Article Text

Abstract
Although premature ventricular beats (PVBs) in young people and athletes are usually benign, they may rarely mark underlying heart disease and risk of sudden cardiac death during sport. This review addresses the prevalence, clinical meaning and diagnostic/prognostic assessment of PVBs in the athlete. The article focuses on the characteristics of PVBs, such as the morphological pattern of the ectopic QRS and the response to exercise, which accurately stratify risk. We propose an algorithm to help the sport and exercise physician manage the athlete with PVBs. We also address (1) which athletes need more indepth investigation, including cardiac MRI to exclude an underlying pathological myocardial substrate, and (2) which athletes can remain eligible to competitive sports and who needs to be excluded.
- athlete’s heart
- sudden cardiac death
- arrhythmias
- ectopic beats
- premature ventricular contraction
- eligibility
- disqualification
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- athlete’s heart
- sudden cardiac death
- arrhythmias
- ectopic beats
- premature ventricular contraction
- eligibility
- disqualification
Introduction
Adolescents and young adults engaged in competitive sports activity have a risk of sudden cardiac death (SCD) that is three times higher than their sedentary counterparts.1 ,2 Ventricular arrhythmias (VAs), including premature ventricular beats (PVBs), on an athlete’s ECG or during an exercise ECG test may warn of increased arrhythmic risk during sports participation.3 As a consequence, PVBs on an athlete’s ECG warrant an accurate clinical and secondary investigation that usually includes 24-hour ambulatory ECG monitoring, maximal exercise testing and echocardiography to rule out the presence of a cardiac disease.4 5
Some arrhythmic substrates, such as the apical variant of hypertrophic cardiomyopathy, segmental arrhythmogenic cardiomyopathy or non-ischaemic left ventricular scar, may be missed by routine echocardiography and detectable only by cardiac magnetic resonance (CMR) with late gadolinium enhancement (LGE).6–8 This imaging test is time-consuming, expensive and not widely available, and thus it cannot be proposed for systematic evaluation of athletes with PVBs.
This review addresses the prevalence, clinical meaning and assessment of PVBs in the athlete. The article focuses on the characteristics of PVBs, such as the morphological pattern of the ectopic QRS and the response to exercise, which are key features for risk stratification. An algorithm of clinical management of the athlete with PVBs is provided, which aims to guide sports physicians during decision-making for a more indepth work-up including CMR to exclude an underlying pathological myocardial substrate. Implications for eligibility to competitive sports activity according to current guidelines are also addressed.
Is there a greater prevalence of PVBs in athletes?
PVBs are a common ECG finding in the general population and are recorded in up to 75% of healthy individuals undergoing 24-hour ambulatory ECG monitoring, with a prevalence that increases with ageing.9–12 Whether PVBs are more frequently observed in athletes than in their sedentary counterparts is unclear.
In a group of 355 elite Italian athletes with VA and no underlying structural abnormalities, arrhythmias tended to decrease after detraining and the follow-up was uneventful, suggesting that PVBs may be a consequence of the structural and neuroautonomic remodelling of the athlete’s heart.13
On the other hand, most studies comparing the prevalence of VAs on 24-hour ambulatory ECG monitoring in healthy athletes versus sedentary individuals demonstrated that only a minority of athletes exhibit frequent or complex VAs, with a prevalence that did not differ with that of their sedentary counterparts14–21 (table 1).
Summary of studies that compared the ventricular arrhythmic burden at 24-hour ambulatory ECG monitoring in apparently healthy athletes and sedentary controls
Which characteristics of PVBs confer a worse prognosis?
Burden
Holter monitoring is a key test for the evaluation of the ‘arrhythmic burden’, that is, the number of PVBs during 24 hours and their tendency to form couplets, triplets or non-sustained ventricular tachycardia (VT). More than 500 PVBs per 24 hours on Holter monitoring may signal risk of SCD and is a diagnostic criterion for arrhythmogenic cardiomyopathy.22 23 However, frequent PVBs are associated with a benign prognosis if an underlying disease and tachycardia-mediated left ventricular dysfunction are excluded.11 24–28 Ectopic foci located in the right or left ventricular outflow tract or in the fascicles of the left bundle branch may give rise to very frequent PVBs (>10 000/24 hours) that are usually isolated and occur in the absence of a pathological myocardial substrate.24 25
On the other hand, systematic investigation of SCD in young people and athletes from the Veneto region of Italy and retrospective evaluation of the ECG tracings of SCD victims obtained during life demonstrated that the presence of a single PVB on basal preparticipation ECG may be a warning sign of an underlying heart disease at risk of SCD in an otherwise asymptomatic individual.29 Current consensus standards for ECG interpretation in athletes suggest that two or more PVBs on a resting ECG are required to initiate additional investigation in an asymptomatic athlete, but even one PVB, particularly with an ‘at-risk’ QRS morphology, may be a significant finding.30
Complex PVBs may reflect the propensity of the arrhythmia to become sustained and potentially malignant, and hence require a more indepth clinical evaluation of the underlying substrate. Elite athletes with frequent (>2000/24 hours) PVBs and non-sustained VT were reported to have a higher probability of an underlying heart disease compared with athletes with less complex PVBs.13
Morphology
The assessment of the morphology of the ectopic QRS complex on the ECG helps to identify the anatomical origin of the VA (table 2). Idiopathic PVBs are characterised by the absence of an underlying structural heart disease and a favourable prognosis and exhibit distinctive ECG patterns.31 32
Morphology and characteristics of premature ventricular beats that may be encountered in clinical practice
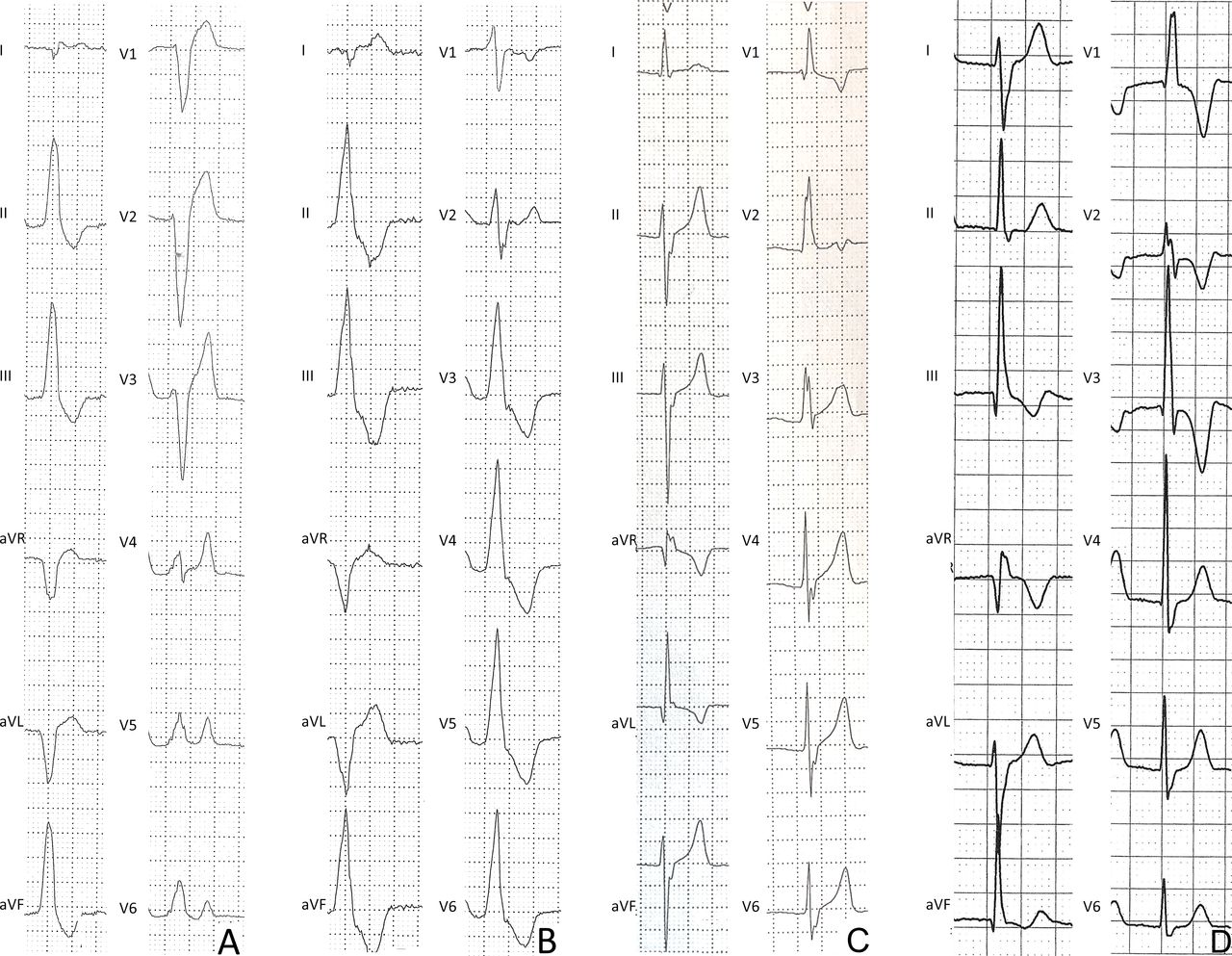
The most common form of idiopathic PVBs shows an ECG pattern of the left bundle branch block (LBBB) with inferior QRS axis (also referred to as an ‘infundibular’ pattern). An LBBB pattern is recognised by a negative QRS complex in lead V1, while a negative QRS complex in lead aVL and positive QRS in the inferior leads (II, II, aVF) denote an inferior axis. When the ectopic QRS becomes positive beyond V3, the origin of the arrhythmia is usually the right ventricular (RV) outflow tract (figure 1A). A similar morphology but with small R-waves in V1 and earlier precordial transition (the ectopic QRS complex becomes positive by V2 or V3) often indicates the PVB origin from the left ventricular (LV) outflow tract (figure 1B). On Holter monitoring, the ectopic beats usually manifest as frequent isolated PVBs and rare couplets, but occasionally triplets or runs of non-sustained VT may also occur. The ventricular ectopy is usually more frequent during the day than at night or following a period of exercise and is transiently suppressed by sinus tachycardia. Characteristically, during stress testing, idiopathic PVBs from the RV or LV outflow tract decrease or disappear at peak of exercise and reappear during recovery.33
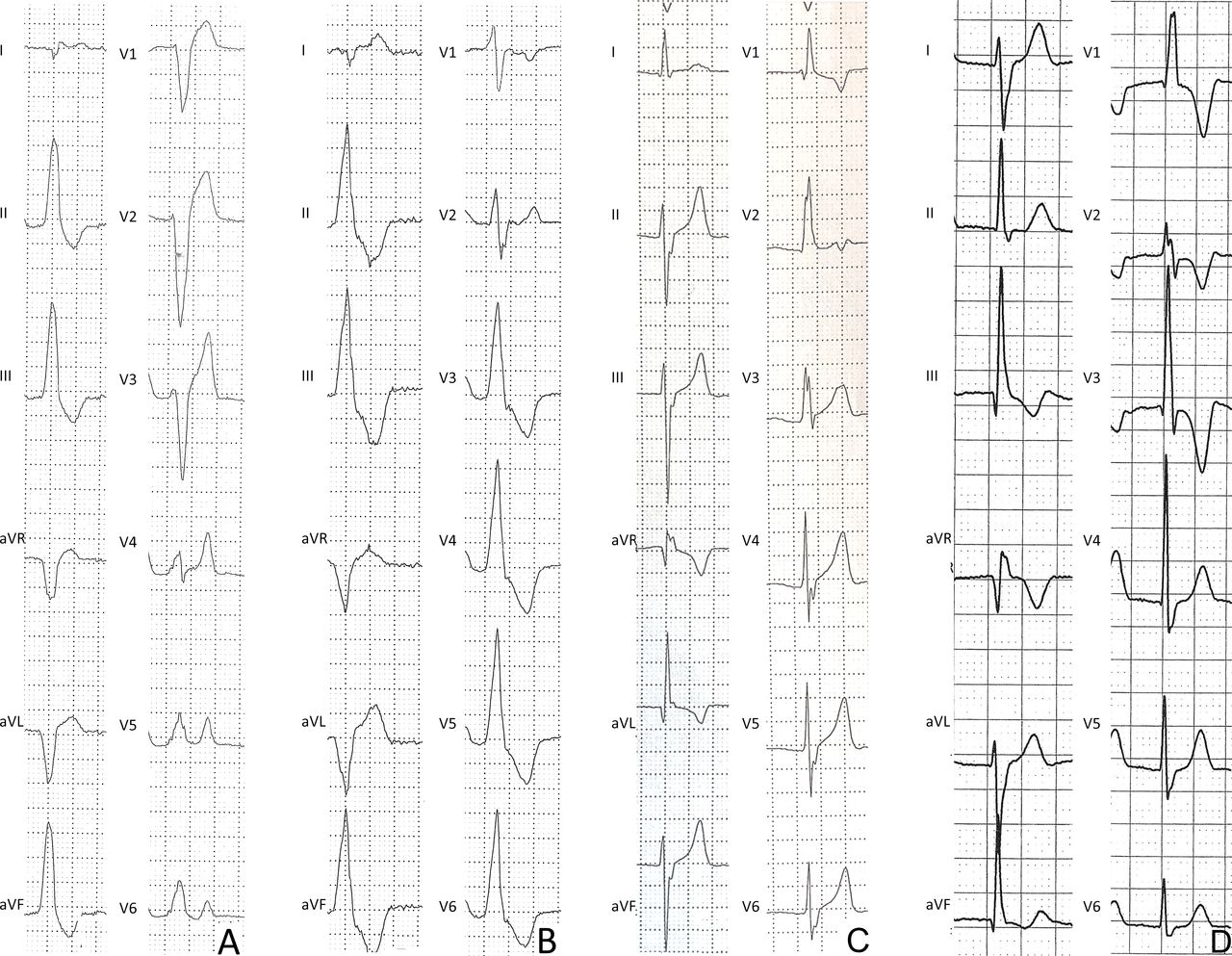
Morphologies of common premature ventricular beats in healthy athletes. Premature ventricular beat with negative QRS complex in V1 (left bundle branch block-like), precordial S/R transition in V4 and inferior QRS axis in the limb leads consistent with origin from the right ventricular outflow tract (A). Premature ventricular beat with negative QRS complex in V1 (left bundle branch block-like pattern), precordial S/R transition in V2/V3 and inferior QRS axis in the limb leads, suggestive of the origin from the left ventricular outflow tract (B). Premature ventricular beat with a relatively narrow QRS (120–130 ms) and typical right bundle branch block/superior axis configuration, suggestive of the origin from the posterior fascicle of the left bundle branch (C). Premature ventricular beat with a relatively narrow QRS (120–130 ms) and typical right bundle branch block/inferior axis configuration, suggestive of the origin from the anterior fascicle of the left bundle branch (D).
Another pattern consistent with idiopathic and benign PVBs is the ‘fascicular’ pattern, characterised by a typical right bundle branch block (RBBB), superior QRS axis morphology and QRS duration <130 ms (figure 1C). A typical RBBB is recognised by an rSR′ pattern in lead V1 and an S-wave wider than R-wave in lead V6, while a superior axis is denoted by a negative QRS in the inferior leads. This pattern features an RBBB with left anterior fascicular block and indicates the origin of the PVBs from the left posterior fascicle of the left bundle branch. Rarely, PVBs originate from the left anterior fascicle and show a typical RBBB and inferior axis morphology featuring an RBBB with left posterior fascicular block (figure 1D).34 Less common sources of LV idiopathic PVBs include the mitral valve annulus and the papillary muscles. In both cases, PVBs show a wide (>130 ms) QRS with an ‘atypical’ RBBB pattern (positive QRS complex in V1 but not resembling a typical RBBB) and variable QRS axis.35 This pattern can be similar to that occurring in the context of structural heart disease and thus requires a more comprehensive evaluation.
A study showed that in the majority of competitive athletes (68%) with PVBs at exercise testing in the absence of an underlying disease, the ectopic QRS morphology was consistent with origin from the RV outflow tract.36 In 15%, PVB morphology suggested a fascicular origin and in 9% a LV outflow tract origin. Other morphologies such as LBBB/superior axis or RBBB/QRS >130 ms were rare. These findings were in agreement with another study reporting that 73% of athletes with PVBs at preparticipation evaluation showed an LBBB morphology of the ectopic QRS, 21% had fascicular PVBs, and only 6% had PVBs with an RBBB/QRS >130 ms morphology.27 Similarly, in a cohort of young athletes with PVBs referred for further investigations, the majority showed an ectopic QRS morphology suggestive of an infundibular origin.37 When 12-lead 24-hour Holter monitoring was used to compare the burden and QRS morphology of VAs in 286 young athletes and 143 sedentary controls, only 6 (2.1%) athletes showed >500 PVBs/day and 5 of them had an infundibular or fascicular morphology of the ectopic QRS.20 Similarly, in a study on 136 middle-aged endurance athletes, 8 of 10 with >500 PVBs/day exhibited an infundibular or fascicular morphology.21
These findings indicate that frequent PVBs in the athlete most often show either an infundibular (LBBB/inferior axis) pattern or a fascicular (typical RBBB and QRS <130 ms) morphology. Both types of PVBs arise from an automatic ventricular focus and usually occur in the absence of underlying structural heart disease.33 34
On the contrary, other morphologies of PVBs such as LBBB/intermediate or superior axis or RBBB/intermediate or superior axis and wide QRS are uncommon in the athlete, and when present are usually less numerous, complex (repetitive, polymorphic, short-coupled) and/or exercise-induced and may be associated with an underlying myocardial disease. Studies on athletes undergoing CMR for evaluation of VAs demonstrate that PVBs with an RBBB-like morphology and wide QRS (>130 ms) more often predict myocardial lesions (particularly non-ischaemic LV myocardial scar as evidenced by LGE).8 20 38 39
Because of the importance of the morphology of the ectopic QRS in guiding the diagnostic work-up and risk assessment, all efforts should be made to accurately characterise the ectopic QRS morphology on a 12-lead resting ECG, exercise test, or 12-lead 24-hour ambulatory ECG monitoring.
Coupling interval
Regardless of QRS morphology, short-coupled PVBs, or PVBs that are superimposed on the preceding T-wave (peak or earlier), should be regarded as a warning sign for myocardial electrical instability as a consequence of early/inhomogeneous ventricular repolarisation which may predispose to ventricular fibrillation in the absence of structural heart disease (ie, idiopathic ventricular fibrillation)40 (figure 2). Athletes with short-coupled PVBs, particularly when associated with the ECG pattern of inferolateral early repolarisation with prominent terminal QRS slurring, should be referred to a specialist for evaluation by electrophysiological study.

Coupling interval of premature ventricular beats. Normal coupling interval in a common (infundibular) pattern of premature ventricular beats (A). Short-coupled premature ventricular beats and terminal QRS slurring in the inferolateral leads followed by a flat ST segment in an athlete with idiopathic ventricular fibrillation (B).
Relation to exercise
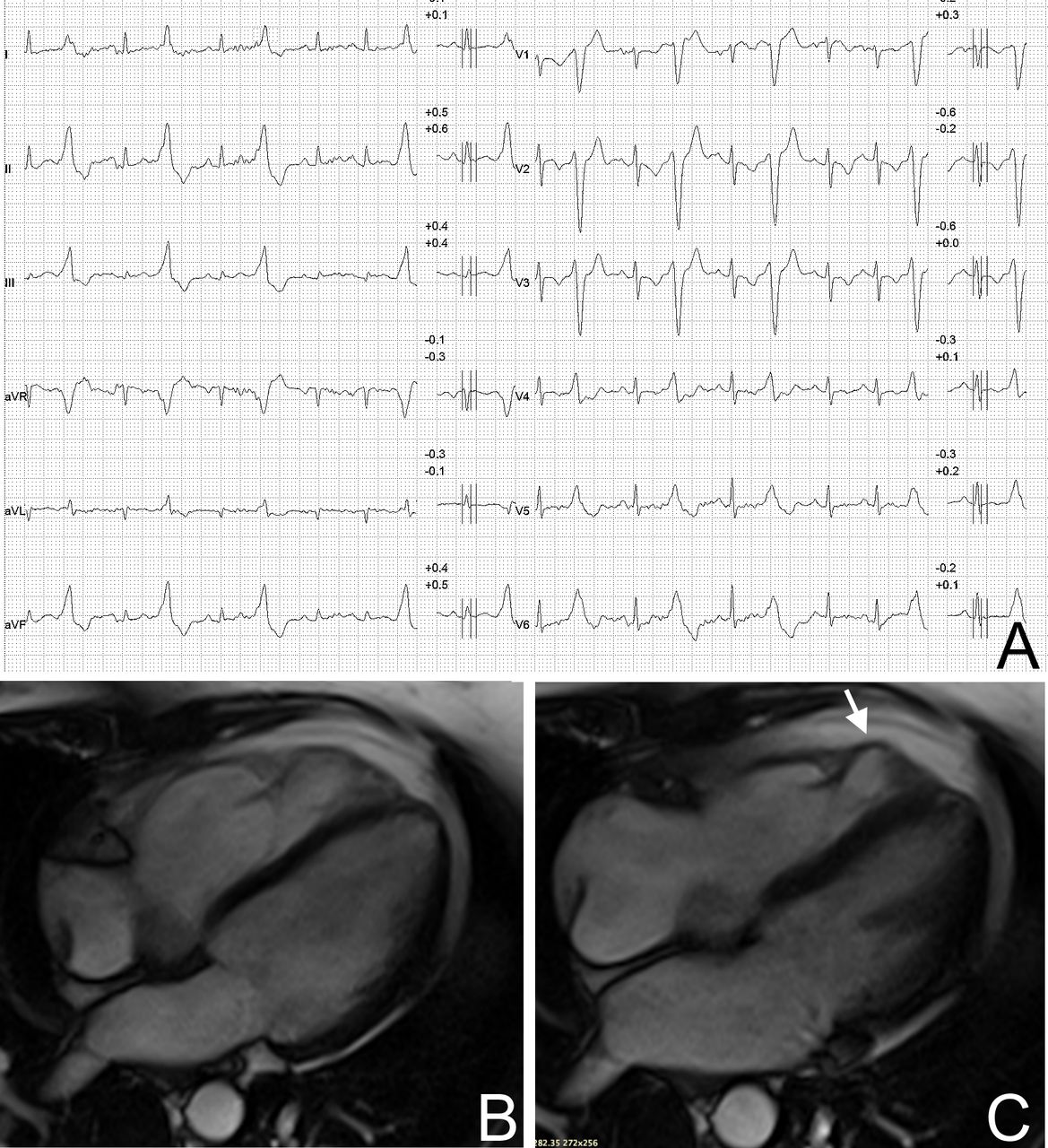
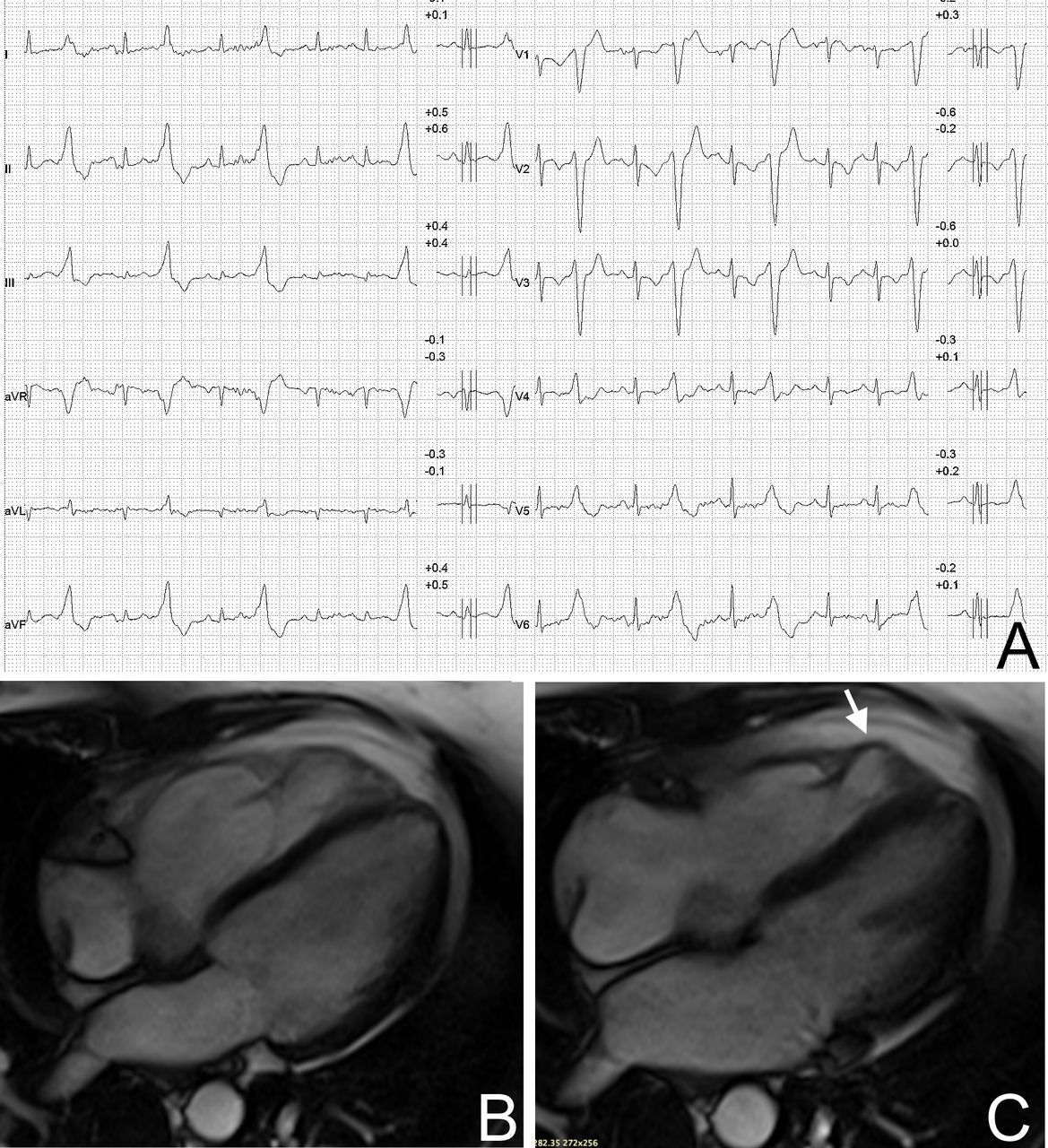
PVBs induced by exercise raise clinical warning because VAs associated with heart diseases such as cardiomyopathy, myocarditis and ion channel diseases are often worsened by adrenergic stimulation.1 8 20 38 41–43 On the other hand, PVBs that become less frequent or disappear with increasing exercise load are usually idiopathic and benign VAs and often have an infundibular origin (ie, from the RV or LV outflow tract).44 45 Compared with resting ECG, exercise testing has the potential to increase the diagnostic sensitivity for identification of clinically silent arrhythmogenic heart diseases because of its ability to induce adrenergic-dependent VAs.46 In a cohort of athletes who underwent CMR for evaluation of PVBs, a higher prevalence of pathological myocardial substrates was found among athletes with exercise-induced PVBs compared with those with exercise-suppressed VAs.38 In particular, exercise-induced complex VAs with an RBBB morphology and QRS >130 ms were the strongest predictors of pathological findings on CMR (OR=5.3) (figure 3). Therefore, clinicians should evaluate the inducibility of PVBs and how the PVBs respond to maximal exercise testing when aiming to identify athletes with an arrhythmic myocardial substrate. In particular, PVBs occurring (or persisting) at high workload and/or exercise-induced complex PVBs may signal underlying heart disease.
Premature ventricular beats with a right bundle branch block-like pattern of the ectopic QRS and underlying left ventricular myocardial disease. Frequent and coupled premature ventricular beats with a right bundle branch block/superior axis QRS morphology during exercise testing in a 42-year-old martial arts athlete (A). Long-axis view (B) and short-axis view (C) of postcontrast cardiac magnetic resonance sequences showing a subepicardial/mid-myocardial ‘stria’ of late gadolinium enhancement involving the anterolateral, lateral and inferolateral segments of the left ventricular wall (arrows). Modified from Zorzi et al.8
Exercise-induced PVBs with multiple morphologies of the ectopic QRS, especially with beat-to-beat alternating morphologies (the so called ‘bi-directional’ pattern), are associated with a high risk for effort-related SCD. Indeed, this arrhythmic pattern may be expression of an inherited ion channel disease, catecholaminergic polymorphic VT, which predisposes to adrenergic-dependent VAs which can degenerate into ventricular fibrillation.43
Response to detraining
A previous study demonstrated that in the majority of athletes with PVBs and no underlying heart disease, the arrhythmia decreased or disappeared after a period of 3–6 months of detraining. While athletes with a persistence of PVBs were deemed not eligible for competitive sports, those who had a reduction in the burden of PVBs after detraining were allowed to resume competitive sports activity and had an uneventful long-term follow-up.36 These findings suggest that the prognosis of exercise-induced PVBs that are unrelated to a structural heart disease and resolve with detraining is favourable.
However, other studies showed conflicting results and called into question the prognostic value of detraining athletes with PVBs. Biffi et al 47 demonstrated that healthy Olympic athletes with frequent PVBs most often show reduction or disappearance of the arrhythmia with detraining. This finding has been interpreted as support that PVBs are part of the physiological spectrum of electrical and structural adaptive changes of the heart to physical exercise (the so-called ‘athlete’s heart’).On the other hand, the same authors in subsequent studies found that (1) retraining athletes did not cause PVBs to relapse48 and (2) there was no correlation between the arrhythmic burden and the degree of training-induced left ventricular hypertrophy.49 Delise et al 50 did not find any differences in the behaviour of VA (persistence or reduction) during follow-up in a group of athletes who continue training versus a group of athletes who interrupted sport activity.
How to evaluate the athlete with PVBs
Table 3 classifies PVBs in the athlete based on number, morphological pattern, complexity, response to exercise and clinical manifestations. The table provides criteria to distinguish ‘common’ and benign PVBs from ‘uncommon’ PVBs that are associated with a higher risk of cardiac pathology. This approach is pivotal to the appropriate management of an athlete with PVBs to guide arrhythmic risk stratification and the diagnostic work-up to confirm (or exclude) underlying heart disease.
Classification and risk stratification of premature ventricular beats in the athlete
The presence of PVBs on an athlete’s resting ECG or during exercise testing does not lead to a diagnosis of a heart disorder in itself, but it should launch a cascade of further cardiovascular evaluations to confirm (or exclude) cardiac pathology. The international criteria for ECG interpretation in athletes suggested that further evaluation is warranted when ≥2 PVBs are recorded on a resting 12-lead ECG.30 However, even a single PVB may deserve attention especially in the presence of one or more of these five features: (1) positive family history of premature SCD or cardiomyopathy, (2) relevant symptoms, (3) associated ECG abnormalities, (4) uncommon PVB morphology (table 2) and (5) short coupling interval.
Electrocardiography
The ECG is an essential part of the evaluation of athletes with PVBs because concomitant repolarisation/depolarisation abnormalities may provide important information on a possible underlying cardiomyopathy or channelopathy.3 30 51
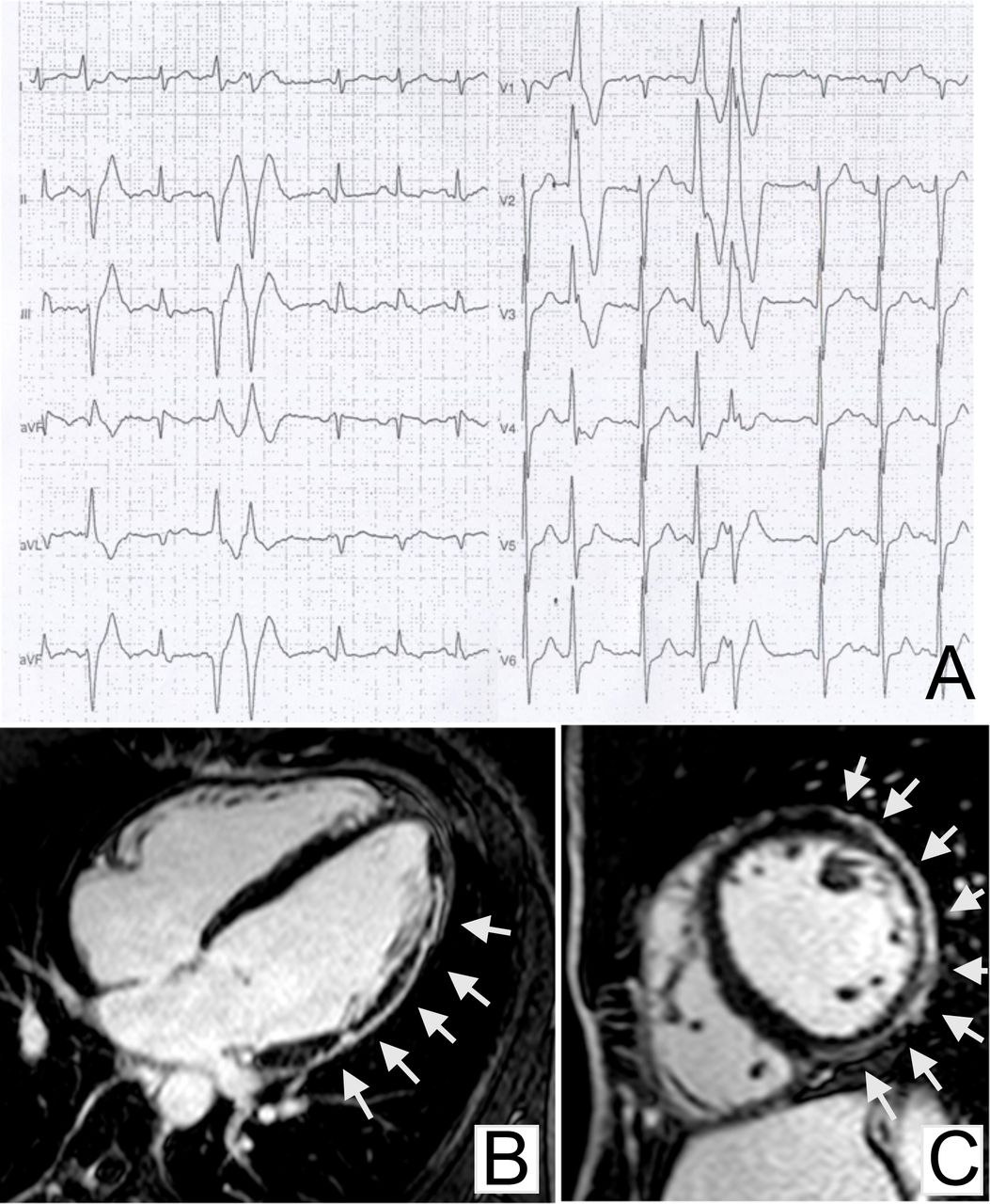
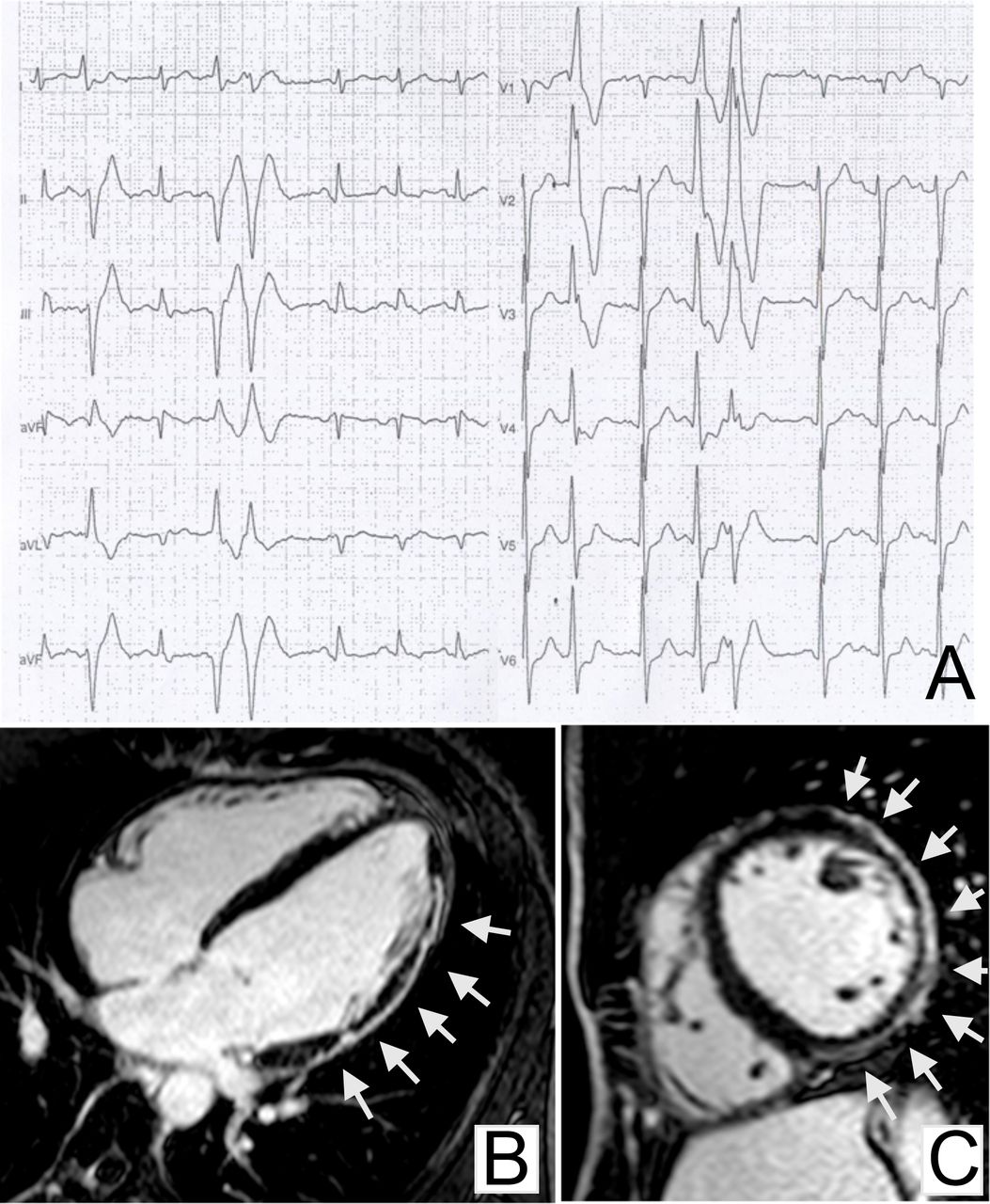
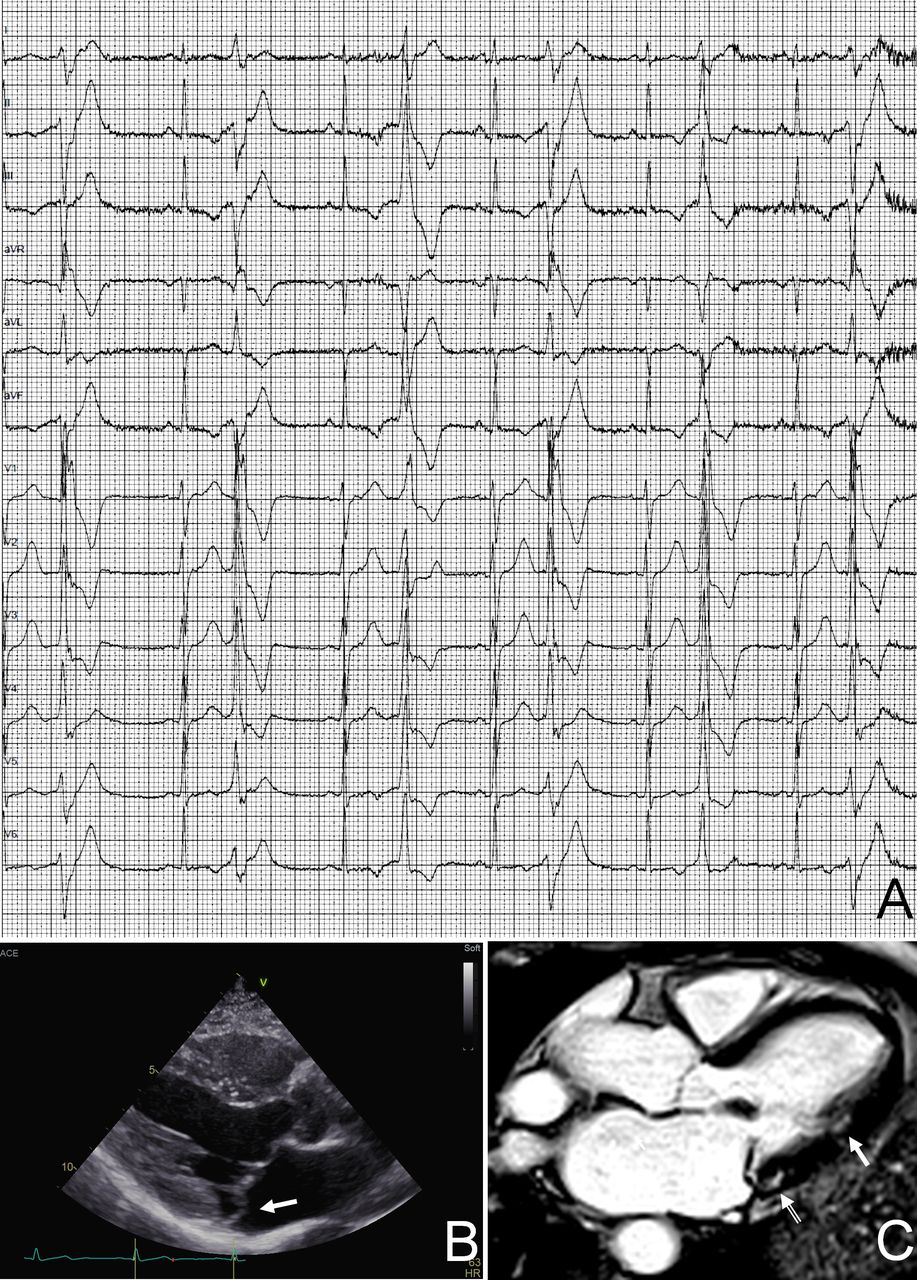
The most relevant ECG abnormalities which are consistent with an at-risk heart muscle disorder include repolarisation abnormalities such as T-wave inversion and ST segment depression, pathological Q-waves, intraventricular conduction disturbances, ventricular pre-excitation and a long QT interval. These ECG abnormalities are classified by current recommendations for interpretation of the athlete’s ECG as abnormal and training-unrelated ECG findings that warrant additional investigation to exclude myocardial disease.3 30 51 The association between a PVB with a LBBB morphology and other ECG abnormalities such as T-wave inversion, prolonged S-wave upstroke (≥55 ms from the nadir of the S-wave to the end of the QRS complex in leads V1–V3) or a epsilon wave (small positive deflection or notch between the end of the QRS complex and onset of the T-wave in leads V1–V3) in the non-ectopic beats is highly suggestive of arrhythmogenic cardiomyopathy22 52–54 (figure 4). On the other hand, PVBs with an RBBB pattern >130 ms and negative T-waves in the left precordial leads (V5–V6) in the non-ectopic beats should raise the suspicion of a LV myocardial disease, such as dilated cardiomyopathy, non-ischaemic LV scar (figure 3), hypertrophic cardiomyopathy, left-dominant arrhythmogenic cardiomyopathy or arrhythmic mitral valve prolapse (figure 5).8 29 55 Athletes with PVBs and concomitant repolarisation/depolarisation abnormalities require an indepth cardiovascular evaluation aimed to confirm (or exclude) such heart muscle diseases.
Premature ventricular beats with a left bundle branch block-like pattern of the ectopic QRS and underlying right ventricular myocardial disease. Premature ventricular beats with a left bundle branch block/intermediate axis pattern, associated with ECG abnormalities (low QRS voltages in the limb leads and negative T-waves in V1–V3 in non-ectopic beats), which increased during exercise testing in a 34-year-old female runner (A). Cine cardiac magnetic resonance sequences (four-chamber view) revealed right ventricular dilation with hypertrabeculation (diastolic frame) (B) and dyskinesia (arrow) of the right ventricular free wall (systole frame) consistent with arrhythmogenic cardiomyopathy (C).

Premature ventricular beats in an athlete with arrhythmic mitral valve prolapse. Premature ventricular beats with a right bundle branch block morphology and variable QRS axis, suggesting multiple ectopic foci in the left ventricular myocardium (A). Echocardiography (long-axis parasternal view) showing thickened and prolapsing mitral valve leaflets (arrow) (B). Postcontrast cardiac magnetic resonance sequence (apical four-chamber view) showing potentially arrhythmogenic areas of myocardial fibrosis/late gadolinium enhancement which are localised behind the posterior leaflet of the mitral valve (open arrow) and at the implant of the posterolateral papillary muscle (arrow) (C).
Exercise testing
Exercise testing is part of the first-line evaluation of athletes with PVBs. It allows assessment of the behaviour of PVBs with increasing workload and other abnormal findings suggestive of an underlying cardiac disease, such as ST segment changes, abnormal blood pressure response to exercise or an impaired exercise capacity. Exercise testing in the athlete should not be stopped at 85% of the theoretical maximal heart rate but continued until exhaustion in order to increase the test sensitivity of unmasking adrenergic-dependent PVBs or myocardial ischaemia occurring at high workload.
Echocardiography
Echocardiography represents the first test for investigating a possible structural heart disease in athletes with PVBs. Echocardiography aims to assess the systolic function (both global and regional), the diastolic filling pattern and ventricular wall thickness and chamber size, as well as to evaluate for wall motion abnormalities suggestive of ischaemic heart disease, valvular abnormalities, congenital heart diseases and cardiomyopathies. Echocardiography is also the basal screening modality for characterisation of the coronary artery take-off from the aorta and offers the potential to detect congenital coronary artery anomalies which are leading causes of ischaemia-induced VAs and SCD in the athlete.56 Zeppilli et al 57 and Pelliccia et al 58 demonstrated the feasibility of echocardiographic imaging of the origin of coronary arteries in the vast majority of young athletes who usually have an optimal ultrasound window with excellent image quality.
However, echocardiography shows significant limitations in the evaluation of athletes with PVBs due to its inability to detect some conditions potentially associated with SCD during sports such as intramyocardial course of coronary arteries, atherosclerotic coronary artery stenosis, apical hypertrophy or segmental subepicardial-mediomural myocardial fibrosis.
Cardiac magnetic resonance
CMR provides additional diagnostic value to echocardiography in athletes with PVBs.39 It allows accurate evaluation of cavity dimensions, wall thickness, global systolic function and regional wall motion abnormalities of both ventricles; in addition, it has the unique power to identify and quantify myocardial tissue abnormalities such as oedema, fatty infiltration or replacing-type fibrosis through LGE technique. It has been reported that contrast-enhanced CMR is able to identify the presence of a non-ischaemic LV scar, otherwise missed by echocardiography, in a sizeable proportion of athletes with apparently unexplained PVBs or repolarisation abnormalities.20 21 38 39 59 60 These scars are undetectable by wall motion analysis on echocardiography because they affect a segmental area of the ventricular musculature and spare the subendocardial wall layer that mostly contributes to myocardial thickening.61 As a consequence, CMR has become a key test for the evaluation of athletes with PVBs with high-risk morphological features on resting 12-lead ECG or exercise testing. CMR is also valuable when echocardiography is inconclusive, particularly if the ectopic QRS is wide (>130 ms) and shows an RBBB/superior axis pattern, which suggests origin from the inferolateral left ventricular wall. The probability to detect an underlying myocardial abnormality on CMR in athletes with PVBs is highest when they are complex and/or exercise-induced.38 According to current consensus standards for ECG interpretation in athletes, additional evaluation with CMR is also indicated in athletes with ≥2000 PVBs per 24 hours (regardless of the PVB morphology, complexity and response to exercise). This recommendation for CMR, which is merely based on the number of PVBs, may be out of date in light of more modern scientific perspectives on arrhythmic risk stratification in the athlete.
Summarising the evaluation
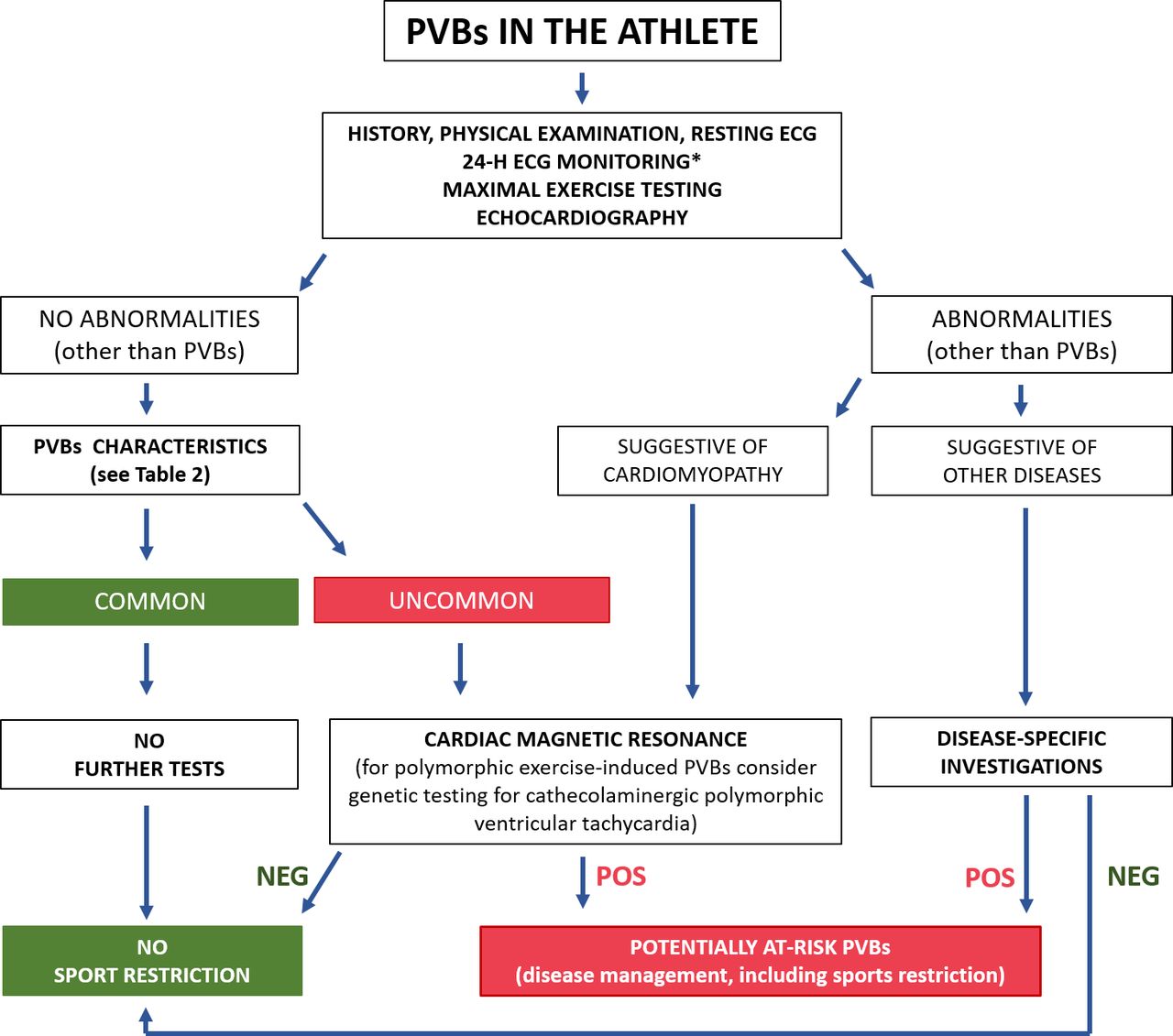
Figure 6 presents a practical flow chart for the clinical evaluation of the athlete with PVBs. First-line examinations include echocardiography, maximal exercise testing and 24-hour ambulatory ECG monitoring (ideally with a 12-lead configuration and inclusion of a training session). If these exams are abnormal, further tests depend on the suspected disease. The work-up of athletes with negative results of first-line examinations relies on the characteristics of PVBs. Athletes with a ‘common’ PVB pattern (table 3) do not require further testing and can be considered eligible for competitive sports, unless the clinical suspicion of disease remains high because of serious arrhythmic symptoms or a positive family history for SCD or cardiomyopathy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposed algorithm for evaluation of athletes with premature ventricular beats. *24-hour ECG monitoring should ideally have 12-lead configuration and include a training session. NEG, negative; POS, positive; PVBs, premature ventricular beats.
Athletes with an ‘uncommon’ PVB pattern should undergo a contrast-enhanced CMR, regardless of symptoms or familial background or the results of first-line examinations, to rule out a concealed myocardial substrate at risk of malignant arrhythmic events during sports activity. Other examinations such as coronary CT or coronary angiography may be considered in selected middle-aged and senior athletes with exercise-induced PVBs and a high coronary risk score.
PVBs that occur during exercise testing and become complex with increasing workload may be a sign of catecholaminergic polymorphic VT whose definitive diagnosis (or exclusion) relies on molecular genetic testing for pathogenetic mutations of the ryanodinic receptor or calsequestrin genes.43
According to the proposed management flow chart of athletes with PVBs, further diagnostic evaluation with sophisticated (and costly) imaging tests or molecular genetic testing is limited to the small subset of athletes with ‘uncommon’ PVB characteristics, which may reflect a clinically concealed but potentially lethal heart disease, whose diagnosis may be missed by routine tests. On the contrary, recording most ‘common’ PVBs such as those with an ‘infundibular’ or ‘fascicular’ pattern should provide reassurance to continue to participate in competitive sports, provided that first-line examinations are normal, the athlete is asymptomatic and family history for inherited cardiac disease or premature SCD is negative. The use of this modern and detailed approach to PVB interpretation and the subsequent diagnostic work-up is expected to improve the cardiovascular care for athletes before participation in sports.
Implications for competitive sports eligibility
The presence of an underlying heart disease is a key prognostic factor and the most important determinant regarding eligibility recommendations for competitive sports activity for athletes with PVBs.
According to the 2015 recommendations of the American Heart Association and the American College of Cardiology, athletes with PVBs or couplets in the absence of structural heart disease should be considered eligible for all competitive sports. The recommended intensity of exercise is to remain under the threshold for the occurrence of arrhythmia-related symptoms such as presyncope, dizziness or dyspnoea. If at-risk cardiovascular disease is identified, only sports activities at low cardiovascular demand are allowed.5
The 2006 consensus document of the Working Group on Sports Cardiology of the European Society of Cardiology provided more strict criteria for eligibility and recommended to exclude from competitive sports activity athletes with >2000 PVBs/day and complex or exercise-induced PVBs even in the absence of an underlying structural heart disease, unless they disappear after 3–6 months of detraining.4 However, these recommendations appear out of date considering more recent scientific data on the morphology and clinical meaning of PVBs.
Conclusions
PVBs detected on the athlete’s ECG should prompt an accurate clinical work-up aimed to exclude relevant—potentially lethal—cardiac disease. All efforts should be made to record the 12-lead ECG pattern of PVBs to assess the morphology of the ectopic beats. First-line investigations include an echocardiogram and 24-hour Holter monitoring (with 12-lead configuration if available), which includes an exercise session and maximal exercise testing, to evaluate the tendency of the arrhythmia to worsen during effort. The decision for more indepth investigations, with particular reference to the use of CMR for excluding myocardial tissue abnormalities otherwise missed by echocardiography, should be guided by the assessment of morphology, complexity and exercise inducibility of PVBs rather than by their absolute number on 24-hour Holter monitoring.
What is already known
Premature ventricular beats (PVBs) in athletes warrant an accurate clinical work-up to exclude a heart disease at risk of sudden cardiac death during sports; however, in the majority of cases, PVBs are unrelated to an underlying pathological substrate (idiopathic).
What are the new findings
Differentiating between common idiopathic PVBs and potentially malignant arrhythmias should be based on multiple features (particularly the morphology of the ectopic QRS complex) rather than just the arrhythmic burden (number of PVBs) on 24-hour ECG monitoring.
If clinicians use the proposed algorithm for clinical work-up of athletes with PVBs (see figure 6), further diagnostic evaluation with sophisticated (and costly) imaging tests or molecular genetic testing will be limited to a very small subset of athletes with ‘uncommon’ PVB characteristics.
References
Footnotes
Contributors All authors contributed to writing and reviewing the manuscript.
Funding Supported by BIRD (Budget for Integrated Department Research Project) 2016–2018, University of Padova, Italy.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.