Article Text

Abstract
Objective To evaluate the comparative effectiveness of current treatment options for plantar heel pain (PHP).
Design Systematic review and network meta-analysis (NMA).
Data sources Medline, EMBASE, CINAHL, AMED, PEDro, Cochrane Database, Web of Science and WHO Clinical Trials Platform were searched from their inception until January 2018.
Study selection Randomised controlled trials (RCTs) of adults with PHP investigating common treatments (ie, corticosteroid injection, non-steroidal anti-inflammatory drugs, therapeutic exercise, orthoses and/or extracorporeal shockwave therapy (ESWT)) compared with each other or a no treatment, placebo/sham control.
Data extraction and analysis Data were extracted and checked for accuracy and completeness by pairs of reviewers. Primary outcomes were pain and function. Comparative treatment effects were analysed by random effects NMA in the short term, medium term and long term. Relative ranking of treatments was assessed by surface under the cumulative ranking probabilities (0–100 scale).
Results Thirty-one RCTs (total n=2450 patients) were included. There was no evidence of inconsistency detected between direct and indirect treatment comparisons in the networks, but sparse data led to frequently wide CIs. Available evidence does not suggest that any of the commonly used treatments for the management of PHP are better than any other, although corticosteroid injections, alone or in combination with exercise, and ESWT were ranked most likely to be effective for the management of short-term, medium-term and long-term pain or function; placebo/sham/control appeared least likely to be effective; and exercise appeared to only be beneficial for long-term pain or function.
Conclusions Current evidence is equivocal regarding which treatment is the most effective for the management of PHP. Given limited understanding of long-term effects, there is need for large, methodologically robust multicentre RCTs investigating and directly comparing commonly used treatments for the management of PHP.
PROSPERO registration number CRD42016046963.
- primary care
- meta-analysis
- review
- foot
Statistics from Altmetric.com
Introduction
Plantar heel pain (PHP) is the most prevalent soft tissue foot complaint, affecting 10% of adults during their lifetime1 and accounting for 25% of all foot disorders in athletes.2 Characterised by insidious onset, localised pain in the plantar heel region which may extend to the medial arch of the foot, the cause of PHP is unclear but is likely multifactorial. Risk factors include obesity, pronated foot type, reduced ankle or first metatarsophalangeal joint range of motion and prolonged weight-bearing.3–5 PHP reduces mobility, impairs foot and physical function and the capacity for work, all of which have a negative impact on health-related quality of life.1 6 7
In terms of primary care management, current guidance suggests a period of watchful waiting with self-management advice followed by conservative interventions if there is no improvement, including; therapist-led exercises, foot orthoses, corticosteroid injections and extracorporeal shockwave therapy (ESWT).8–10 Although PHP is commonly thought to be a self-limiting condition, resolution of symptoms in some patients may take up to 18 months.11 Research to date suggests treatments do offer potential benefits in terms of reduced pain and improved function,1 but clinical decision-making is hampered due to a lack of robust evidence to inform the choice of treatment.
A Cochrane systematic review12 considered a range of interventions (including exercises, foot orthoses, corticosteroid injections, ESWT, laser therapy and therapeutic ultrasound) for PHP, but was not able to pool the available data, found inconclusive evidence for the effectiveness of treatments and overall, found limited evidence to inform clinical practice. Since the publication of this review, a number of additional randomised controlled trials (RCTs) have been conducted, of which the evidence has yet to be synthesised. A recent review13 of conservative treatments for PHP included many interventions (eg, laser therapy, orthoses, pulsed radiofrequency, dry-needling), which are not commonly used for managing PHP, and analyses were limited by lack of power (two to three studies, mostly small sample sizes) except for the ESWT versus placebo comparison. Also, other previous systematic reviews10 12 14–16 have focused mostly on pairwise comparisons of two or three treatment options.
Day-to-day clinical decision making, however, often involves consideration of the ‘most effective’ among available treatment options for PHP. Network meta-analysis (NMA) as a novel synthesis of evidence allows for simultaneous inferences regarding clinical effectiveness of all available treatment options, by drawing together evidence from direct and indirect comparisons of multiple treatments.17Compared with traditional pairwise comparisons, NMA has the potential to increase the precision of the estimates of effects. Also, NMA enables a ranking of the different treatments relative to each other and aids clinical/shared decision making for clinicians and patients who may desire to know the ‘best treatment’ on average.17
There is a need therefore, to undertake a comprehensive, up-to-date systematic review of the comparative effectiveness of treatment options for PHP. Using an NMA, this study aimed to evaluate and compare the most common conservative treatment options for the management of PHP.
The specific objectives of this study were to:
determine the comparative effectiveness of treatments for relieving pain and improving function in patients with PHP;
identify gaps in the available evidence, as well as identify promising treatments that require investigation in future RCTs.
Methods
Protocol/protocol registration
This review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension statement for systematic reviews incorporating network meta-analyses for healthcare.18 An a priori protocol was established for this review and registered with the international prospective register of systematic reviews, PROSPERO number CRD42016046963 (http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42016046963).
Patient involvement
Patient involvement was central to the development of the research question. Within an advisory workshop which included participants who currently have or have experienced PHP (n=6) and clinicians (n=12; physiotherapists and podiatrists) involved in the management of foot pain, patients discussed their experiences of PHP and their concerns about the need to determine effective treatment options for relieving symptoms and improving function (ie, pain-free walking).
Study eligibility
We evaluated each identified RCT against the following predetermined selection criteria:
Study population: adults, aged 18 years and older with PHP (including plantar fasciitis, plantar fasciopathy, plantar fasciosis) as diagnosed by clinical examination and/or diagnostic imaging.
Interventions: the review focused on four therapeutic interventions (ie, exercise therapy, corticosteroid injections, non-steroidal anti-inflammatory drugs (NSAIDs) and orthoses) that are commonly used in the management of PHP in the UK19 and an additional treatment (ie, ESWT), which is commonly reported in the literature.
Due to an envisaged lack of suitable data on dosage and procedural variations of treatment options, this systematic review and NMA focused primarily on comparisons of the specified core therapeutic interventions (exercise therapy, corticosteroid injections, orthoses, NSAIDs and ESWT).
Comparator: direct comparisons between any of the five core therapeutic interventions (ie, exercise therapy, corticosteroid injections, NSAIDs, orthoses and ESWT) or comparisons with usual care/placebo/sham for PHP in any healthcare setting (community, primary healthcare or secondary healthcare), and without restrictions regarding duration, frequency or intensity of treatment. Studies only comparing different procedural techniques of the same intervention (eg, focal vs radial shockwave) were excluded.
Outcome measure: the primary outcomes for this review were pain and functional disability. In order to be eligible for inclusion, assessment of pain and/or functional disability was required, studies with <24 hours follow-up were excluded. Pain measures were placed in a hierarchy as follows: first step pain, pain in the morning, pain on activity (eg, walking), overall pain (or other measures of pain). This hierarchy was used to analyse the most clinically relevant data when multiple pain outcomes were reported in an RCT.
Information sources and search strategy
A comprehensive search strategy was developed in collaboration with an information specialist, with input from clinicians and academics in the review team. Eight electronic databases (Medline, EMBASE, CINAHL, AMED, PEDro, Cochrane Database of Systematic Reviews Cochrane Controlled Clinical Trials (CENTRAL), Web of Science and WHO International Clinical Trials Registry Platform) were searched from their inception until January 2018 (see online supplementary appendix 1 for full search strategies). No language restrictions were applied. The bibliographies of relevant review articles and selected articles were examined for additional potentially relevant trials.
Supplementary file 1
Study selection
In pairs, reviewers (OB, AL, CL, LSC, MJT, DvdW, ER) independently evaluated the eligibility of identified trials. At each stage of titles, abstracts and full-text selection, discrepancies were resolved through discussion between pairs of reviewers or via consensus in review team meetings.
Risk of bias assessment
The Cochrane Collaboration’s Risk of Bias tool20 was used to assess the quality of included trials. Trials were graded (unclear, high or low risk of bias) based on: (i) sequence generation, (ii) allocation concealment, (iii) blinding of personnel, (iv) blinding of outcome assessor, (v) incomplete outcome data, (vi) selective outcome reporting and (vii) other bias. For each study, risk of bias items was judged as unclear when there was either insufficient information to judge as (low/high risk) or there was no related information regarding the risk of bias item in the report (further details on risk of bias assessment are presented in online supplementary appendix 1).
Data extraction
Using a customised, pretested and piloted data extraction form, risk of bias and data extraction for each included trial were performed by pairs of reviewers. Differences in quality appraisal and extracted data were resolved through discussion between pairs of reviewers and where appropriate, the opinion of other members of the review team. For each included trial, details were extracted on: design, sample size, population characteristics (eg, age, diagnosis, duration of heel pain, interventions (professional delivering intervention, dose, duration and number of sessions) and outcome assessment (type of outcome measure, length of follow-up and outcome measurements)). Studies that provided a point estimate of the outcome together with a measure of variability (eg, a mean and SD), were taken forward for analysis. Where only sample size, median, range and/or IQR was given, methodology from Wan et al 21 was used to calculate the sample mean and SD. In instances of missing or incomplete data (eg, lack of measures of variability for follow-up data), additional information was requested and obtained (where possible) through contacting primary study authors.
Data synthesis and analysis
All analyses were performed using STATA V.15.1 (StataCorp, Texas, USA), under a frequentist approach, with restricted maximum likelihood used to estimate parameters. Prior to analyses, extracted data were further checked independently for completion and accuracy by the study statistician while profiling a database for the analyses. Furthermore, in order to define the treatment nodes for the network, two reviewers (HBM and ER), a podiatrist and rheumatologist, independently reviewed and classified the therapeutic interventions following a consensus process. As the objective of this systematic review was to compare different treatment options, and not to investigate the influence of dosage or intensity of interventions, the specified core therapeutic interventions (exercise therapy, corticosteroid injections, orthoses, NSAIDs, and ESWT), and usual care/placebo/sham, were allocated to six distinct nodes. Furthermore, studies involving combination(s) of any of the specified core treatments were used in our analyses in addition to the six nodes as treatment nodes with combination treatments. For example, where trial arms have involved a combination of exercise therapy and a corticosteroid injection as an intervention, corticosteroid injection+exercise was classed as a distinct treatment node. Also, where RCTs included more than one arm with the same type of treatment, the data were pooled together (eg, for a three-armed trial22 involving a prefabricated orthoses arm, and two custom orthoses arms (differentiated by a rigid and soft material), an average of the mean outcomes and SD was taken from the custom orthoses arms and a sum taken from the arm sample sizes, in order to create a single pooled orthoses arm).
In order to obtain direct treatment effect estimates (with a 95% CI) for each included comparison, pairwise meta-analyses were performed. Direct and indirect estimates of effects were then analysed together in an NMA.
Network coherence (consistency and heterogeneity)
The important assumption underlying an NMA is that of network consistency, that is, true treatment effects are on average the same, regardless of whether they are estimated from direct or indirect evidence. This was assessed in three ways: (i) using a global Wald test (with high p values favouring consistency)23; (ii) using a node-splitting technique, which judges the consistency of direct and indirect estimates separately for each treatment comparison (with high p values favouring consistency)24 and (iii) graphically (as a crude test), by inspection of forest plots comparing direct and pooled NMA results. Furthermore, the choice of a random or fixed effects model for each analysis was based on the magnitude of τ2 (ie, the common between-study variance across all treatment comparisons). A structured between-studies variance-covariance matrix was used, which assumes that all treatment comparisons have a common heterogeneity variance.
Primary outcomes of pain and function
Primary outcomes of pain and function were classified as: (i) short term (1 to ≤6 weeks post-treatment), (ii) medium term (6 to ≤12 weeks post-treatment) or (iii) long term (>12 weeks post-treatment). For short-term and medium-term outcomes, the latest outcome data within each time category was used for analysis. For example, if a study reported 3-week and 6-week pain outcomes, only the 6-week data were used. However, because the long-term category has no upper bound, a different approach was taken to reduce potential heterogeneity in results; we evaluated the spread of long-term outcomes and selected the most prevalent time point, and only retained data matching this time point for analysis. A total of six NMAs were possible (pain or function outcomes analysed separately for each time category), and a network plot was used to graphically present the direct evidence base and assess connectedness of each network.
Assessing comparative effectiveness of treatments
The principal summary measure used for pain and function outcomes was the standardised mean difference (SMD). SMDs are advantageous in homogenising outcomes from different scales and instruments onto a common scale. The direction of outcome scales in the raw data were reversed where appropriate (by multiplying values by −1), to ensure all outcomes were interpreted with lower values indicative of improvements in pain or functional disability. Estimates of effects (SMDs) were interpreted according to Cohen’s rule of thumb, with values of 0.2, 0.5 and 0.8 indicative of small, moderate and large effects, respectively.25 Direct pairwise (where available) and pooled NMA estimates, along with 95% CIs, are reported for all treatment comparisons. SMDs with 95% CIs that did not include the null value (of SMD=0, ie, no difference in comparative treatment effect), were classed as statistically significant.
Ranking of treatments
To further assess the comparative effectiveness of treatments, the ranking probability distributions of each treatment were generated from a simulation of 1000 replications. We used mean rank, surface under cumulative ranking curve (SUCRA) values and cumulative ranking plots. These statistics rank treatments according to their ability to generate the largest treatment effects in each simulation, and are averaged over the 1000 replications.
Sensitivity analysis
To assess the robustness of the findings for pain and functional outcomes, sensitivity analysis based on risk of bias was planned but not performed. This was due to most studies showing similar (unclear) risks of bias. Sensitivity analysis by the removal of studies with unclear risk led to insufficient data to support the network.
Results
Characteristics of included studies
The literature search yielded 1400 unique citations, of which 263 full-text articles were selected for full review. The study flow chart is presented in figure 1. Of the 263 full-text articles, 59 met the inclusion criteria and were subjected to quality assessment and data extraction. A further 28 articles could not be included in the NMA due to: being duplicate reports of the same RCT (n=1); examining dose regimen/technique comparisons of the same intervention (n=9); examining a similar but different treatment to commonly used interventions for PHP, that is, intracorporeal pneumatic shock therapy (n=1) and data/reporting problems where authors could not be contacted or failed to respond to queries after repeated attempts over a 3-month period (n=17). Summary of findings and the characteristics of eligible studies that could not be incorporated into the meta-analysis are presented in online supplementary appendix 2,tables 1 and 2.
Supplementary file 2

Study flow chart.
Comparative effectiveness results for pain outcome analyses, for each of (A) short-term outcomes, (B) medium-term outcomes and (C) long-term outcomes
Network meta-analysis treatment ranking results for pain outcome analyses, for each of short-term outcomes, medium-term outcomes and long-term outcomes
Thirty-one RCTs involving 2450 participants across 10 different (combinations of) interventions (ESWT, ESWT+exercise, ESWT+orthoses, exercise, NSAID injection+exercise, oral NSAIDs, orthoses, corticosteroid injection, corticosteroid injection+exercise and placebo/sham) provided sufficient data for inclusion in the NMA. (online supplementary appendix 1, table 1) presents the characteristics of the included RCTs. RCTs were published between 1999 and 2017. The maximum length of follow-up ranged from 4 weeks to 104 weeks. Most RCTs were from Europe (n=8), followed by Asia (n=6) and Australia (n=5). RCTs recruited participants mostly from primary care sources and outpatient departments of hospitals and rehabilitation centres and investigated a combination of participants with duration of PHP symptoms ranging from 10 to 287 weeks.
Risk of bias in the evidence base
The risk of bias assessment for the 31 included trials is presented in figure 2A and B. All included studies were RCTs; however, a significant proportion (35%) did not adequately report how randomisation was performed. High risk of bias was considered present most frequently (in 26% of trials) in relation to lack of blinding of participants and personnel. Many of the trial outcomes were patient reported but outcome assessment procedures were reported as blinded in 45% of the trials. The reporting of most of the trials did not provide sufficient information to accurately assess concealment of treatment allocation, thus generating a large proportion of ‘unclear’ responses (61% of trials). Overall, 1422 26–38 of the 31 trials were considered to be of low quality with fewer than 50% of risk of bias items (ie, ≤3/7) classed as low risk.

(A) Risk of bias for all individual studies (n=31) included in the analysis. (B) Summary of risk of bias across all (n=31) studies included in the analysis. + (green circle), low risk of bias; ? (amber circle), unclear risk of bias; - (red circle), high risk of bias.
Network coherence (consistency and heterogeneity)
NMA was possible for all (six) connected networks of evidence, which investigated pain and function outcomes separately, with follow-ups at: (i) short term, (ii) medium term and (iii) long term. There were no signs of the consistency assumption being violated for any network (where applicable, ie, only considering closed-loop networks). Firstly, the global Wald tests for inconsistency were not significant (p=0.822, 0.971, and 0.925 for short term pain, medium term pain, and short term function, respectively). Second, no statistically significant difference was observed between direct and indirect estimates when assessed separately for each treatment comparison through a node-splitting technique (all p values were >0.05). Third, the 95% CIs of the network and pairwise meta-analysis summary results overlapped for all three closed-loop networks (online supplementary figure 1S). The heterogeneity term, τ2, was ‘moderate’ to ‘large’ in magnitude (as classed by Cohen’s rule of thumb25) for all of the networks except long-term function (online supplementary appendix 1, table 2). Hence, random effects analyses were used for all but the long-term function network (whereby fixed effects analyses were used). Full raw outcome data used (including outcome scales) are provided in supplementary appendix 1, table 3.
Supplementary file 3
Comparative effectiveness results for function outcome analyses, for each of (A) short-term outcomes, (B) medium-term outcomes and (C) long-term outcomes
Treatments for PHP: pain outcomes
Evidence base: there were 22 studies22 26–28 30 31 33 37 39–53 (21x two-arm, 1×3 arm) in the short-term pain evidence base, with a similar sized network of 23 studies27–32 34 37 39–42 44–47 49–56 (22x two-arm, 1×3 arm) in the medium term pain, and a smaller network of 10 studies29 34–38 40 44 45 49 55 (all two-arm) in the long-term pain; as presented in figure 3. Eight different treatment nodes were used in the short-term analysis, with these same treatments and the addition of a ninth (ESWT+exercise) used in the medium term, and eight treatments in the long term. Placebo/sham-ESWT comparisons were most prevalent across all pain outcome networks (n=6 studies in short term and medium term, n=4 in long term), and the number of participants ranged from 31 (NSAID injection+exercise in long term) to 574 (ESWT in medium term). Direct evidence was available for 12 out of a possible 28 pairwise comparisons in the short term, 12/36 in the medium term and 7/28 in the long term. Outcome follow-up ranged from 2 to 6 weeks in the short term (n=1744 total participants used), 2–3 months in the medium term (n=2018) and was fixed at 12 months for the long term (n=778).

Network graph of included studies for pain outcomes, with thickness of lines and size of circles proportional to number of studies and number of participants, respectively. (A) Short-term evidence, (B) medium-term evidence and (C) long-term evidence. Black text represents number of studies, and blue text number of participants. ESWT, extracorporeal shockwave therapy; ESWT+Exe, extracorporeal shockwave therapy combined with exercise; ESWT+Orthoses, extracorporeal shockwave therapy combined with orthoses; Exe, exercise; NSAID Inj+Exe, oral non-steroidal anti-inflammatory drug combined with exercise; Oral NSAID, oral non-steroidal anti-inflammatory drug; Orthoses, prefabricated or customised foot orthoses; Placebo, usual care/placebo; Steroid Inj, corticosteroid injection; Steroid Inj+Exe, corticosteroid injection combined with exercise.
Comparative effectiveness of treatments
Full pairwise and network analyses results for pain are presented in table 1. Across both pairwise and network analyses, corticosteroid injection demonstrated a statistically significant larger reduction in short-term pain over oral NSAIDs (SMD 2.60, 95% CI (0.81 to 4.39)); and corticosteroid injection combined with exercise showed a statistically significant larger reduction in pain compared with exercise alone (SMD 1.20, 95% CI (0.14 to 2.26)). Compared with other treatments, oral NSAIDs were most often associated with the least statistically significantly reductions in short-term pain (by SMD 2.25, 95% CI (0.18 to 4.33) compared with orthoses, and by SMD 2.61, 95% CI (0.13 to 5.09) compared with corticosteroid injection combined with exercise).
Most treatments were not statistically significantly superior to one another and underlying estimates of effect presented with very wide CIs. For instance, the network comparison of ESWT combined with orthoses showed a non-statistically significant reduction in medium-term pain compared with ESWT in combination with exercise (SMD=2.36, 95% CI (−2.17 to 6.89)).
With the highest SUCRA values of 79.5 and 74.4, and the best mean ranks of 2.4 and 2.8, corticosteroid injection alone and in combination with exercise ranked among the three most effective treatments for short-term pain, 82.7% and 65.7% of the time, respectively (figure 4A, table 2). In contrast, oral NSAIDs (which ranked among the three least effective treatments 97.3% of the time), exercise alone, and placebo/sham interventions demonstrated the least comparative effectiveness for pain relief in the short term. General trends from the NMA and direct comparisons for medium-term pain indicated that ESWT combined with orthoses may be more effective than other treatments (highest SUCRA value of 80.3; figure 4B, table 2). Oral NSAIDs, exercise and exercise combined with ESWT were least likely to have beneficial effects for the treatment of pain due to PHP in the medium term compared with other treatments. While placebo and orthoses appeared least likely to be beneficial for long-term pain (85.7% and 81.0% of the time ranking among three least effective treatments, respectively; figure 4C, table 2), superiority of one treatment over another for the remaining six treatments was less clear, with most of these treatments having similar rankings (average SUCRA of 60.8).

Cumulative ranking plots to show comparative effectiveness of treatments from a pain outcome network meta-analysis, for each of (A) short-term outcomes, (B) medium-term outcomes and (C) long-term outcomes. Results based on a simulation of 1000 replications. ESWT, extracorporeal shockwave therapy; ESWT+Exe, extracorporeal shockwave therapy combined with exercise; ESWT+Orthoses, extracorporeal shockwave therapy combined with orthoses; Exe, exercise; NSAID Inj+Exe, oral non-steroidal anti-inflammatory drug combined with exercise; Oral NSAID, oral non-steroidal anti-inflammatory drug; Orthoses, prefabricated or customised foot orthoses; Placebo, usual care/placebo; Steroid Inj, corticosteroid injection; Steroid Inj+Exe, corticosteroid injection combined with exercise.
Treatments for PHP: function outcomes
Evidence base: for function outcomes, there were fewer RCTs available for analysis compared with the pain (14 studies were in the network for short-term function,26 30 33 37 39 41–46 48 49 52 53 11 for medium-term function,30 37 41 42 44–46 49 52 53 55 and 5 for long-term function35 37 44 45 49 55; all two-armed), as shown in figure 5. Similar treatment nodes were used across the networks, with the same six used in short-term and medium-term function analyses (ESWT, ESWT+exercise, orthoses, placebo, corticosteroid injection with and without exercise), while the long-term analysis did not contain corticosteroid without exercise. Placebo/sham-ESWT comparisons were most common in the short term (n=4 studies) and long term (n=2 studies), while ESWT/corticosteroid injection and corticosteroid injection with exercise/exercise alone comparisons (n=3 studies) were joint most common for medium term. The number of participants ranged from 20 (exercise in long term) to 226 (ESWT in short term), and direct evidence was available for 7 out of a possible 15, 5/15 and 4/10 comparisons, in the short term, medium term and long term, respectively. Outcome follow-up ranged from 2 to 6 weeks in the short term (n=868 total participants used), 2.5–3 months in the medium term (n=811) and was fixed at 12 months for the long term (n=312).
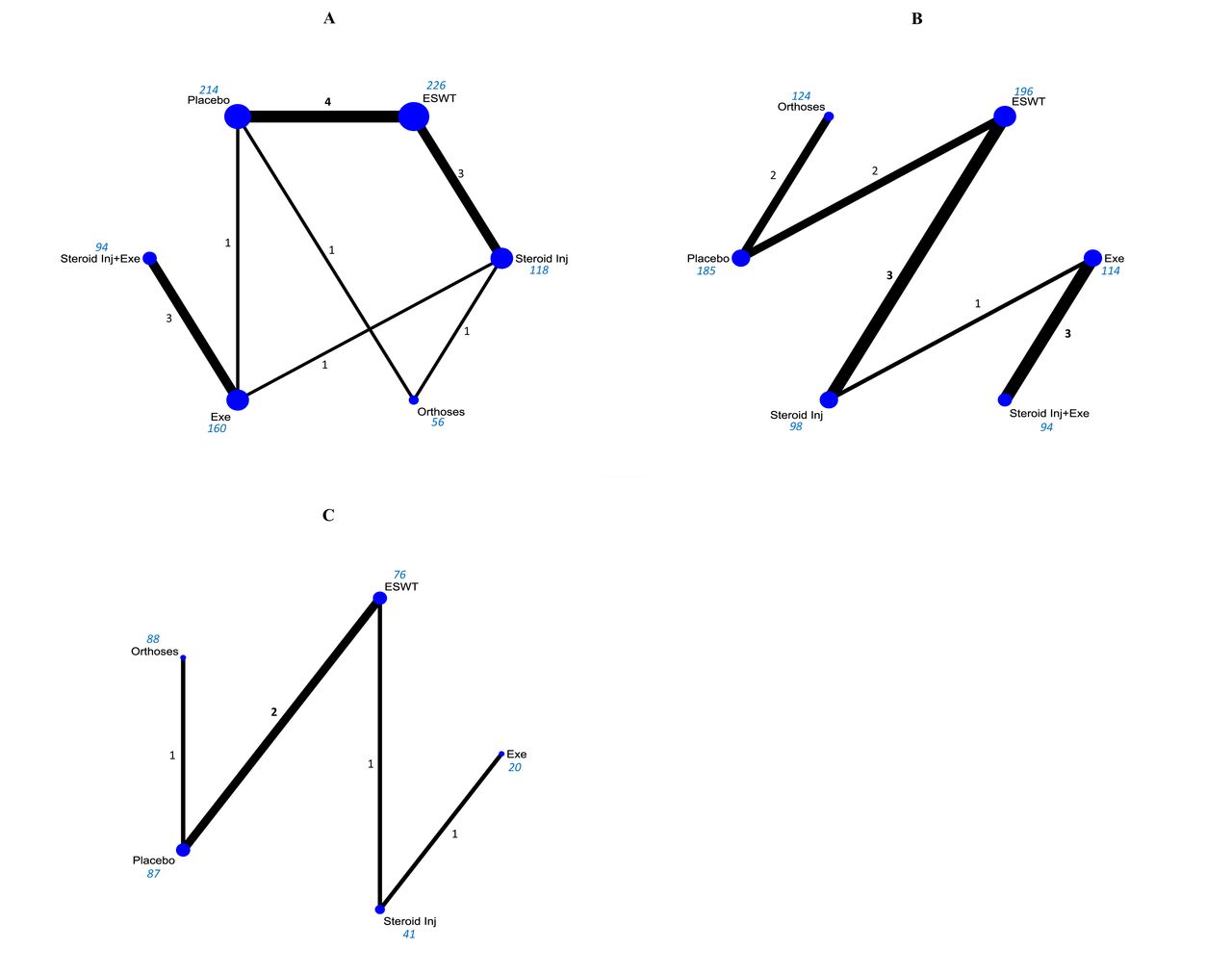
Network graph of included studies for function outcomes, with thickness of lines and size of circles proportional to number of studies and number of participants, respectively. (A) Short-term evidence, (B) medium-term evidence and C) long-term evidence. Black text represents number of studies, and blue text number of participants. ESWT, extracorporeal shockwave therapy; Exe, exercise; Orthoses, prefabricated or customised foot orthoses; Placebo, usual care/placebo; Steroid Inj, corticosteroid injection; Steroid Inj+Exe, corticosteroid injection combined with exercise.
Comparative effectiveness of treatments
The comparative effectiveness of treatments (both pairwise and network meta-analyses) on function outcomes are presented in table 3. As with pain outcomes, most treatments were not significantly better than one another in the short term, medium term and long term; CIs were often wide. Placebo/sham interventions were comparatively worse at improving functional ability than other treatments, for example, NMA showed statistically significant reductions in long-term functional ability (by SMD 0.93, 95% CI (0.23 to 1.63) compared with corticosteroid injection, by SMD 1.09, 95% CI (0.15 to 2.03) compared with exercise and by SMD 0.95, 95% CI (0.50 to 1.40) compared with ESWT).
In agreement with the analyses on pain outcome treatment effects, placebo/sham interventions ranked least likely to improve function for patients with PHP (SUCRA values: 16.9, 28.1 and 7.3, in the short term, medium term and long term, respectively; figure 6 and table 4), followed by orthoses (SUCRA: 31.8, 42.4 and 19.4, in the short term, medium term and long term, respectively), and exercise alone (SUCRA: 32.2 and 29.9 in the short term and medium term, respectively). However, exercise appeared most likely to improve functional ability for long-term function (SUCRA: 82.1); while corticosteroid with and without exercise, and ESWT consistently ranked in the top three treatments most likely to improve functional ability.
Network meta-analysis treatment ranking results for function outcome analyses, for each of short-term outcomes, medium-term outcomes and long-term outcomes

Cumulative ranking plots to show comparative effectiveness of treatments from a function outcome network meta-analysis, for each of (A) short-term outcomes, (B) medium-term outcomes and (C) long-term outcomes. Results based on a simulation of 1000 replications. ESWT, extracorporeal shockwave therapy; Exe, exercise; Orthoses, prefabricated or customised foot orthoses; Placebo, usual care/placebo; Steroid Inj, corticosteroid injection; Steroid Inj+Exe,corticosteroid injection combined with exercise.
Comparison of effectiveness of treatments across pain and function outcomes
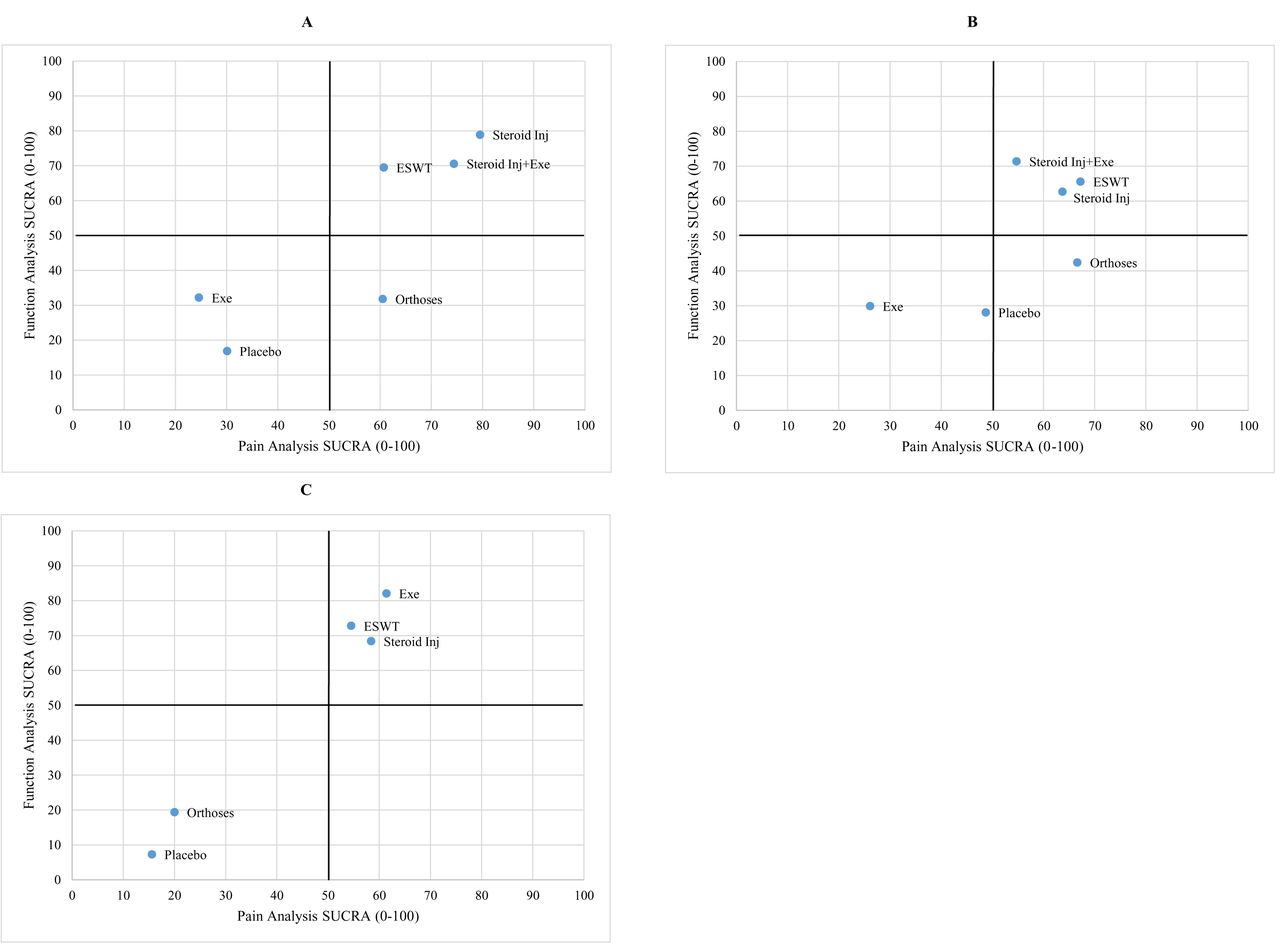
Corticosteroid injection with and without exercise, and ESWT interventions appear most likely to have beneficial effects for both pain and function outcomes over all time periods (figure 7). In contrast, placebo/sham interventions appear least likely to improve either pain or function outcomes across all time periods, while exercise appears to have a non-beneficial effect for short term and medium term, but a beneficial effect for long-term pain and function.
{kind=link}
{kind=link}
![[SP3.jpg]](https://bjsm.bmj.com/content/bjsports/53/3/182/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter plots to show comparative effectiveness of treatments*, through surface under cumulative ranking curve (SUCRA) values (0–100), for pain (X-axis) and function (Y-axis) outcomes. Shown separately for each of: A) short-term outcomes, (B) medium-term outcomes and C) long-term outcomes. Higher SUCRAs indicate better performing treatments. Horizontal and vertical lines added at SUCRA=50 values as a crude guide to identifying comparatively better/worse performing treatments for pain/function. ESWT, extracorporeal shockwave therapy; Exe, exercise; Orthoses, prefabricated or customised foot orthoses; Placebo, usual care/placebo; Steroid Inj, corticosteroid injection; Steroid Inj+Exe, corticosteroid injection combined with exercise. *SUCRA results for four treatments are completely omitted, as data were only available for pain, but not function outcomes. ESWT+Exe, extracorporeal shockwave therapy combined with exercise; ESWT+Orthoses, extracorporeal shockwave therapy combined with orthoses; NSAID Inj+Exe, oral non-steroidal anti-inflammatory drug combined with exercise; Oral NSAID, oral non-steroidal anti-inflammatory drug.
Summary of findings for RCTs without suitable data for NMA
Findings from 17 RCTs of 7 different comparisons and/or treatment combinations, including ESWT versus placebo/sham (n=11), exercise versus ESWT (n=1) and custom versus prefabricated orthosis/placebo/sham (n=3), for which suitable data could not be obtained are presented in online supplementary appendix 2, table 1. For the comparison between ESWT and placebo/sham, with an unclear to high risk of bias across trials, ESWT is reported to be significantly more effective than sham/placebo for reducing pain in two out of three trials in the short term, and four out of seven in the medium term. There was no evidence for the effect of ESWT on function in the short term but two trials reported reduction in functional disability in the medium term. However, there was uncertainty in evidence across trials and time points as shown by very large CIs and inconsistency of the magnitude of effects. For both pain and function outcomes and across time points (short term, medium term and long term), trials found no difference between custom and prefabricated orthoses. All other treatment comparisons/combinations contained only one trial with mostly small sample sizes.
Discussion
Available evidence does not suggest that any of the commonly used treatments for the management of PHP are significantly better than any other, although the results of this NMA show that corticosteroid injections alone or in combination with exercise are effective treatments for reducing pain and improving function in the short term. However, the magnitude of estimate of effect varied widely across trials with large CIs. Furthermore, the overall effect of corticosteroid injections on PHP is modest, and the potential for adverse effects15 57 such as postinjection steroid-induced increase in pain, fat pad atrophy, nerve injury and rupture of the plantar fascia require careful consideration. There was a greater amount of evidence for ESWT, but we found no evidence that this treatment confers more beneficial effects (compared with the other treatments in this study) for reducing pain and improving function among patients with PHP.
In the network meta-analyses of both pain and function, placebo/sham interventions and NSAIDs were generally shown to be the least effective treatment options. Considering PHP has long been considered to be a self-limiting pain condition, our findings indicate that first-line management recommendations of PHP with over the counter pain medications, NSAIDs and a watchful waiting approach may be suboptimal. Previous literature has suggested that delaying treatment may worsen prognosis, and potentially create a need for further healthcare use.57 The findings of this present study support the notion that access to treatments without a period of watchful waiting may be beneficial.
As the current NMA is the first to examine the comparative effectiveness of the most common treatments for PHP, it is difficult to directly compare the findings of the present study with those of previous NMAs which examined a limited number of treatments,58 or compared dosage/technique for specific treatment options.59 Previous reviews collectively indicate that exercise and foot orthoses are promising interventions for short-term and medium-term improvements in pain and function.60 61 In this review, exercise as a stand-alone treatment was not found to consistently confer beneficial effects in reducing pain and improving function for patients with PHP in the short term, but a beneficial effect was found for long-term pain and function. There is a lack of evidence regarding the most effective exercise dose or delivery method. In this systematic review, included RCTs reported varying exercise therapy protocols, dose and regime. As with the review by Almubarak and Foster,60 exercise as a treatment in this review included stretching and strengthening exercise trials; treatment comparisons including exercise in combination with other treatments such as corticosteroid injection mostly had calf stretching as the ‘exercise’ component. These exercises were mostly home based (apart from the first session that may be supervised) and were not individualised or progressed. Within the networks, foot orthoses (prefabricated or custom), were not found to be effective as a stand-alone treatment for PHP, but were mostly effective in combination with ESWT. Our findings agree with those of recent systematic reviews showing that foot orthoses are better than sham/placebo and may be effective for reducing pain in the medium term.13 61
Study strengths and limitations
In this study, direct and indirect evidence has been combined in order to assess comparative effectiveness of interventions that have not yet (or only minimally) been directly compared in robust high-quality trials. There was agreement between the direct and indirect evidence which achieved consistency for specified treatments; however, tests for inconsistency are likely to be underpowered, due to lack of data, as evidenced by wide 95% CIs for SMDs. As an alternative to frequentist methods which was used in the current NMA, a Bayesian three-level hierarchical NMA model may be employed. This approach has been shown to increase precision of effect estimates in meta-analysis of few trials, or a large number of treatment options which can be further subdivided.62 However, this approach was deemed to be out of scope for our NMA which mainly focusses on comparisons across different treatments. Future NMAs, especially those incorporating dose comparisons and procedural variations of the same treatment options, would benefit from Bayesian analysis.
The current study is not without limitations and must be interpreted with caution. First is the inclusion of only the most common treatments as opposed to all available treatments for the management of PHP. This decision was made in order to inform choice of treatment in primary care settings where PHP patients are mostly seen, and to evaluate interventions that are widely available and accessible to patients. Furthermore, networks would likely be disconnected when including a large number of treatments evaluated in only a small number of trials. The sparsity of data did not allow for a statistical exploration of publication bias; however, we conducted a comprehensive search of published and unpublished literature as well as employed a paired screening process to ensure all available evidence was identified. However, the findings of this review are still likely to be influenced by the small number of trials (mostly with small sample sizes) available to support direct and indirect comparisons in the network. For instance, many nodes in the networks (figure 3 and figure 5), were connected by only a single trial and (for some treatments) with few participants.
The loss of data associated with absence of suitable data for analysis was a challenge in this review. Related first, and more importantly, to the disparate reporting of data in scientific reports in this field, a lot of data from otherwise eligible (but excluded trials) could not be analysed mostly due to lack of reporting of treatment outcomes with a mean as well as a measure of variability. Despite concerted efforts to request this additional data from trial authors, the inability of our review to incorporate such data into evidence synthesises inadvertently led to notable research waste. As a minimum, for all trials in this field, reporting an average and a measure of variability (eg, a mean and a SD) per trial arm for each follow-up period should be required. Furthermore, to avoid substantial heterogeneity, data from some trials which used a very different approach to measuring outcomes could not be combined in the network. However, this problem could be overcome through the development of and adherence to an agreed standardised set of core outcomes to be used in trials in this field. In order to minimise the loss of potentially useful evidence, details of all otherwise eligible trials were extracted with a narrative summary of findings presented (online supplementary appendix 2, table 1). Generally, the results from these trials were found to be in agreement with the evidence presented in the NMA.
Implications for clinical practice, policy and future research
Within the NMA, control treatments (including placebo/sham interventions, watchful waiting approach, over-the-counter pain medications)` and NSAIDs generally showed lack of beneficial effects for patients with PHP. For primary care first-point-of-contact decision-making purposes, our findings suggest that access to treatments may be beneficial for patients with PHP.
However, findings from this review must be interpreted with caution due to limitations in quality of the evidence underpinning the analyses. Of particular concern are predominantly small sample sizes, low quality reporting of aspects of study design (especially concealment of treatment allocation) and variability in outcome measures across included studies (online supplementary appendix 1, table 3). Furthermore, this review cannot comment on evidence for comparative effectiveness of treatment options where the influence of duration of symptoms prior to treatment may be of concern. This is due to the wide variability in the range of duration of symptoms at recruitment across studies included in this review and the fact that most trials did not report data regarding the duration of symptoms per trial arm. Future research involving patients with PHP should therefore focus on the design of large trials with head-to-head comparisons of active treatments, long-term follow-up and higher reporting standards. Furthermore, careful consideration of trials investigating the same treatment comparisons (especially for the most promising interventions in the short term and long term) is an important next step. This will enable exploration of the optimal mode of delivery, dosage and intensity of treatments required for successful management of PHP.
Conclusion
This is the first NMA to examine the comparative effectiveness of commonly used treatments for PHP and brings together available evidence in order to aid evidence-informed clinical decisions in the management of PHP. For pain and functional outcomes, most treatments were not significantly better than others in the short term, medium term and long term. The comparative effectiveness of commonly used treatments (ie, exercise therapy, corticosteroid injections, orthoses, NSAIDs and ESWT) is limited by large variation in magnitude and imprecision of effect estimates. Findings indicate the need for large, multicentre trials directly comparing commonly used treatments for the management of PHP.
What is already known on this topic?
Existing pairwise meta-analyses are limited to comparisons of two or three treatment options for plantar heel pain.
Clinical decision making regarding the best treatment option is often difficult.
What are the new findings?
For the management of plantar heel pain, available evidence does not support the superiority of any of the commonly available treatments over another.
However, corticosteroid injections, alone or in combination with exercise, and ESWT appear more likely to be effective for relieving plantar heel pain and improving function compared with other treatments in the short term, medium term and long term.
Control treatments (which include over-the-counter pain medications and watchful waiting, as well as placebo interventions) generally show less beneficial effects than other treatments for patients with plantar heel pain.
The review highlights the need for large high-quality randomised controlled trials of the commonly used interventions for the management of plantar heel pain.
Acknowledgments
The authors would like to thank Dr Nadia Corp for her help with the search strategy.
References
Footnotes
Contributors Investigation: OOB, MT, CL, LSC, AL, HBM, ER, DvdW. Formal analysis: OOB, AL. Writing—original draft: OOB, AL. Writing—review and editing: OOB, AL, CL, LSC, MT, HBM, ER, DvdW. Supervision: DvdW, ER. Project administration: OOB, DvdW.
Funding AL is supported by a National Institute for Health Research (NIHR) Research Methods Fellowship. MJT has received funding through a NIHR School for Primary Care Research Launching Fellowship and is currently supported by a Health Education England (HEE)/NIHR Integrated Clinical Academic Programme Clinical Lectureship (ICA-CL-2016-02-014).
Disclaimer The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR, HEE or the Department of Health and Social Care.
Competing interests None daclared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.