Article Text

Abstract
Objectives To update our previous evaluation of the exercise interventions used in randomised controlled trials of breast cancer survivors in relation to (1) the application of the principles of exercise training in the exercise prescription; (2) the reporting of the components of the exercise prescription; and (3) the reporting of adherence of participants to the prescribed interventions.
Design Systematic review.
Data sources The OVID Medline, Embase, CINAHL and SPORTDiscus electronic databases were searched from January 2010 to January 2017.
Eligibility criteria Randomised controlled trials of at least 4 weeks of aerobic and/or resistance exercise in women diagnosed with breast cancer, reporting on physical fitness or body composition outcomes.
Results Specificity was appropriately applied by 84%, progression by 29%, overload by 38% and initial values by 67% of newly identified studies. Reversibility was reported by 3% anddiminishing returns by 22% of newly identified studies. No studies reported all components of the exercise prescription in the methods, or adherence to the prescribed intervention in the results. Reporting of reversibility has increased from 2010, but no other improvements in reporting were noted from the previous review.
Summary/Conclusion No studies of exercise in women with breast cancer attended to all principles of exercise training, or reported all components of the exercise prescription in the methods, or adherence to the prescription in the results. Full reporting of the exercise prescribed and completed is essential for study replication in research and translating research findings into the community, and should be prioritised in future trials.
- cancer
- breast
- review
- exercise training
- methodology
Statistics from Altmetric.com
Introduction
Based on the most recent global estimates, 1.7 million new cases of breast cancer are diagnosed worldwide each year, making breast cancer the most commonly diagnosed cancer in women.1 Survival following a breast cancer diagnosis has greatly increased as a result of treatment advancements, with a five-year survival rate of 87%2 in developed countries such as Canada. Due to this trend, there is a growing worldwide population of women who are living long after a cancer diagnosis, but who are faced with many late and long-term side effects. Research is now focused on addressing late and long-term cancer treatment side effects along with competing risks of mortality and morbidity. Clinical practice guidelines recommend that breast cancer survivors be continuously monitored for lymphoedema, cardiotoxicity, cognitive impairment, distress, depression and anxiety, fatigue, bone health, pain and peripheral neuropathy, and should receive health promotion counselling related to obesity, physical activity, nutrition and smoking cessation.3
There is growing evidence demonstrating the beneficial role of exercise in mitigating several adverse effects of breast cancer and its treatment, and this evidence has been summarised in a number of systematic reviews and meta-analyses.4–8 However, systematic reviews and meta-analyses tend to aggregate exercise programmes into general categories and rarely investigate the specific features of exercise programmes that may make them more or less effective. While helpful for providing a general consensus regarding the benefits of exercise, this clustering of training programmes may impede translation of effective programmes from research to practice and provides little guidance about the salient features of a training programme for this clinical population.
In 2012, our team published a systematic review evaluating the application of the general principles of exercise training in studies of women diagnosed with breast cancer.9 This was in response to our observation that the use of well-established exercise training principles in the field of exercise research and practice (see table 1) were not commonly being reported in the exercise oncology literature. We also reviewed the reporting of the exercise prescription components of frequency, intensity, time and type (FITT), and the reporting of adherence to the prescribed intervention. We found that of the 29 studies reviewed, no studies applied all principles of exercise training, or all components of the exercise prescription in their methods or results. We urged researchers in the field to improve their tracking and reporting of these key details.
Exercise training principles
Since the publication of the 2012 review, many new randomised controlled trials (RCTs) have been published and included more participants and interventions of longer duration and with extended follow-up. Therefore, there was a need to update our previous review to include these new trials. The objective was to highlight potential areas of improvement in exercise prescription methods and reporting in order to move the exercise oncology field forward. We have updated our previous evaluation of the exercise interventions used in RCTs for breast cancer survivors in relation to (1) the application of the principles of exercise training in the development of the exercise prescription; (2) the reporting of the components of the exercise prescription (ie, FITT) in both the study methods and results; and (3) the adherence of participants to the prescribed interventions.
Methods
We used the same protocol as our previously published review9; no other protocol for this update has been published. The Medline, CINAHL, SPORTDiscus and Embase electronic databases were searched from January 2010 to January 2017. This overlapped with our previous search (completed in May 2010) to avoid any missed papers that were in the process of indexing during the search. This review includes the papers from the original review with the addition of new papers published between 2010 and 2017. The previous subject heading terms related to breast cancer and exercise, specific to each database, were used and combined with the AND term. The search was then limited to English-language publications in peer-reviewed journals. Key publications, including relevant systematic reviews identified during the literature search, were hand-searched for relevant publications.
We included RCTs with one or more treatment arms involving at least four weeks of aerobic and/or resistance exercise, conducted in women diagnosed with breast cancer. Studies including participants diagnosed with other types of cancer were excluded, as were alternative exercise interventions such as yoga, Pilates or Tai Chi, as well as therapeutic interventions (ie, shoulder rehabilitation). Interventions focused primarily on physical activity behaviour change and those in which the only outcomes reported were physical activity levels or psychosocial outcomes were excluded. To be eligible for inclusion, studies had to report at least one relevant physiological outcome related to exercise (eg, aerobic capacity, muscular strength, functional capacity or body composition). Additional publications from previously included trials were also added to the database of included articles to allow for review of previously extracted data and updates regarding inclusion of information on use of exercise training principles, exercise prescription or adherence to exercise prescription data, particularly the principles of reversibility and diminishing returns reported in follow-up papers.
Two reviewers (SNS and KAB) independently screened the title and abstract of each study identified to determine eligibility. If required, full-text articles were obtained and reviewed for eligibility. Eligibility lists were compared using an online software system (Covidence Systematic Review software, Veritas Health Innovation, Melbourne, Australia). Discrepancies were resolved by consensus and the input of a third reviewer (KLC) when necessary.
Data were extracted in duplicate by the two reviewers using online software (Covidence), including sample size, timing of intervention delivery (during/after treatment), study duration and follow-up, measured outcomes, and study findings. Specific exercise prescription data were abstracted according to the ‘FITT’ format from each publication’s methods section, including frequency (number of sessions per week), intensity (relative or absolute intensity of activity), time (duration of activity) and type of activity.
For each exercise prescription described, a rating was assigned for the application of each principle of exercise training (see table 1). Application of a principle was assigned a ‘+’ when the application was clearly reported, and an ‘NR’ (not reported) if there was no indication that the principle was used in the exercise prescription. A ‘?’ was assigned when the principle was mentioned but not described, was inconsistently applied or was otherwise unclear. Adequate reporting of the prescription according to the FITT format and reporting of participant adherence to the prescription were also assigned a ‘+’, ‘NR’ or ‘?’. For multiarm trials comparing different interventions, the application of the principles of exercise training and the exercise prescription was evaluated separately for each intervention arm. For trials that were previously included, newly identified articles were screened for new information to determine whether the previously assigned ratings should be altered.
The number and percentage of included studies that met each criterion were calculated (1) among newly identified studies and (2) among all studies identified to date. To determine whether there has been an improvement in the reporting of each criteria over time, a χ2 test was used calculate difference in proportions of those reporting + versus ‘?’ or NR among studies identified in our first review (2010 and prior) and new studies identified in this review (2010 and later).
Results
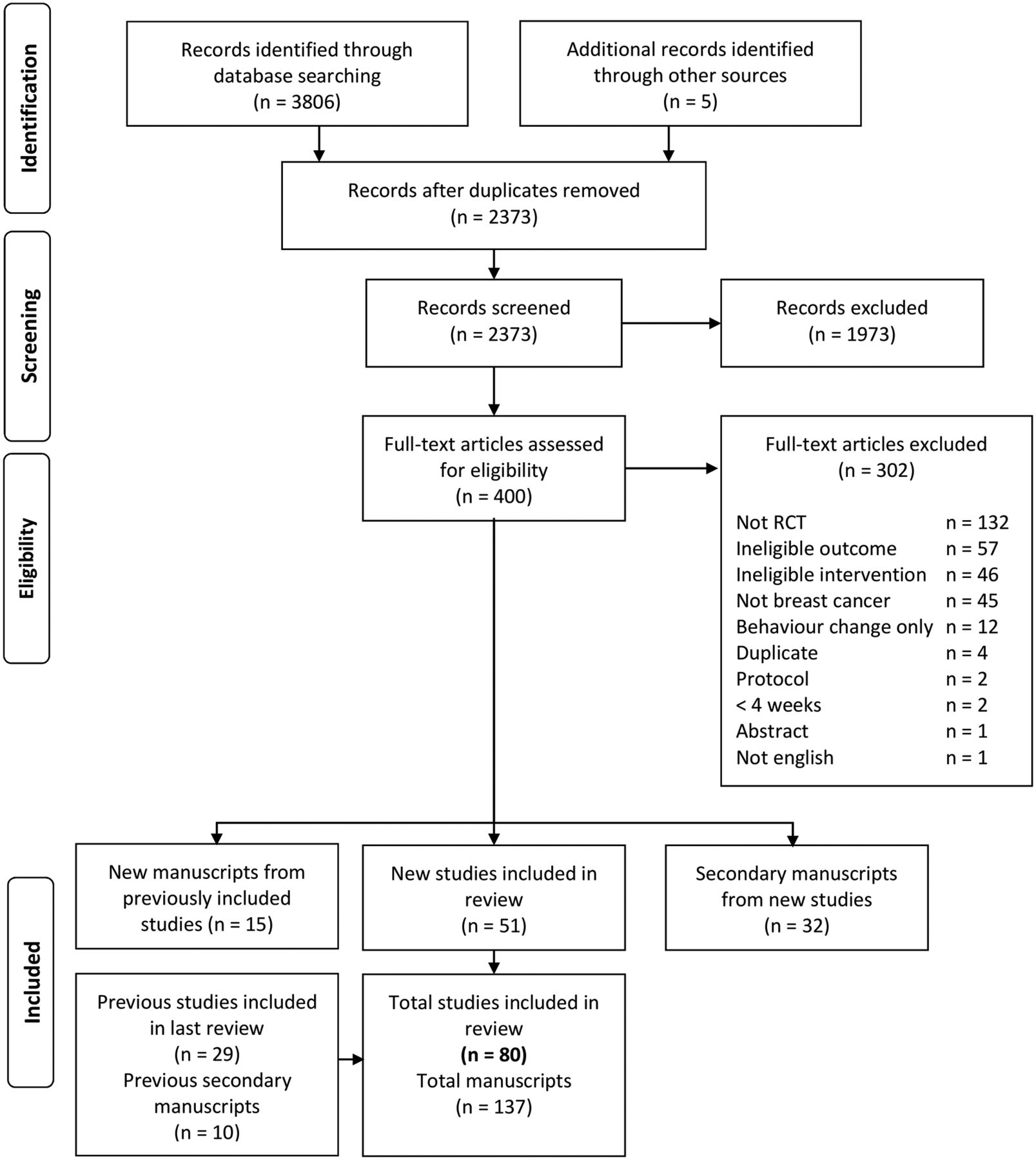
Eighty-three manuscripts describing 51 trials published since 2010 were identified and included (figure 1). Sixteen new manuscripts from previously identified trials were also identified and reviewed for new information provided on relevant methods and outcomes (ie, follow-up). This resulted in a total of 138 articles describing results from 80 trials published between 1994 and 2017 (see online supplementary table 1 , for full list of included articles). Of the 16 newly identified articles from previously included studies, 10 (63%) reported on different outcome measures,10–19 3 (19%) reported secondary analysis of already reported outcomes20–22 and 3 (19%) reported findings from postintervention follow-up.23–25
Supplementary file 1
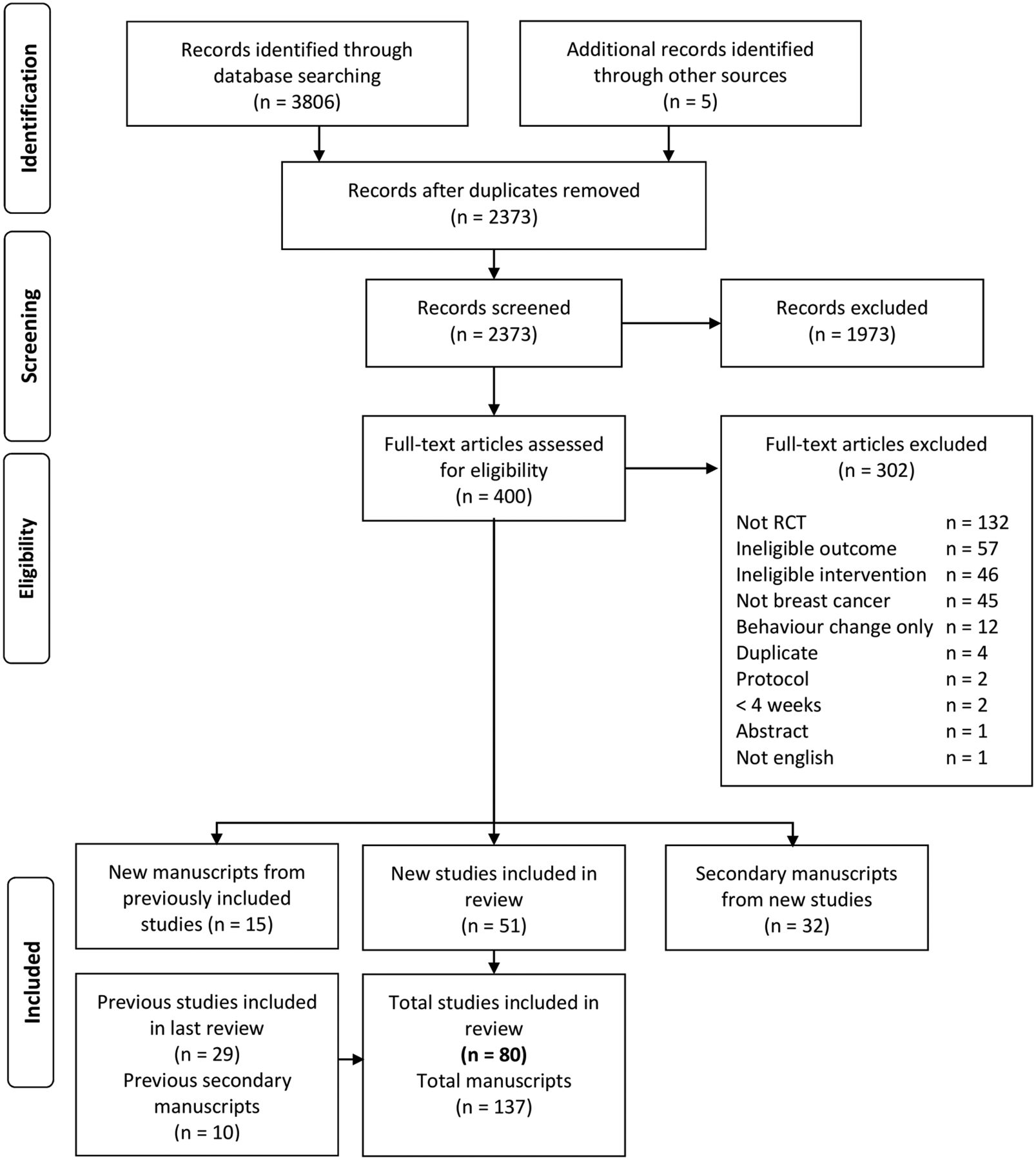
Flow chart of study selection process. (RCTs, randomised controlled trials)
Fourteen new studies (27%) prescribed aerobic exercise only,26–39 7 new studies (14%) prescribed resistance exercise only,40–46 25 new studies (49%) prescribed aerobic and resistance exercise together,47–71 and 5 new studies (10%) were multiarm trials (12 intervention arms) comparing aerobic with resistance or aerobic and resistance exercise72–76 (online supplementary table 1). Eighteen new studies (35%) were conducted in women undergoing adjuvant treatment for breast cancer,26 30 32 33 35 39 42 44 50 55–57 65 69 71 73 75 76 and 31 new studies (61%) were conducted in women after completion of adjuvant breast cancer treatment.28 29 31 34 36–38 40 41 43 45 46 48 49 51–54 58–64 66–68 70 72 74 One study included women who had undergone surgery for breast cancer and may or may not have been undergoing chemotherapy and/or radiation therapy,47 and one study did not report the timing of the intervention.27 Newly included interventions ranged from 4 to 52 weeks, with follow-up measures taken from 3 weeks to 5 years postintervention.
Application of the principles of exercise training
Table 2 details the ratings of the principles of exercise training for previously included and newly identified studies. After reviewing newly published articles from previously included trials, one study’s77 rating of reversibility and diminishing returns was changed from NR to + after publication of follow-up data. Χ2 tests show no significant difference in the proportion of newly included versus previously identified studies reporting the principles of specificity, progression, overload or initial values. There was a significant difference in the distribution of reporting of the principles of reversibility (P<0.01) and diminishing returns (P<0.001) as more newly included studies were assigned a ‘?’ instead of an ‘NR’ for these two principles (data not shown).
Application of the principles of exercise training and outcomes in exercise intervention studies in breast cancer survivors
The following results are presented for newly identified studies, and with a comparison to the total number of studies in the review from both the original search and this update. Among newly identified studies, specificity was appropriately applied by 12 aerobic studies26–30 32–37 39 (86% vs 75% overall), 6 resistance studies40–42 44–46 (86% vs 90% overall), 19 mixed studies47–49 51–56 58 59 61–64 66–69 (76% new and overall) and all 12 intervention arms within multiarm studies72–76 (100% vs 94% overall). Specificity was unclear in 2 aerobic studies31 38 (14% vs 18% overall), 1 resistance study43(14% vs 10% overall) and 6 mixed studies50 57 60 65 70 71 (24% new and overall). No new studies were assigned an NR for specificity.
Progression was appropriately reported by 5 aerobic26 28 30 36 39 (36% vs 43% overall), 6 resistance40–42 44–46 (86% vs 80% overall), 4 mixed49 51 54 64 (16% vs 15% overall) and 2 interventions within a multiarm trial73 (17% vs 33% overall). Progression was unclear in 4 aerobic27 34 35 37 (29% vs 32% overall), 1 resistance43 (17% vs 10% overall), 16 mixed47 48 50 52 55 56 58–61 63 66 67 69–71 (64% vs 59% overall) and 7 interventions within multiarm trials72–74 76 (58% vs 39% overall). Five aerobic29 31–33 38 (36% vs 25% overall), 5 mixed53 57 62 65 68 (20% vs 26% overall) and 2 new multiarm trials75 76 (25% vs 28% overall) did not report progression.
Among newly identified studies, 6 aerobic26 28–30 33 38 (43% vs 36% overall), 6 resistance40–42 44–46 (86% vs 80% overall), 4 mixed47 49 51 69 (16% vs 18% overall) and 6 multiarm trials73 75 76 (50% vs 44% overall) correctly applied the principle of overload. Overload was unclear in 4 aerobic31 36 37 39 (29% vs 32% overall), 1 resistance43 (14% vs 10% overall), 9 mixed50 52 54 56 58 62 64 66 70 (36% vs 32% overall) and 4 multiarm trials74 75 (33% vs 22% overall). Overload was not reported in 4 aerobic27 32 34 35 (29% vs 32% overall), 12 mixed48 53 55 57 59–61 63 65 67 68 71 (48% vs 50% overall) and 2 arms within multiarm trials72 (17% vs 33% overall).
The principle of initial values was correctly reported for 9 aerobic26 30 32 33 35–39 (64% vs 57% overall), all 7 resistance40–46 (100% new and overall), 16 mixed48 50 54–58 60 62 64–69 71 (64% vs 65% overall) and 7 multiarm trials73 75 76 (58% vs 61% overall), and was unclear in 1 aerobic29 (7% vs 18% overall), 2 mixed51 61 (8% vs 6% overall) and 5 multiarm trials72 74 (42% vs 39% overall). Initial values were not reported in 4 aerobic27 28 31 34 (29% vs 25% overall) and 7 mixed studies47 49 52 53 59 63 70 (28% vs 29% overall).
Reversibility was correctly reported in 2 resistance studies45 46 (29% vs 20% overall). Two aerobic26 36 (14% vs 11% overall), 10 mixed48–50 52–55 57 69 71 (40% vs 29% overall) and 7 multiarm trials72 73 76 (58% vs 39% overall) incorrectly reported reversibility. The remaining 12 aerobic27–35 37–39 (86% new and overall), 5 resistance40–44 (71% vs 80% overall), 15 mixed47 51 56 58–68 70 (60% vs 68% overall) and 5 multiarm trials74 75 (42% vs 61% overall) did not report reversibility.
Diminishing returns were reported by 2 aerobic27 39 (14% vs 7% overall), 3 resistance43 45 46 (43% vs 40% overall), 6 mixed52 55 58 63 70 71 (24% vs 21% overall) and 2 multiarm trials72(17% vs 11% overall). Diminishing returns were unclear in 4 aerobic26 30 35 36 (29% vs 18% overall), 7 mixed49 50 53 54 56 57 69 (28% vs 21% overall) and 5 multiarm trials73 76 (42% vs 28% overall). The remaining 8 aerobic28 29 31–34 37 38(62% vs 75% overall), 4 resistance40–42 44 (57% vs 60% overall), 12 mixed47 48 51 59–62 64–68 (48% vs 59% overall) and 5 multiarm trials74 75 (42% vs 61% overall) did not report on diminishing returns.
Reporting of the components of the exercise prescription
There were no changes to the reported exercise prescriptions in previously included trials. When comparing ratings between previously included and newly identified trials, there was a significant difference in the proportion who adequately reported exercise intensity (P=0.01) with more new trials assigned an ‘?’ than ‘+’ for prescribed intensity, but no differences for reporting of prescribed frequency, time and type.
Reporting of the components of the exercise prescription for all included studies is displayed in figure 2. Of the newly identified studies, 3 aerobic29 31 37 (21% vs 32% overall), 18 mixed48 50 53 55–60 62–68 70 71 (72% vs 67% overall) and 3 multiarm trials72 74 (25% vs 33% overall) failed to report all components of the exercise prescription. All seven resistance-only interventions40–46 (100% new and overall) reported all aspects of the exercise prescription. With respect to prescribed frequency in new studies, 1 aerobic29 (7% vs 6% overall) and 2 mixed interventions58 70 (8% vs 9% overall) were assigned an unclear rating, and 1 mixed intervention55(8% vs 3% overall) did not report frequency. Three aerobic29 31 37 (21% vs 11% overall), 12 mixed48 50 55 56 58–60 64 66–68 70 (48% vs 38% overall) and 1 multiarm intervention72 (8% vs 6% overall) were not clear in their reporting of prescribed intensity, and 5 mixed studies53 57 62 65 71 (40% vs. 21% overall) did not report intensity at all. Two aerobic31 37 (14% vs 11% overall), 13 mixed50 53 55–58 60 62 63 66 67 70 71 (52% vs 50% overall) and 1 multiarm74 (8% vs 6% overall) intervention were unclear in their reporting of prescribed duration of exercise. One multiarm trial did not report prescribed duration at all74 (8% vs 17% overall). Three aerobic29 31 37 (21% vs 18% overall) and 8 mixed studies53 56 59 62 65 68 70 71 (32% vs 29% overall) were unclear in their reporting of the prescribed exercise type.

Reporting of components of the exercise prescription. (NR, not reported)
Reporting of adherence to the prescribed intervention
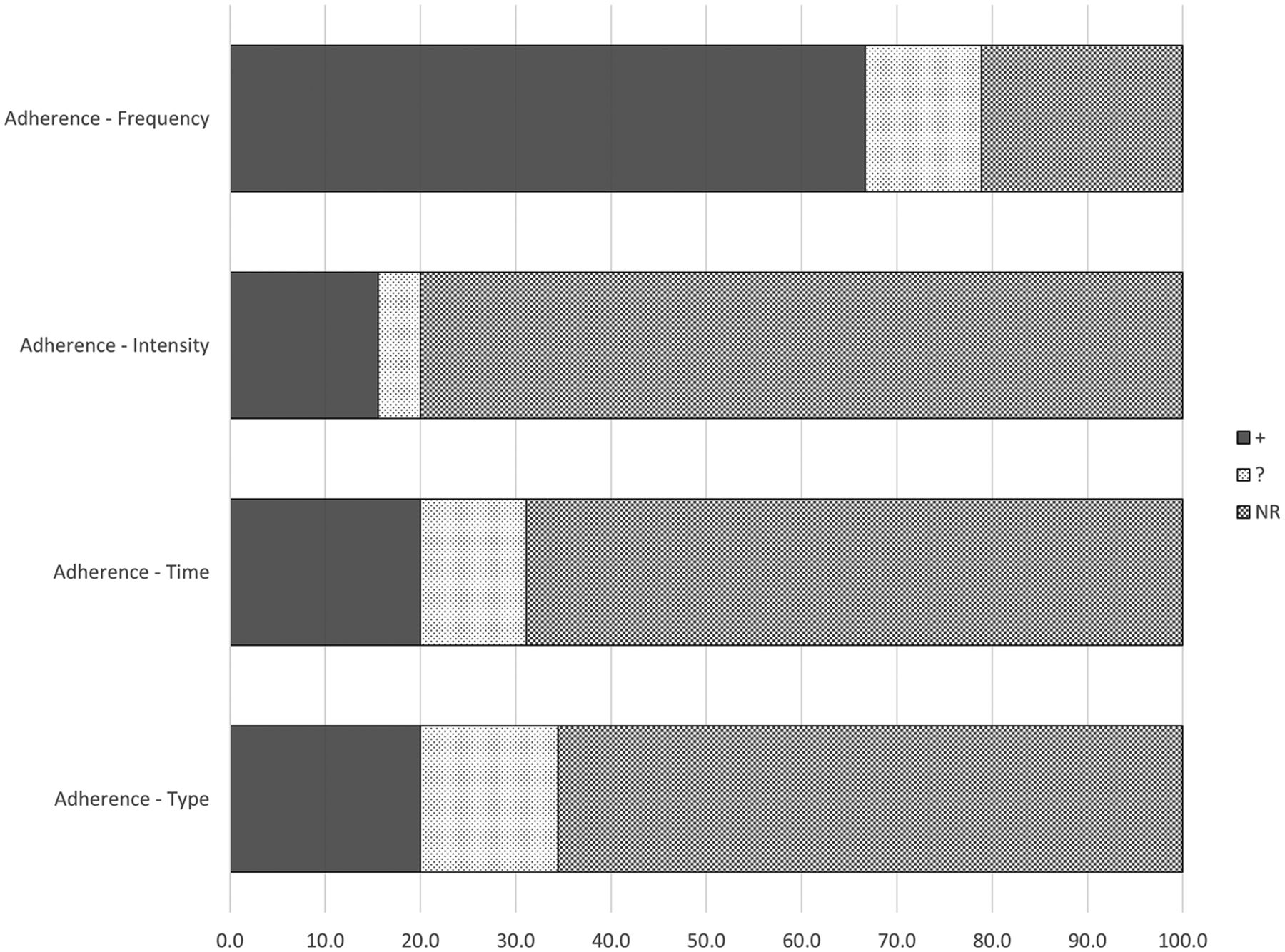
Reporting of adherence to the prescribed interventions or actual exercise completed by participants is displayed in figure 3. Of the newly identified studies, 3 aerobic26 35 39 (21% vs 11% overall), 1 resistance45 (14% vs 10% overall) and 1 multiarm trial73 (8% vs 6% overall) reported on participants’ adherence to all aspects of the prescribed interventions. Four aerobic27 32–34 (28% vs 21% overall), 1 resistance43 (14% vs 10% overall), 6 mixed51 52 59 64 70 71 (24% vs 21% overall) and 2 multiarm75 trials (17% vs 11% overall) did not report adherence. Frequency of exercise completed was reported in 7 aerobic26 28 30 35 37–39 (50% vs 64% overall), 5 resistance40 42 44–46 (71% vs 80% overall), 14 mixed47–50 53–55 60–63 67–69 (56% vs 65% overall) and 8 multiarm trials72–74 (67% new and overall). Frequency was unclear in 3 aerobic29 31 36 (21% vs 11% overall), 1 resistance41 (14% vs 10% overall), 5 mixed56–58 65 66 (20% vs 15% overall) and 2 multiarmed trials76 (17% vs 11% overall). Intensity of exercise completed was reported in 4 aerobic26 29 35 39 (28% vs 21% overall), 2 resistance40 45 (29% vs 20% overall), 1 mixed50 (4% vs 3% overall) and 3 multiarm trials73 (25% vs 17% overall). Intensity of exercise performed was not reported in 8 aerobic27 31–34 36–38 (57% vs 71% overall), 4 resistance41–44 (57% vs 70% overall), 23 mixed47–49 51–62 64–71 (92% vs 94% overall) and 9 multiarm trials72 74–76 (75% vs 72% overall). Intensity of exercise completed was unclear in 2 aerobic studies28 30 (14% vs 7% overall), 1 resistance46 (14% vs 10% overall) and 1 mixed63 (4% vs 3% overall). The duration of exercise completed was reported in 5 aerobic26 28 35 37 39 (36% vs 39% overall), 1 resistance45 (14% vs 10% overall), 1 mixed71 (4% vs 9% overall) and 3 multiarm trials73 (25% vs 17% overall). Duration of exercise completed was not reported in 8 aerobic27 29 31–34 36 38 (57% new and overall), 5 resistance40–44 (71% vs 80% overall), 17 mixed47 48 51–56 59–62 64 65 68–70 (68% new and overall) and 9 multiarm trials72 74–76 (75% vs 83% overall). The duration of exercise completed was unclear in 1 aerobic30 (7% vs 4% overall), 1 resistance46 (15% vs 10% overall) and 7 mixed49 50 57 58 63 66 67 trials (28% vs 24% overall). The type of exercise performed was reported in 5 aerobic26 28 30 35 39 (36% vs 39% overall), 2 resistance45 46 (29% vs 20% overall), 1 mixed71 (4% vs 6% overall) and 1 multiarm trial73 (8% vs 17% overall). Mode of exercise was not reported in 8 aerobic27 29 31–34 36 38 (57% new and overall), 4 resistance41–44 (57% vs 70% overall), 16 mixed47 48 51–53 56–59 61 62 64 65 68–70 (64% vs 68% overall) and 9 multiarm trials72 74–76 (75% vs 72% overall), and was unclear in 1 aerobic37 (7% vs 4% overall), 1 resistance40 (14% vs 10% overall), 8 mixed49 50 54 55 60 63 66 67 (32% vs 26% overall) and 2 multiarm trials73(16% vs 11% overall).

{kind=link}
{kind=link}
{kind=link}
Reporting of adherence to the exercise intervention. (NR, not reported)
There were no changes to the reported adherence to exercise interventions in new articles. Compared with reported adherence in the trials included in the previous review, there was a significant difference in reporting of frequency of exercise performed (P=0.02), with fewer new trials adequately reporting the frequency of exercise completed (58% vs 82%). There were no differences in reporting of adherence to exercise intensity, time and type.
Discussion
In almost seven years, 51 new trials meeting our eligibility criteria were identified, bringing the total number of RCTs evaluating the effect of exercise on physiological parameters in women diagnosed with breast cancer to 80 trials (6878 women). Given the now overwhelming evidence on the benefits of exercise during and after breast cancer treatment on a variety of health-related and psychosocial outcomes, there is a need to identify the best exercise prescriptions in terms of FITT to improve specific outcomes at various time points along the cancer continuum. While it is impossible for a single trial to answer this question, findings from multiple trials can be compared. However, the comparison of findings across numerous exercise trials requires best practice in exercise prescription and full reporting of both the exercise intervention prescribed and actual exercise completed by participants.
There was no change (since our 2012 review) in the proportion of studies reporting proper application of the principles of specificity, progression, overload and initial values. Failure to apply these critical points may help to explain some of the heterogeneity in outcomes that have been observed in other systematic reviews and meta-analyses.4 5 7 8 In some cases, improper exercise prescription, as outlined below, may underestimate some of the benefits of exercise. Improving the reporting of exercise prescriptions in exercise oncology trials will allow for more specific recommendations for types and dose of exercise in published exercise guidelines for breast cancer survivors. This will also assist in translation of these interventions outside of the research setting, allowing for the delivery of appropriate, safe and effective exercise interventions to be delivered in a community or clinical setting.
Application of the principle of specificity was commonly reported, consistent with findings in our previous review. However, nine newly identified studies had not appropriately applied the principle of specificity, as the exercise prescribed did not clearly match the desired study outcomes. For example, one study prescribed resistance exercise to improve fatigue but only measured aerobic capacity (6 min walk test) to determine the effectiveness of the intervention.57 When inappropriate populations are targeted for improvements in a desired outcome, or the exercise prescription is not well suited to promote change in the primary outcome of interest, the effect of exercise may be underestimated. A lack of statistically significant or clinically meaningful change observed may be due to the exercise prescription chosen, rather than a lack of efficacy of exercise.
Less than one-third of included studies properly reported the principle of progression, and it was unclear in almost half of the newly included studies. Studies were given a rating of ‘unclear’ if they stated that the exercise prescription was updated or progression was included, but how this was done was not described. This information, particularly the rate of progression that is well tolerated by participants at various stages (ie, during or after treatment), is critical for those designing future interventions or implementing exercise programmes outside of research settings. A lack of progression could lead to null findings. Full reporting of whether women were progressed more slowly than prescribed should be considered as this information allows for proper interpretation of study findings and better informs future exercise programme implementation within clinical practice and community settings.
Almost 40% of newly identified trials adequately described applying the principle of overload in the exercise prescription. This increases the likelihood that an adequate training stimulus was applied by ensuring the dose of exercise was either greater than self-reported levels of physical activity or prescribed based on fitness levels measured at baseline. Several publications have shown the safety of maximal exercise testing to measure aerobic capacity and muscular strength in women diagnosed with breast cancer,78–80 which can be used for prescribing adequate workloads. We advocate for the use of these methods whenever possible. The utility of predictive equations or submaximal exercise testing for aerobic and resistance exercise created for the general populations is uncertain in women after a breast cancer diagnosis due to changes in cardiovascular, muscular and metabolic parameters due to breast cancer and its treatment.81 82 However, these equations or tests could be similarly useful and more practical in community settings. Continued research is needed in this area to understand the best method of exercise prescription in this population.
Approximately two-thirds of studies adequately reported application of the principle of initial values in the exercise prescription. This was typically achieved by excluding participants who were already highly active at baseline. Despite reported low levels of physical activity in both women diagnosed with breast cancer, and the general population, researchers cannot assume that all participants are sedentary at baseline. Those who agree to participate in exercise trials may already be more active, and prescribing a lower dose of exercise than what participants are already doing can result in detraining, lowering the overall estimate of the effect of exercise. Studies including those with the lowest initial values have the greatest potential to show the benefits of exercise. In studies that include participants with higher initial values, exercise prescription should be adjusted to ensure a training stimulus is offered to all participants. Future studies could include additional analysis to understand the influence of baseline values on training responses, so that realistic timelines for training and expectations of benefits are appropriately translated.
Diminishing returns and reversibility were more commonly reported in the newly identified studies. This is due to the publication of studies of longer durations, and those that incorporated a follow-up assessment after the intervention had ended. An important next step in the field of exercise oncology is to understand the long-term effects of exercise, and what ‘maintenance-dose’ of exercise is sufficient to sustain the benefits seen in short-term interventions. Unfortunately, many of the newly included studies were unclear in the application of diminishing returns and reversibility reported. Either interim or follow-up measures were reported, but they were not examined in the context of the exercise prescribed or adhered to. Future studies that report interim measures during an intervention or follow-up measures after an intervention is complete should also report what dose of exercise was prescribed and/or completed during those periods so that the patterns of change over time can be understood.
Duration of exercise and some indication of the average exercise intensity are necessary to reproduce findings and understand the minimum dose of exercise needed to elicit positive benefits. More studies in the current review were unclear in their reporting of intensity than studies in the original review (28 vs 3%). Fewer studies adequately reported the actual frequency of exercise completed (58 vs 82%). Reporting of the exercise completed by participants is needed for contextualising study findings, and understanding what exercise dose is feasible for participants to complete in future studies and in community settings. Variations in adherence to trials with similar exercise prescriptions may also help to explain some of the variation in results seen across different trials. Researchers may report adherence in terms of an average frequency, intensity and duration of exercise by mode, as well as the proportion of participants who met the exercise prescription. One study reported prescribing a higher than desired frequency of exercise in anticipation that most participants will not adhere to that target.54 While we do not necessarily advocate for this approach, as it may increase the likelihood of overtraining by some participants, understanding the proportion of adherence to different prescriptions will help to design interventions that are both physiologically beneficial but also acceptable to participants.
Word and page limits in scientific journals limit the amount of information that can be included, which may contribute to information being reported incompletely. We did not contact authors of studies where an unclear or not reported were assigned. Therefore, some of the included trials may have adhered to some of the principles of exercise training, just not reported them. Reporting of the exercise prescription and adherence to the prescribed programme is essential for moving the field forward. Researchers conducting new studies can build on successful interventions or improve on interventions that failed to find significant improvements. Full reporting will also allow for interpretation of differences across studies and will assist in the development of future evidence-based practice guidelines and ultimately translation into community and clinical practice.
Recently, guidelines have been published for reporting of exercise programmes in academic research.83 We encourage authors of exercise studies in breast cancer survivors to follow the Consensus on Exercise Reporting Template, including the frequency, intensity, duration and type of exercise prescribed under section 13, ‘When, How Much’, and exercise actually completed under section 16, ‘How Well: Planned, actual’. Several articles included in this review also provide excellent examples of how the exercise prescriptions can be reported in either text35 73 or table format26 39 45 for both aerobic26 35 39 73 and resistance45 73 exercise.
Since the June 2009 round table discussion that led to the publication of the American College of Sports Medicine’s exercise guidelines for cancer survivors,84 there have been at least 50 RCTs of exercise in breast cancer survivors (reviewed here), plus more that did not meet our eligibility criteria. New literature may now be sufficient to make more specific recommendations for women diagnosed with breast cancer—it might be time to revisit these guidelines. Reviewing the strength of the evidence on specific exercise prescriptions to elicit changes in various outcomes of interest is beyond the scope of this review. However, this review may be helpful in identifying trials that report the attention to the principles of exercise training in their study design and fully report the exercise prescription and exercise completed so that the most robust literature can be given appropriate, and potentially preferential, consideration when updating the existing exercise guidelines.
Conclusions
In conclusion, while the evidence for the benefits of exercise in women diagnosed with breast cancer continues to grow, no studies of exercise in women with breast cancer attended to all key principles of exercise training, or reported all components of the exercise prescription in the methods, or adherence to the prescribed intervention in the results. In order to move this growing evidence into practice, we call for best practices for exercise prescription, as well as full reporting of the exercise prescription used and adherence to the prescribed exercise programme.
What are the findings?
No studies have reported all components of the exercise prescription in their methods, or adherence to the prescribed intervention in their results.
The exercise training principles of specificity and initial values are most often applied, while reversibility, diminishing returns and progression are included by <30% of published studies.
More recent studies have attempted to use reversibility and diminishing returns in their exercise prescription, but there have been no other improvements in use of exercise training principles or reporting since 2010.
Acknowledgments
None
References
Footnotes
Contributors KMW-S and KLC conceptualised the original review. SN-S conceived the update. SN-S and KAB conducted the literature search, screened and appraised articles. SN-S drafted the manuscript with input and revisions from KMW-S, KAB and KLC. All authors approved the final manuscript.
Funding SN-S is supported by a postdoctoral fellowship from the Canadian Institutes of Health Research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.