Article Text

Abstract
Background This updated systematic review reports data from 2009 on the prevalence, and risk factors, for knee osteoarthritis (OA) more than 10 years after anterior cruciate ligament (ACL) tear.
Methods We systematically searched five databases (PubMed, EMBASE, AMED, Cinahl and SPORTDiscus) for prospective and retrospective studies published after 1 August 2008. Studies were included if they investigated participants with ACL tear (isolated or in combination with medial collateral ligament and/or meniscal injuries) and reported symptomatic and/or radiographic OA at a minimum of 10 years postinjury. We used a modified version of the Downs and Black checklist for methodological quality assessment and narrative synthesis to report results. The study protocol was registered in PROSPERO.
Results Forty-one studies were included. Low methodological quality was revealed in over half of the studies. At inclusion, age ranged from 23 to 38 years, and at follow-up from 31 to 51 years. Sample sizes ranged from 18 to 780 participants. The reported radiographic OA prevalence varied between 0% and 100% >10 years after injury, regardless of follow-up time. The studies with low and high methodological quality reported a prevalence of radiographic OA between 0%–100% and 1%–80%, respectively. One study reported symptomatic knee OA for the tibiofemoral (TF) joint (35%), and one study reported symptomatic knee OA for the patellofemoral (PF) joint (15%). Meniscectomy was the only consistent risk factor determined from the data synthesis.
Conclusion Radiographic knee OA varied between 0% and 100% in line with our previous systematic review from 2009. Symptomatic and radiographic knee OA was differentiated in two studies only, with a reported symptomatic OA prevalence of 35% for the TF joint and 15% for PF joint. Future cohort studies need to include measurement of symptomatic knee OA in this patient group.
PROSPERO registration number CRD42016042693.
- anterior cruciate ligament
- knee osteoarthritis
- risk factor
Statistics from Altmetric.com
Introduction
Anterior cruciate ligament (ACL) tears are common injuries1 with an annual incidence in the general population of 68.6 per 100 000 person-years.2 However, the incidence rates among specific sports are reported to be higher (eg, soccer, football, team handball).1 The ACL tears occur mostly in young athletes,3 and about 50% of those injured do not return to their preinjury sport activity.4 The most important consequence of an ACL tear is development of knee osteoarthritis (OA) at a relatively young age. Post-traumatic OA results in a longer period of joint-related morbidity compared with the non-traumatic OA as developed in elderly,5 and reduced quality of life is found in this group.6
In 2009, we published a systematic review on the prevalence and risk factors for radiographic knee OA after ACL tear.7 The systematic review included 7 prospective and 24 retrospective cohort studies. In the studies with the best methodological quality, that is, the seven prospective studies, 0%–13% of participants with isolated ACL tears had radiographic OA and 21%–48% of those with additional meniscus injury. Most studies were retrospective, with high quality and low quality (24 of 31 studies). Since this review, additional reviews have investigated different aspects of ACL tear and its consequences. Ajuied et al 8 found ACL tear to increase the risk of radiological knee OA [defined with the Kellgren & Lawrence (K&L) classification system] by nearly five times. Riccardo et al 9 reported mild signs of joint degeneration in 12 included studies of isolated ACL tears. Other studies investigated predictors for tibiofemoral (TF) and patellofemoral (PF) OA,10 or compared operative and non-surgical management.11–13 The lack of high-quality studies was highlighted, and caution recommended when reviewing the results. No systematic reviews reported the prevalence of symptomatic knee OA. Knee pain is the most important criteria to diagnose OA,14 and there is lack of knowledge of symptomatic OA in individuals with ACL tear. We argue that radiographic diagnosed OA alone has limited clinical interest. The aim of this study was to conduct an update of the systematic review from 2009 on the prevalence and risk factors for radiographic knee OA more than 10 years after ACL tear. In addition, we added a summary of the prevalence and risk factors for symptomatic knee OA more than 10 years after ACL tear.
Methods
We reported this systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.15 This systematic review is an update of a previous systematic review with the same inclusion and exclusion criteria. We included only new data from 1 August 2008 to 1 August 2018 in this study.
Study selection
The inclusion criteria were: prospective or retrospective cohort study designs, participants with ACL tear treated surgically or non-surgically, isolated ACL tear or ACL tear combined with meniscal and/or medial collateral ligament tear, radiographic assessment as one of the outcomes, a follow-up time of a minimum 10 years, studies published after 1 August 2008, and studies reported in English or Scandinavian languages. The exclusion criteria were: studies on skeletally immature participants, and animal studies. If several cohort studies appeared to be from the same study sample, we included the study that was most relevant according to our research question with emphasis on the prevalence of radiographic and symptomatic OA, and risk factors for OA.
Data sources and searches
Systematic searches were performed until 1 August 2018 in five different databases by two of the authors (MML and BEØ): PubMed, EMBASE, Cinahl, AMED and SPORTDiscus. A librarian at the Oslo Metropolitan University helped building up the systematic searches. The search strategy for the databases is presented in online supplementary appendix 1. Additionally, we hand searched for relevant published papers in recent systematic reviews, the included studies reference list and other relevant studies.
Supplemental material
Data extraction
Two authors (MML and BEØ) extracted the study characteristics, including: type of study, number of participants at start and follow-up, age, sex, type of treatment, concomitant injuries, reinjuries, the knee compartment investigated, the prevalence of symptomatic and radiographic OA, the radiological classification system used, and the radiological method. In cases where studies reported raw data for the radiographic outcome, we based the extracted data on the specified radiological classifications systems’ cut-off values. Reported risk factors were extracted from all studies that used regression analysis.
Study methodological quality assessment
Four of the authors (MML, LE, KS and MAR) independently assessed the study quality according to guidelines from the Centre of Reviews and Dissemination,16 and questions from the Downs and Black checklist.17 The checklist was modified and operationalised for the purpose of this systematic review. Each component of study quality was rated with YES (1 point), NO (0 points) or UNCLEAR (0 points). Studies with a score ≥8 (>60% of the maximal attainable score) were classified as high quality according to another systematic review from our group.18 Two authors scored the studies independently, and then the scores were compared (MML and LE; MML and KS; MML and MAR). In cases of disagreement, the authors tried to achieve consensus. If consensus was not reached, a third author (BEØ) gave a final judgement.
Data synthesis
The large heterogeneity in the reporting of outcomes in the included studies precluded meta-analysis. We used narrative synthesis to investigate and report similarities, differences and results between the included studies.19 20 The results from this update were discussed against the results from the systematic review from 2009.
Results
Identification and selection of the literature
The systematic searches identified 1853 new studies from 1 August 2008. After removing duplicates, 1712 studies were screened by title and/or abstract. A total of 57 studies were considered as eligible and were read in full-text. Of these, 16 studies were excluded, as they did not fulfil our inclusion and/or exclusion criteria. Finally, 41 studies were included in this systematic review (figure 1). Of these, 23 had a prospective study design,21–42 and 18 had a retrospective study design.43–60

Flow diagram. OA, osteoarthritis.
Excluded studies
We were not able to extract the OA prevalence from five studies.58 61–64 The respective authors were contacted by mail in an attempt to receive the data, and one author responded.58 The systematic searches identified 16 studies using data from the same cohort.27 28 32 36 41 42 54 65–73 We excluded eight of these66–73 to avoid reporting OA prevalence from the same cohort. In the study by Holm et al 42 we only extracted the PF OA prevalence as the TF OA prevalence data was reported in the study by Øiestad et al.27
Description of the included studies
The characteristics of the included studies are presented in online supplementary table 1. A total of 4919 participants were included, and sample sizes ranged from 18 to 780 participants. The male and female sample sizes varied from 7 to 106 and 0 to 109, respectively. Age at inclusion ranged from 23 to 38 years (28.1±3), and age at follow-up ranged from 31 to 51 (42.2±5) years. A total of 4709 participants (96%) were treated surgically, and 210 (4%) were treated non-surgically. Thirty-five studies evaluated surgically treated participants only,21–30 32 34 35 38–46 48–53 55–60 65 and six studies evaluated both surgically and non-surgically treated participants.31 33 36 37 47 54 Twelve studies21 27 28 37 39 40 42 45–48 53 reported OA results for the contralateral knee, involving 833 knees. Eighteen studies used bone-patellar-tendon-bone (BPTB) graft,23 28–30 32 36–38 42–44 47 48 51 53 54 56 57 12 used hamstring tendon (HT) graft,22 24 25 33 39 41 46 49 50 52 58 60 seven studies included both BPTB and HT graft,21 26 27 35 45 59 65 two studies used synthetic graft,34 55 and one study used HT and synthetic graft.40 One study did not report the type of graft.31 The follow-up time ranged from 10 to 24 years, with a mean follow-up time of 13.7 years.
Supplemental material
Methodological quality
Online supplementary table 2 shows the methodological quality assessments. The lowest score achieved was 3, and the highest was 11. Nineteen studies (46%) achieved a score ≥8 and were considered to have high quality. The prospective studies achieved a mean score of 7.8 with a highest score of 11 and a lowest score of 3. The retrospective studies achieved a mean score of 6.7 with a highest score of 11 and a lowest score of 3. In 3.6% of the questions the authors could not reach consensus regarding the score, and the third author (BEØ) gave final judgement. Twenty-seven studies21–23 31–37 39–41 44–46 48 49 51–55 57 58 60 65 did not fulfil the criteria for confounding factors, 30 studies21–23 25–27 29–36 38 40 42 45 48 50–58 60 65 did not fulfil the criteria of appropriate sample size calculation and drop-out rates, and 22 studies23 25 29 30 34–36 38 43 44 49–59 65 73 did not fulfil the criteria for description of qualified radiologist in the Method section. In total, 12 studies23 34–36 51–55 57 58 65 failed to report both confounding factors, sample size calculation and drop-out rate, and had no information on qualified radiologist was included in the outcome assessment.
Supplemental material
Prevalence of radiographic OA
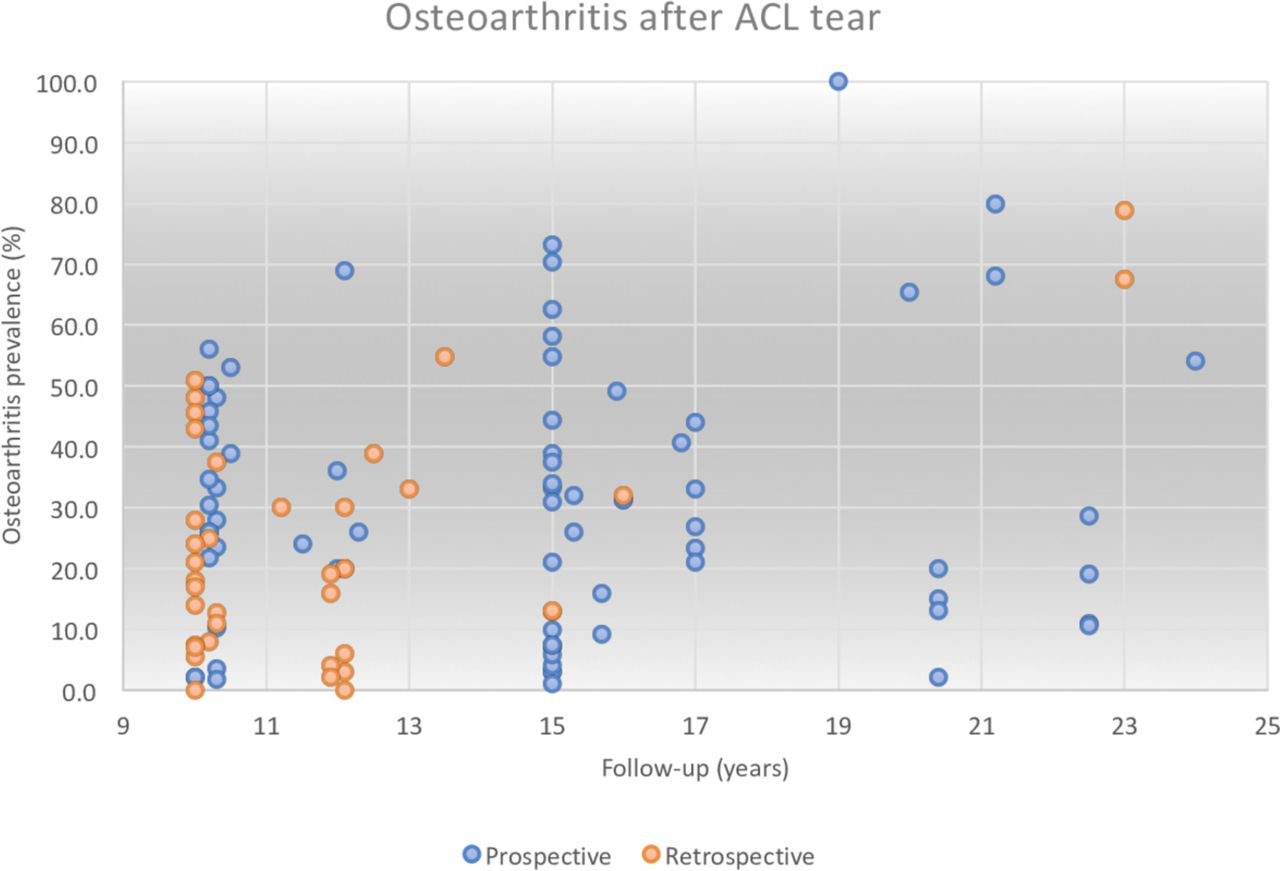
The prevalence of radiographic OA in the TF joint ranged from 0% to 100% (online supplementary table 3). The retrospective and prospective studies reported a prevalence of radiographic knee OA between 0%–79% and 0%–100%, respectively. The high-quality and low-quality studies reported a prevalence of radiographic knee OA between 1%–80% and 0%–100%, respectively. Fourteen of the included studies22 23 25 28 31 32 36 38 39 42 43 49 59 60 reported radiographic OA prevalence for the PF joint, ranging from 0% to 41%. Of these, one study28 reported and investigated the prevalence of radiographic OA in the PF joint solely (26%). Six studies31 33 36 37 47 54 reported OA prevalence for surgically and non-surgically treated participants, which varied from 23% to 80% and 8% to 68%, respectively. Participants treated with BPTB graft had OA prevalence varying between 2% and 80%, and participants treated with HT graft had OA prevalence varying between 0% and 73%. Three studies34 40 55 investigated OA prevalence in participants treated with synthetic graft, showing an OA prevalence of 39%, 50% and 100%. Figure 2 illustrates the radiographic OA prevalence for the range of follow-up time.
Supplemental material

Illustration of radiographic osteoarthritis prevalence. ACL, anterior cruciate ligament.
Eleven of the included studies21 27 28 37 39 40 45–48 53 reported radiographic OA prevalence in the contralateral knee, ranging from 2% to 38%. Of these, five studies reported results from uninjured contralateral knees,27 28 45 48 53 four studies21 39 40 42 reported additional injuries to the contralateral knee (ACL injury, chondral lesion, meniscal injury, medial collateral ligament and lateral collateral ligament injury), while three studies37 46 47 did not provide any information regarding additional injuries to the contralateral knee.
Prevalence of symptomatic OA
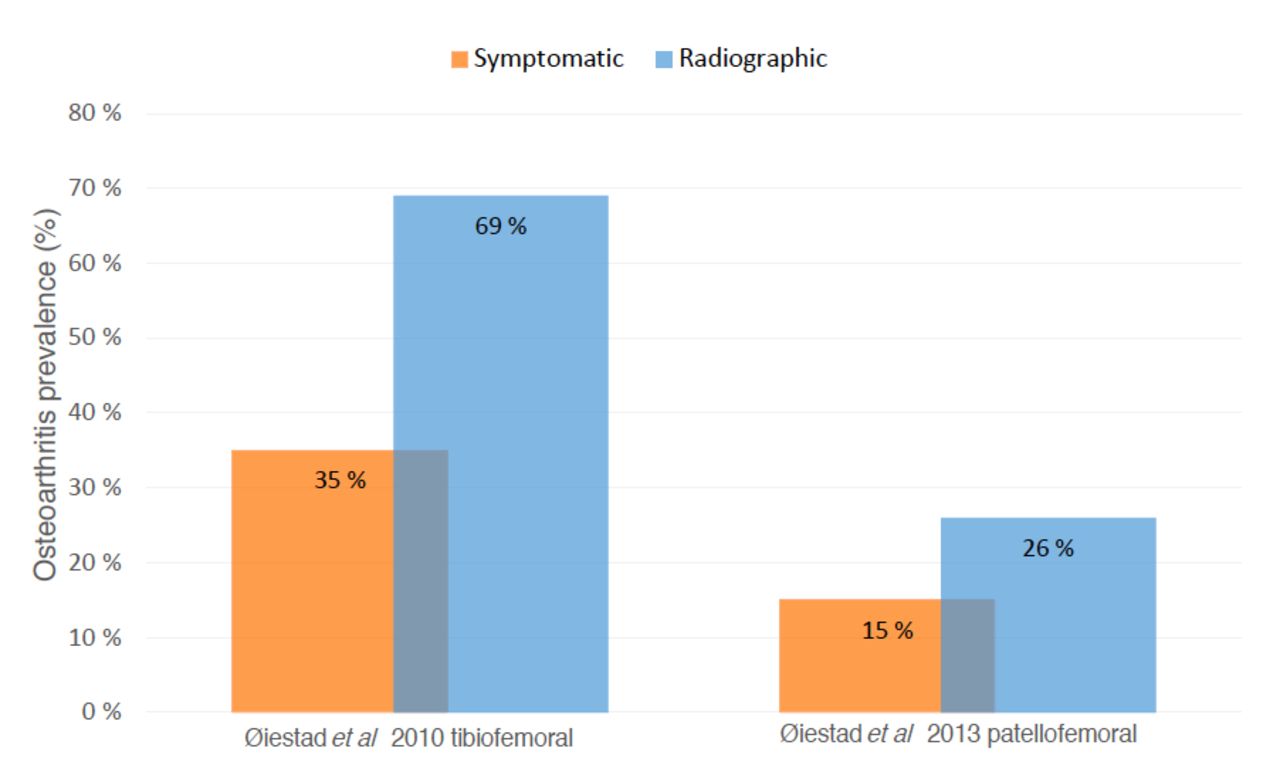
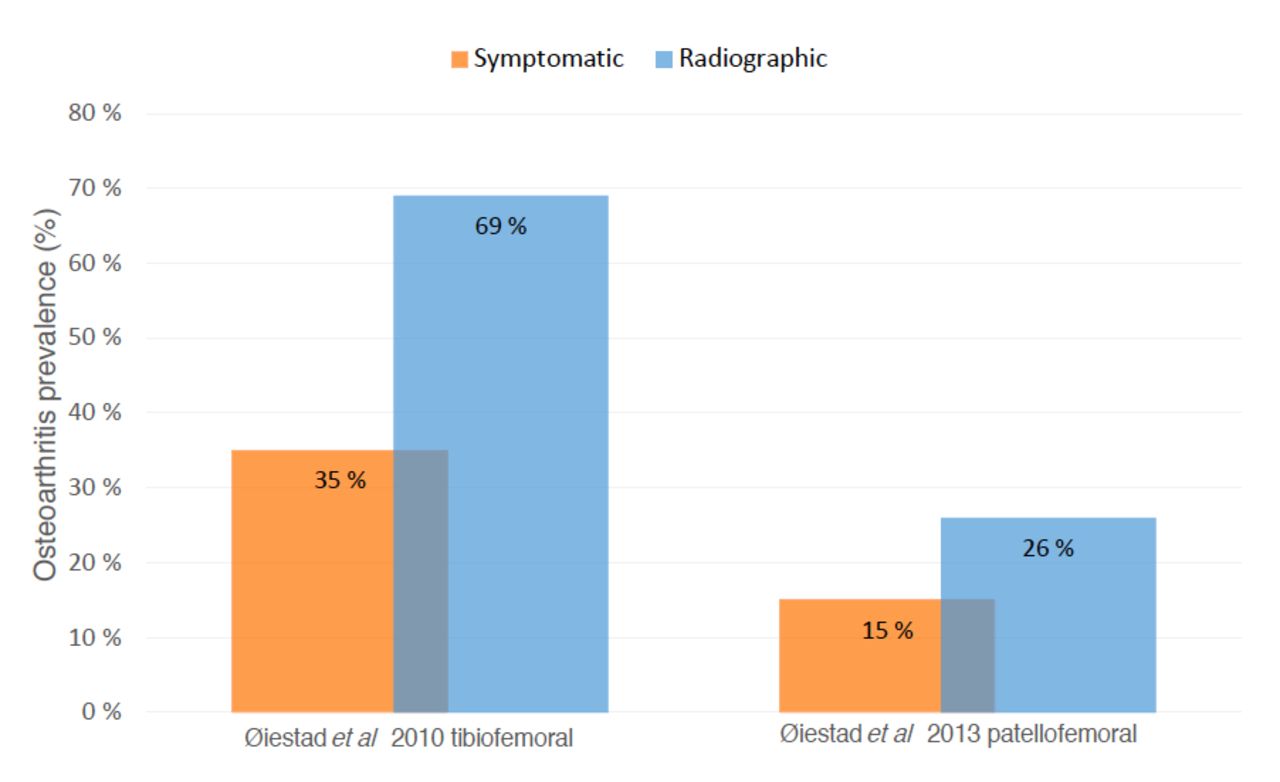
Two studies evaluated the prevalence of symptomatic knee OA.27 28 Of these, one study27 reported a 35% symptomatic OA prevalence for the TF joint, and one28 study reported a 15% symptomatic OA prevalence for the PF joint (figure 3).
{kind=link}
{kind=link}
{kind=link}
Comparison of symptomatic and radiographic knee osteoarthritis.
Risk factors for the development of knee OA
A total of 26 studies reported risk factors, and all but one study23 used statistical analysis for identification of risk factors. Twelve studies investigated risk factors by regression analysis,22 24 26–30 32 38 43 50 59 and three reported adjustment for confounding variables.27 28 30 Of these three, two27 30 studies reported risk factors for radiographic knee OA, one study27 investigated risk factors for symptomatic knee OA and one study28 investigated risk factors for PF OA.
Risk factors for radiographic OA
The reported risk factors for radiographic TF OA were increased age at surgery, additional injury, range of motion loss at final follow-up, partial medial meniscectomy and articular cartilage damage. For PF OA, the reported risk factors were increased age, TF OA, impaired knee function, more symptoms, pain during activity and kneeling pain.
The variables reported as non-significant risk factors for TF OA were quadriceps muscle weakness measured in absolute values (joules) or absolute values normalised to bodyweight (%BW), functional tests and removal of lateral meniscus. For PF OA the variables reported as non-significant were knee laxity, self-reported knee function, quadriceps strength and hop test up to 2 years postoperatively.
Risk factors for symptomatic OA
The reported risk factors for symptomatic knee OA were impaired self-reported knee function 2 years postoperatively and loss of quadriceps strength between 2 and 10–15 years. Non-significant risk factors for symptomatic knee OA were quadriceps muscle weakness measured in absolute values (joules) or absolute values normalised to bodyweight (%BW) and functional tests. Online supplementary appendix 2 shows the results for the reported risk factors for all 12 studies using regression analysis.
Supplemental material
Discussion
This updated systematic review found that knee OA prevalence varied from 0% to 100%. We identified 41 new studies from 2008 investigating 4919 individuals with ACL tear with a mean follow-up time of 13.7 years. Low methodological quality was revealed among more than half of the studies. In the present review we also investigated the prevalence of symptomatic knee OA, and found it to be 35% for the TF joint and 15% for the PF joint.
The reported prevalence of radiographic OA varied between 0% and 100%, regardless of follow-up time as shown in figure 2, which is consistent with the reported prevalence from the previous systematic review from 2009. In three of the 41 studies, the participants had isolated ACL injury at study start, but at follow-up all 41 studies reported additional injuries. Importantly, the majority of the studies did not concretise how many of the participants who had an additional injury or not, and none of the included studies reported radiographic and/or symptomatic OA prevalence only for participants with isolated ACL tears at follow-up. In the review from 2009, eight studies reported OA prevalence for knees with isolated ACL tear with a prevalence varying between 0% and 13%, contrary to 21%–48% in combined ACL injuries.7 The lower OA prevalence reported in isolated ACL tears indicates that the additional injuries occurring at the time of ACL tear, and/or subsequently may be an important contributor to OA development,74 as is also supported by others.9
Radiographic OA was described in 2%–38% of contralateral knees (from 12 studies). This indicates a higher OA prevalence in the contralateral knee compared with the global age-standardised prevalence, which is reported to be 3.8%.75 An ACL tear may cause bilateral movement responses, leading to proprioceptive deficits in the healthy knee from the ACL injured knee.76–78 Such adaptations may predispose the contralateral knee to overuse and result in premature OA development, compared with the general population. As knee OA is a complex interaction affected by multiple factors, one cannot rule out the possibility that heavy physical work, kneeling, crawling, repetitive movements and/or genetics79 80 have contributed to the higher occurrence of OA in the contralateral knee as seen in this systematic review.
PF radiographic OA prevalence ranged between 0% and 41%. Hart et al 81 reported structural damage from MRIs of the PF joint, with a prevalence of 29% in ACL injured or reconstructed participants. Although K&L, The International Knee Documentation Committee (IKDC) and The Osteoarthritis Research Society International (OARSI) are commonly used to quantify the severity of PF OA, neither of these radiological classification systems have validated definitions of the PF joint, which likely may explain some of the variation in the results.81 82 More studies are needed to evaluate the different radiological classification systems ability to detect degenerative changes in the PF joint to get a better understanding of PF OA.
OA prevalence >10 years post-ACL tear was not different in those treated surgically (8%–68%) compared with non-surgically (24%–80%), which indicates little difference in OA development between treatment options. The findings are in line with a randomised controlled trial study by Frobell et al 83 who reported no difference between surgically and non-surgically treated participants at 5-year follow-up. This is confirmed by recent systematic reviews and meta-analyses, but no RCT studies were included in these reviews.11–13 Studies have shown that ACL reconstruction is not a prophylactic treatment in the development of OA,84 85 which may explain the small differences between treatment options. Similarly, no new knowledge about the influence of graft type can be extracted from this review, also in line with findings from other studies.86–88
Symptomatic knee OA prevalence was reported in two included studies only. One study27 investigated the TF joint, and one study28 investigated the PF joint with a reported prevalence of 35% and 15%, respectively. In these two studies, approximately half of those who were diagnosed with radiographic knee OA had symptomatic knee OA. A number of authors have highlighted the poor correlation between radiologically determined OA and pain,89–93 but very few studies have investigated the prevalence of symptomatic knee OA following ACL tear. Suter et al 94 estimated that the lifetime risk of symptomatic knee OA after ACL and meniscal tears was 34%, which is similar to our findings for the TF joint. Also, Lohmander et al 95 reported 42% symptomatic radiographic knee OA in female soccer players 12 years after ACL tear, comparable to the other studies of symptomatic knee OA after ACL tear. Jones et al 96 compared participants with early and advanced structural changes in the TF joint. Their results showed that the severity of the reported pain was similar between the groups, suggesting that the degree of radiological changes does not correspond with the severity of pain. The reason for the weak correlation between radiographic findings and pain is still not fully understood.92 93 97
Risk factors for development of knee OA
Twelve of the included studies performed a thorough analysis of risk factors for OA. Nine of these did not report if they had taken confounding variables into consideration, which reduces confidence in the results. Similar findings were reported in a systematic review by van Meer et al 10 who highlighted the absence of suitable analytical approaches. A consequence of insufficiently planned studies is that the risk factors investigated are due to chance. Not adjusting for confounding variables can lead to false-positive results, as the reported findings may be a result of other underlying factors.
In total, three of the included studies did a multivariate regression analysis adjusting for confounding variables. Meniscectomy was the only consistent risk factor for radiographic OA across several studies. Meniscus injury, often treated by meniscectomy, is the most investigated and documented risk factor, and it occurs in approximately 75% of participants with ACL injury.98 The menisci provide stability in the TF joint, distributes load, absorbs shock, lubricates the knee joint and protect the articular cartilage from excessive axial loading.99 100 When damaged, the axial loading on the articular cartilage increases, which predispose and increased the risk of OA development.9 100 Studies have shown a strong correlation between meniscal lesions, cartilage loss and subchondral bone marrow lesions which are important factors in OA development.101 In the present review, meniscal injuries were commonly reported at initial ACL injury or during follow-up period, which may explain the increased OA prevalence that we report compared with isolated ACL injuries.9
In addition to meniscectomy, increased age at surgery, range of motion loss at final follow-up and articular cartilage damage were reported as risk factors for radiographic knee OA. Two of the included studies reported that quadriceps muscle weakness was not a significant risk factor for knee OA development,27 28 but prior systematic reviews have provided conflicting conclusions regarding this association.18 102 The reported risk factors are in line with other findings,10 103 but do not add new insight or increase the understanding of the development of OA. We suggest that multivariate regression analysis should be used in future multicentre prospective cohort studies with frequent follow-ups to investigate risk factors for development of symptomatic knee OA,104 and studies need to differentiate between radiographic and symptomatic OA to thoroughly explore this association.
Methodological quality assessment
Overall, the 41 included studies mean methodological quality assessment score was 7.2 out of 12 (range 3–11). Our review revealed small differences in the reported OA prevalence between the high-quality and low-quality studies. This does not correspond with the findings from the 2009 review,7 where the high-quality studies reported lower OA prevalence. It should be noted that we used different checklists and therefore the results cannot be directly compared. Unlike the 2009 review, we did not distinguish between study design in the quality assessment, which may explain the small difference between the prospective and retrospective studies.
In the literature there is no consensus regarding high or low methodological quality, and evaluating studies from this perspective can be problematic.16 We chose to distinguish between high and low quality in line with another similar article, with a cut-off score of >60%, which in this case was a score of >8.18 The results are only valid for this systematic review, and should not be directly transferred to other contexts, or interpreted as the truth.
A weakness of our quality assessment was that we did not distinguish between the impact of particular questions. Lack of fulfilling the criteria for question number 5, 7, 9 and 12 may be of greater concern for the methodological quality as these questions investigates the reporting of confounding variables, the power of the study, validity and reliability of the outcome measures, and the reliability of the radiographic readers. Many of our results did not fulfil these criteria. Consequently, the reported results from these studies have potentially a lower quality and should be considered with caution.
Limitations
This systematic review has some limitations. The studies were heterogeneous, which precluded a meta-analysis. We only included studies written in English or Scandinavian languages. Not all studies had a main purpose to evaluate the OA prevalence. The methodological quality assessment has no gold standard and should be carefully interpreted. We attempted to retrieve missing OA data, but only establish contact with the authors of one study. There is no consensus of how to define symptomatic knee OA in the literature, and the two studies in this review defined symptomatic OA as K&L >2 and reported pain on most days the last month before the assessment. Two of the included studies used the highest cut-off from the radiographic scoring system to define symptomatic knee OA. We chose not to report these findings, as one cannot assume that those with the worse radiological grading automatically corresponds with pain and symptoms. Finally, we did not include data from our study from 2009 in this update because we reported the results descriptively, and merging the studies would not change our descriptive results.
Conclusion
At a minimum of 10 years following an ACL tear the reported prevalence of radiographic knee OA varied between 0% and 100%. Two studies investigated symptomatic knee OA, showing a prevalence of 35% for the TF joint and 15% for the PF joint. Meniscectomy is a significant risk factor for OA development. No firm conclusion can be drawn from non-significant risk factors based on our results. More high-quality studies are required to detect the true prevalence of knee OA following ACL injuries. There is a strong need for studies differentiating symptomatic and radiographic knee OA. Symptomatic knee OA has high clinical relevance, and is the reason why people seek healthcare.
What is already known
The prevalence of knee osteoarthritis (OA) in individuals with anterior cruciate ligament (ACL) injury varies between 0% and 13% for isolated injuries and between 21% and 43% for combined ACL and meniscal injuries more than 10 years after the injury.
Meniscectomy is the most important risk factor for development of knee OA after ACL injury.
What are the new findings
Very few studies have differentiated between symptomatic and radiographic knee OA in ACL injured individuals.
The prevalence of symptomatic knee OA was 35% for the tibiofemoral joint and 15% for the patellofemoral joint more than 10 years after ACL injury.
The reported prevalence of radiographic knee OA varies between 0% and 100% regardless of follow-up time.
There is still an insufficient number of high-quality studies clearly reporting prevalence of knee OA after ACL injury.
Acknowledgments
None
References
Footnotes
Contributors All coauthors have read, commented and reviewed at least two versions of the manuscript and the final draft. All coauthors have been involved in the quality assessments of the articles included in the systematic review. All coauthors agreed to update the systematic review with this design and the new added research question on symptomatic knee OA. MML and BEØ performed the systematic searches and selected articles for inclusion.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.