Article Text

Abstract
Objectives To identify common recommendations for high-quality care for the most common musculoskeletal (MSK) pain sites encountered by clinicians in emergency and primary care (spinal (lumbar, thoracic and cervical), hip/knee (including osteoarthritis [OA] and shoulder) from contemporary, high-quality clinical practice guidelines (CPGs).
Design Systematic review, critical appraisal and narrative synthesis of MSK pain CPG recommendations.
Eligibility criteria Included MSK pain CPGs were written in English, rated as high quality, published from 2011, focused on adults and described development processes. Excluded CPGs were for: traumatic MSK pain, single modalities (eg, surgery), traditional healing/medicine, specific disease processes (eg, inflammatory arthropathies) or those that required payment.
Data sources Four scientific databases (MEDLINE, Embase, CINAHL and Physiotherapy Evidence Database) and four guideline repositories.
Results 6232 records were identified, 44 CPGs were appraised and 11 were rated as high quality (low back pain: 4, OA: 4, neck: 2 and shoulder: 1). We identified 11 recommendations for MSK pain care: ensure care is patient centred, screen for red flag conditions, assess psychosocial factors, use imaging selectively, undertake a physical examination, monitor patient progress, provide education/information, address physical activity/exercise, use manual therapy only as an adjunct to other treatments, offer high-quality non-surgical care prior to surgery and try to keep patients at work.
Conclusion These 11 recommendations guide healthcare consumers, clinicians, researchers and policy makers to manage MSK pain. This should improve the quality of care of MSK pain.
- education
- effectiveness
- evidence based
- knowledge translation
- review
Statistics from Altmetric.com
What is already known
There is an urgent need to improve quality of care for musculoskeletal (MSK) pain conditions. This is a priority for clinicians, health care services, researchers and policy makers.
MSK pain in different body areas share similar features, and it may be possible to identify consistent overarching recommendations for assessment and management. Identifying common recommendations could be a useful way to improve care quality.
What are the new findings
We identified 11 consistent recommendations for MSK pain from high-quality clinical practice guidelines.
These could be used to improve MSK pain care by assessing care quality, for example, through audit, guide clinical decision making and identify clinician education needs.
Background
Musculoskeletal (MSK) pain conditions are the biggest cause of disability internationally1 and a major societal burden. One contributor to this burden, which is becoming increasingly recognised, is poor quality healthcare.2 Common healthcare problems for MSK pain are summarised in box 1 and include overuse of radiological imaging, surgery and opioids and a failure to provide patients with education and advice.
Summary of common problems in musculoskeletal (MSK) pain care
Overuse of imaging: between 25% and 42% of patients with low back pain (LBP) undergo imaging34 49 even though its routine use is discouraged and associated with harms. Sixty-nine per cent of general practitioners would refer patients for radiography at first presentation of rotator cuff tendinopathy and 82% would refer for ultrasound,35 despite findings demonstrating a poor relationship of imaging findings with symptoms.50
Overuse of surgery: knee arthroscopy for knee osteoarthritis is not recommended, yet its rate of use in the general US population increased from 3% to 4% from 2006 to 2010.51 The rates of shoulder subacromial decompression and rotator cuff repair52 have increased markedly even though surgical outcomes are comparable with exercise-based rehabilitation53 or sham surgery.54
Overuse of opioids: the efficacy of opioids for MSK pain management is questionable for both chronic55 and acute MSK pain conditions.42 The early use of opioids has been associated with poorer outcomes in LBP care.56 Although limiting the use of opioids is recommended,44 there is increasing use and an ‘epidemic’ of prescription opioid-related harms.57
Failure to provide education and advice: these are cornerstones of managing MSK pain conditions, yet only 20% of patients with LBP were given advice and education in a primary care setting.36
Evidence-to-practice gaps such as these are problematic because they waste healthcare resources and prevent patients from receiving appropriate care.
One of the ‘foundations of efforts to improve healthcare’,3 and to reduce evidence-to-practice gaps, are clinical practice guidelines (CPGs). CPGs are ‘statements that include recommendations intended to optimise patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options’.4 CPGs aim to improve care in a number of ways including: guiding clinical and patient decision making, acting as a standard of care, contributing to the development of clinical decision-making aids, informing all stakeholders about what constitutes best practice and guiding allocation of healthcare resources.4
Care that is more concordant with CPG recommendations results in better patient outcomes and lower costs.5 6 However, CPGs have been criticised because clinicians have difficulty using them. Issues include: a multitude of CPGs for the one condition or when they are voluminous documents that are not user-friendly,7 shortcomings in their quality such as when developers have undisclosed interests8 and a lack of transparency in their development.9 These problems are reflected in contemporary MSK pain CPGs. We recently reported that most MSK pain CPGs are of poor quality, use inconsistent terminology, over-represent some conditions (eg, low back pain [LBP] and osteoarthritis [ OA]) and under-representation other conditions (eg, cervical and thoracic spine pain) and fail to outline how to implement CPGs.10 Nevertheless, we also identified a small number of higher quality CPGs that could be used to inform healthcare for MSK pain conditions.
There is increasing recognition that MSK pain conditions in different body areas share similarities with respect to mechanisms, prognostic factors and clinical course.11 12 We were interested in whether there was common ground among CPGs for MSK pain. We were also interested in recommendations of care across MSK pain conditions that could potentially be applied across different levels of healthcare (ie, primary, tertiary and emergency). Therefore, we aimed to identify a common set of recommendations, obtained from contemporary high-quality CPGs, to assess and manage a broad range of MSK pain conditions.
Methods
We undertook a systematic review and synthesis of contemporary MSK pain CPGs for three of the most common MSK pain sites1 13: spinal pain (lumbar, thoracic and cervical spine), hip/knee pain including hip/knee OA and shoulder pain. The methods, including search strategy and selection processes, have been previously published.10 We selected CPGs published within 5 years of the original search date (since 2011). This cut-off date was selected as CPGs developed or updated within the previous 5 years better reflect up-to-date research evidence.4 The International Prospective Register of Systematic Reviews (PROSERO) registration number was CRD42016051653.
Our initial search included 34 CPGs that were developed between January 2011 and September 2016, for adults, in English, that reported development processes and were an original body of work. We excluded CPGs for: traumatic MSK pain, a single treatment modality (eg, surgery), traditional healing/medicine, specific disease processes (eg, inflammatory arthropathies) or those that were private for-profit and required payment to access. Article titles/abstracts were initially screened by one investigator (IL). Full text articles were then reviewed independently by two investigators (IL and LW). In August 2017, one investigator (IL) updated the search to identify any newly developed CPGs (online online supplementary file 1). The updated list was reviewed for completeness by all authors. Ten additional CPGs were included.
Supplemental material
Appraisal
Three investigators (IL, LW and RW) independently appraised the quality of CPGs using the Appraisal of Guidelines for Research and Evaluation II (AGREE-II) instrument. The AGREE II instrument is the most widely used generic instrument to measure the development and reporting of CPGs and has acceptably high construct validity (significant differences in 18 of 21 item scores between high/low quality CPGs)14 and reliability (item internal consistency between 0.64 and 0.89).14 15
Analysis
Using AGREE PLUS on the AGREE II website16 individual item scores, domain scores (scope and purpose, stakeholder involvement, rigour of development, clarity of presentation, applicability and editorial independence) and overall AGREE II scores were calculated for each CPG. AGREE PLUS calculates domain and overall scores as a percentage of the maximum possible score. Data were entered and analysed using SPSS (IBM SPSS Statistics V.24.0). Means and SD for each of the 23 items (1–7 scale) and six domain scores (percentage) were calculated. Inter-rater agreement was determined using intraclass correlation coefficients (ICCs) with a two-way random effects model for each domain and overall rating scores. We classified level of agreement as poor (ICC <0.40), fair (ICC 0.40–0.59), good (ICC 0.60–0.74) or excellent (ICC 0.75–1.00).17
Similarly to our previous study,10 we classified high-quality CPGs as those that had an AGREE II score equal to or greater than 50% of the maximum possible score in three domains: rigour of development (domain 3), editorial independence (domain 6) and stakeholder Involvement (domain 2). Our cut-off value of 50% is consistent with other studies, for example, ref 18, and the AGREE II developer’s recommendation that users decide on criteria for high and low quality CPGs based on the context of their work.16
CPG synthesis and identifying consistent recommendations
Synthesis consisted of four stages: extracting CPG recommendations, classifying recommendations, developing a narrative summary and, where possible, identifying consistent/common recommendations across MSK conditions. We also identified common recommendations within each MSK pain condition.
Extracting recommendations
Recommendations from high-quality CPGs were extracted independently by two reviewers (IL and either RW or LW). The evidence supporting each recommendation, as reported by each CPG, was recorded (eg, level of evidence and strength of recommendation). Extracted recommendations were compared and discrepancies resolved through discussion and consensus.
Classifying recommendations
Two reviewers independently classified the recommendations. In order to accommodate the varying terminology used in different CPGs, we classified recommendations as ‘should do’, ‘could do’, ‘do not do’ or ‘uncertain’ (table 1). CPGs for which there were no recommendations in a particular topic, that is, it was out-of-scope of the CPG and was not included, were not classified.
Recommendation classification, definition and examples of terminology for each classification
Narrative summary
A narrative summary was developed initially by one author (IL) and then reviewed and refined by all authors. This included grouping recommendations into theme areas. This was a deviation from our original PROSPERO protocol. In our original protocol, we proposed that two authors would independently undertake initial thematic analysis. The author group included three academic and practising physiotherapists (IL, RW and PPBO), two MSK pain researchers (CGM and LS), an indicator development researcher (LW), a specialist emergency care physician (YN), a senior medical officer in emergency medicine (MG) and a pain medicine physician (RG). We undertook multiple rounds of review with the summary refined following each round. For example, recommendations were reorganised with manual therapy and surgery initially classified under ‘physical therapies’ and ‘interventions’, and following review, classified under ‘passive interventions – non-invasive’ and ‘passive interventions – invasive’.
Identifying consistent recommendations
We identified consistent recommendations when there was a majority of ‘should do’ or ‘do not do’ recommendations and no conflicting recommendations in CPGs. Consistent recommendations applied across at least three MSK pain conditions. Additionally, we identified common recommendations within single MSK pain conditions based on the same criteria, a majority of ‘should do’ or ‘do not do’ recommendations in CPGs and no conflicting recommendations. We did not identify common recommendations when recommendations were weaker, that is, ‘could do’, ‘uncertain’ or there were conflicting recommendations.
Results
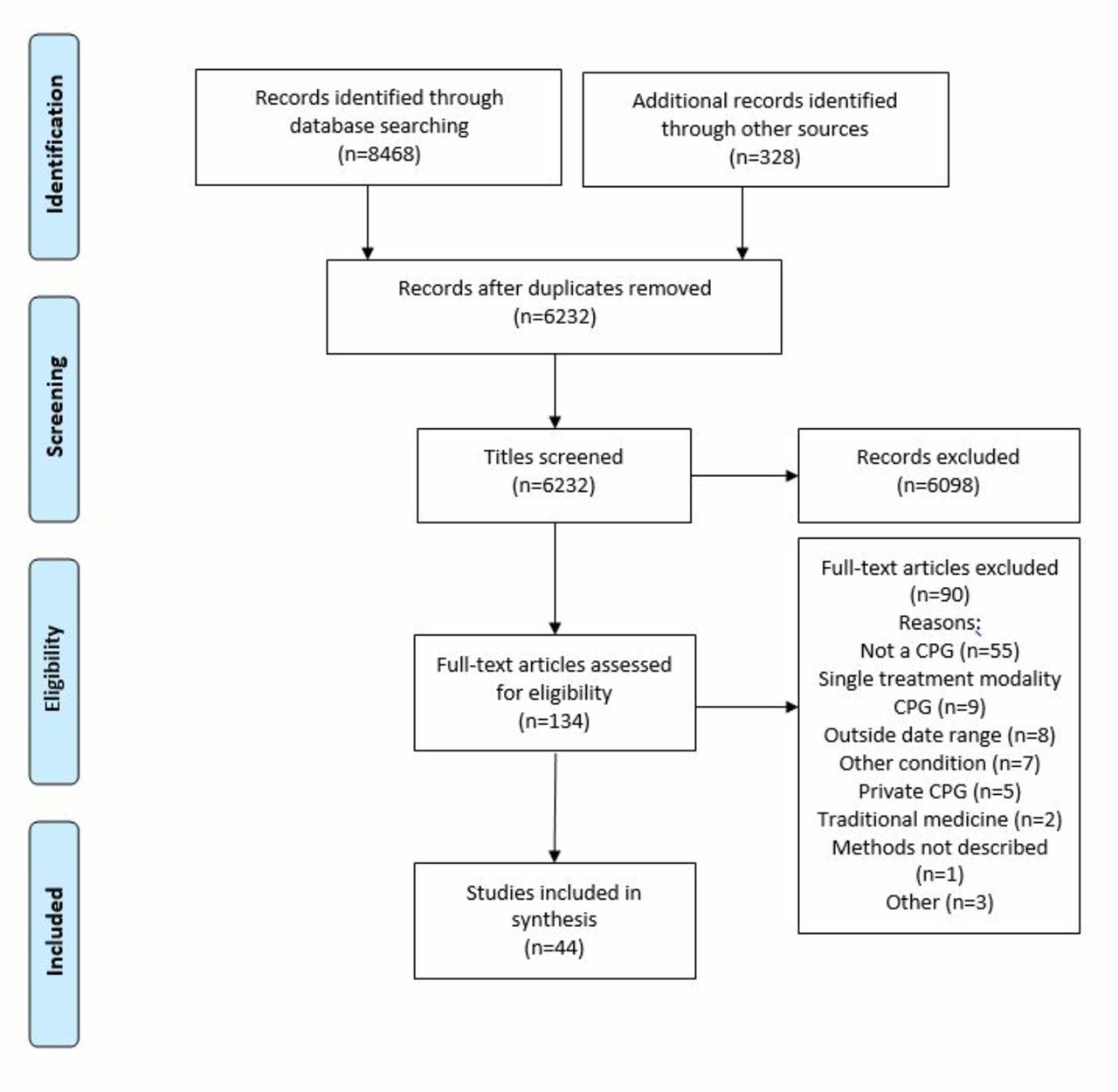
Our searches, including an updated search, identified 6232 discrete records, from which 44 CPGs (34 CPGs initial search and 10 CPGs updated search) were selected for inclusion (figure 1). Fifteen of the included CPGs were for LBP, 14 were for OA, 6 for shoulder conditions and 5 for the neck. We included single CPGs for the neck/thoracic spine, knee, ‘musculoskeletal injuries’ and lower limb (online supplementary file 2).
Supplemental material

{kind=link}
PRISMA flow diagram. CPG, clinical practice guidelines; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included CPGs
With the exception of CPGs from Malaysia19 and the Philippines,20 all CPGs originated or involved panel members from high-income countries. CPGs were from 11 individual countries and ‘international’ collaborations, involving authors from multiple countries. Most were from the USA (n=17), ‘international’ (n=10) and Canada (n=6). The Netherlands, UK and Italy each contributed two CPGs (online supplementary file 2).
CPGs from the USA were most commonly for LBP (n=8), ‘international’ CPGs were most commonly for OA (n=7), and half of Canadian CPGs were for neck pain (n=3). The majority of CPGs were developed by medical societies (n=23, 52.3%) which were either related to a profession/specialty group,21, or MSK condition of interest, for example, ref 22.
Appraisal of CPGs: inter-rater agreement
Inter-rater agreement was ‘fair’ for scope and purpose (domain 1), ‘good’ for clarity of presentation (domain 4) and ‘excellent’ for all other domains and overall AGREE II score (table 2).
Inter-rater agreement for AGREE II domains and overall scores
Appraisal of CPGs: quality
The mean (SD) AGREE II scores for each item, domain and overall scores across all guidelines are displayed in online supplementary file 3. The domain with the lowest mean score was ‘Applicability’ (27.6%, SD=18.3), and the highest mean score was for ‘Scope and Purpose’ (73.7%, SD=13.8).
Supplemental material
The AGREE II scores for each CPG are displayed in online supplementary file 4. In our previous review,10 eight high-quality MSK pain CPGs were identified for OA,21–24 LBP,25 26 neck pain,27 and shoulder pain.28 Of the 10 additional CPGs identified in our updated search, three were rated as high-quality and included in our synthesis, including two for LBP29 30 and one for neck pain31 (online supplementary file 3).
Supplemental material
Consistent recommendations
Following synthesis (table 3, online supplementary file 5), 11 common/consistent recommendations were identified across MSK pain conditions (box 2).
Supplemental material
Classification of recommendations
Care should be patient centred. This includes care that responds to the individual context of the patient, employs effective communication and uses shared decision-making processes
All CPGs described delivery of patient-centred care, most commonly as an introductory principle and sometimes specifically articulated within recommendations. Patient-centred care included providing individualised care based on the context of the patient and their preferences,21–26 28–31 shared decision making,24 26 28 using effective communication21 24 26 28 and/or an explicit discussion of ‘patient centred care’.27 29
Practitioners should screen patients to identify those with a high likelihood of serious pathology/red flag conditions
Seven CPGs offered ‘should do’ recommendations to screen patients for possible serious or structural pathology/‘red flag’ conditions during an initial assessment.24–29 31 Examples included suspicion of infection, malignancy, fracture, inflammatory causes of pain, severe and progressive neurological deficit (including cauda equina syndrome) and serious conditions that masquerade as MSK pain, for example, aortic aneurysm. The National Institute for Health and Care Excellence (NICE) OA CPG identified important differential diagnoses as gout, other inflammatory arthritides, septic arthritis and malignancy (bone pain).24
Psychosocial factors should be assessed
Nine CPGs, including four for LBP,25 26 29 30 two for neck pain,27 31 two for OA23 24 and one for rotator cuff disorders28 recommended assessing psychosocial factors. These factors included ‘yellow flags’, mood/emotions (depression and anxiety), fear/kinesiophobia and recovery expectations. Two LBP CPGs25 29 recommended using the STarT Back32 or Orebro Musculoskeletal Screening tools33 to identify psychosocial prognostic risk factors and subsequently match care to the level of patient risk.
Radiological imaging is discouraged unless: (1) serious pathology is suspected, (2) there has been an unsatisfactory response to conservative care or unexplained progression of signs and symptoms or (3) imaging is likely to change management
Six CPGs discouraged routine use of radiological imaging.24–26 28–30 In the case of LBP, routine imaging was discouraged unless serious pathology is suspected (ie, ‘red flag’ conditions), findings are likely to ‘change management’ (such as if administration of an epidural or spinal surgery is under consideration25 29), or if there has been a limited response to conservative care.26 Two LBP CPGs recommended explaining to patients that imaging may not be needed.25 29 In contrast one chiropractic CPG recommended consideration of imaging if there is ‘suspicion of an underlying anatomical anomaly, such as spondylolisthesis, moderate to severe spondylosis’ or ‘mechanical instability’.26 The NICE CPG encouraged clinical diagnosis of OA without imaging.24
Assessment should include physical examination. Physical examination could include neurological screening tests, mobility and/or muscle strength
Seven CPGs recommended undertaking a physical examination when assessing MSK pain conditions.23–29 Physical assessments included mobility/movement, strength,23 28 position and proprioception.23 CPGs for spinal pain also recommended tests of neurological function.26 27 29 The purpose of physical examination tests were to assist in the diagnosis or classification of MSK pain disorders. For the shoulder, this included differentiating between tendon, articular or referred pain origin.28 Neurological testing in the lumbar spine was used to differentiate pain of radicular origin.29 Physical examination procedures in the cervical spine were recommended to classify neck pain disorders into grades I–III.27 One CPG noted a lack of empirical support for physical assessments, although concluded that ‘the repercussions of not performing an examination would lead to dissatisfaction and unwarranted demand for tests or further referrals’.25
Patient progress should be evaluated, including the use of validated outcome measures
Five CPGs recommended evaluating patient progress23 24 26–28 and four of these recommended clinicians use validated outcome measures. Recommended outcome measures included a seven-point patient self-rated recovery question,27 pain intensity,26 functional capacity/activities of daily living26 28 and/or quality of life.24
All patients should be provided with education/information about their condition and management options
Ten CPGs recommended providing education or information either to: (1) encourage self-management22 23 25 27 29–31 and/or (2) inform/reassure patients about the condition or management (eg, prognosis and psychosocial aspects).23 24 26–31 In all CPGs, education/information was recommended as part of a package of care alongside other treatments, and a number of CPGs emphasised the need for education to be individualised based on patient need.23 25 29 30
Patients should receive management that addresses physical activity and/or exercise
All CPGs included recommendations relating to activity/exercise, with the strength of recommendation varying according to the type of activity/exercise and between different MSK conditions. CPGs for OA,21–24 LBP25 26 29 30 and neck pain27 31 made general recommendations for physical activity/exercise including maintenance of activity/‘normal’ physical activity, aerobic exercises, ‘exercise’ and/or ‘general exercise’. CPGs for OA had strong recommendations for specific exercise, most commonly strengthening,21–24 as well as mobility (eg, range of motion and stretching),22 23 water-based exercises,22 23 neuromuscular education21 or tai chi.22 For rotator cuff disorders, one CPG recommended initial treatment with prescribed exercise, such as stretching, flexibility and strengthening.28 Three CPGs for LBP recommended supervised exercise.25 26 30 neckpain and associated disorders (NAD) CPGs recommended supervised graded neck strengthening for NAD grade III and as part of multimodal care for NAD grades I–II.27 31
If used, manual therapy should be applied only in conjunction with other treatments
Manual therapy was a ‘could do’ recommendation for seven CPGs24 25 27–31 and a ‘should do’ recommendation for one.26 However when included, manual therapy was consistently recommended as a component of multimodal care, in conjunction with other management strategies, including exercise, psychological therapy, information/education, and activity advice rather than a stand-alone treatment.
Unless specifically contraindicated (eg, ‘red flag’ condition[s]), offer evidence-informed non-surgical care prior to surgery
Four CPGs recommended that patients be provided non-surgical treatments prior to consideration of surgery.24 25 28 29 The CPG for rotator cuff disorders was the only to specify a trial duration for non-surgical care, recommending surgical review if 3 months of non-surgical management had been unsuccessful and/or following non-surgical care there was a symptomatic full thickness rotator cuff tear on review.28
Facilitate continuation or resumption of work
Five CPGs offered a ‘should do’ recommendation for re-engagement with or continuation of work for patients with MSK pain, including neck pain,27 OA,23 rotator cuff syndrome28 and LBP.29 One CPG for LBP offered a ‘could do’ recommendation to advise patients to stay active, avoid inactivity and gradually increase activity levels, including work involvement.30 Three CPGs emphasised early return to work29 including engagement with vocational rehabilitations services, communication between worker, employer and health provider and planning processes to facilitate return to work.28
Single MSK conditions and conflicting recommendations
We also identified common recommendations for single MSK pain conditions including seven for LBP, four for OA and one for NAD (box 3, online supplementary file 5).
Conflicting recommendations for CPGs both between MSK pain conditions and within CPGs for a specific condition were noted for medication prescription (including paracetamol and non-steroidal anti-inflammatory drugs [NSAIDs]), electrotherapy, the use of braces and orthoses and acupuncture. There were also conflicting recommendations regarding the prescription of opioids including ‘could do’, ‘do not do’ and ‘uncertain’ recommendations. CPGs that offered ‘could do’ recommendations advocated caution, including careful consideration of risk and benefits,24 30 use of opioids ‘for the shortest period possible’29 and ‘not routinely’.25
Consistent recommendations across musculoskeletal (MSK) pain conditions
Care should be patient centred. This includes care that responds to the individual context of the patient, employs effective communication and uses shared decision-making processes.
Screen patients to identify those with a higher likelihood of serious pathology/red flag conditions.
Assess psychosocial factors.
Radiological imaging is discouraged unless:
Serious pathology is suspected.
There has been an unsatisfactory response to conservative care or unexplained progression of signs and symptoms.
It is likely to change management.
Undertake a physical examination, which could include neurological screening tests, assessment of mobility and/or muscle strength.
Patient progress should be evaluated including the use of outcome measures.
Provide patients with education/information about their condition and management options.
Provide management addressing physical activity and/or exercise.
Apply manual therapy only as an adjunct to other evidence-based treatments.
Unless specifically indicated (e.g. red flag condition), offer evidence-informed non-surgical care prior to surgery.
Facilitate continuation or resumption of work.
Consistent recommendations within single musculoskeletal (MSK) pain conditions
Osteoarthritis (OA)
Offer self-management programmes.
Provide interventions targeting weight loss to people with OA who are overweight or obese.
Do not use glucosamine or chondroitin for disease modification.
Do not undertake knee arthroscopic lavage and debridement unless there is a rationale (such as mechanical knee locking).
Low back pain
Do not offer paracetamol as a single medication.
Do not offer opioids for chronic LBP.
Do not offer selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, tricyclic antidepressants or anticonvulsants for LBP.
Do not offer rocker shoes or foot orthotics.
Do not offer disc replacement.
Only offer spinal fusion if part of a randomised controlled trial.
Spinal injections (eg, facet joint injections, medical branch blocks, intradiscal injections, prolotherapy and trigger point injections) should not be used for LBP.
Neck pain
Neck pain disorders should be classified as grades I–IV.
Discussion
We identified 11 common recommendations for MSK pain care (box 2) that applied to patients with OA, LBP, neck pain and shoulder pain. These recommendations may provide clinicians, healthcare managers, funders, policy makers and researchers with a simple and clear consensus of current MSK pain priorities. In turn, this could help address the variable quality of clinical care delivered for MSK pain conditions.34–36
The common recommendations could be used in a number of ways to improve care. First, they could guide consumers in making informed healthcare decisions or assist them to identify when they are receiving suboptimal care. Second, clinicians could apply the recommendations to guide care decision making, to identify areas for learning and development and to assess their practice. Third, health services could assess the quality of care by applying them as minimum standards during clinical audit. Finally, a broader strategy (eg, for researchers, health planners/policy makers or funders) could be the continued development of the common recommendations into a set of quality indicators that could be used for reporting or to benchmark care quality. The recommendations could be used as a preliminary set of standards that could be refined via a rigorous, structured process.37
Our findings are similar to a recent review by Babatunde et al that was a synthesis of MSK pain management in primary care.11 Recommended care included self-management advice, education and exercise as first-line treatments for MSK pain. The authors recommended short-term NSAIDs and opioids for pain relief provided risks and harms were considered. There was limited evidence for aids and devices (eg, taping and braces) and passive treatments (eg, acupuncture, transcutaneous electrical nerve stimulation and laser) and inconsistent evidence for surgery (equivalent to conservative care options in the longer term).11 In contrast to our review, the authors reported support for psychosocial interventions, especially for those at risk of poor prognosis. We found that while CPGs in our review universally recommended psychosocial assessment, only LBP and neck pain CPGs reported on psychological treatments (‘could do’ recommendations for psychological therapies for LBP and contradictory recommendations for neck pain). Although our review included more recent CPGs, for example,25–27 29–31 CPGs for other common MSK pain conditions including OA and hip pain, Babatunde et al 11 included other sources of literature such as trials and systematic reviews. Psychological-informed management for MSK pain is an area that is currently lacking in CPGs.
Our review identified CPGs for LBP, OA, NAD and rotator cuff disorders. Arguably the common recommendations are relevant to other MSK pain conditions. For example, in tendinopathy, psychosocial factors are known predictors of outcome38; radiological imaging is of questionable clinical utility because of a moderate relationship between symptoms and outcome,39 and high value non-surgical approaches to management such as education and exercise form the cornerstones of care.40 41 Although high-quality CPGs are currently lacking for other MSK pain conditions, we speculate that the consistent recommendations could be applied broadly to managing non-traumatic MSK pain.
Due to the potential for harm, an area we were interested in was opioid prescribing. We were unable to identify a consensus among CPGs relating to opioids, and there were conflicting recommendations both within and across MSK pain conditions. While there were conflicting views, almost all CPGs urged caution and/or discouraged opioid use. Recent research has reported no additional benefit of an opioid over a NSAID for acute LBP,42 and further efficacy studies are underway.43 Recent opioid-prescribing CPGs for patients with chronic pain44 45 recommend risk assessment to identify those at higher likelihood of opioid-related harms. Although outside the scope of this review, these recommendations should be considered by clinicians.
Our findings were similar to recent reviews of LBP management in emergency care.46 47 In emergency care, clinicians should use ‘red flags’ to assess the likelihood of serious pathology, apply judicious use of radiological imaging, identify psychosocial risk factors, provide targeted education and reassurance, offer exercise, cold and heat and promote early return to work and function.46 The similarities of these recommendations and our findings suggest they could be applied in varied healthcare settings.
Results of our updated search reinforced our previous findings10 that most MSK pain CPGs were of poor quality, which is a waste of resources. In addition to directing resources to fewer, higher quality CPGs, another way to reduce waste is for developers to focus on gaps in recommendations, areas for which there is currently limited consensus, and on other MSK pain conditions. As previously described, medication prescribing and psychologically oriented management of MSK pain are areas that lack research or have not been addressed by CPGs to date. CPGs targeting thoracic pain and non-OA knee pain are MSK pain areas that are lacking.
Limitations
The AGREE II instrument reflects methodological processes, not necessarily content, and scores may reflect reporting rather than methodological quality. The AGREE II developer’s suggest research groups identify their own criteria for CPG quality.16 Our group defined high-quality CPGs as those who scored higher than 50% in three AGREE II domains. Although consistent with the AGREE II developer’s recommendations, investigator-developed criteria have the potential for bias by including or excluding CPGs based on non-empirically derived criteria. While a cut-off value of 50% is consistent with other studies, for example,18 our criteria is somewhat generous when compared with some other reviewers for example.48 CPGs were appraised by three authors and ideally four should be used.14 Our research group was interprofessional; CPG appraisers were academic and clinical physiotherapists (IL and RW) and an indicator development researcher also with a background in physiotherapy (LW). Our synopsis of CPGs and interpretation of their recommendations (eg, as ‘should do’, ‘could do’ and so on), due to variations in the reporting and language of CPGs, relied on the interpretation of the research group. This is an inherent issue where there is heterogeneity in the way CPGs are conceptualised and their recommendations and underpinning evidence are presented. For example, some CPGs offer broad generalised recommendations26 compared with others that address specific, highly targeted questions.31 To account for this, we have ensured our interpretation and methodological steps have been clearly reported. As always, the search strategy may have failed to identify all relevant documents, and we only reviewed CPGs available in English. Nevertheless, our involvement of a reference librarian during searching and the experience of the research group means we are confident that relevant CPGs were included.
Conclusion
Variation in the quality of care is a barrier to providing high value MSK pain care. CPGs are an important tool to address MSK pain care quality. We identified 11 consistent recommendations (box 2) for the management of MSK pain conditions. These recommendations can be used by consumers, clinicians and at health services and policy levels to improve the quality of MSK pain care. Optimising the implementation of these recommendations comprises the next challenge.
Acknowledgments
We acknowledge Anne Smith for statistical assistance.
References
Footnotes
Contributors All authors were involved in the conception, design and interpretation of data. IL, LW and RW performed the data analysis and initial interpretation. IL was responsible for initial writing and drafting of the article, which was reviewed by all authors. All authors revised critically for important intellectual content and approved the final version to be submitted.
Funding IL is funded by an Australian National Health and Medical Research Council Early Career Fellowship (APP1090403). CGM’s fellowship (APP1103022) is funded by Australia’s National Health and Medical Research Council, and his research is supported by a Program Grant (APP1113532) and CRE Grant (APP1134856). LW works on a project funded by a National Health and Medical Research Council Program Grant (APP1054146).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.