Article Text

Abstract
Sport-related concussion (SRC) is a common injury in recreational and organised sport. Over the past 30 years, there has been significant progress in our scientific understanding of SRC, which in turn has driven the development of clinical guidelines for diagnosis, assessment and management of SRC. In addition to a growing need for knowledgeable healthcare professionals to provide evidence-based care for athletes with SRC, media attention and legislation have created awareness and, in some cases, fear about many issues and unknowns surrounding SRC. The American Medical Society for Sports Medicine (AMSSM) formed a writing group to review the existing literature on SRC, update its previous position statement, and to address current evidence and knowledge gaps regarding SRC. The absence of definitive outcomes-based data is challenging and requires relying on the best available evidence integrated with clinical experience and patient values. This statement reviews the definition, pathophysiology and epidemiology of SRC, the diagnosis and management of both acute and persistent concussion symptoms, the short-term and long-term risks of SRC and repetitive head impact exposure, SRC prevention strategies, and potential future directions for SRC research. The AMSSM is committed to best clinical practices, evidence-based research and educational initiatives that positively impact the health and safety of athletes.
- concussion
- athlete
- sport
Statistics from Altmetric.com
Background and purpose
The American Medical Society for Sports Medicine (AMSSM) represents over 3800 sports medicine physicians who have completed specialty training in sports medicine after a residency programme in family medicine, internal medicine, paediatrics, emergency medicine, or physical medicine and rehabilitation, many of whom have extensive expertise in concussion evaluation and management, including serving as sideline team physicians at all levels of sport. Sport-related concussion (SRC) is an important topic for sports medicine physicians and there is a rapidly expanding knowledge base in this area. SRC has become a focus of both public concern and media attention. The purpose of this statement is to provide a narrative review of the existing literature and best practices to assist healthcare providers with the evaluation and management of SRC, and to establish the level of evidence, current knowledge gaps and areas requiring additional research. The first AMSSM position statement on SRC was published in 2013 and this is an update to that statement.1
Writing group selection and process
The AMSSM Board of Directors appointed the chair (KGH) to assemble a writing group that was carefully selected to include a balanced panel of sports medicine physicians experienced in sideline and office evaluation and management of SRC, actively engaged in SRC research, and with demonstrated leadership in the area of SRC. Select subspecialty experts were invited to provide diverse viewpoints. Select members of the board, the publications committee and writing group were surveyed to determine topics of interest for the statement and generate an initial outline. Systematic reviews were used as primary literature sources when available. The writing group engaged in conference calls, review of the literature and written communication prior to an inperson meeting in Chicago, Illinois, on 9–10 February 2018. There were additional conference calls, emails and iterations of the outline and manuscript to produce the final document. This document uses the Strength of Recommendation Taxonomy to grade level of evidence2 (table 1).
Strength of Recommendation Taxonomy
Who should evaluate and manage SRC?
The clinical care, including assessment and management, of athletes with SRC is ideally performed by healthcare professionals with appropriate training and experience. Sports medicine physicians are uniquely trained to provide care along the continuum of SRC from the acute evaluation through return to learn and return to sport, and to manage both complications of SRC and coexisting medical issues. While the majority of SRCs resolve within 1–4 weeks, athletes with complicated or prolonged recovery may require a multidisciplinary team with specific expertise across the scope of concussion management. (C)
Definition of concussion
Concussion is defined as a traumatically induced transient disturbance of brain function that involves a complex pathophysiological process.1 Concussion is a subset of mild traumatic brain injury which is classified based on acute injury characteristics at the less severe end of the brain injury spectrum.1 The clinical signs and symptoms of concussion cannot be otherwise explained by drug, alcohol, medication use, or other injuries (such as cervical injuries or peripheral vestibular dysfunction) or other comorbidities (psychological or medical conditions).3 4
Pathophysiology
The pathophysiology of concussion is not completely understood but has been characterised as force delivered to the brain causing disruptive stretching of neuronal cell membranes and axons resulting in a complex cascade of ionic, metabolic and pathophysiological events.5 Current understanding of the pathophysiology of concussion is primarily based on animal models that have limitations when extrapolated to humans. It appears that stress applied to the neuron causes changes in intracellular ion concentrations, indiscriminate release of neurotransmitters, mitochondrial dysfunction leading to the production of reactive oxygen species, and increased utilisation of glucose to restore sodium and potassium balance.5 The increased glucose utilisation combined with the injury-related decrease in resting cerebral blood flow creates an energy mismatch.6 7 Inflammatory cell activation, axonal degeneration and altered plasticity may occur in the subacute and chronic stages of concussion. Animal and human studies support the concept of increased brain vulnerability following an initial injury to a second brain tissue insult that can result in worsening cellular metabolic changes and more significant deficits.8–10
Epidemiology
Concussion is common in organised scholastic and non-scholastic sport, non-traditional recreational activity (eg, extreme, individual), and routine activities of daily living. A recent report using data from emergency room visits, office visits and a high school injury surveillance system estimated 1.0–1.8 million SRCs per year in the 0–18 years age range and a subset of about 400 000 SRCs in high school athletes.11 While this estimate is likely accurate, determining actual sport-based or activity-based concussion rates is difficult.
Injury surveillance systems in the USA primarily study a small sample of organised college or high school sports to estimate concussion rates. Numbers are limited or not available for recreational or club sports or for activities such as bicycling, skiing, snowboarding, skateboarding, the fighting arts or for youth/early adolescent athletes. An estimate of risk requires a numerator (the number of concussions) and a denominator (the amount of time participating in the activity). Numerators may vary based on under-reporting or over-reporting of concussion or inaccurate diagnosis, while denominators are difficult to accurately track. Most current estimates use ‘athlete-exposures’ as the denominator, defined as an athlete participating in one practice or game; however, estimates of risk may change dramatically if actual hours of participation are tracked or if a seasonal or annual risk of concussion is determined. Seasonal or annual risk may be a more readily understood concept. It is estimated that over 50% of concussions in high school-aged youth are not related to organised sports and only 20% are related to organised school team sports.11 Between 2% and 15% of athletes participating in organised sports will suffer a concussion during one season12–29 (table 2).
Seasonal risk of concussion in sports
Diagnosis of concussion
The diagnosis of concussion is challenging and based on clinical assessment. Concussion diagnosis is complicated by a lack of validated, objective diagnostic tests, a reliance on self-reported symptoms, and confounding symptoms caused by other common conditions. Non-specific symptoms such as headaches, mood changes, ‘fogginess’, dizziness, visual changes, fatigue and neck pain are all associated with concussion but can also originate from other aetiologies. In addition, symptoms may be delayed in onset or initially unrecognised by the athlete. Concussion remains a clinical diagnosis made by carefully synthesising history and physical exam findings as the injury evolves. (C)
Preseason
Preparation for the care of athletes begins prior to any practice or competition with a preparticipation physical evaluation (PPE) and the development and practice of an emergency action plan.30 The PPE should include history of concussion or other traumatic brain injury (number, recovery course and time between injuries), as well as the presence of other premorbid/comorbid conditions, or modifiers, that may make the diagnosis or management of concussion more difficult, including a history of learning disorder, attention deficit disorder, motion sickness or sensitivity, mood disorders or a personal or family history of migraine headache disorder, and information on current medication use. (C)
Several organisations recommend baseline evaluation prior to sports participation to assist with diagnosis and return-to-play decisions in an athlete with a suspected concussion.3 31 32 Several factors require consideration before implementing any test into an evaluation programme for baseline or postinjury purposes. There is considerable normal variation in test performance with repeat testing in non-injured athletes23 33 34; some tests are associated with a cost, and in younger athletes with rapidly developing brain function both the ideal interval to repeat baseline testing and age-related differences in test performance are unknown. Common baseline evaluations include the battery of standard sideline assessment tests found in the Sports Concussion Assessment Tool Fifth Edition (SCAT5) and/or computerised proprietary neuropsychological tests such as CogSport, Automated Neuropsychological Assessment Metrics, Central Nervous System Vital Signs, or the Immediate Post-Concussion Assessment and Cognitive Testing. An initial baseline evaluation including a symptom checklist, cognitive evaluation and balance assessment has been considered ‘best practice’ for all athletes by the National Collegiate Athletic Association. However, repeat annual baseline testing after an initial baseline evaluation is no longer recommended for collegiate athletes.31 Baseline testing may be useful in some cases but is not necessary, required or an accepted standard of care for the appropriate management of SRC. (B)
Sideline assessment
Observation of athletes during practice and competition by medical personnel is valuable for potential concussion recognition and initial management. Reasons for immediate removal and prompt evaluation include loss of consciousness (LOC), impact seizure, tonic posturing, gross motor instability, confusion or amnesia. Any of these reported or observed signs should result in removal from practice or competition for at least the rest of the day. Concerns for more serious head injury including prolonged LOC, severe or worsening headache, repeated emesis, declining mental status, focal neurological deficit or suspicion of significant cervical spine injury should trigger activation of the emergency action plan. (C)
Along with directly observed signs of potential concussion, if video review demonstrates findings such as LOC, motor incoordination or balance problems, or having a blank or vacant look, the athlete should be immediately removed from participation for evaluation.35–37 A healthcare professional familiar with the athlete is best suited to detect subtle changes in the athlete’s personality or test performance that may suggest concussion. If a concussion is suspected but not diagnosed, removal from play and serial evaluations are recommended.38 Concussion assessment should be performed in a distraction-free environment with adequate time for examination and administration of concussion tests. If it is clear an athlete has an SRC, additional sideline testing can be discontinued. Sport-specific rules may not allow adequate time for evaluation, and modifying these rules remains an area for improvement within the governing bodies of some sports. (C)
When the sports medicine clinician becomes aware of a potential injury, the athlete is approached and a brief history of the event is obtained from the athlete and those who witnessed the event or athlete behaviour. How the athlete responds to the elements of orientation, memory, concentration and balance is evaluated, as well as speech patterns and how the athlete appears to be processing information. Cervical palpation and range of motion (ROM) are also typically performed to assess for other injury. If SRC is suspected, these preliminary evaluations are followed by a thorough and specific concussion assessment. (C)
The psychometric properties of sideline assessment tools need to be understood to accurately interpret the results.39 Knowledge of test reliability, or the stability of a test administered on more than one occasion, can assist in differentiating SRC changes from normal variation. The test–retest reliability of commonly used sideline concussion evaluation tests is below the generally accepted threshold for clinical utility (0.75–0.90).33 39 Many concussion tests have a learning effect that must be factored into analysis with repeated administration of the test. The sensitivity (ability of a test to correctly identify a condition) and specificity (ability of a test to correctly identify those without a condition) of many of the individual tests used to evaluate concussion are not ideal. The area under the curve of a receiver operator characteristic curve is another way to evaluate the usefulness of a test, with values greater than 0.9 considered excellent, 0.8 good, 0.7 fair, 0.6 poor and 0.5 failing. Table 3 outlines the psychometric properties and the number of subjects and concussions studied of commonly used sideline evaluation tools. There is evidence that combining tests of different functions to form a multimodal assessment increases sensitivity and specificity for diagnosis.22 33 The age of the athlete needs to be considered when using and evaluating testing tools. SRC is a heterogeneous injury which contributes to the varied sensitivity of screening tools, which are often domain-specific assessments. All tests should be interpreted in combination with relevant clinical information to arrive at the most accurate conclusion. (B)
Psychometric properties of sideline assessment tests*
Symptoms are the most sensitive indicator of concussion.23 40 The reliability of athlete-reported symptoms depends on accurate reporting, which may be affected by a lack of recognition of the signs and symptoms of concussion or conscious false reporting to avoid loss of playing time. An athlete experiencing any increase in symptoms after a suspected concussion should be held from play until further evaluation can confirm or exclude SRC. (B)
The SCAT541 and the Child SCAT542 are the evaluation tools recommended by the Concussion in Sport Group (CISG) for assessing a suspected concussion. These tests offer a standardised approach to sideline evaluation which incorporates multiple domains of function and are widely available at no cost. The SCAT5 comprised a brief neurological examination, a symptom checklist, a brief cognitive assessment (the Standardized Assessment of Concussion [SAC]) and a balance assessment (the modified-Balance Error Scoring System). The SAC in the SCAT5 offers optional 10-word lists for immediate and delayed memory and longer digit backwards sequencing to minimise the ceiling effect, which was a weakness of the SCAT3.43 There are currently no studies of the SCAT5 or Child SCAT5’s sensitivity and specificity for SRC to determine if these versions are improved over the earlier versions. (C)
The primary endpoint for sideline assessment is to determine the probability that an athlete has sustained a concussion. If the athlete is deemed unlikely to have had a concussion, continued participation should be safe. If the evaluation indicates a definite or probable concussion, the athlete should be removed from participation with no same-day return to play. SRC is an evolving injury and should be serially reassessed when suspected. (C)
Office/Subacute assessment
An office assessment should include a comprehensive history and neurological examination including details of injury mechanism, symptom trajectory, neurocognitive functioning, sleep/wake disturbance, ocular function, vestibular function, gait, balance and a cervical spine exam. The utility of sideline neurocognitive and balance assessments to identify concussion decreases as early as 3 days after injury.41 Symptom checklists can be useful to track symptom trajectory. To confirm the diagnosis of SRC, there should typically be a clear mechanism consistent with concussion; characteristic signs, symptoms and time course of concussion; and no other cause for the constellation of clinical findings. It is not unusual for symptoms, signs and testing to normalise by the time an office visit occurs,44 in which case the visit should focus on recommendations for safe return to school and sport. (C) If computerised neurocognitive tests were performed prior to injury, they are often repeated during this assessment period.
If an athlete has ongoing symptoms at the time of the first office visit, the visit should focus on excluding other pathologies and providing anticipatory guidance. Other pathologies like cervicogenic pain, headache/migraine disorder, mood disorders and peripheral vestibular conditions may either be the cause of symptoms or may represent previous pathology worsened or unmasked by concussion. A complete cervical spine evaluation, screenings for psychosocial or mental health disorders, and additional tests evaluating the vestibular and oculomotor system may be helpful in the office setting to determine the aetiology of symptoms. Vestibular symptoms occur in 67%–77% and ocular impairment occurs in approximately 45% of SRC.45 46 The Vestibular/Ocular Motor Screening (VOMS) tool offers a brief, standardised way to assess vestibular-ocular function that can be used in athletes older than 10 years of age.46 It is a no-cost evaluation of symptom provocation with smooth pursuits, saccades, the vestibular ocular reflex, vestibular motion sensitivity and convergence distance.46 (C)
Other considerations in the assessment of concussion
There is a need for definitive, objective and clinically useful tools for the diagnosis of concussion. This interest has led to innovation and fast-paced changes with the ongoing need for refinement and validation of these efforts.
Emerging sideline concussion evaluation tools
Other sideline evaluation tools have been developed, including tests of vestibular-ocular function and reaction time. The physical exam components of the VOMS are becoming more frequently used in the office setting, but the role of formal VOMS testing on the sideline has not yet been studied. The King-Devick (KD) test is a proprietary, timed saccadic eye movement test requiring individuals to quickly read numbers aloud.28 The KD requires a baseline test as well as an understanding of potential learning and practice effects to be useful. Simple reaction time as a sideline screen has also been studied using a dropped weighted stick.47 Further research including larger numbers and control subjects is needed for these tests.
Other technologies such as app-based measures of reaction time, eye trackers, postural stability, speech pattern, quantitative electroencephalography and various abbreviated neurocognitive tests are being developed. Some are available on portable electronic platforms with the ability to share information with multiple users. These newer technologies do not have sufficient research to establish their utility. The mention of all of these sideline tools does not imply AMSSM endorsement. (C)
Helmeted and non-helmeted impact monitors
Current impact sensor systems indirectly monitor linear and angular acceleration forces to the brain; however, they may not consistently record head impacts or forces transmitted to the brain. Neither a device nor a specific threshold measure of force or angular acceleration can be used to diagnose concussion.38 48 Some athletes experience high forces with no clinical symptoms of concussion, and some athletes sustain a concussion at much lower impact forces, making current impact measures a poor predictor of SRC.49 The number, location, density and individual thresholds of head impacts may be important parameters. At this time impact monitors are a research tool requiring additional study and are not validated for clinical use in the diagnosis or management of SRC. (B)
Biomarkers of concussion
Head CT is rarely necessary in the evaluation of SRC but should be used when clinical suspicion for intracranial bleeding or macrostructural injury exists. Intracranial bleeds are rare in the context of SRC, but can occur, and CT is the standard evaluation tool for these and other suspected neurosurgical emergencies in acute and critical care. Conventional brain MRI is not commonly used in the evaluation of concussion, but may have value in cases with atypical or prolonged recovery. Newer, advanced multimodal MRI technologies (eg, diffusion tensor imaging, resting-state functional MRI, quantitative susceptibility imaging, magnetic resonance spectroscopy, arterial spin labelling) are being studied in research protocols aimed at understanding the neurobiological effects and recovery after SRC.50 Additional research will be required to determine the clinical utility of advanced neuroimaging in the setting of SRC. (B)
The role of fluid biomarkers (blood, saliva, cerebrospinal fluid) in the diagnosis of SRC is also under active investigation.50 Proteomic markers of injury and recovery in more severe forms of civilian neurotrauma and traumatic brain injury have shown some promise; however, in recent systematic reviews, the overall level of evidence is low for using fluid biomarkers for diagnosis of SRC.50 Fluid biomarkers have potential for informing the pathophysiology of concussion and neurobiological recovery, but more research is required to determine their clinical utility.50 Recent Federal Drug Administration (FDA) approval of a two-protein brain trauma indicator with glial fibrillar acidic protein and ubiquitin carboxy-terminal hydrolase L1, and clinical use of S100 calcium-binding protein β in Europe, shows promise for ruling out intracranial bleeds and structural damage to reduce utilisation of head CTs in the emergency department setting. At this time, none of these tests has a role in the diagnosis or management of SRC. (B)
There is currently no scientific support for genetic testing in the evaluation and management of athletes with SRC, and additional research is needed to determine how genetic factors influence risk of injury and recovery after SRC.50 (B)
Clinical profiles
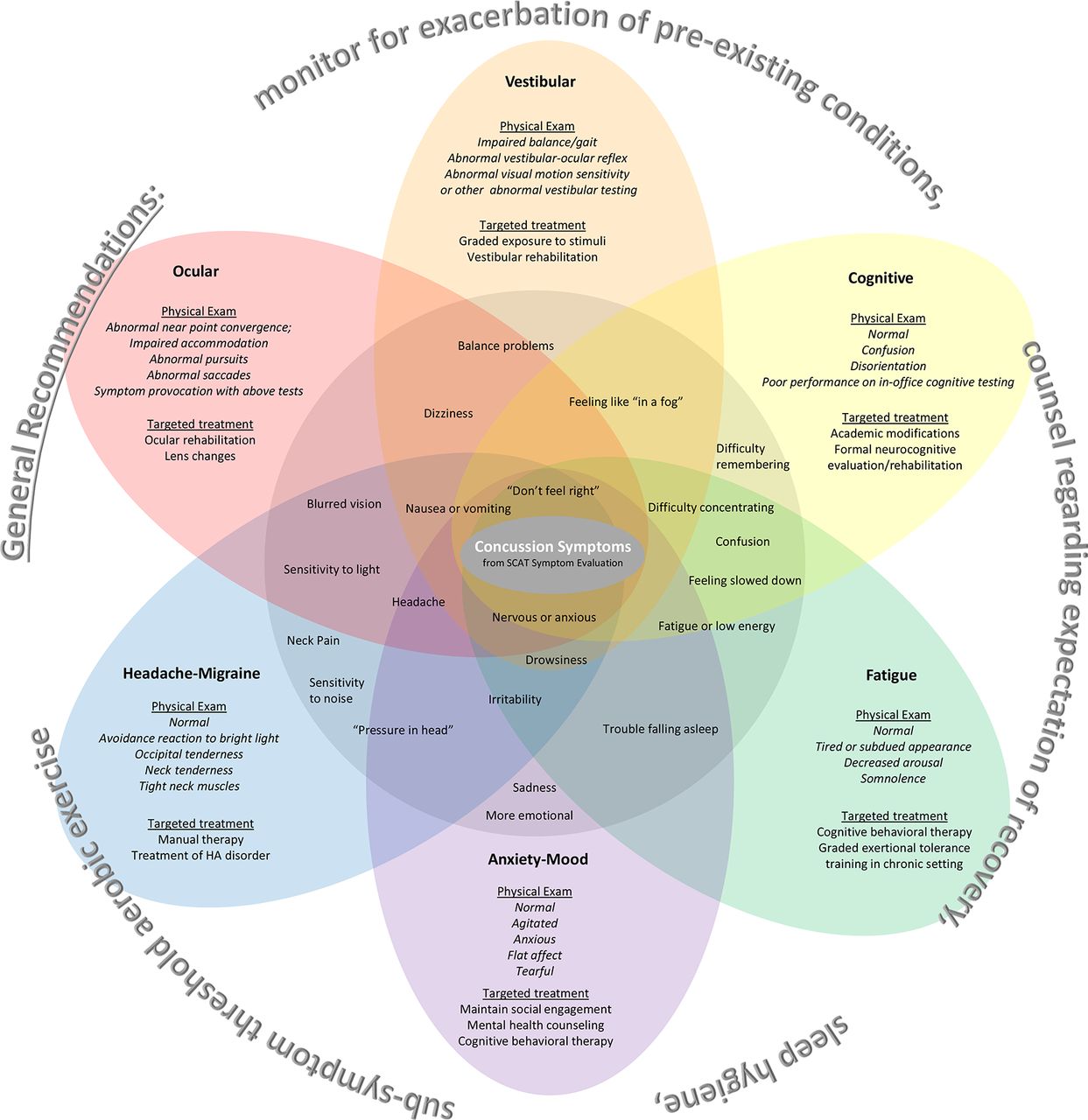
The recognition of heterogeneity among concussion presentations has led to the concept of ‘clinical profiles’ or ‘clinical domains’ with the potential for more specific prognostic value and targeted treatment.51–53 It must be stressed that this is an emerging concept and does not represent clinical standards or norms but may serve to facilitate individualised patient management. Although SRC may present with symptoms representing only one clinical profile, it is more often that SRC presents with symptoms and impairment supporting multiple profiles. It is currently unknown at what postinjury time point these profiles become clinically important as most SRCs resolve with time. Thus, clinical profiles may be more applicable to athletes with persistent symptoms. More research in this area is needed. The diverse symptoms and functional impairments of SRC are variously categorised with overlapping symptom clinical profiles that may include cognitive, affective (anxiety/mood), fatigue, migraine/headache, vestibular and ocular52–54 (see figure 1). How clinical profiles fit into the clinical care of SRC warrants additional research. (C)

{kind=link}
Overlapping clinical profiles: an emerging concept to facilitate individualised management after sport-related concussion. Most patients have features of multiple profiles. HA, headache; SCAT, Sports Concussion Assessment Tool.
Management of concussion
SRC clinical symptoms typically resolve spontaneously, with 80%–90% of concussed older adolescents and adults returning to preinjury levels of clinical function within 2 weeks.55 In younger athletes, clinical recovery may take longer, with return to preinjury levels of function within 4 weeks.56 It is important to communicate the usual time course and outcome to patients and families to relieve the anxiety that often accompanies this injury. Symptom checklists are useful for tracking symptomatic recovery. Clinical recovery based on our current evaluation methods and SRC testing may not coincide with complete physiological recovery, although the functional, clinical and long-term significance of persistent imaging findings and subtle neuropsychological deficits on tests used in research settings is unknown.44
Predicting recovery
The most consistent predictor of recovery from concussion is the number and severity of acute and subacute symptoms.57 Subacute headache and depression after injury are risk factors for symptoms persisting for >1 month.57 A preinjury history of mental health problems, particularly depression, appears to increase the risk for prolonged symptoms.56 Athletes with learning disabilities or attention deficit/hyperactivity disorder do not appear to be at risk for prolonged recovery.57 More research is needed to address other SRC modifiers, including age and sex, although some studies demonstrate a longer period of reported symptoms in women compared with men and for adolescent athletes.57 Newer research suggests that a lower symptom-limited heart rate threshold during graded exercise testing within a week of SRC in adolescents predicts a longer recovery time.58 (B)
Treatment of SRC
In this section the role of rest, physcial activity and nutraceuticals are discussed.
Prescribed rest
Prescribed cognitive and physical rest has been the mainstay of treatment for the last several decades despite insufficient evidence to support this approach.59 60 Earlier animal data suggested that uncontrolled or forced early exercise is detrimental to recovery61–63; however, recent data in aerobically trained animals given early access to exercise showed improved outcomes compared with no or delayed exercise or to social isolation.64 In human studies, strict rest after SRC slowed recovery and led to an increased chance of prolonged symptoms.65 66 Total rest, that is, ‘the dark room’ or ‘cocoon therapy’, may have detrimental effects similar to social isolation effects seen in animal studies and is no longer recommended.3 51 Consensus guidelines endorse 24–48 hours of symptom-limited cognitive and physical rest followed by a gradual increase in activity, staying below symptom-exacerbation thresholds.3 Further research is needed to define the role of prescribed rest in recovery. (C)
Activity and exercise
Exercise intolerance is an objective physiological sign of acute concussion that appears to reflect impaired autonomic function and control of cerebral blood flow.67 68 Exercise improves autonomic nervous system balance and CO2 sensitivity, cerebral blood flow regulation, brain-derived neurotrophic factor gene upregulation, and both mood and sleep.69 70 Emerging data suggest that symptom-limited activity, including activities of daily living and non-contact aerobic exercise, may begin as soon as tolerated after an initial brief period (24–48 hours) of cognitive and physical relative rest.3 There is some preliminary evidence that subsymptom threshold exercise improves recovery in acute concussion,71 72 and early symptom-limited graded exercise testing appears to be safe in athletes.58 Understanding for whom and when to begin early exercise after SRC remains an ongoing area of exploration. Early activity and exercise do not take the place of a graded return to sport. (B)
Role of nutraceuticals
Interest in nutraceuticals for prevention and treatment of concussion is high. There is emerging evidence in animal models of concussion that some supplements may protect or speed recovery from concussion, specifically focused on certain B vitamins, omega-3 fatty acids, vitamin D, progesterone, N-Methyl-D-aspartate, exogenous ketones and dietary manipulations (eg, ketogenic diet).73–75 There is a gap, however, between experimentally produced injury in an animal model and the heterogeneous mechanisms that cause human concussion during sports activities. There is no human evidence that nutraceuticals prevent or ameliorate concussion in athletes.76 Supplements are not FDA-regulated and potential for harm or contamination should be considered. This is an area that requires significantly more research to guide future recommendations. (C)
Persistent postconcussive symptoms
Postconcussion syndrome or disorder is a term that has been frequently used to describe patients with lingering symptoms after a sport-related or recreation-related concussion, but often those patients do not meet the diagnostic criteria for these diagnoses. A preferred term is persistent postconcussive symptoms (PPCS), defined as symptoms that persist beyond the expected recovery time frame (>2 weeks in adults, >4 weeks in children).44 Persistent symptoms do not necessarily represent ongoing concussive injury to the brain. It is not unusual for common symptoms to be inappropriately or mistakenly attributed to concussion; therefore, it is critical to understand pre-existing or coexisting symptoms and conditions in the evaluation of PPCS.
Targeted treatments
Recent systematic reviews have advocated including vestibular, oculomotor, psychological, sleep, cervical and autonomic nervous system evaluations in the assessment in order to facilitate individualised and targeted management of PPCS.77
Exercise for persistent postconcussive symptoms
Activity and exercise that do not exacerbate symptoms are recommended for those with persistent postconcussive symptoms. A formal symptom-limited aerobic exercise programme has been shown to be safe and improve resolution of persistent symptoms compared with controls and should be considered in athletes with symptoms lasting longer than expected.78–80 The Buffalo Concussion Exercise Treatment Protocol, a progressive subsymptom threshold aerobic exercise programme based on systematically establishing the level of exercise tolerance on the Buffalo Concussion Treadmill Test, is the most studied controlled exercise programme.81 It is ideal for those with persistent postconcussive symptoms to be evaluated by a provider or multidisciplinary team with expertise in complicated concussion management. (C)
Physical therapy, vestibular therapy and collaborative care
Athletes with migraine/headache should be evaluated for underlying headache disorders, cervical dysfunction causing headache and other possible contributors, and treated appropriately with non-pharmacological and pharmacological treatments.77 Vestibular therapy should focus on specific deficits identified and use an ‘expose-recover’ model performed by clinicians with expertise in vestibular rehabilitation.51 82 There is preliminary evidence that addressing cervical spine and/or vestibular dysfunction with a targeted physical therapy programme improves outcomes in those with PPCS.83 84 Cognitive work should be modified or limited to that which does not exacerbate symptoms.60 In athletes with sleep disturbances following SRC, sleep hygiene should be addressed, sleep monitored and treated with non-pharmacological or pharmacological strategies.85 Individuals experiencing psychological symptoms such as irritability, sadness and anxiety should be evaluated and offered appropriate treatment. A collaborative care model including cognitive behavioural therapy can improve outcomes in those with persistent postconcussive symptoms.86 (C)
Return to learn
SRC can induce changes in attention, cognitive processing speed, learning, short-term memory and executive function that make learning difficult.87 Return to learn is the process of transitioning back to the classroom following concussion using individualised academic adjustments87 88 (see table 4). School personnel should be informed of the injury and implement an initial school support plan without delay.89 Many concussed athletes recover quickly enough to return to the classroom with no or very brief adjustment of academic activities, but schools should be prepared to provide additional support in the event that recovery takes longer. Athletes with persisting symptoms should be provided an individualised return to learn accommodation plan that allows for symptom-limited learning activity similar to return to physical activity protocols. Early introduction of symptom-limited physical activity is appropriate; however, return to sport training activities should follow a successful return to the classroom for student-athletes. (C)
Return to learn
Return to sport
Concussion-related symptoms and signs should be resolved before returning to sport. A return-to-play progression involves a gradual, stepwise increase in physical demands and sport-specific activities without return of symptoms before the final introduction of exposure to contact (see table 5). The athlete should also demonstrate psychological readiness for returning to play. The return-to-sport progression is individualised and is a function of the injury, the athlete’s age, prior SRC and level of play, and the ability to provide close supervision during the return to activity. The return-to-sport progression presented by the CISG is widely accepted but empiric, without evidence to support either the progression sequence or the time spent in each stage. In general, for young athletes, each stage of the progression should be at least 24 hours without return of symptoms before progressing to the next stage. (C)
Return to sport
Return to driving
In addition to return to learning and sporting environments, older athletes may need to return to driving, where subtle deficits could compromise safety. Most sports medicine physicians do not counsel athletes with SRC about driving.90 Driving is a complex process involving coordination of cognitive, visual and motor skills, as well as concentration, attention, visual perception, insight and memory, which can all be affected by SRC.90 Little is known about the risk of driving after SRC, but preliminary data suggest some impairment exists when patients with concussion report they are asymptomatic.91 Currently, no widely accepted return to driving protocols exist; however, in athletes who drive, discussing the potential risks and harms is appropriate. (C)
Risks related to concussion
Short and long-term risks of concussion are an area of growing concern.
Short-term risks of continued exposure after concussion or premature return to play
Continuing to play immediately following a concussion is a risk for increased symptom burden, worsening of the injury and prolonged recovery.92–95 Athletes who return to sport prior to full recovery are at increased risk of repeat concussion.96 Some research has demonstrated that athletes who return to sport after SRC following standard return to sport protocols had an increased rate of musculoskeletal injury.97 98 The ‘Second Impact Syndrome’ is both rare and controversial. It is considered by some to be a potentially life-threatening complication of reinjury during the initial postinjury time period that is not fully understood and appears primarily limited to paediatric and adolescent athletes.99 (C)
Long-term risks after concussion
Mental health problems and depression
Sport and exercise are protective against depression.100 Most studies examining the relationship of contact sports to mental health problems or depression later in life have low methodological quality, high risk of bias or both.101–103 Several studies have reported that NFL and college football athletes with a history of concussion are more likely to experience depression, although the risk of mental health issues, including suicide, among former NFL players is lower than age-matched controls.101–103 Former high school football players show no difference in cognitive function testing and have lower depression scores when compared with non-contact sport controls.104 Mental health issues are common, multifactorial and often present independent of participation in contact or collision sport. Longitudinal research on contact sport athletes that addresses multiple variables is needed to understand the long-term risks. (C)
Chronic traumatic encephalopathy
Chronic traumatic encephalopathy (CTE) and other neurodegenerative diseases have been described in former athletes with a history of concussion or repetitive head impact exposure, typically accompanied by behavioural change. The incidence and prevalence of CTE in the general population, in former athletes, or in former athletes with a history of concussion or repetitive head impact exposure, are unknown. A cause and effect relationship between postmortem CTE changes and antemortem behavioural and cognitive manifestations has not been demonstrated, and asymptomatic players have had confirmed CTE pathology at autopsy.105 106 It is also unknown if CTE is a progressive disease, and whether tau deposition is the cause of CTE or a byproduct or marker of a disease.107 (C)
The expression of CTE-associated symptoms may be related to impact load and type, duration of career, underlying genetic factors, or other lifestyle behaviours including alcohol, drug and anabolic steroid use, general health, psychiatric disease, and other factors. Some retrospective studies have reported increased risk of neurodegenerative disease in former professional football players; however, former high school football players do not show a higher prevalence of neurodegenerative disease when compared with non-football peers.108 109 The most widely described risk factor to date is extensive exposure to both multiple concussions and repetitive head impacts, but the degree of necessary exposure is likely specific to the individual and subject to multiple modifying risk factors.110 Athletes and former athletes who present with neuropsychiatric symptoms and signs that have been ascribed to CTE should be evaluated for potentially treatable comorbid conditions that share symptoms, and not be assumed to have CTE.111 (C)
Repetitive head impacts
Subconcussive or non-concussive head impacts have been discussed as an entity apart from concussion history that may create risk of long-term neurological sequelae. Subconcussive impacts are defined as transfer of mechanical energy to the brain causing presumed axonal or neuronal injury in the absence of clinical signs or symptoms.112 It is unclear if a biomechanical threshold or other factors lead to injury or if this entity qualifies as injury since it does not seem to be associated with neuropsychological changes.113 Although subconcussive impacts have been associated with CTE, the short-term and long-term effects of repetitive head impacts, similar to SRC, cannot be accurately characterised using current technology. Future research will depend on developing technologies that can assess brain changes following repetitive asymptomatic head trauma in living subjects. (C)
Disqualification from sport
There are no evidence-based guidelines for disqualifying or retiring an athlete from sport after concussion; therefore, each athlete should be carefully and individually assessed to determine the safety and potential long-term health consequences of continued participation. There is no ‘set’ number of concussions or repetitive head impact exposures that should force retirement from a season or from sport, and it is likely that athletes with higher numbers of diagnosed concussions will be seen in clinical settings as the recognition and awareness of concussion are improved. (C)
Considerations for retirement from sport include the length of concussion recovery (progressively longer time intervals for symptom resolution), patterns of developing concussion with less force or increasing severity of concussions, as well as the athlete’s readiness or apprehension regarding return to sport. Additional contraindications for continued participation may include behavioural changes, post-traumatic seizures, persistent neurological deficit or imaging findings suggesting additional/other pathology. Individual and family tolerance of risk and perception of the benefit of sport participation (eg, personal identity, financial motivation) should be considered and explored in a process of shared decision making.114 (C)
Prevention
Prevention of SRC is ultimately more effective in reducing the burden of this condition than any treatment, and while primary prevention of all SRC is not possible measures to decrease the number and severity of concussions are of value. Rule changes, enforcement of existing rules, technique changes, neck strengthening and equipment modifications have been the primary focus of prevention. There is moderate evidence that delaying the introduction of body checking in youth hockey reduces concussion rates.115–117 The effectiveness of rule changes in youth soccer and football to reduce concussion incidence is not clear; however, there is initial evidence that practice modification and changes in tackling technique may reduce injury.118 119 There is conflicting evidence regarding mouthguards and concussion reduction, and mouthguards should primarily be used for preventing dental trauma.117 Helmets prevent skull trauma and intracranial bleeding, but their protective effects for concussion are less pronounced. Some football helmet designs have improved the ability to absorb force, but it is unknown if this will reduce concussion incidence. Studies of headgear in other sports have produced mixed results. Player behaviour can change when athletes wear new or ‘improved’ protective equipment, encouraging a more aggressive style of play, potentially increasing the risk for injury. (B)
Future research directions
The panel identified these key areas for further study:
High-quality epidemiological studies in younger athletes, recreational activities, non-traditional sports and non-school sponsored team sports (select, recreational) should be considered.
Continued studies of high school, college and professional athletes to better understand concussion rates, repetitive head impact exposure, mechanisms, recovery patterns, risk factors and the success of specific intervention and prevention strategies.
Research regarding objective tests, including neuroimaging and fluid biomarkers, to determine their diagnostic and prognostic utility over and above current clinical assessment methods.
Research regarding specific factors or modifiers that are associated with prolonged recovery.
Investigation into the utility of clinical profiles/concussion domains for diagnosis, prognosis and treatment.
Research on the role, if any, of nutraceuticals in the prevention and treatment of acute concussion and for those with prolonged symptoms.
The role of aerobic exercise, physical therapy (treatment of associated injuries such as cervical and vestibular abnormalities) and psychological therapy in the treatment of SRC.
Advanced studies to increase understanding of neurobiological effects and recovery after SRC.
Development of evidence-based return-to-learn and return-to-sport paradigms.
Exploration of the potential long-term effects of SRC and repetitive subconcussive impacts on neurological health via prospective longitudinal studies and laboratory research.
The role of genetic susceptibility to acute and chronic effects of SRC and subconcussive impacts.
Further development and implementation of primary and secondary prevention measures.
Conclusion
Sport related concussion is a complex, heterogeneous brain injury that typically resolves clinically in 1–4 weeks. The diagnosis of concussion is challenging as it relies on self-reported symptoms that can be caused by other common conditions and there are no readily available objective diagnostic tests to confirm the diagnosis. Sports medicine physicians and others who diagnose concussion should be familiar with the psychometric properties of the sideline and office assessment tools they are using. After a brief period of rest, acutely concussed patients can be encouraged to gradually and progressively increase physical and cognitive activity while staying below their symptom-exacerbation thresholds. In cases of prolonged symptoms, a multidisciplinary team experienced in the diagnosis and treatment of concussion should be considered. Further research is necessary to better understand the potential long-term effects from concussions and repetitive subconcussive impacts, as well as incidence, prevalence and modifiable risk factors. There are many beneficial aspects to participation in sport and exercise that should be balanced against the concern for concussion. The AMSSM supports continued research in the area of SRC to enhance safe participation in sport.
References
Footnotes
This article has been co-published in the Journal of Sports Medicine and Clinical Journal of Sports Medicine.
Patient consent for publication Not required.
Contributors All authors listed contributed to the statement with attendance at an inperson meeting, multiple conference calls and emails, and multiple revisions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KGH has research grants from Vulcan Industries and the Pac-12, outside of submitted work JRC reports grants from Banyan Biomarkers, grants from Florida High Tech Corridor Matching Funds Program, and grants from NCAA-DoD CARE Consortium, outside the submitted work. SH has stock options in Vicis, outside of submitted work. APK has research contracts with GE-NFL Head Health Initiative, Abbott Labs and ElMindA, and receives royalties from the book ’Concussion', outside of submitted work. JJL has research grant from the AMSSM, outside of submitted work.
Provenance and peer review Not commissioned; internally peer reviewed.