Article Text

Abstract
Objective To describe the incidence of injuries and illnesses sustained during the XXIII Olympic Winter Games, hosted by PyeongChang on 9–25 February 2018.
Methods We recorded the daily number of athlete injuries and illnesses (1) through the reporting of all National Olympic Committee (NOC) medical teams and (2) in the polyclinic and medical venues by the PyeongChang 2018 medical staff.
Results In total, 2914 athletes (1210 women, 42%; 1704 men, 58%) from 92 NOCs were observed for occurrence of injury and illness. NOC and PyeongChang 2018 medical staff reported 376 injuries and 279 illnesses, equalling 12.6 injuries and 9.4 illnesses per 100 athletes over the 17-day period. Altogether, 12% of the athletes incurred at least one injury and 9% at least one illness. The injury incidence was highest in ski halfpipe (28%), snowboard cross (26%), ski cross (25%), snowboard slopestyle (21%) and aerials (20%), and lowest in Nordic combined, biathlon, snowboard slalom, moguls and cross-country skiing (2%–6%). Of the 376 injuries recorded, 33% and 13% were estimated to lead to ≥1 day and >7 days of absence from sport, respectively. The highest incidences of illness were recorded in biathlon (15%), curling (14%), bobsleigh (14%) and snowboard slalom (13%). Thirty per cent of the illnesses were expected to result in time loss, and 70% affected the respiratory system. Women suffered 61% more illnesses than men.
Conclusion Overall, 12% of the athletes incurred at least one injury during the Games and 9% an illness, incidences that are similar to the Olympic Winter Games of 2010 and 2014.
- surveillance
- injury
- illness
- winter sports
- elite athletes
- prevention
Statistics from Altmetric.com
Introduction
It is well recognised that routine physical activity elicits a number of health benefits, including a reduction in the risk of numerous chronic diseases and premature death.1 2 Compared with the general population, elite athletes seem to gain additional health benefits in the form of greater life expectancy and lower risk of disease and hospital admission.3–7 However, concomitantly they run a higher risk of musculoskeletal disorders during and long-term disability after the end of their careers.4 8–11
Systematic injury and illness surveillance is a prerequisite to effective protection of the health of the athletes, by providing essential information on the extent and incidence of injuries and illnesses occurring in sports. These epidemiological data contribute to better planning and provision of athlete healthcare, and importantly objectively inform and help to advance the development of measures to prevent injury and illness. Guided by these data, future injury and illness risk factor and mechanism research can identify and influence factors linked to injury or illness risk, such as the safety precautions in sport rules and regulations, or the training programmes and equipment used by athletes.12 13
Several International Sports Federations and research institutes have set up injury and illness surveillance systems either longitudinally, over one or more seasons, or during certain main events.14–76 At the Beijing 2008 Olympic Games, the IOC commissioned the first major IOC injury surveillance system,77 78 which was subsequently expanded for Vancouver 2010 to also include illnesses.79 Since then, the surveillance system has been continued and further developed in London 2012,80 Sochi 201481 and Rio 2016.82 In these Games, the injury and illness incidences ranged from 9.6 to 14.0 injuries and from 5.4 to 8.9 illnesses per 100 athletes.
Our aim was to describe the incidence and characteristics of the sports injuries and illnesses occurring during the PyeongChang 2018 Olympic Winter Games.
Methods
We employed the IOC injury and illness surveillance system for multisport events in this prospective cohort study.77 We invited all National Olympic Committee (NOC) medical teams to report the daily occurrence (or non-occurrence) of athlete injuries and illnesses using an electronic report form (side module of General Electric Athlete Management Solution; GE AMS). Concurrently, we retrieved the same information on all athletes treated for injuries and illnesses in the polyclinic and all other medical venues operated by the Organizing Committee of the Olympic and Paralympic Games PyeongChang 2018 medical staff. These data were collected through an electronic medical record system (GE AMS).
Implementation
Three months in advance we informed the NOCs about the study by letter. The day before the opening of the Games, we organised a meeting for all NOC medical staff. At this meeting we informed them about the protocol, answered questions, created user accounts for the GE AMS injury and illness reporting system, and distributed tablet computers to facilitate their daily reporting.
Throughout the data collection, we actively followed up NOCs comprising 10 or more participating athletes with frequent visits to address any questions and encourage continuous reporting during the games. We recorded the response rate of all the 92 participating NOCs. At the end of the Games, NOC medical staff with a response rate of 100% could keep their tablet computer.
Definition of injury and illness
We defined injuries and illnesses as new (pre-existing, not fully rehabilitated conditions were not recorded) or recurring (athletes having returned to full participation after a previous condition) incurred in competition or training during the PyeongChang Olympic Games (9–25 February 2018) receiving medical attention, regardless of the consequences with respect to absence from competition or training.77 Injuries included musculoskeletal complaints, concussions and other non-musculoskeletal trauma. In cases where a single incident caused multiple injury types, we recorded only the most severe diagnosis—as determined by our research team based on all available clinical data—for analysis. Severe injuries and illnesses were defined as injuries or illnesses estimated to lead to absence from training or competition of more than 1 week.
Injury and illness report form
Our injury and illness report form followed the template of that used in the Vancouver 2010, London 2012, Sochi 2014 and Rio 2016 Olympic Games.79–82 With respect to injuries, we recorded the following data: accreditation number, name, sport and event, whether the injury occurred in competition or training, date and time, body part, type, cause, and estimated time lost from competition or training. We recorded data on illnesses in a similar fashion: accreditation number, sport and event, date, affected system, main symptom(s), cause, and estimated time loss.
We provided instructions and examples on how to complete the form correctly. Furthermore, the report form was available in nine languages: English, French, Arabic, Chinese, German, Japanese, Korean, Russian and Spanish.
Confidentiality
In addition to the aforementioned variables, we queried the IOC athlete database for the age, sex, and nationality of the injured or ill athlete. We treated all information confidentially, and de-identified our database after the Games, ensuring anonymity of all athletes.
Patient and public involvement
Patients were not involved in planning the research priorities, research questions, outcome measures, study design or conduct. We will invite patients and the public to help with dissemination and evaluation of the study and the results.
Data analysis
In cases where athletes were treated for the same condition by both the NOC and PyeongChang 2018 medical staff, we retained the most complete data source.
We calculated the summary measures of injury and illness incidences (i) according to the formula i=n/e, where n is the number of injuries or illnesses in competition, training or in total during the study period, and e the respective number of exposed (participating) athletes, with incidence proportions presented as injuries/illnesses per 100 athletes. We also calculated the summary measures of injury and illnesses per 1000 athlete-days, where athlete-days correspond to the total number of athletes multiplied by 17 days. We calculated confidence intervals (CI) of the risk ratio (RR) of the number of injuries or illnesses between the two groups by a Poisson model, assuming constant hazard per group and adjusting for sport, sex and/or NOC size (by the number of athletes) where appropriate. We present injury and illness incidences as means and RRs with 95% CIs. We regarded two-tailed p values <0.05 as significant.
Results
In total, 2914 athletes took part in the PyeongChang Olympic Games. Of these, 1210 were women (42%) and 1704 men (58%). There were 67 double-starters, meaning athletes who participated in two different sports or disciplines, giving a total of 2981 athlete exposures to injury or illness.
Throughout the 17 days of the Games, NOCs submitted 1242 of a maximum of 1564 daily reports (79%; 15 countries did not submit any data) (table 1). The response rate of the 36 NOCs with ≥10 participating athletes (accounting for 95% of all the athletes) was 98% (598 of 612 reports).
Response rates, injuries and illnesses in NOCs of different sizes (measured by number of athletes)
Injuries overall, by sport and sex
We recorded a total of 376 injuries, equalling 12.6 injuries (95% CI 11.3 to 13.9) per 100 exposed athletes. This corresponds to 7.4 injuries per 1000 athlete-days. On average, 12% (n=351) of the athletes sustained at least one injury. In addition, there were 25 athletes with two injuries each.
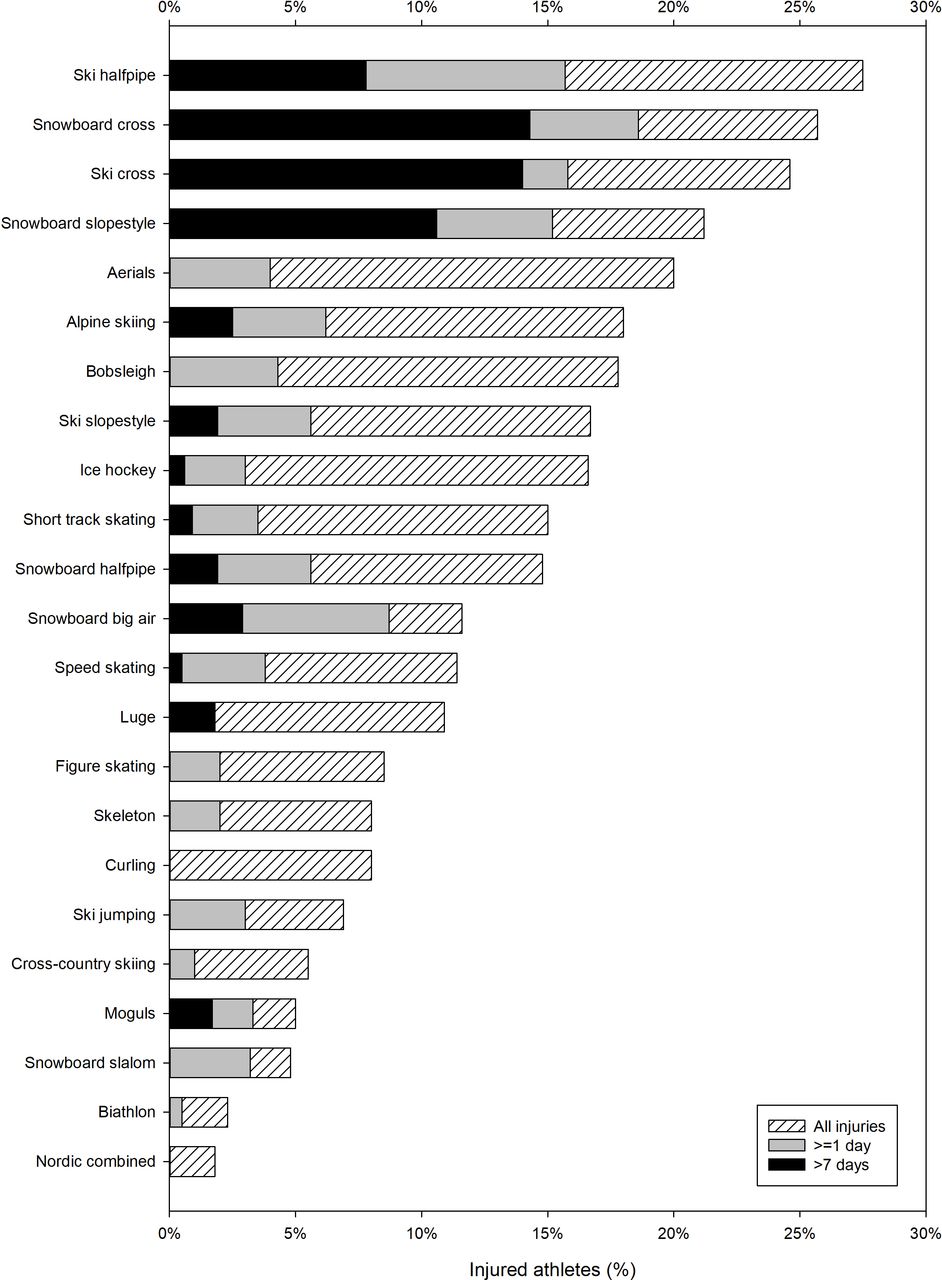
Figure 1 shows the incidence proportion of injured athletes in each sport (additional details are available in online supplementary appendix 1). The incidence of injury was highest in ski halfpipe (27.5 injuries (95% CI 13.1 to 41.8) per 100 athletes), snowboard cross (25.7 (95% CI 13.8 to 37.6)), ski cross (24.6 (95% CI 11.7 to 37.4)), snowboard slopestyle (21.2 (95% CI 10.1 to 32.3)) and aerials (20.0 (95% CI 7.6 to 32.4)), and lowest in Nordic combined, biathlon, snowboard slalom, moguls and cross-country skiing (ranging from 2 to 6 injuries per 100 athletes).
Supplemental material

Proportions of athletes (%) in each sport with injury, injury with estimated time loss ≥1 day and injury with estimated time loss >7 days.
When adjusting for sport and NOC size, there was no difference in overall injury incidence between women (13.7 injuries (95% CI 11.6 to 15.7) per 100 athletes) and men (11.9 (95% CI 10.3 to 13.5), RR=1.15 (95% CI 0.94 to 1.41); online supplementary appendix 2). However, female athletes were at significantly higher risk of injury in luge (RR=5.33 (95% CI 1.61 to 17.71)) and ice hockey (RR=1.68 (95% CI 1.09 to 2.59)), while at lower risk in curling (RR=0.13 (95% CI 0.02 to 0.99)) and speed skating (RR=0.29 (95% CI 0.10 to 0.87)).
Supplemental material
Severity of injuries
While two-thirds of the injuries were estimated to result in no time loss from sport (n=252, 67%), 33% of the injuries (n=124) were expected to prevent the athlete from participating in competition or training (online supplementary appendix 1). It was estimated that 15% of the injuries (n=56) would result in an absence from sports from 1 to 3 days, 5% (n=19) in an absence from 4 to 7 days, 6% (n=21) in an absence from 8 to 28 days, and 7% (n=28) in an absence for more than 28 days. Figure 1 shows the incidence of injuries estimated to lead to ≥1 day and >7 days of absence in each sport, with snowboard and ski cross presenting the most injuries in both severity categories. Box 1 presents the details of the 49 injuries classified as ‘severe’.
Information on the 49 severe injuries (estimated absence >7 days), with the sports with the highest numbers in brackets
17 fractures (4 in ski cross, 4 in snowboard cross, 2 in snowboard slopestyle, 2 in luge).
12 ligament ruptures/sprains (5 in alpine skiing, 4 in snowboard cross).
5 dislocations or subluxations (3 in snowboard slopestyle).
5 concussions (2 in ice hockey, 1 in ski halfpipe, 1 in ski cross, 1 in snowboard slopestyle).
3 bone contusions (1 in ski cross, 1 in snowboard big air, 1 in snowboard cross).
2 lesions of meniscus or cartilage (1 in alpine skiing, 1 in snowboard slopestyle).
2 tendon strains/ruptures (1 in speed skating, 1 in ski halfpipe).
1 spinal cord injury (ski cross).
1 impingement (ski halfpipe).
1 muscle contusions or haematoma (snowboard halfpipe).
Location and type of injuries
The most commonly injured locations were the knee (n=53), ankle (n=34), hand/fingers (n=29) and lower back (n=27). The most common injury types were sprain/ligament rupture (n=62), bone contusion (n=57) and muscle contusion/haematoma (n=50). The distributions of injury locations and injury types per sport are presented in online supplementary appendix 3 and 4, respectively.
Causes, mechanisms and onset of injury
While 89% (n=333) of the injuries were reported to occur acutely, 10% (n=39) and 1% (n=2) were reported to be recurrent or chronic, respectively (information missing for two injuries). However, overuse was reported as the cause of 16% of injuries. The most commonly reported injury mechanisms were contact with a stagnant object (31%) and non-contact acute injury. These mechanisms were particularly common in the sports presenting with the highest injury rates, such as ski halfpipe, snowboard slopestyle, and ski and snowboard cross (online supplementary appendix 5).
Supplemental material
The time of injury onset showed that 46% of the injuries were sustained in competition and 48% during training (information missing for 22 injuries; online supplementary appendix 1). The frequency of severe injuries (those estimated to result in greater than 7 days of absence) was greater in competition than in training (RR=2.50 (95% CI 1.35 to 4.65)).
Injuries in training and competition differed significantly in characteristics (location, type, mechanism and subsequent time loss from sport) and in terms of incidence in different sports. Competition injuries were less common than training injuries in speed skating (RR=0.20 (95% CI 0.06 to 0.69)), bobsleigh (RR=0.26 (95% CI 0.11 to 0.64)), snowboard slalom (3 injuries in training vs 0 in competition) and biathlon (4 vs 0 injuries). Ice hockey was the only sport in which there were significantly more competition injuries compared with training injuries (RR=3.11 (95% CI 1.83 to 5.29)).
Illnesses overall, by sex, sport and severity
Among the 2981 exposed athletes, a total of 279 illnesses were reported, resulting in 9.4 illnesses (95% CI 8.3 to 10.5) per 100 athletes. This corresponds to 5.5 illnesses per 1000 athlete-days. On average, 9% (n=259) of the athletes incurred an illness, as there were 20 athletes with two illnesses each. When controlling for sport and NOC size, women (11.8 illnesses (95% CI 9.9 to 13.7) per 100 athletes) were at significantly greater risk of experiencing an illness than men (7.6 (95% CI 6.3 to 8.9), RR=1.61 (95% CI to 1.26 to 2.04); online supplementary appendix 6).
Supplemental material
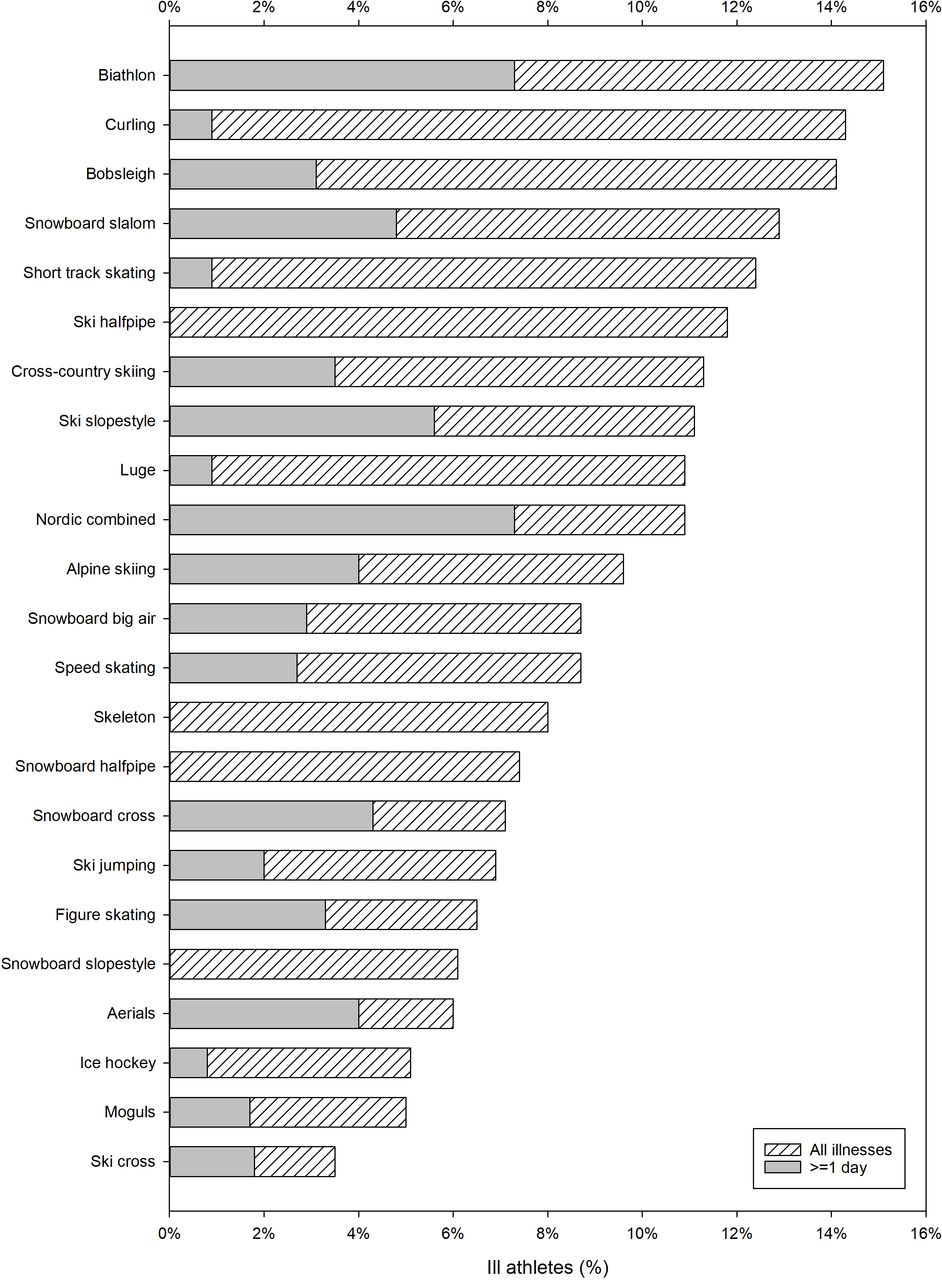
Figure 2 shows the incidence proportion of illness in each sport (additional details are available in online supplementary appendix 1). Biathlon was the sport with the highest illness incidence (15.1 illnesses (95% CI 9.9 to 20.2) per 100 athletes), followed by curling (14.3 (95% CI 7.3 to 21.3)), bobsleigh (14.1 (95% CI 8.3 to 19.9)) and snowboard slalom (12.9 (95% CI 4.0 to 21.8)). The lowest incidences of illness were seen in ski cross, moguls and ice hockey (ranging from 3 to 5 illnesses per 100 athletes).
{kind=link}
{kind=link}
Proportions of athletes (%) in each sport with illness and illness with estimated time loss ≥1 day.
One in three illnesses (n=83, 30%) were expected to result in absence from training or competition.
Affected system, main symptoms and causes of illness
A total of 194 illnesses (70%) affected the respiratory system. The second, third and fourth most frequently affected systems were the digestive system (n=36, 13%), skin and subcutaneous tissue (n=15, 5%) and the nervous system (n=11, 4%), respectively. Infection was the most common cause of illness (n=176, 63% of the illnesses). Of the 194 respiratory illnesses, 144 (74%) were caused by an infection. The distributions of affected systems, main symptoms and causes of illness per sport are presented in online supplementary appendices 7–9, respectively.
Data sources, and injuries and illnesses per NOC size
Only 27% of all injuries and 6% of all illnesses were captured by both the NOCs and the PyeongChang 2018 staff. While 49% of the injuries and 69% of the illnesses were recorded solely by the NOCs, 24% and 25% of the injuries and illnesses, respectively, were recorded solely by the PyeongChang 2018 staff.
The majority of injured and ill athletes from the larger NOCs were seen internally by their own NOC medical staff, but by contrast athletes from smaller NOCs were to a greater extent relying on diagnosis and treatment from the PyeongChang 2018 medical staff (table 1).
When adjusting for sport and sex, there was also an inverse relationship between NOC size (measured in number of participating athletes) and the incidence of illness, with athletes from smaller NOCs suffering more illnesses (NOCs with <10 athletes: 16.4 (95% CI 10.1 to 22.6) illnesses per 100 athletes vs NOCs with >99 athletes: 8.8 (95% CI 7.4 to 10.1) illnesses per 100 athletes (RR=1.85 (95% CI 1.19 to 2.86)).
Discussion
Injuries in the Olympic sports
The aim of the present paper was to describe and analyse the athlete injuries and illnesses which occurred during the PyeongChang 2018 Olympic Games. The incidence of injury in the PyeongChang Games (12%) was slightly higher than those in Beijing 2008 (10%),78 Vancouver 2010 (11%),79 London 2012 (11%)80 and Rio 2016 (8%),82 and identical to that of Sochi 2014 (12%).81 It was also lower than the injury incidences reported from the recent Paralympic Games.25 27–29 31 33
When comparing each sport in PyeongChang 2018 with Vancouver 2010, higher injury incidences were found in luge (11% vs 2% of the athletes injured) and speed skating (11% vs 3%). When doing a similar comparison with Sochi 2014, the injury incidences in PyeongChang were higher in ice hockey (17% vs 11%) and speed skating (11% vs 5%), but lower in biathlon (2% vs 7%), aerials (20% vs 49%) and moguls (5% vs 25%).
In general, our findings on the sports-specific injury rates in PyeongChang are corroborated by a large body of research from the Fédération Internationale de Ski (FIS) World Cup, where snowboard cross and halfpipe,44 52 aerial and halfpipe skiing and ski cross,46 54 as well as particularly downhill of the alpine skiing events,45 51 have been identified as disciplines with higher rates of injury.
A change in injury incidence can be a consequence of changes in the composition of the Olympic Games programme, environmental factors, venue or track design, competition rules, or changes in equipment. In addition, in PyeongChang 2018, a new electronic medical record was used for the first time by both the NOC and organising committee medical staff, which could potentially influence the sensitivity of the data collection. Also, incidence differences (lower or higher) may simply be the result of a natural variability of athletes’ exposure to risk, an observation that emphasises the value of ongoing surveillance to monitor trends over time, for example, the effect of venue design, rule or equipment changes in the period between major sports events.
Severity of injuries
In major sports events, like the Olympic Games, injuries or illnesses of even minor severity with or without time loss have the potential to be both participation-limiting and performance-inhibiting, and thus prevent athletes from possibly fulfilling their potential and reaching their lifetime achievement. In the PyeongChang Games, 33% of the injuries were estimated to result in time loss from competition or training of at least 1 day. This places PyeongChang 2018 between Sochi 2014 and Vancouver 2010, in which the equivalent numbers were 39% and 23%, respectively. In contrast, athletes in PyeongChang incurred fewer injuries of higher severity (13% of the injuries estimated to result in an absence greater than 7 days) compared with athletes in Sochi 2014 and Vancouver 2010 (16% and 17%, respectively).
Causes, mechanisms and onset of injury
The causes, mechanisms and circumstances of injuries in competition and training differed significantly between the different sports. The vast majority of injuries in PyeongChang were reported to be acute, whereas overuse injuries accounted for just a tenth of the injuries. Although similar distributions were reported from both the summer and winter Olympic Games previously, these numbers should be interpreted with caution due to the limitations in the recording of overuse injuries in the current methodology.83–87
In ski halfpipe, snowboard slopestyle, and ski and snowboard cross, the most commonly reported injury mechanisms were contact with a stagnant object and non-contact acute injury. These aetiological data seem to confirm findings from previous studies showing that a preponderance of the injuries in these sports occur from falls and crashes related to jumps, kickers and the halfpipe, in other words in features that facilitate aerial manoeuvres.50 53 88 89
With a fairly even distribution of injuries between training and competition (48% vs 46%, respectively), the findings are similar to those from Vancouver 2010 (54% vs 46%), but differ from Sochi 2014 (63% vs 35%). As in Sochi 2014, ice hockey was the only sport in PyeongChang 2018 in which injuries occurred more commonly in competition than in training. These results correspond with earlier epidemiological findings.90–94 Ice hockey is a team and contact sport where the intensity, speed of play, number of body checks and fatigue are considerably higher in games—where more is at stake—than in training, where a significant amount of time is used for recovery and training drills of lower intensity.
Illness risk during the Olympics
The rate of illness in PyeongChang 2018 was similar to those reported in the Vancouver Games and Sochi Games (9% of all athletes affected in PyeongChang vs 8% Sochi and 7% in Vancouver).79 81 Also consistent with the Vancouver and Sochi data is the difference in the illness incidence between female and male athletes, with women in PyeongChang experiencing 61% more illnesses than men. The same disproportion has previously been reported in the Rio 2016 Paralympic Games,34 the 2009 athletics35 and aquatics41 world championships, but not in the 2011 athletics36 or 2013 aquatics42 world championships, the 1994–2009 US open tennis championships,95 or the London 2012 and Sochi 2014 Paralympic Games.30 32
The high incidence of respiratory infections mirrors data from other elite sport events.28 30 32 34–36 41 59 95–100 While the primary causes are viruses such as the rhinovirus and parainfluenza virus,101 102 high-intensity and prolonged training and competition load is associated with an increased risk of both subclinical immunological changes (that may increase the risk of illness), and actual symptoms of illness or diagnosed illness.103–105 It is also known that frequent and prolonged international travel—an inherent part of the elite athlete’s life—can increase the risk of illness in athletes.97 106
The Olympic Games are also subject to crowding of athletes, support staff and organising committee staff in the Olympic Village and venues. In addition, in PyeongChang, there were concerns about the hygiene in the Village and the workforce. These are factors that can influence the facility with which viruses and bacteria spread, and hence the incidence of infectious disease. Finally, a number of the cross-country skiing and biathlon events were held late in the evening, chiefly to accommodate projected peak viewership hours of international broadcasting. This may potentially have negatively influenced the frequency of respiratory illness, as the environmental and thermoregulatory conditions (cold temperatures and high wind speeds) often were exacerbated at these late hours.
When preparing for and going to events, athletes and their support staff should be aware that several effective behavioural, nutritional and training strategies exist to lower the exposure to pathogens and limit the extent of exercise-induced immunodepression, thereby mitigating the risk of illness.103 107–109
Methodological considerations
In studies on sports injury, it is usually recommended to express incidences using a measure of time exposed to risk as the denominator.28–30 110 111 However, considering the inherent complexity and size of the Olympic Games, this was not feasible in the present study. Instead, we expressed the injuries or illnesses by means of absolute risk: the number of new cases per 100 exposed athletes (incidence proportion). This approach erroneously assumes that the frequencies and lengths of exposure are identical in all sports and that the number of athletes at risk in each NOC is constant throughout the Games. Interpretation of differences in injury incidences or patterns should therefore be made with caution.
In the current study we defined injuries and illnesses as new or recurring injuries or illnesses receiving medical attention, regardless of the consequences with respect to absence from competition or training. By using such a definition, predominantly the moderate and severe acute injuries will be recorded. The less serious injuries may be overlooked, since such injuries do not always require medical attention,112 113 although our results show that the majority of reported injuries were not estimated to involve any absence from the sport. This finding may perhaps reflect that elite athletes have different coping mechanisms for pain to endure the demands of elite competition in which they continue to compete despite acute or overuse injury.
In the Olympic Games, all athletes have access to healthcare through the athletes’ village polyclinic and the venue medical stations. However, the availability, size and quality of the NOCs’ own medical teams vary between countries, meaning that not all athletes benefit from identical healthcare, which may bias the injury and illness recording.
In terms of the NOC response rate (of the countries with ≥10 athletes), we received 98% of the expected daily reports. This is higher than in Rio 2016 (74%), but similar to Sochi 2014 (99.7%) and London 2012 (96%). We believe the excellent response rate, as well as an observed improvement of data accuracy (less missing data), can partly be attributed to the implementation of a new electronic data collection system, which facilitated the daily data entry. In addition, as an incentive, we gifted a tablet computer at the end of the Games to NOCs with a 100% response rate.
Twenty-seven per cent of the injuries and a mere 6% of the illnesses were captured by both the NOC and the PyeongChang 2018 medical personnel, underlining the importance of both recorder groups. As it is possible that some cases were captured neither by the NOCs nor the PyeongChang medical staff, our results may potentially underestimate the true incidence of injuries or illnesses. Our study also shows that, in particular, athletes from smaller NOCs benefit from diagnosis and treatment from the local organising committee’s medical staff, whereas the majority of athletes from larger NOCs are seen by their own NOC medical staff. More importantly, we once again identified an inverse relationship between NOC size and the risk of health problems, this time with athletes from the smallest NOCs experiencing significantly more illnesses compared with the largest NOCs. It is unknown whether this trend is related to differences in resources available to the NOCs, or to higher accuracy in the data recorded by PyeongChang 2018 staff (who to a larger degree treated athletes from smaller NOCs). In any event, the larger delegations usually come from countries with well-developed exercise physiology and sports medicine communities, and are generally able to offer their athletes more comprehensive healthcare and closer medical follow-up both in the lead up to and during the Games, potentially giving them a competitive advantage.
Practical implications
It is evident that there is a certain risk of injury inherent to any sports participation. While it would be entirely unrealistic to completely eradicate all injuries in sport, a very reasonable aim is to try to mitigate the risk—without changing the nature of the sport. Finding ways to mitigate health risks and protect the health of athletes, while still preserving the integrity of the sport, is the responsibility of all sports federations.
Based on epidemiological data collected in the Olympic Games and by FIS over the last 8 years, the IOC and FIS have initiated a set of studies looking into how and why injuries in the high-risk sports of snowboard and ski cross and slopestyle occur, with a long-term aim of developing injury prevention measures. The specific aim in these studies is to validate and develop tools to simulate jump construction as part of the course design. Such tools are only as valid as their input parameters, such as the take-off speed and angle, friction between ski/snowboard and the snow, air drag/lift, the range athletes can adjust the take-off direction by muscular work (‘pop’), and use of the table shape/curvature. With this project, we hope to contribute to build a broader understanding of how the variability in these parameters can be monitored and controlled for in a validated model, and thus help to plan the design and construction of safe but attractive jumps in several disciplines. The aim is to mitigate landing impact and injury risk—while still providing the athlete with the desired course characteristics and airtime. As different sports and disciplines change moving in the future, the epidemiological data collected by sports federations must be followed up by mechanism and risk factors studies, which in turn can inform injury and illness prevention initiatives. Such frameworks will allow athletes to perform at their highest level and take sports into the future, all the while keeping risks to their health to a minimum.
Conclusion
In summary, 12% of the athletes had a reported medical encounter for a new or recurrent injury and 9% an illness during the PyeongChang Olympic Winter Games. The variations in incidence and characteristics of injuries and illnesses between sports and sexes indicate significantly different risk factors profiles, influenced by the characteristics and rules of the individual sport. Our results can inform both the planning and provision of healthcare to athletes in different sports, as well as further research on the aetiology of the injuries and illnesses which they incur.
What are the findings?
Overall, 12% and 9% of the athletes incurred at least one injury or illness, respectively, during the PyeongChang 2018 Olympic Games.
Ski halfpipe (28%), snowboard cross (26%), ski cross (25%), snowboard slopestyle (21%) and aerials (20%) were the sports with the highest incidence of injury.
Biathlon (15%), curling (14%), bobsleigh (14%) and snowboard slalom (13%) were the sports with the highest illness incidence.
How might it impact on clinical practice in the future?
These injury and illness data can help inform policy and planning of major multisport events (eg, Olympic Games, Asian Winter Games, Winter X Games).
These data must inform the focus and development of injury prevention measures in sport.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Acknowledgments
We would like to acknowledge the contribution and support of the PyeongChang 2018 staff throughout the different stages of this study, particularly Chief Medical Officer, Prof Dr Young Hee Lee. We would also like to thank Dr Morten Fagerland at the Oslo Centre for Biostatistics and Epidemiology, Oslo University Hospital, for his important contributions to the statistical analyses. Finally, we would like to sincerely thank all the NOC medical staff contributing to the data collection: Dr Alban Merepeza (Albania), Dr Magdalena Kast (Argentina), Dr James McLaren (Australia), Dr Peter Braun (Australia), Dr Juergen Barthofer (Austria), Dr Anar Bagirov (Azerbaijan), Dr Henadz Zaharodny (Belarus), Dr Johan Bellemans (Belgium), Dr Said Fazlagic (Bosnia and Herzegovina), Dr Roberto Nahon (Brazil), Dr Parvran Parvanov (Bulgaria), Dr Robert McCormack (Canada), Dr Rodney French (Canada), Dr Suzanne Leclerc (Canada), Dr Lanne Peters (Canada), Dr David Manning (Canada), Dr Jeff Purkis (Canada), Dr Francis Fontaine (Canada), Dr Erika Persson (Canada), Dr Mireille Belzile (Canada), Dr Katie MacGregor (Canada), Dr Stephen French (Canada), Dr Mark Borzecki (Canada), Dr Jessica Curran (Canada), Dr Jose Rubio (Chile), Dr Carol Shuhua Dai (Chinese Taipei), Dr Judit Hernandez (Colombia), Dr Zoran Prso (Croatia), Dr Jakub Hermanek (Czech Republic), Dr Jiri Neumann (Czech Republic), Dr Vladimir Dobes (Czech Republic), Dr Kim Larsen (Denmark), Dr Pablo Sarmiento (Ecuador), Dr Mihkel Mardna (Estonia), Dr Maarit Valtonen (Finland), Dr Klaus Koehler (Finland), Dr Philippe Le Van (France, Andorra, Monaco), Dr Olivier Matarase (France), Dr Arthur Brule (France), Dr Mamuka Khabareli (Georgia), Dr Bernd Wolfarth (Germany), Dr Derick Macleod (Great Britain), Dr Stratos Karetos (Greece), Dr Erica Yu (Hong Kong), Dr Andras Tallay (Hungary), Dr Toth Szabolcs (Hungary), Dr Maria Magnusdottir (Iceland), Dr Bahram Savehshemshaki (Iran), Dr Sarah Jane McDonnell (Ireland), Dr Lubov Galitskaya (Israel), Dr Barbara Di Giancinto (Italy), Dr Claudio Gallozzi (Italy), Dr Jenny Birch (Jamaica), Dr Makoto Yoshida (Japan), Dr Toru Okuwaki (Japan), Dr Irina Myuller (Kazakhstan), Dr Jungjoong Yoon (Korea), Dr Liga Cirule (Latvia), Dr Raymond Succar (Lebanon), Dr Nebojsha Nastov (Macedonia), Dr Sasho Popovski (Macedonia), Dr Carlos Pruneda (Mexico), Dr Larisa Pipo (Moldova), Dr Bayartuya Bayarsaikhan (Mongolia), Dr Cees-Rein van den Hoogenband (The Netherlands), Dr Rutledge Ginny (New Zealand), Dr Rebecca Longhurst (New Zealand), Dr Effi Usen (Nigeria), Dr Mona Kjeldsberg (Norway), Dr Alexander Fomin (Olympic Athletes from Russia), Dr Shahid Nadeem (Pakistan), Dr Hubert Krysztofiak (Poland), Dr Dan Valentin Anghelescu (Romania), Dr Goran Vasic (Serbia), Dr Roman Fano (Slovakia), Dr Vladimir Vachalik (Slovakia), Dr Matjaz Turel (Slovenia), Dr Inaki Arratibel (Spain), Dr Diego Garcia-German (Spain), Dr Lykke Tamm (Sweden), Dr German Clenin (Switzerland), Dr Stefan Froehlich (Switzerland), Dr Walter Frey (Switzerland), Dr Lukas Weisskopf (Switzerland), Dr Christian Schlegel (Switzerland), Dr Hanspeter Betschart (Switzerland), Dr Patrik Noack (Switzerland), Dr María Vittoria Comune (Thailand), Dr Michel Frenzel-Assih (Togo), Dr Tim Allardyce (Tonga), Dr Adem Cali (Turkey), Dr Igor Marunchak (Ukraine), Dr Bill Moreau (USA), Dr Dustin Nabhan (USA), Dr Kyle Wilkens (USA) and Dr David Weinstein (USA).
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
Footnotes
Contributors All authors contributed to the study conception and design, and data collection and interpretation. TS analysed the data and drafted the paper. All authors provided revisions and contributed to the final manuscript. TS is the guarantor.
Funding The IOC funded the data collection of the study.
Competing interests TS works as Scientific Manager in the Medical and Scientific Department of the IOC. LE is Head of Scientific Activities in the Medical and Scientific Department of the IOC, and Editor of the British Journal of Sports Medicine and Journal of Bone and Joint Surgery.
Patient consent for publication Not required.
Ethics approval The study was reviewed by the Medical Research Ethics Committee of the South-Eastern Norway Regional Health Authority (2011/388).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.