14 (statistical adjustment for potential confounding variables). However, there were too few studies that met the criteria. Therefore, we included all studies in the final analysis (regardless of heterogeneity) because we expected that combining sports with varying risks of ACL injury would result in high heterogeneity. Sources of heterogeneity will be further explored in future analyses of the same data set.43 44
Subgroup analyses
To account for variations in length of follow-up, we compared incidence rates from studies with follow-up lengths of up to 1 year and >1 year. To account for differences in participation levels, we compared incidence rates from amateur, intermediate and elite athletes.
Results
The final search yield was 3774 abstracts. After removal of duplicates, there were 1300 records for screening. After title and abstract screening, 1155 articles were excluded. The remaining 145 articles were manually cross-referenced and experts were consulted to identify additional relevant articles, resulting in inclusion of 17 additional articles. We screened the full texts of 162 articles, and 58 studies were included (figure 1).12–32 45–81

Flow chart summary of the article screening process.
Risk of bias assessment
Studies that fulfilled fewer than 50% of criteria were deemed to be of low quality. Three studies fulfilled 75% or more of the criteria and 44 studies fulfilled 50% or more the criteria (see online supplementary file 2). Fourteen studies fulfilled fewer than 50% of the criteria and were deemed to be of low quality. Studies may have received low or moderate assessment for lack of reporting information. The potentially unreported criteria include total number of eligible individuals, how outcomes were measured and attrition.
Supplemental material
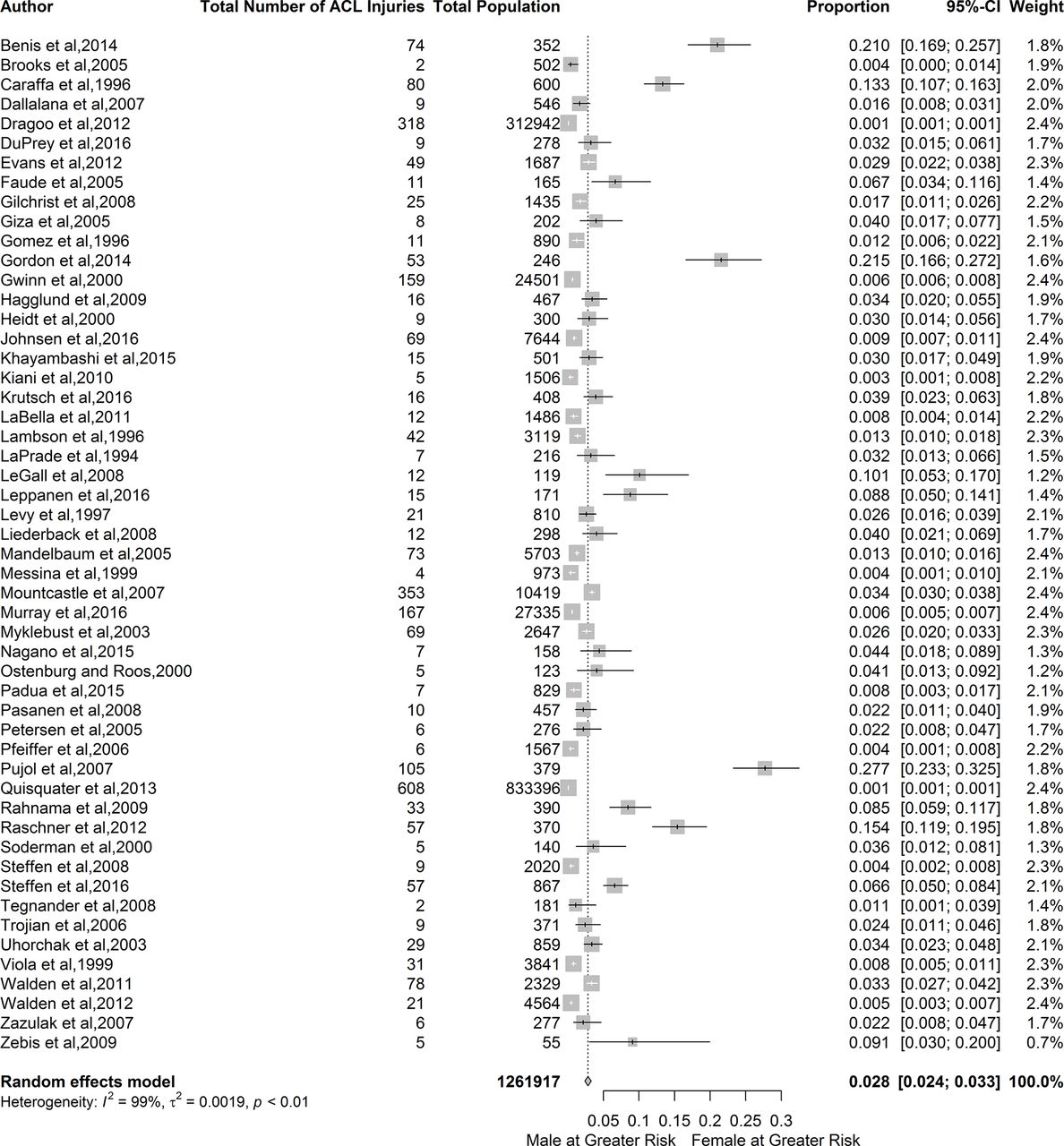
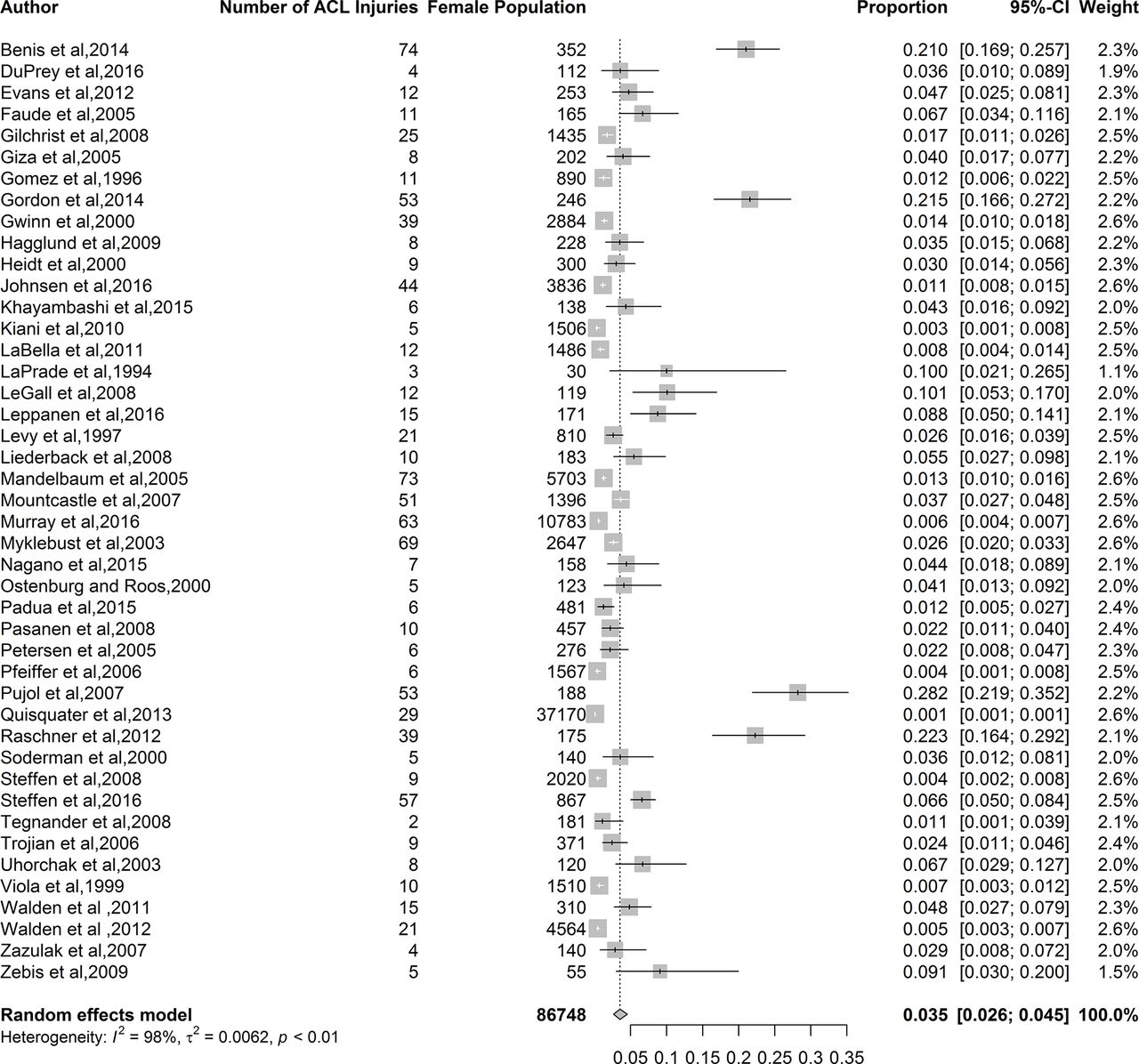
The pooled ACL injury incidence proportion for all athletes was 2.8% (95% CI 2.4% to 3.3%; I²=99%) figure 2), which equates to 1 ACL injury in every 36 athletes. The pooled ACL injury incidence proportion for female athletes was 3.5% (95% CI 2.6% to 4.5%; I²=98.0%; figure 3), which translates to 1 ACL injury in every 29 female athletes. The pooled ACL injury incidence proportion for male athletes was 2.0% (95% CI 1.6% to 2.5%; I²=99%; figure 4), which translates to 1 ACL injury in every 50 male athletes. The RR for ACL injury was 1.5 times higher in female athletes compared with male athletes (RR=1.5; 95% CI 1.2 to 1.9; P<0.01; I²=61%, figure 5). A list of included sports for each sex and the studies used for each analysis are located in online supplementary file 1.

Forest plot for the incidence proportion and 95% CI of ACL injury in male and female athletes.
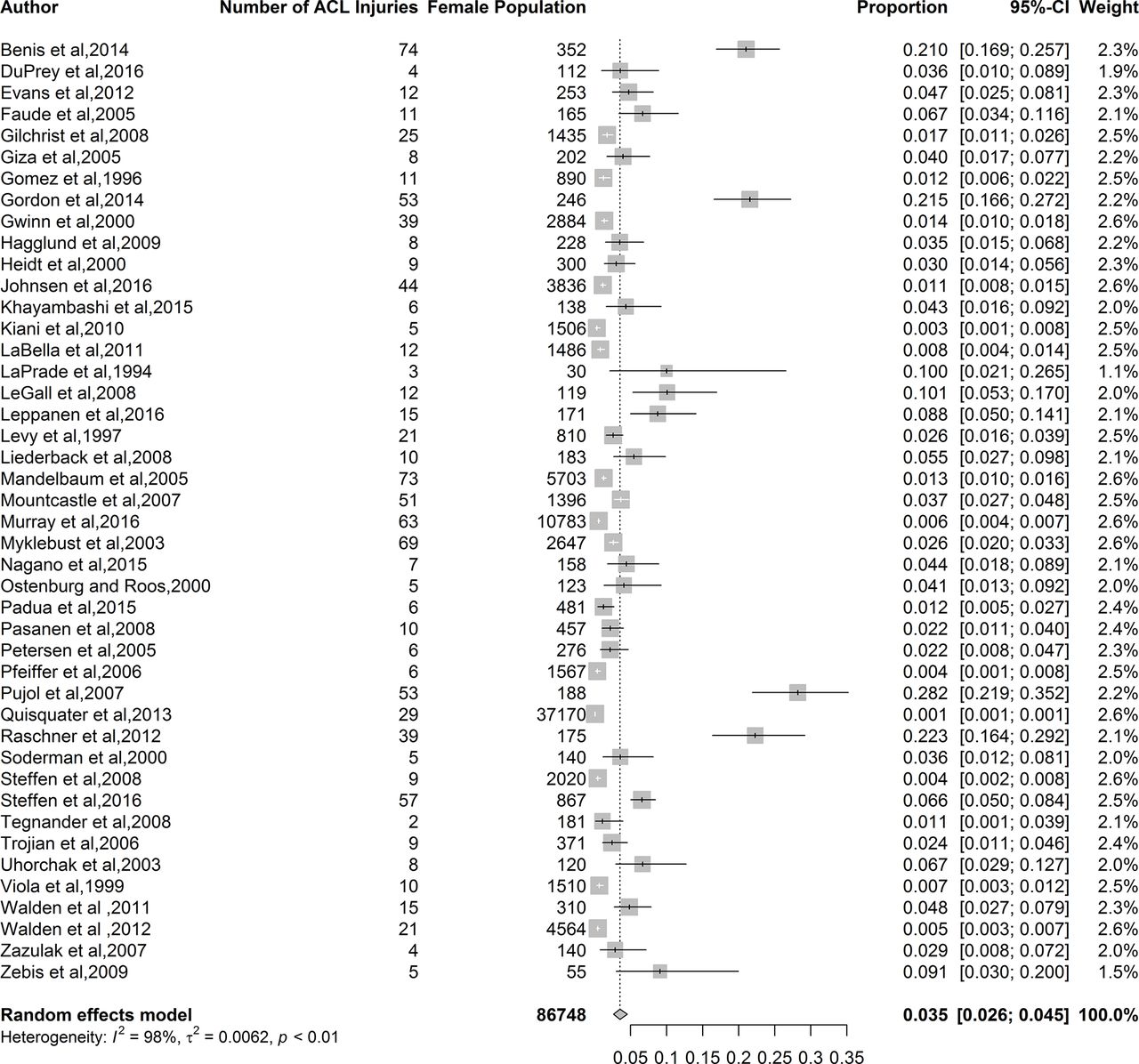
Forest plot for incidence proportion and 95% CI of ACL injury for female athletes.

Forest plot for incidence proportion and 95% CI of ACL injury for male athletes.
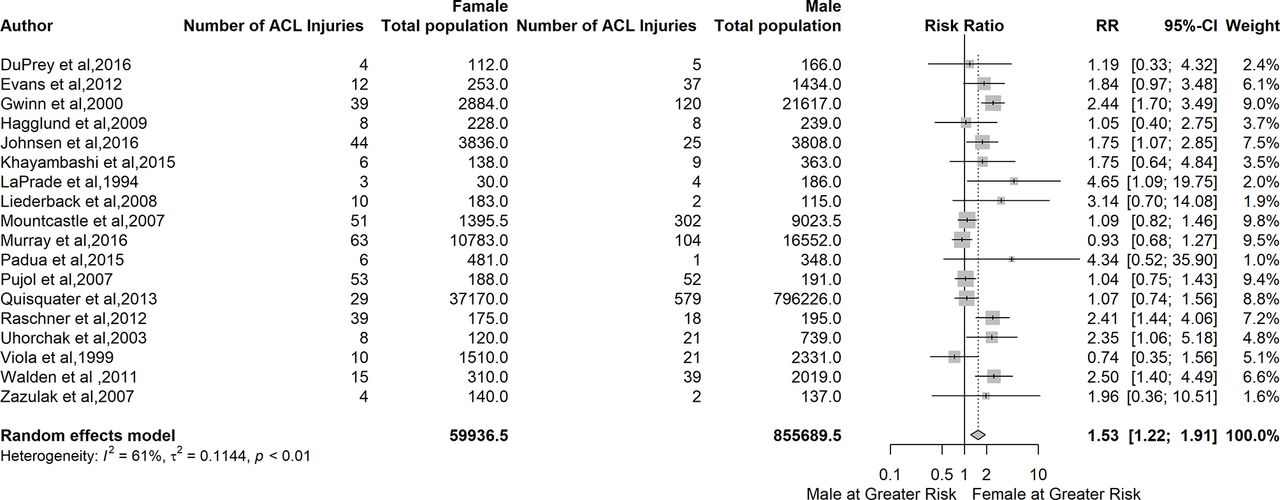
Forest plot for relative risk (RR) and 95% CI of ACL injury in athletes—female vs male. <1=reduced RR in females; >1=reduced RR in males.
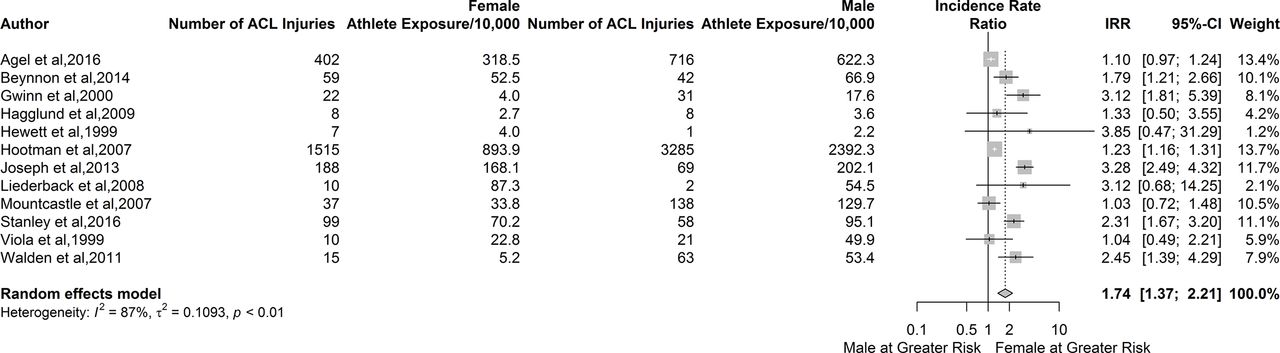
ACL injury incidence among all athletes was 1.5 per 10 000 AEs (95% CI 1.2 to 2.0; I²=99%; figure 6). Female injury incidence was 1.9 ACL injuries per 10 000 AEs (95% CI 1.6 to 2.4; I²=94%; figure 7) and male injury incidence was 0.9 ACL injuries per 10 000 AEs (95% CI 0.7 to 1.1; I²=94%; figure 8). Females athletes had a 1.7-fold increase in incidence rate of ACL injury relative to male athletes (95% CI 1.4 to 2.2; P<0.010; I²=87%; figure 9).

Forest plot for total incidence rate and 95% CI of ACL injury in athletes for males and females combined.

Forest plot for incidence rate and 95% CI of ACL injury for female athletes.
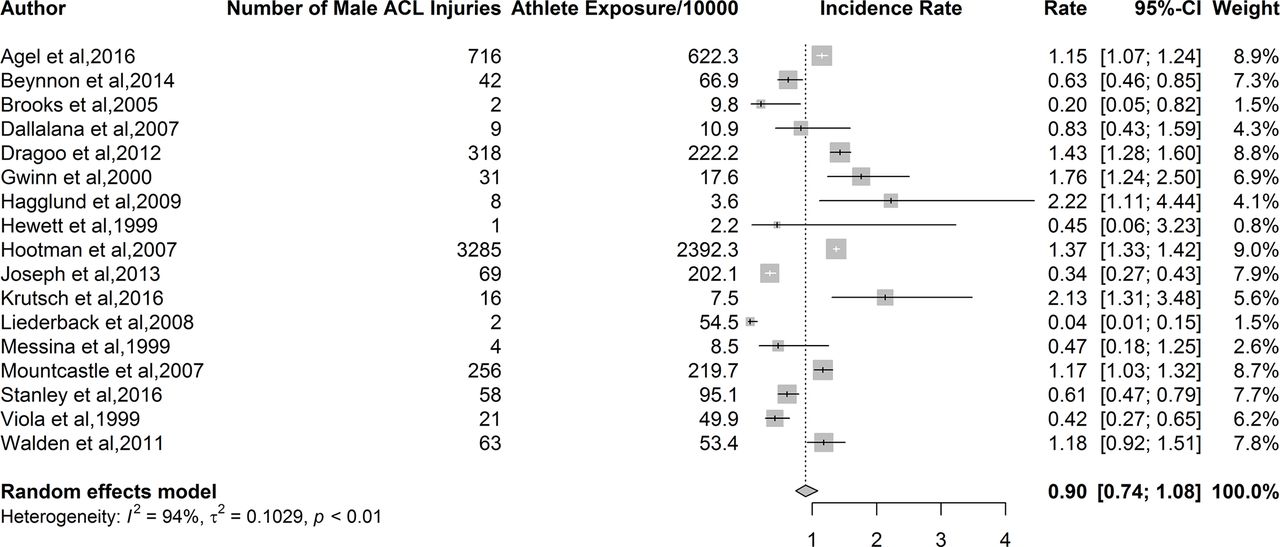
Forest plot for incidence rate and 95% CI of ACL injury for male athletes.

Forest plot for incidence rate and 95% CI of ACL injury for in athletes—female vs male. <1=reduced relative risk in females; >1=reduced relative risk in males.
The IRR) for amateur athletes was 2.1 (95% CI 1.3 to 3.4; P<0.01; I²=82%; figure 10). The IRR was lower for elite athletes (IRR=1.7; 95% CI 1.1 to 2.8; P=0.25; I²=25%) and for intermediate athletes (IRR=1.3; 95% CI 0.9 to 1.7; P<0.01; I²=88%).

Forest plot for incidence rate and 95% CI of ACL injury in athletes—female vs male by participation level. <1=reduced relative risk in females; >1=reduced relative risk in males.
With regard to variations resulting from length of follow-up, the subanalyses indicated that there were differences between sexes with regard to ACL injury incidence rate. The IRR for a follow-up length of <1 year was 1.7 (95% CI 1.3 to 2.6; P<0.01; I²=89%; figure 11). The IRR for a follow-up length of 1 year or greater was 2.1 (95% CI 0.9 to 4.8; P=0.06; I²=65%). While female athletes were at great risk of ACL injury when follow-up was <1 year, this risk was not significant with longer follow-up length. Heterogeneity remained high for studies with a follow-up length of <1 year, but was acceptable in studies with a follow-up length of 1 year or greater.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for incidence rate and 95% CI of ACL injury for in athletes—female vs male by length of follow-up. <1=reduced relative risk in females; >1=reduced relative risk in males.
Sensitivity analyses
Excluding single studies from each analysis did not alter the statistical heterogeneity (I2 statistic). Heterogeneity remained high (> 75 %) throughout the procedure. Excluding studies that did not fulfil item 11 in the risk of bias assessment did not statistically alter the pooled estimates for ACL injury incidence, and heterogeneity remained high. Excluding studies that did not fulfil item 14 in the risk of bias assessment did not statistically alter the pooled estimates for total ACL incidence rate and female ACL injury incidence rate. There were insufficient studies to conduct sensitivity analyses (excluding studies that did not fulfil item 14) for the other ACL injury outcomes.
Publication bias
The funnel plot for RR indicated that almost all studies used for the analysis fell within the expected parameters, most with low SE indicating that most studies were large (see online supplementary file 3). A majority of studies showed females tend to have greater incidence proportion, but to varying degrees. The funnel plot for IRR indicated that most studies fell within the expected parameters (see online supplementary file 4). SE was relatively low, indicating that studies were large, and a majority of studies showed that females were at increased risk relative to males. The studies are not evenly distributed in the funnel, with studies missing from the lower left quadrant. Studies in the lower left quadrant would represent smaller studies that show a greater incidence proportion or incidence rate of ACL injuries in males relative to females. It is possible this quadrant is lacking studies due to publication bias. Therefore, we deemed that the publication bias was low.
Supplemental material
Supplemental material
Discussion
The incidence proportion and incidence rate of ACL injury in female athletes were 3.5% and 1.5/10 000 AEs, respectively. The incidence proportion and incidence rate of ACL injury in male athletes were 2.0% and 0.9/10 000 AEs, respectively. Overall, female athletes had 1.5 times the incidence proportion and a 1.7-fold increase in the incidence rate of ACL injury compared with males. When controlling for follow-up length (<1 year, or approximately one season), females maintained about the same increased incidence of ACL injury. Female athletes had a higher incidence of ACL injury in a season (independent of participation level), compared with male athletes. There was no difference in injury incidence after 1 year between male and female athletes.
We attempted to answer the following research questions: (1) What are the incidence proportions and incidence rates of ACL injuries for all athletes, female athletes and male athletes? and (2) Are there sex differences in RR and IRR of ACL injuries? When pooling data to answer our review questions, there was a trade-off between including more studies, and producing spurious estimates when pooling statistically and clinically heterogeneous data. We did not exclude studies based on either risk of bias or level of evidence, and we judged the risk of bias in included studies as moderate because most included studies (44/58) met 50% or more of the criteria. Moreover, many criteria that were not met were not relevant to epidemiological study quality. However, the large number of included studies enhances the generalisability of our results. Based on the Centre for Evidence Based Medicine, these estimates would receive a Grade of Recommendation of C (level 4 evidence included).82
Our findings support previous research suggesting that female athletes have a 1.5 times increased risk for ACL injury compared with male athletes.10 One possible explanation for the disparity between sexes with regard to ACL injury risk may be differences in modifiable and non-modifiable risk factors. Female athletes may have greater quadriceps activation relative to hamstring activation (quadriceps dominance), greater reliance on stability from ligaments than muscles (ligament dominance), increased strength and coordination in one leg over the other (limb dominance) and altered neuromuscular control of the trunk (trunk dominance) compared with male athletes.3 6 83
There was a 1.7-fold increase in incidence of ACL injuries in females compared with males. One explanation for this might be the increasing number of females participating in sport, and female athletes spending more time participating in sport (ie, the exposure is greater).84 This is especially true in higher risk sports, such as soccer and rugby.85–87 Therefore, continued implementation of rigorous injury surveillance programmes may be important to monitor injury incidence among female athletes. Sports medicine clinicians should be aware of both the sex-specific increased risk of suffering ACL injury in order to prepare strategies that are optimised for sexes. Specifically, efforts to enhance coaches’ understanding of sex-specific risk factors for ACL injury indicate that training programmes are not one-size-fits-all and programmes need to be specifically adjusted to suit the deficits of female athletes (including specific injury prevention strategies). However, the focus on ACL injury prevention strategies should not be at the expense of male athletes—injury prevention and tailored training programmes are equally important for both sexes.
Methods issues
There are three issues related to systematic review methods that must be considered when reading and using the results of our systematic review.
Risk of bias assessment
Poor internal validity (bias within studies) may have contributed to statistical heterogeneity, and precision in effect estimates. Assessing the risk of bias in epidemiological studies can be challenging because the tools available cover methodological issues that do not necessarily contribute to bias in observational studies. For example, existing tools assess whether or not subjects were randomised. However, randomisation is not relevant when investigating whether or not a condition of interest is diagnosed in subjects. Items like this negatively impact risk of bias even though they are irrelevant to the study design or research question. Despite the limitations regarding the assessment of risk of bias, there was bias in included studies. Therefore, caution should be exercised in generalising rates and risks.
Sources of variability
The high I2 statistics in our analyses indicate that the variability in injury rates was due to heterogeneity rather than to chance. One explanation for the high I2 in incidence proportion estimates and ACL injury incidence rate is that we pooled data from studies of different types of sports, with differing risks for ACL injury. Our intention was to provide general estimates of ACL injury, not sport-specific estimates. Subsequent sport-specific analyses on the same dataset are forthcoming.44 We also intended to provide relative estimates of ACL injury in female compared with male athletes. However, conclusions regarding sex differences in ACL injury risk cannot be drawn about specific sports.
Exposure data varied among studies, and we estimated exposure in some studies. Conversion may also have resulted in an underestimate of the true exposure, which would cause an overestimation of the incidence rates. Differences in participation level and length of follow-up likely also contributed to statistical heterogeneity.
Sensitivity and subgroup analyses
We used sensitivity and subgroup analyses based on participation level and length of follow-up to explore potential sources of heterogeneity. However, statistical heterogeneity remained high in all sensitivity and subgroup analyses. We were unable to determine the main sources of statistical heterogeneity, and this reduces the robustness of the estimates in our systematic review.
Limitations
Incidence proportions and rates may have been overestimated in some instances by the inclusion of re-injuries; however, the inclusion of re-injuries is likely a small source of bias. Some studies only included non-contact mechanisms of injury. Therefore, the estimates provided here may be underestimates of the true rates, although it is difficult to be certain. Incidence rates were based on estimated AE for 18 of 38 studies included for rate analyses.
We employed broad inclusion criteria that captured a wide range of studies to enhance generalisability. This entailed including studies that investigated only males and only females, which is another limitation. The lack of homogeneity negatively affects the conclusions that may be drawn from the data.
With regard to the length of follow-up for the incidence proportion estimate, a large range of follow-up periods that made it difficult to standardise. Incidence proportions require a unit of time (eg, 1-year or 2-year incidence proportion). In this review, the length of follow-up in included studies ranged from one season to 25 years. However, there were very few studies with follow- up >1 year. We found that the sex-differences in incidence rate was maintained when follow-up was <1 year. The sex-difference in ACL injury incidence was not significant beyond 1 year.
We did not assess the influence of age on the injury estimates because many studies did not specify participant age or age range. Controlling for age would have substantially reduced the number of studies eligible for inclusion. While the search was systematic and comprehensive, we acknowledge the risk of publication and language bias associated with the current report.
Future research
Whenever possible, future research should investigate injury epidemiology in male and female athletes simultaneously to allow for sex comparisons in future meta-analysis. This is especially true for sports that are not frequently investigated, such as gymnastics and skiing, and for sports that are growing in popularity, such as rugby. This research should use the most specific exposure units possible, such as player-hours, and should detail exact length of follow-up in months or years. Because sport season lengths can vary by location, age and participation level, detailing follow-up length this way is particularly important for standardising the period of time over which exposures are occurring.
Future research should also investigate sport-specific differences in incidence rates between females and males. Making sport-specific distinctions will help to identify where the greatest disparities between sexes lie and which populations could benefit the most from preventive strategies such as neuromuscular training, which can reduce the rate of ACL injury and improve performance.88–91 Addressing aspects of injury prevention, risk factor assessment and athletic performance with a protocol targeted towards younger athletes at the highest risk of ACL injury has important implications for helping to support injury-free sport participation.92 93
Conclusion
Female athletes had 1.5 times greater risk of sustaining an ACL injury compared with male athletes. One in 29 female athletes sustained an ACL injury, and 1 in 50 male athletes sustained an ACL injury over 25 years. The reported sex disparity in ACL injury rates was independent of participation level and length of follow-up.
What is already known?
Total and sex-specific estimates of ACL injury incidence proportions and incidence rates have been reported in isolation, but the overall risk of ACL injury including all sports is relatively unknown.
What are the new findings?
One in 29 female athletes and 1 in 50 male athletes ruptured their ACL in a window that spanned between 1 season and 25 years.
The incidence rate of ACL injury among female athletes in a season was 1.7 times higher than the incidence of ACL injury among male athletes.
The incidence proportion of ACL injury among female athletes was 1.5 times higher than the incidence proportion of ACL injury among male athletes.
The sex differences in ACL injury rates were independent of participation level.
Acknowledgments
The authors would like to acknowledge funding support from the National Institutes of Health/NIAMS Grant U01AR067997.
References
Footnotes
Contributors AMM, DKS, KEW, BB, MSK, and GDM worked on concept, writing, and approving the final draft. LY worked on analysis, interpretation, writing, and approving the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data from this review are available from the journals in which they were published.
Collaborators Emir Veledar, PhD, Robert Stempel School of Public Health and Social Work, Florida International University, Miami, Florida, USA
Correction notice This article has been corrected since it was published Online First. The ’Contributors' section has been updated.