Article Text

Abstract
Research question Does the Nordic hamstring exercise (NHE) prevent hamstring injuries when included as part of an injury prevention intervention?
Design Systematic review and meta-analysis.
Eligibility criteria for selecting studies We considered the population to be any athletes participating in any sporting activity, the intervention to be the NHE, the comparison to be usual training or other prevention programmes, which did not include the NHE, and the outcome to be the incidence or rate of hamstring injuries.
Analysis The effect of including the NHE in injury prevention programmes compared with controls on hamstring injuries was assessed in 15 studies that reported the incidence across different sports and age groups in both women and men.
Data sources MEDLINE via PubMed, CINAHL via Ebsco, and OpenGrey.
Results There is a reduction in the overall injury risk ratio of 0.49 (95% CI 0.32 to 0.74, p=0.0008) in favour of programmes including the NHE. Secondary analyses when pooling the eight randomised control studies demonstrated a small increase in the overall injury risk ratio 0.52 (95% CI 0.32 to 0.85, p=0.0008), still in favour of the NHE. Additionally, when studies with a high risk of bias were removed (n=8), there is an increase of 0.06 in the risk ratio to 0.55 (95% CI 0.34 to 0.89, p=0.006).
Conclusions Programmes that include the NHE reduce hamstring injuries by up to 51%. The NHE essentially halves the rate of hamstring injuries across multiple sports in different athletes.
Trial registration number PROSPERO CRD42018106150.
- hamstrings
- injury prevention
- intervention
- sports and exercise medicine
Statistics from Altmetric.com
Introduction
It is in sports clinicians’ DNA to prevent injuries. But is there evidence to answer the seemingly innocuous clinical question—‘If I prescribe preventive exercise will it reduce injuries?’ Given the substantial burden of hamstring injuries,1–4 we interrogated the literature to answer one question: Does a hamstring prevention exercise—The Nordic hamstring exercise (NHE)—prevent hamstring injuries.
Hamstring muscle injury is the most common muscle injury across a range of different sports.5–7 A number of intervention studies that used eccentric strengthening reduced hamstring injuries.8 Three large prospective trials (two randomised and one non-randomised) reduced injuries by approximately 70% by implementing the NHE in a team’s training regime.9–11
So why then do we need a systematic review of this type of intervention? Goode et al 12 performed a comprehensive systematic review but included just four studies, most likely due to selection criteria that only allowed for the inclusion of randomised control trials, and excluded articles not written in English. The most recent systematic review analysed the effectiveness of injury prevention programmes that included the NHE to reduce hamstring injuries in football while monitoring athlete workload.8 The results from the meta-analysis suggested that teams using the NHE (in isolation or as part of a larger injury prevention programme) reduced hamstring injury rates up to 51%. However, due to the exclusion of studies that did not provide workload data (training and match exposure) and sports other than football, this meta-analysis omits many studies that also included the NHE. The omission of relevant studies in both these previous reviews might lead to a biased estimation of the effect when including the NHE in an injury prevention programme. Further exclusion of studies that used an observational or cross-sectional design, multiple exposure groups, reporting compliance, and language, limits the generalisability of these findings. The basic clinical question is perhaps not best answered in this manner.
We, therefore, carried out an inclusive, comprehensive systematic review and meta-analysis on the effectiveness of injury prevention programmes that included the NHE in reducing the number of hamstring injuries.
Methods
Search strategy and study selection
This review has been registered in the PROSPERO database (CRD42018106150). The PRISMA statement for systematic reviews was utilised to direct the reporting and formatting of this review.13 Relevant articles were identified following a search of the electronic databases: MEDLINE via PubMed, CINAHL via Ebsco, and OpenGrey. Database entries were searched from the earliest reported date (January 1950 for Medline) to August 2018. Search terms were mapped to relevant MeSH terms. Search terms were entered into the database as the keywords ‘Nordic’ and ‘Russian’, which were grouped with the OR operator. These keywords were then combined with the operator AND to the keywords ‘hamstring’ and ‘Injur*’, which produced the search strategy and the final yield. The details from the Medline search can be found in the online supplementary file 1. To supplement the electronic database search, the reference lists of relevant papers were also cross-checked. Publication details from all studies identified in the literature search were exported to the bibliographic software. Once all search results were collated, titles and abstracts were screened for eligibility. All relevant articles were identified for full-text review and inclusion. The study selection process is presented in figure 1.
Supplementary file 1
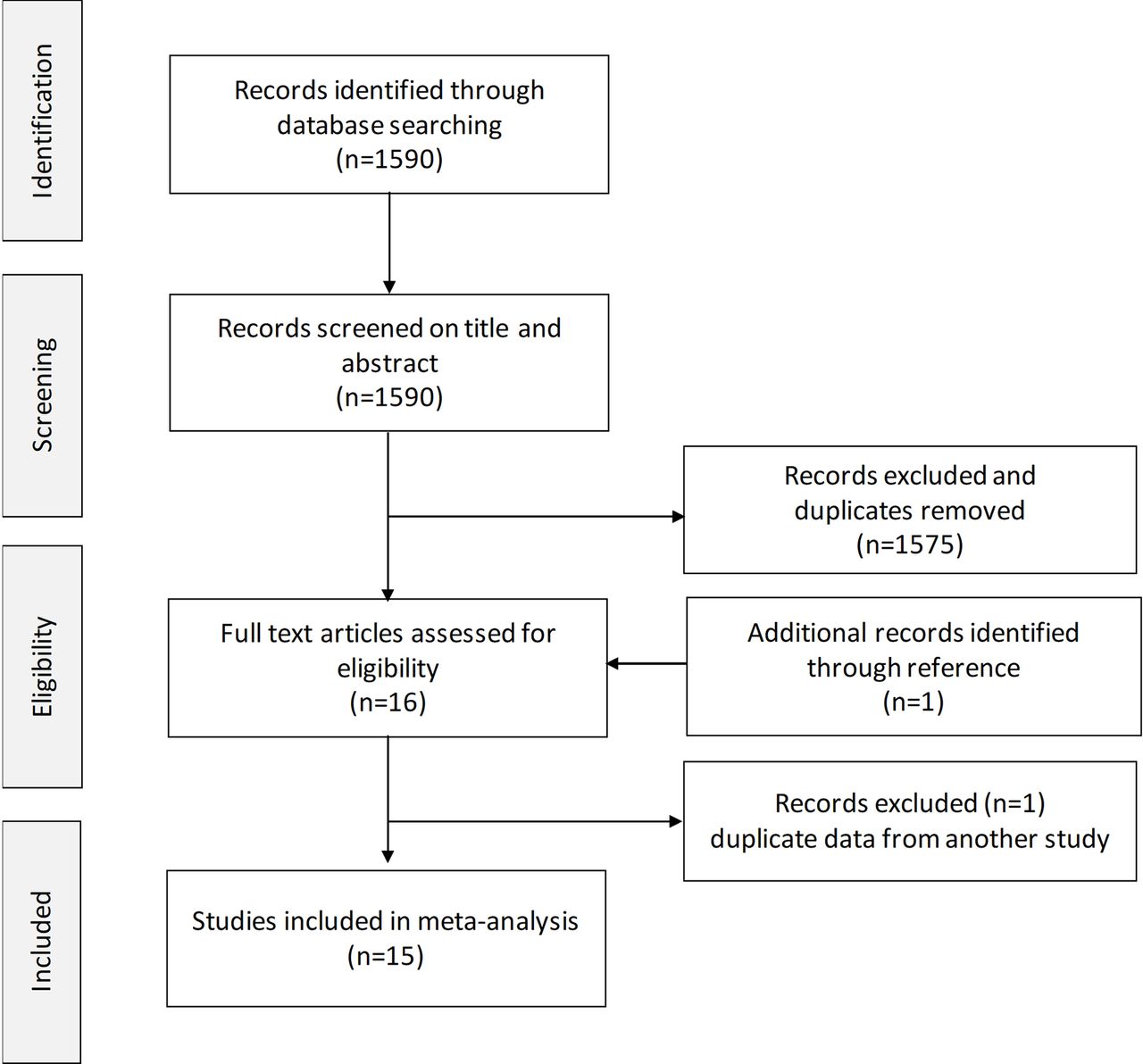
Flow chart of study selection for the analysis of the effect of prevention programmes including the NHE related to hamstring injury rates. NHE, Nordic hamstring exercise.
Eligibility criteria
For this investigation, we considered the population to be any athletes participating in any sporting activity, the intervention to be the NHE or any programme that included the NHE, the comparison to be usual training or other prevention programmes, which did not include the NHE, and the outcome to be the incidence or rate of hamstring injuries. We did not include studies without a comparison or control group, thereby excluding case series and case studies. Studies were not excluded based on gender, age or level of competition. There were no language or time limits set.
Data extraction
Two investigators (NVD and RW) conducted the initial search, duplicates were removed and articles were excluded if they did not meet the eligibility criteria. A third investigator (FPB) facilitated group consensus when disagreements were identified.
Data from the selected full-text articles were independently extracted by two investigators (NVD and RW). For each study, outcome data extracted included the number of participants and injury rates (or a number of hamstring injuries). The outcome data were imported into Review Manager (RevMan) V.5.3 (Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) where all further analyses were performed.
Assessment of methodological quality and risk of bias
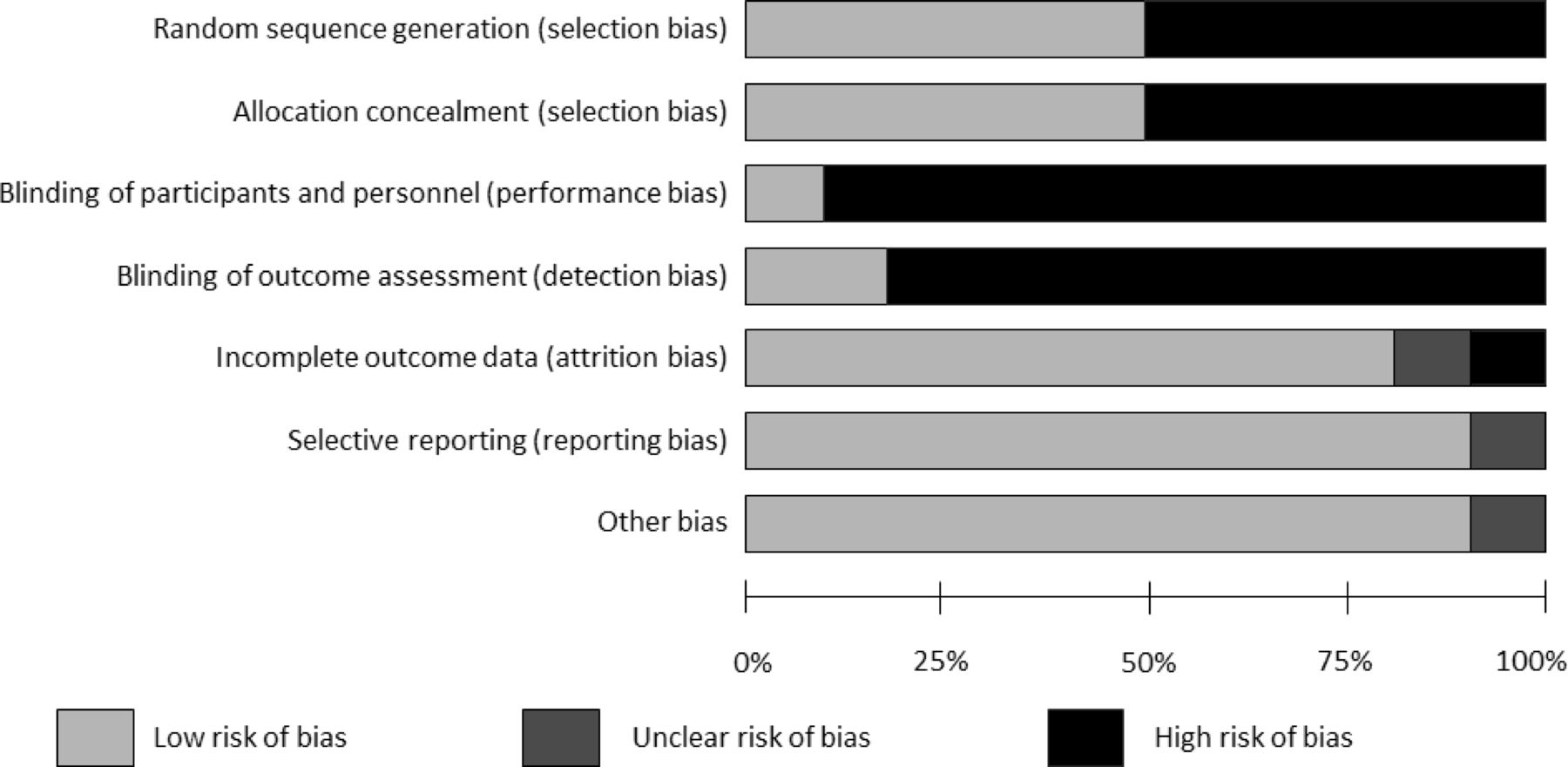
The methodological quality of each study was independently assessed by two investigators (NVD and FPB), with the third investigator (RW) resolving any discrepancies. The quality and risk of bias were evaluated according to the Cochrane risk of bias tool,14 where six domains of bias are assessed: selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias. A value of high, low or unknown risk of bias was provided for each domain.
Data analysis
The meta-analysis was performed according to the Cochrane methodology.14 The risk ratio with 95% CI was determined for the outcome of hamstring injury, and calculated as: risk of an injury in the intervention group/risk of an injury in the control group. A risk ratio of 1 indicates no difference, and a risk ratio of <1 indicate a positive intervention effect. In this meta-analysis, a random-effects model was selected, based on the assumption that the studies included diverse populations and different contexts. The NHE intervention also varied in terms of dose and test procedure.
Sensitivity analyses were performed to determine the difference in outcome when (1) only including ‘high’-quality studies (randomised control trials), (2) removing studies at high risk of allocation, detection or attrition bias, and (3) examining the pooled effect when excluding each study individually.
Results
Identification of studies
The initial database search yielded a total of 1590 potentially relevant studies. After reviewing the titles and abstracts, 15 full-text articles were retrieved for analysis. Searching the reference lists and the authors’ personal databases revealed one additional relevant study for inclusion. Following communication with one author of two eligible studies, one of the two shortlisted studies was excluded, as there was overlapping data between the studies. Consequently, the final number of studies for inclusion was 15.
Characteristics of the included studies
The characteristics of the 15 studies included in the analysis are summarised in table 1. Eight controlled trials (seven randomised and one non-randomised) and seven cohort studies were included. The studies represent different regions, including North America (n=3), UK and Europe (n=7), Scandinavia (n=5) and Australia (n=1). Two studies were performed in female athletes, while the remaining 13 studies included male athletes. The investigations were performed mainly in football (soccer), with one investigation in rugby, baseball and Australian football, respectively. The definition of injury and re-injury (or recurrent injury) varied somewhat across the 15 included studies. Seven studies do not report whether multiple injuries were included, four studies reported on recurrent injuries and four studies included only index injuries. Compliance is not reported in five studies, while four studies observed compliance of <50%. The remaining six studies all reported compliance of over 70%. The level of sport varied across the different studies and included the highest level of competition, subdivisions (second to fifth) in football, all competition levels in major league baseball, including collegiate, youth and amateur players. The players were aged 18–40 years, apart from one study in youth players (13–18 years). The NHE programme was used in isolation in six studies, while four studies included the NHE as part of the FIFA 11+ programme. All the other investigations included the NHE together with other strength, flexibility or warm-up exercises. The prescription and training volume of the NHE protocol used for each study are presented in table 2.
Characteristics of the included studies
The training protocol using the NHE across different studies (n=14)
Methodological quality and risk of bias
The risk of bias assessment is summarised in figure 2. A high risk of performance and detection bias was identified, with moderate selection bias. Attrition and reporting bias was low across the included studies. The individual assessment of high, low or unknown risk of bias for each individual study is presented in table 3.

Risk of bias summary. The authors’ judgements about each risk of bias item is presented as percentages across all included studies.
Assessment of methodological quality for each study
In the examination of the funnel plots, there is slight asymmetry, indicating that risk of publication bias may not be present (figure 3). No adjustment of the overall point estimate was warranted.

Funnel plot based on SE and log risk ratio of the studies in assessing publication bias. The diagonal lines represent the pooled injury risk ratio (RR) which is the summary measure of the study. The vertical tips of the diagonal lines are the overall effect and the lateral ends on the x-axis are the associated CIs.
Meta-analysis
The pooled data for 8459 individuals including 525 hamstring injuries were analysed from the 15 included studies. Exposure data were not available for six studies. In the remaining nine studies, the incidence of hamstring injuries (weighted by sample size) was 0.1/1000 hour for players exposed to NHE, and 0.2/1000 hour in those players who continued with usual training.
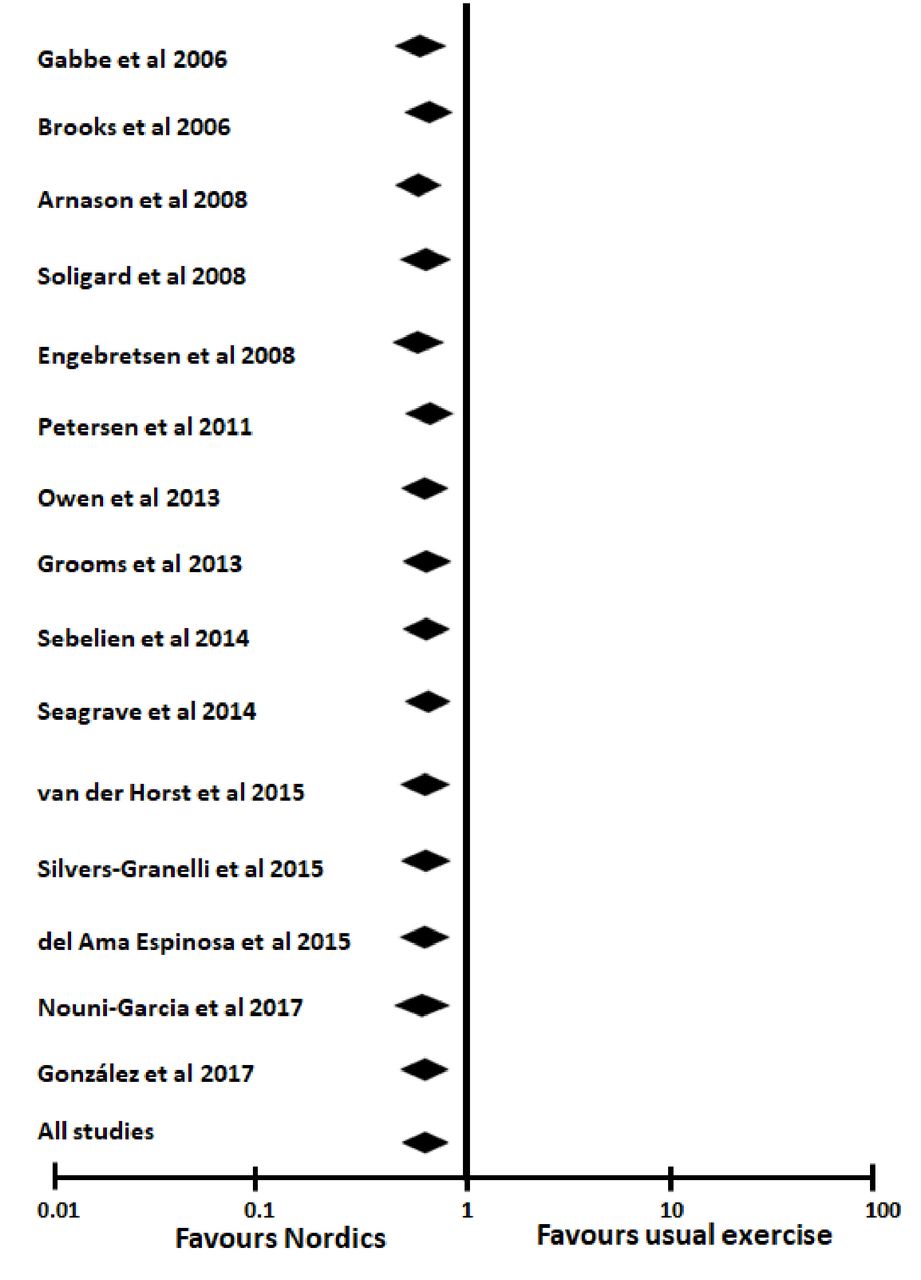
The pooled results show a 51% overall reduction in hamstring injury in the intervention group that included the NHE compared with the control group (RR 0.49, 95% CI 0.32 to 0.74, p=0.0008) (figure 4). Statistical heterogeneity across the different studies was large (I2=74%).

Primary analysis of overall hamstring injury rates in NHE prevention programmes compared with control intervention. M-H, Mantel-Haenszel; NHE, Nordic hamstring exercise.
Sensitivity analysis
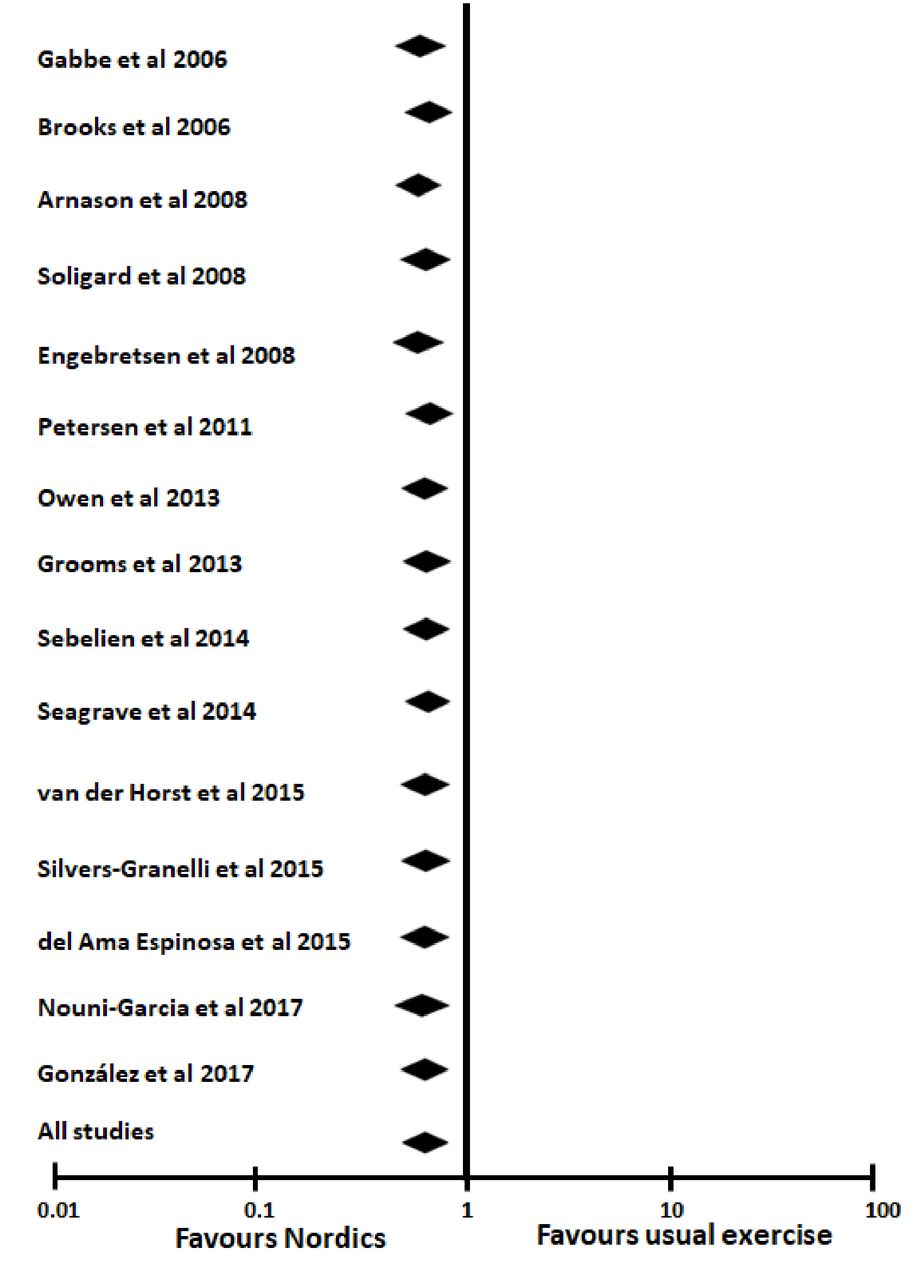
The pooled data for only the randomised control trials were analysed and the point estimate changed by 0.03 (RR 0.52, 95% CI 0.32 to 0.85, p=0.0008) (figure 5). Additional sensitivity analyses were performed by removing studies with high risk of allocation and detection bias, as well as one study with a high risk of attrition bias (figure 6), with a change in the point estimate of 0.06 (RR 0.55, 95% CI 0.34 to 0.89, p=0.006). The overall shift in effect size when systematically removing each study individually was small (figure 7).
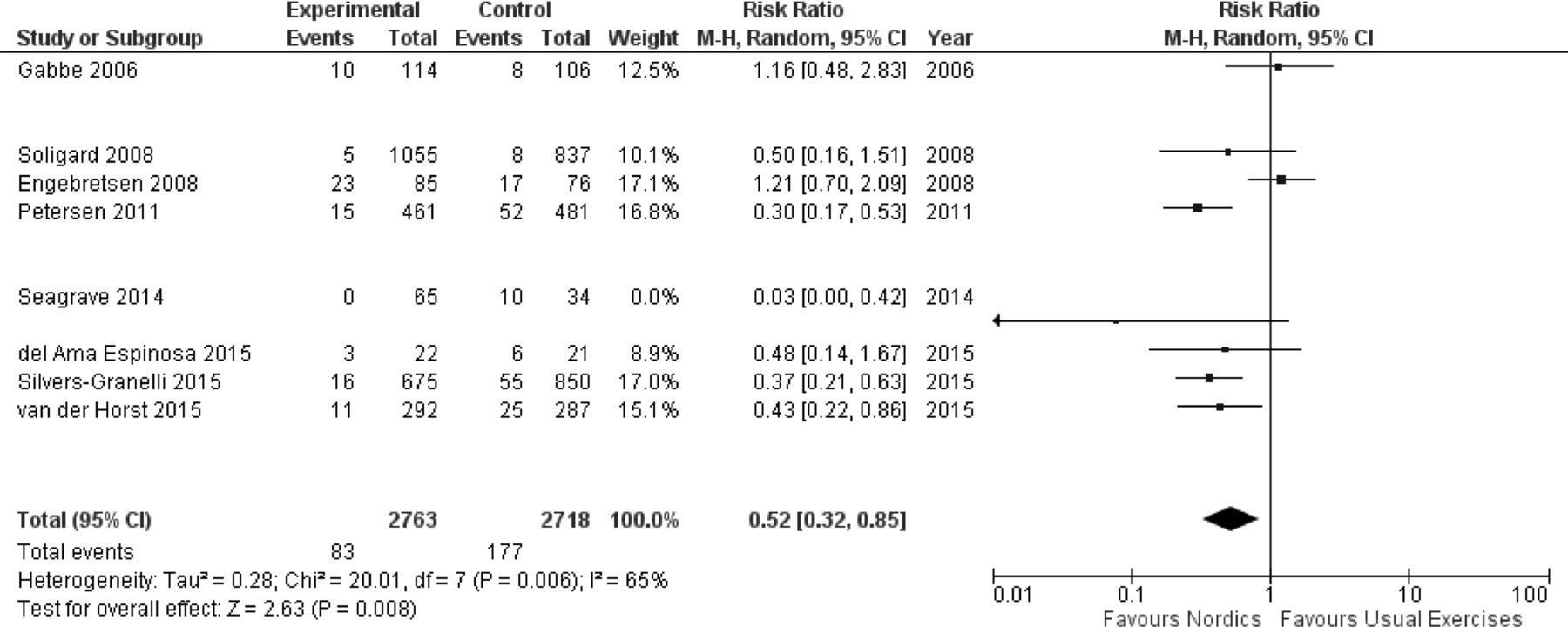
Secondary analysis of overall hamstring injury rates in NHE prevention programmes compared with control intervention when only including randomised control trials. M-H, Mantel-Haenszel; NHE, Nordic hamstring exercise.

Secondary analysis of overall hamstring injury rates in NHE prevention programmes compared with control intervention when excluding studies at high risk of allocation, detection and attrition bias. M-H, Mantel-Haenszel; NHE, Nordic hamstring exercise.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sensitivity analysis demonstrating the change in effect by systematically removing individual studies included in the meta-analysis. The effect size shown is the pooled effect when a single (named) study is removed, with the overall effect listed as a reference.
Discussion
In this systematic review and meta-analysis, including 8459 athletes and 525 hamstring injuries, the primary outcome was the overall hamstring injury rates when introducing the NHE as a preventative measure. The results indicate a statistically significant and clinically meaningful reduction of 51% in hamstring injuries for all athletes competing at different levels of competition and across multiple sports. These results support the use of the NHE in prevention programmes.
It is important to compare the results of this systematic review with previous findings from similar investigations. In 2010, Goldman and Jones reported in a Cochrane review on interventions aimed at reducing hamstring injuries.15 Of the six studies included, only two investigated the NHE as an intervention,16 17 and the results were inconclusive as to the effectiveness of the interventions. In 2014, Goode et al performed an intention to treat analysis and in their study, eccentric strengthening, with good compliance, seemed to be successful in hamstring injury prevention.12 However, due to strict inclusion criteria, only four studies were included, one of which involved a form of eccentric training other than the NHE.18 In a recent meta-analysis of injury prevention programmes including the NHE, hamstring injuries were reduced by up to 51% compared with teams that did not use any intervention.8
Different methodological approaches meant that previous meta-analysis only included studies in football and that reported exposure. The present meta-analysis included an additional 10 studies, 2 of which were published after the previous meta-analysis reported in 2016. There is an overall pooled-effect of 51% reduction of hamstring injuries when the NHE is implemented. This confirms the previous findings, irrespective of a large amount of heterogeneity identified between the studies in the present analysis. However, the use of the NHE in practice and its implementation as a prevention measure is limited.19
Systematic reviews should inform clinical practice where they can
Staying up to date with the latest scientific evidence is challenging for all clinicians. A recent educational review advocated three key steps in making quality decisions about evidence in practice: (1) systematically searching and assessing the quality of published literature, (2) combining quality research evidence with quality clinical evidence, and (3) considering the feasibility of use in the practical setting.20 Systematic reviews promise a high-quality, comprehensive summary of the research regarding an intervention, such as NHE for preventing hamstring injuries. And while we might expect systematic reviews to be accurate, they are bound by certain decision-making in how they are conducted. To ensure methodological rigour, most reviews and meta-analyses impose strict selection criteria.21 22 The purpose is to ensure methodological quality, allowing the subsequent analysis to be performed with greater precision and accuracy. However, readers must stay alert to publications with provocative titles but clinical conclusions that are not fully supported by the study results.23
In the case of the NHE, the strict methodological selection criteria might disguise the simple clinical question: regardless of gender, sport or age, will the NHE reduce hamstring injuries if I prescribe them? Many clinicians are faced with a similar reality—managing male and female athletes from a range of different sports and age groups. Therefore, we pragmatically included more clinically heterogeneous studies in this analysis.
Apart from the clinical diversity represented in these studies (different participant characteristics performed in different settings), the importance of methodological and statistical heterogeneity, and how it may influence results must not be overlooked. Grindem et al suggest different measures of assessing statistical heterogeneity, such as a funnel plot or the I2 statistic.24 Although studies were purposefully included that would increase the heterogeneity, the risk of bias assessment (figure 2) and funnel plot (figure 3) suggest that it was acceptable in this analysis. To account for methodological heterogeneity, a further sensitivity analysis was performed. When only randomised controlled trials were included, considering these studies to represent the highest level of evidence for this type of intervention, the overall pooled effect changes only minimally (figure 5). And after removing studies at high risk of bias (all studies that were determined to present a high risk of allocation and detection bias, and one study due to attrition bias), there is again no substantial change in the overall effect (figure 6).
It is worth highlighting that there was no significant reduction of hamstring injuries in the two studies investigating the effect of the NHE in female populations. Similarly, one study in Australian rules football demonstrated no significant reduction in hamstring injuries. However, none of the studies included in the analysis has a dramatic outcome on the overall effect of the meta-analysis (figure 7), which suggests that no individual study grossly influenced the overall findings. Based on these results, clinicians are encouraged to include the NHE in their prevention efforts to reduce the number of hamstring injuries, regardless of sporting code, gender or age.
Study biases and limitations
Moderate selection bias was present in the studies included, and a high risk of performance bias (figure 2). However, blinding the assessor or the participant to the intervention is likely impossible in this type of study, as it would be difficult to introduce an NHE placebo. A high risk of detection bias is present, and blinded assessors would have reduced the potential bias when outcomes are measured.
Substantial variability is present in the training protocol across different studies (table 2). It is not clear what the ideal prescription of the exercise is, although recent studies have demonstrated similar tissue adaptation and strengthening when comparing low and high volume training regimes.25 Regardless, we observe a strong overall effect even with a large amount of variability between studies.
The risk of an index hamstring injury is different from a recurrent hamstring injury.3 5 6 Only four studies in our meta-analyses focus on index injury, while the risk reduction is greater in the four studies reporting on recurrent injuries. Seven studies do not report on whether the injuries included were either index injuries or included recurrent injuries as well; therefore, a conclusive recommendation is not possible.
Clinical implications
A large amount of evidence now supports the use of the NHE to prevent hamstring injuries. The overall effectiveness of this exercise has been demonstrated repeatedly, although the mechanisms by which the NHE provides a protective effect is not yet fully understood. The NHE may increase fascicle length, leading to morphological changes that may protect the hamstring muscle from injury.26 Harøy et al have demonstrated that when performing the NHE as part of a prevention programme, an increase in strength is observed27; increasing eccentric strength may reduce the risk associated with a hamstring injury. The value of eccentric training and the NHE is recognised at elite level football,28 but the adoption of the exercise into regular training programmes is poor,19 and the overall use of the NHE in other sports is not known. The need for better understanding the factors surrounding the implementation of prevention programmes in sport has been highlighted through the Translating Research into Injury Prevention Practice framework.29
Perhaps a key component to ensuring greater success in our implementation efforts is understanding the context in which the intervention is being introduced.30 31 This would require the involvement of key stakeholders in the process of injury prevention, including the medical team, the coach and the player.32 Only when we design our prevention programmes to address hamstring injuries, and perhaps all sports injuries, in such a comprehensive manner will we be able to translate the research evidence into actual clinical practice.
Conclusion
This systematic review and meta-analysis demonstrate that the NHE is effective in reducing hamstring injuries. There is, unsurprisingly, a large amount of heterogeneity across multiple sports and differences such as age and gender between athletes, but the overall effectiveness of the NHE remains unchanged, and clinicians are encouraged to include the NHE in their prevention programmes.
What is already known
Hamstring muscle injury is a common muscle injury across different sporting codes that affects many athletes. The Nordic hamstring exercise (NHE) is an effective injury prevention tool that may reduce the number of hamstring injuries if implemented successfully.
Systematic reviews should inform clinical practice where possible, and clinicians can be confident that the inclusion of a NHE programme is supported when hamstring injury reduction is a goal.
To improve adaptation and implementation of the NHE, the focus should be directed towards dose–response relationships, as well as compliance and adherence with the prescribed exercise to improve prevention programme efficacy.
What are the findings
Hamstring injuries are reduced by 50% when the NHE is introduced as preventative training, confirming previous findings isolated to football.
The overall effectiveness of the NHE remains unchanged despite a large amount of heterogeneity between the studies in terms of age, gender and type of sport.
There is a large amount of variability in the training protocols used to introduce eccentric training through the NHE.
References
Footnotes
Contributors NvD and RW: concept, design and analysis, writing and editing of the manuscript. FPB: analysis, writing and editing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Full dataset and/or statistical code are available from the corresponding author.
Patient consent for publication Not required.