Article Text

Abstract
Objective Describe the self-reported prevalence and nature of Olympic-career injury and general health and current residual symptoms in a self-selected sample of retired Olympians.
Methods 3357 retired Olympians from 131 countries completed a cross-sectional online survey, distributed by direct email through World Olympians Association and National Olympian Associations databases. The survey captured Olympic sport exposure, significant training and competition injury history (lasting >1 month), general health (eg, depression) during the athlete’s career, and current musculoskeletal pain and functional limitations.
Results 55% were men (44% women, 1% unknown), representing 57 sports (42 Summer, 15 Winter), aged 44.7 years (range 16–97). A total of 3746 injuries were self-reported by 2116 Olympians. This equated, 63.0% (women 68.1%, men 59.2%) reporting at least one significant injury during their Olympic career. Injury prevalence was highest in handball (82.2%) and lowest in shooting (40.0%) for Summer Olympians; and highest in alpine skiing (82.4%) and lowest in biathlon (40.0%) for Winter Olympians. The knee was the most frequently injured anatomical region (20.6%, 120 median days severity), followed by the lumbar spine (13.1%, 100 days) and shoulder/clavicle (12.9%, 92 days). 6.6% of Olympians said they had experienced depression during their career. One-third of retired Olympians reported current pain (32.4%) and functional limitations (35.9%).
Conclusions Almost two-thirds of Olympians who completed the survey reported at least one Olympic-career significant injury. The knee, lumbar spine and shoulder/clavicle were the most commonly injured anatomical locations. One-third of this sample of Olympians attributed current pain and functional limitations to Olympic-career injury.
- injury
- athlete
- injury prevention
- health
- olympics
Statistics from Altmetric.com
INTRODUCTION
Elite athletes are cumulatively exposed to high physiological training and competition loads, including repeated mechanical stresses and impacts.1 2 While these loads and impacts can vary by sport, it is known that sport participation, in particular elite-level participation, is associated with an increased risk of acute and overuse musculoskeletal injury.3–6 Sports injury prevention and the protection of athlete health is a key mandate for the World Olympians Association (WOA), IOC and International Federations (IFs),7–9 and there are numerous studies describing elite athlete injury patterns seasonally10–13 and during major sporting events.4 5 13 14 However, little is known about injury and health patterns across an elite athlete’s entire sporting career.
While former elite athletes are generally reported to present a lower overall morbidity risk and better self-reported health in later years compared with the general population,15–17 they also report ongoing pain, musculoskeletal dysfunction and a greater rate of osteoarthritis (OA).18–21 Increasing our understanding of the characteristics and aetiology of injuries faced by elite athletes across their athletic career will help inform strategies22 aimed at mitigating the risk of injury and their long-term consequences.23–25 Therefore, we aimed to describe (1) the prevalence and nature of Olympic career-related injuries, (2) general health status and (3) athletes’ self-report of injury-related residual symptoms.
Methods
This was a cross-sectional study collecting self-report data using an online questionnaire available in eight languages (English, French, German, Spanish, Russian, Chinese, Japanese and Korean). Data collection was conducted between April 2018 and February 2019, recruiting athletes who had participated in at least one Summer and/or Winter Olympic Games (Olympians), who were aged 16 years or older and considered themselves retired from the Olympic-level training and competition.
Recruitment
The survey was promoted to Olympians globally through WOA and IOC communication platforms. Channels included the Olympic-athlete network Olympians.org, National Olympians Associations (NOAs), National Olympic Committees (NOCs), IFs, Athlete 365 and the Olympic Studies Centre. Researchers are unaware of how many Olympians these promotions reached (see the Discussion section). Recruitment targeted Olympians who considered themselves retired from Olympic participation and who were interested in taking part in the survey. Those wishing to participate were asked to register with the WOA Database (‘the OLY database’), if they were not already registered, where their status as an Olympian was verified and they were added. A password-protected survey link was then emailed to all Olympians on the database. Additionally, the WOA engaged with NOAs, who then also emailed the survey to their countries’ Olympians.
Detailed study information, including information on data handling and confidentiality, was provided at the start of the survey. We explicitly outlined that by completing and submitting the questionnaire, the participants’ were consenting that their information would be used anonymously for the study.
Questionnaire survey
The questionnaire was an online web-based survey hosted by SurveyMonkey, containing four main sections: (1) baseline demographics, (2) Olympic-career sport participation and self-reported injury history details, (3) self-reported current musculoskeletal health, and, (4) Olympic career and current general health, and quality of life.
Baseline questions requested Olympians demographics including age (years), sex, country of birth and country of residence. Current and previous height (cm) and weight (kg) were collected to calculate current and Olympic-career body mass index (BMI kg/m2). Olympic sport participation included sport and Olympic Games participated in, country competed for, total years competing in sport, years of international participation (at senior level) and date of retirement from Olympic sport.
Participants completed the survey questions about Olympic career-related training and competition injury. They were asked to recall the anatomical location, injury type, severity, cause (acute vs overuse) and mechanism (eg, contact with the static object).6 26 27 Pressure to return to sport during injury and current symptoms that the participants attributed to their Olympic injury (eg, lasting pain, functional limitation) were also recorded. The presence of disease (eg, depression, asthma) during an Olympian’s career was ascertained by asking ‘During your Olympic career did you ever suffer from any of the following diseases’.
Definitions of career and injury
An individual’s Olympic career was defined as the period of training and competition (eg, preparation and qualification) from the lead up to their first Olympic Games until retirement following their last Olympic Games. The definition for a retired Olympian in this study was ‘an Olympian who considered themselves retired from Olympic competition (ie, those who no longer intended to qualify for or compete at any upcoming Summer or Winter Olympic Games)’. Significant ‘injury’ was defined as ‘any injury causing significant pain and/or dysfunction for a period of 1 month (or more) where ongoing sport participation during that time was disrupted’.25 28 Injuries lasting less than 1 month were not recorded. For the purposes of the present study, we only counted injuries that occurred during training for, or competition in, the athlete’s Olympic sport, during the athlete’s Olympic career. Training referred to any/all conditioning activities in addition to Olympic sport-specific activities. Injury severity was defined by the estimated total number of days between the day of the injury and the athlete’s return to full fitness/sport participation.
Patient and public involvement
A patient advisory group of nine retired Olympians provided input in the face validation of the questionnaire content and design. A draft form of the survey was piloted for question understanding and clarity and overall questionnaire length and acceptability. At the end of the test period, comments from the patient advisory group were incorporated into the final version of the survey.
Ethics and confidentiality
Ethical approval for the study was obtained from the Edinburgh Napier University ethics committee (SAS/00011). No identifying parameters were recorded, and individual Olympians were not identifiable at any stage of the research. All data were treated confidentially, ensuring athlete anonymity at all times.
Data analysis
Descriptive statistics are presented as frequencies (proportion) for categorical variables, and mean and SD, or median and range where data are not normally distributed, for numerical variables. For severity (days) median and mean are presented together, the latter to allow comparison with other studies. Self-reported injury prevalence was calculated dividing the number of injured athletes by the total number of athletes and presented as percentage (%) with 95% CIs. Prevalence ratios (PR) with 95% CI were reported between groups. Differences in values for numerical variables were analysed by t-tests, or Mann-Whitney where appropriate, and comparisons between groups for categorical variables were conducted by the χ2 test.28 Significance was accepted at p<0.05 (equal variances assumed).
Results
Olympian characteristics
At the close of the survey, there were 4735 Olympian online survey entries. A total of 1388 ineligible (ie, blank, incomplete, duplicate) entries were removed leaving 3357 completed questionnaires for data analysis. Olympians completing the survey (55% men, 44% women, 1% (n=29) sex not reported) represented 131 countries and 57 Olympic Sports (42 Summer, 15 Winter). Respondents had a median age of 44.7 years (range; 16–97), mean 10.4 years (SD 5.6) of Olympic/International level participation (table 1). Olympian participation spanned 36 Summer and Winter Olympic Games from London 1948 to PyeongChang 2018, with 61.0% of Olympians participating in one Olympic Games, 26.5% in two and 11.9% competing in three to six Olympic Games.
Olympian characteristics
Injuries by sport
A total of 2116 Olympians reported 3746 injuries equating to 63.0% (95% CI 61.4–64.7) of Olympians reporting at least one significant Olympic career-related injury, with the prevalence of career injury greater in women (68.1% (65.7–70.4)) than men (59.2% (57.0–61.5); PR=1.15 (1.12–1.18); p<0.001). Overall, each Olympian reported a mean of 1.1 injuries (women 1.25, men 1.01) during their Olympic career, with the majority of injuries 63.8% (n=2389) attributed to training (table 2). Injury prevalence was lower for Summer Olympians 62.0% (60.2–63.8) compared with Winter Olympians 69.0% (64.9–73.0) (PR=0.90 (0.87–0.93); p<0.001). By sport, injury prevalence was highest in handball (82.2% (71.1–93.4)), badminton (78.4% (65.1–91.6)), judo (77.4% (68.9–85.9)), wrestling (73.1% (56.0–90.1)), athletics (72.2% (68.3–76.1)) and artistic gymnastics (71.1% (61.3–80.0)) for Summer Olympians. For Winter Olympians, prevalence was highest for alpine skiing (82.4% (73.3–91.4)), freestyle skiing (81.6% (69.3–93.9)), snowboarding (77.3% (59.8–94.8)), short-track speed skating (75.0% (60.9–89.1)), luge (74.4% (60.6–88.1)) and bobsleigh (69.7% (59.4–80.1)). Conversely, injury prevalence was lowest for shooting (40.0% (27.6–52.4)) and swimming (48.5% (44.1–52.8)), and biathlon (40.0% (22.5–57.5)) and curling (54.3% (37.8–70.8)) for Summer and Winter Olympians, respectively (sports with n≥20 participants). By decade of Olympic Games participation, injury prevalence steadily increased from 25.9% to 65.7% for Summer Olympians and from 33.3% to 75.4% for Winter Olympians, between 1950 and 2010 (figure 1).
Injuries by sport
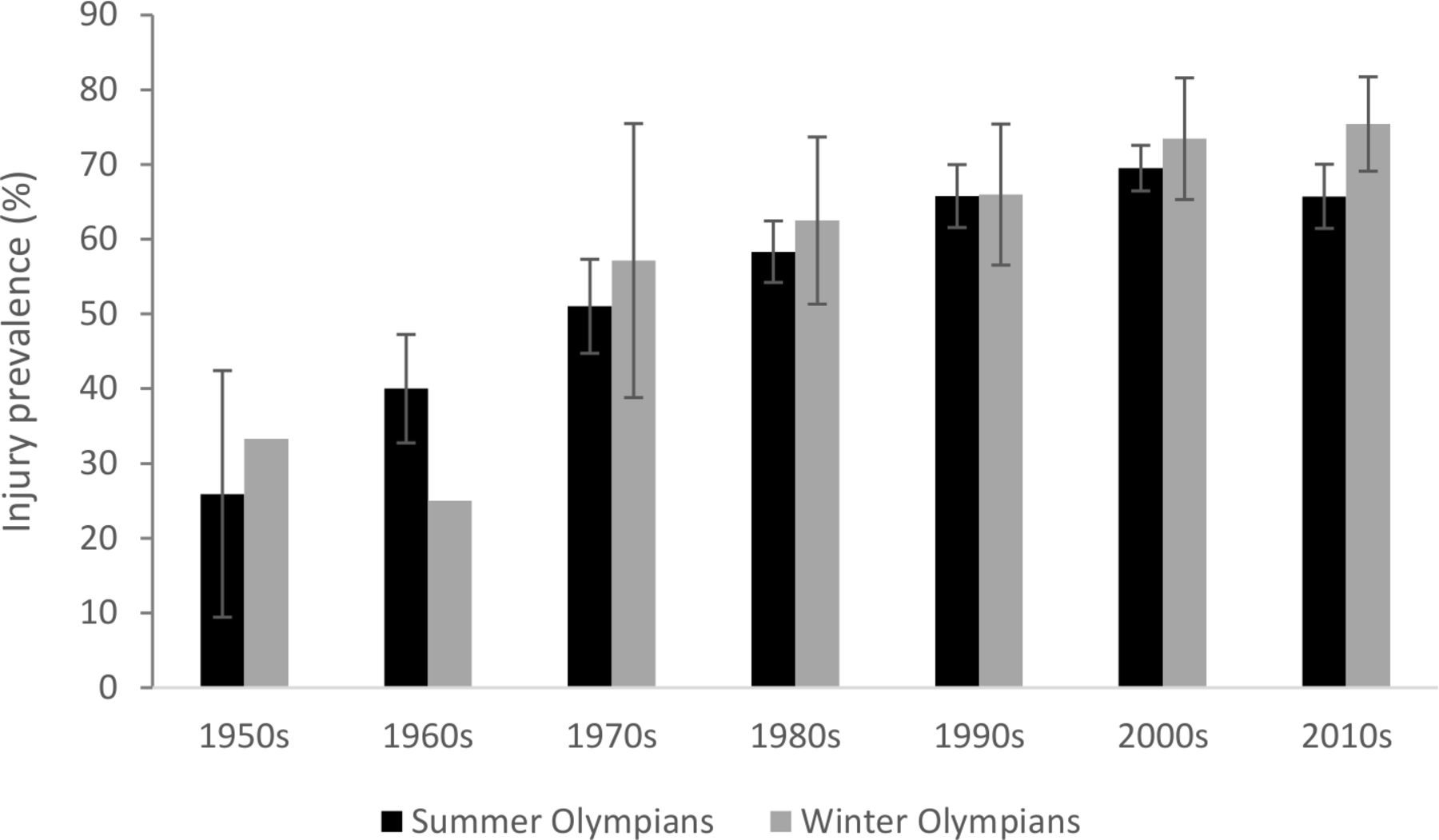
Injury prevalence by decade of Olympic Games participation. (decade of participation denoted by first Olympic Games if multiple Games competed in).
Injuries by location, type and cause
Injuries most frequently affected the knee (20.6% of all injuries, median severity 120 days (mean 197 days)), lumbar spine (13.1%, 100 days (mean 227 days)) and shoulder/clavicle (12.9%, 92 days (mean 180 days)). The most common injury types were fracture (12.0%, 60 days (mean 111 days)), strain/muscle rupture/tear (11.9%, 70 days (mean 158 days)) and ligament rupture (10.4%, 180 days (mean 186 days)). By specific diagnosis knee lesion of meniscus/cartilage (24.6% of all knee injuries, 100 days (mean 199 days)), knee ligament rupture (19.6%, 180 days (mean 194 days)), lumbar spine nerve/spinal cord (16.2% of all lumbar spine, 150 days (mean 231 days)), shoulder dislocation/subluxation (15.1% of all shoulder, 100 days (median 184 days)) and thigh muscle strain/rupture/tear (49.3% of all thigh, 60 days (mean 126 days)) were predominant. These patterns were similar for both Summer and Winter Olympians. Of all lumbar spine injuries, 65.6% were reported to be recurrent in nature, shoulder/clavicle injuries 52.7% and knee injuries 46.6%.
The majority of injuries were acute in nature accounting for 75.8% and 82.3% of all injuries for Summer and Winter Olympians, respectively, with overuse reported as the cause of injury for the remainder. The most common reported injury mechanisms were overuse gradual onset (41.4%), overuse sudden onset (23.5%) and non-contact trauma (14.5%) for Summer Olympians, and contact: stagnant object (29.8%), overuse gradual onset (26.5%) and overuse sudden onset (19.8%) for Winter Olympians.
Returning from injury
During the injury, 23.6% (21.3–25.8) of Olympians reported continuing all training/competition activities with performance decline. A fifth (21.6% (19.4–23.8)) of Olympians reported that they stopped all training/competition and performed rehabilitation exercises and allowed the injury to fully heal (19.1% (17.0–21.2)) (table 3).
Olympian behaviours during injury
One-third (29.3% (27.8–30.9)) of Olympians reported that they continued to compete and/or train using painkillers and 40.7% (39.0–42.3) reported that they competed/trained using non-steroidal anti-inflammatory drugs (NSAIDs). 11.1% competed/trained using a steroid injection and 11.5% a local pain-killing injection, for their injury.
When experiencing an injury, 75.5% of Olympians indicated that they put pressure on themselves to return to sport as quickly as possible. This was followed by pressure felt from coaches (33.6%), sport governing body (15.5%) and teammates (13.6%) (figure 2).

{kind=link}
{kind=link}
Prevalence (%) of injured Olympians expressing having felt pressure to return to sport, by source of pressure (multiple option selection permitted).
Olympic-career health and residual symptoms
The prevalence of depression reported by Olympians was 6.6% during their career and 9.5% during their transition into retirement. Of Olympians who reported depression during their career, 83.7% also reported sustaining a significant injury (88.3% women, 77.8% men) compared with 16.3% reporting no injury. Asthma prevalence was 8.3% (triathlon 26.3%; cross-country skiing 20.0%, long-track speed skating 17.6%), and regular painkiller and NSAID use during an Olympian career 16.7% and 29.8%, respectively. Overall, the prevalence of health issues, for example, depression during Olympic career (PR=2.09 (1.96–2.23) p<0.001), asthma (PR=2.10 (1.98–2.22); p<0.001), and painkiller use (PR=1.31 (1.23–1.39); p<0.001) were significantly higher in women compared with men (table 4). A third of Olympians reported current, ongoing pain (32.4% (30.8–34.0)) and functional limitation (35.9% (34.2–37.5)) attributed to significant injuries sustained during their Olympic career, with the prevalence of pain higher for women compared with men (PR=1.33 (1.28–1.38); p<0.05). Injuries to the knee, lumbar spine, shoulder/clavicle and ankle were most commonly associated with ongoing symptoms.
Health during Olympic career and residual symptoms
Discussion
This is the first worldwide study of self-reported injuries suffered by Olympians. The aims were to describe the prevalence and nature of sport-related significant injuries, including residual symptoms and general health, across an Olympians’ Olympic Games career. The main findings were: (1) 63% of retired Olympians reported having had at least one Olympic-career injury that equated to a mean 1.1 injuries per Olympian over 10.4 years of participation; (2) the knee, lumbar spine and shoulder/clavicle were the most frequently injured; (3) career depression prevalence was higher in those with injury compared with those without; and (4) one-third of Olympians reported current, ongoing pain and functional limitation attributed to injuries sustained during their Olympic career.
Olympic-career injury
To date, there is only one other cross-sectional study available on whole-career injuries in Olympians. In Great Britain (GB) Olympians (D Cooper Doctoral thesis, unpublished data, 2016), the prevalence of self-reported injury was 52% and with 2.0 injuries reported per athlete across 9.2 years of participation, where a similar injury definition was used. The rate of injury may reflect regional variations, differences in the length and level of exposure to the high-level sport and the length of recall.29 In the present study, Olympians were retired 18.3 years vs 30.5 years in the GB study meaning a longer period from which to remember (or forget) significant injuries during their sporting career for GB Olympians. In agreement with the GB study, female Olympians had a higher prevalence of injury than male Olympians.
Although female Olympian injury rates were higher overall, the present survey pointed to no sex differences in injury rates across Olympic sports between male and female athletes other than in rowing and sailing. In Rio 2016 and PyeongChang 2018 (prospective data with medical diagnosis), there were no differences in the rates of injury between men and women, with significant differences observed in only a handful of sports, for example, sailing, shooting, mountain biking, luge and ice hockey.14 26
By sport, the self-reported prevalence of injury was highest for handball, badminton, judo and wrestling for Summer Olympians and alpine skiing, freestyle skiing and snowboarding for Winter Olympians. Conversely, the lowest injury rates were reported for shooting and swimming for Summer Olympians and biathlon and curling for Winter Olympians. These findings are consistent with data from Summer and Winter Olympic prospective surveillance studies. In London 2012, handball and badminton were among the sports with the highest injury rates.5 Although in Rio 2016, injury rates decreased for these sports, they remained in the top half for injury incidence.26 Consistently, shooting and swimming presented the lowest prevalence during both Games.5 26 Badminton, handball5 and wrestling26 also presented the highest rates of more severe injuries (>7 days absence) in the London and Rio Olympic Games. In Sochi 2014 and PyeongChang 2018 alpine skiing, freestyle skiing disciplines and snowboarding disciplines presented the highest winter sport injury rates while again biathlon and curling were among the lowest.6 14 Snowboard cross, ski cross and snowboard slopestyle also presented the most number of severe injuries (>7 days absence) of all sports.6 14
The risk of injury across different sports is understood to be influenced by a number of factors and frequent events, such as player to player contact (ie, during handball, judo and wrestling),26 30 or a combination of factors such as speed and jumps leading to falls and crashes (ie, during alpine and freestyle skiing and snowboarding)14 31–34 have been reported to increase the rate and severity of athlete injury. These high speeds, jumps and contact events characterised in a large proportion of winter sport disciplines may explain the higher prevalence of injury reported by Winter compared with Summer Olympians.
The knee, followed by the lumbar spine and then shoulder/clavicle were the three most common injury locations and fracture, strain/muscle rupture/tear and ligament rupture the most frequent injury types. These findings are consistent with those of previous prospective and self-report studies showing the knee, lumbar spine and shoulder most commonly injured in the current35 and retired (D Cooper Doctoral thesis, unpublished data, 2016) GB athletes and similar to Olympic Games surveillance studies where knee and sprain/ligament rupture injuries were most prevalent.14 26
It is important to remain cognisant of the effect that differences in both recording methodology and injury definitions may have when comparing results. For example, a broad medical attention definition in the Olympic surveillance studies permits the recording of more frequent, minor injuries compared with the present study significant injury definition. Hence, sports with more frequent, but less severe injuries, such as abrasions, contusions and lacerations, may present with a higher injury prevalence in the latter studies. Additionally, Olympian numbers in some sports in this study were too low to provide a reasonable measure of prevalence in previously reported higher risk sports for example, BMX.
Olympic-career health
In addition to injury, Olympians answered questions on key health indicators during their Olympic career. Overall, 6.6% reported experiencing depression at some point during their Olympic career and this increased to 9.5% on retirement from their sport. The self-reported prevalence of depression in Olympians in this study is not directly comparable with other studies due to the time period of measurement (10.4 years); however, the rate overall is low when compared with the 15%–21% previously reported over one season in college athletes,36 37 and compared with 1 year (6.7%) within the general population.38 39
Depression may present as a postinjury sequela in athletes40 41 and the present results confirm this finding where four out of five of those athletes reporting depression also reported injury during their career. Similar to other athlete studies36 42 and rates found within the general population,38 female Olympians in our sample reported higher rates of depression than did the male Olympians both during their career and at retirement. Retirement from sport marks a period of major life transition for elite athletes. Findings in this study agree with previous research on career termination and depression whereby retirement may precipitate behavioural and emotional difficulties in some athletes and an increase in the occurrence of depression and anxiety.43–45 Wippert and Wippert concluded that the manner in which retirement occurred (eg, planned vs involuntary retirement) may also influence the magnitude of depression symptomatology.45
Olympians reported regularly using non-steroidal anti-inflammatories (NSAIDs, 29.8%) and painkillers (opioids) (16.7%) during their Olympic careers with the use of NSAIDs most predominant. This supports previous findings of their widespread use in elite athletes from football,46 triathlon,47 American collegiate sports48 and during major game events.49 The use of painkillers by athletes has the potential to worsen injury due to the inhibition of the pain response and/or inflammatory process,50 and NSAID use in athletes has been linked to five times higher incidence of adverse events, for example, gastrointestinal cramps and bleeding, haematuria and cardiovascular events, such as arrhythmia and palpitations.51 Additionally, longer-term use decreases protein synthesis in muscle after exercise and increases the risk for small intestine mucosal injury.52 53
Athletes in the present study reported feeling pressure to return to sport and continuing to train and compete while injured. Continuing to train and compete with underlying health problems is not new in elite sport,54 and it is often associated with a painkiller and NSAID use, disregard of medical advice and hiding symptoms from others.55 56 Athletes who perceive more social pressure to compete hurt are likely to be more rest-averse54 and an athlete’s behaviour during injury and the concept of ‘playing hurt’55 56 likely delays recovery.15
Current symptoms and their association with Olympic-related injuries
A third of the Olympians in this sample attributed current, ongoing pain and functional limitation to injuries they sustained during their Olympic careers. This suggests that there may be longer-term musculoskeletal consequences related to some sports injuries and the knee, lumbar spine, shoulder/clavicle and ankle were the most common locations for both past injury and for ongoing current symptoms.
Significant joint injury is a risk factor for the development of OA, and evidence in retired athletes from football,57–59 Rugby Union60 and most recently Olympic sports25 speaks to an association between joint injury and ongoing pain, and the development and progression of OA. It is important, however, to understand if the rate of OA differs between Olympians and the general population. To date, few retired athlete studies have included these comparisons, and where comparisons with a general population control are made, they were limited to studies in one geographic region, in either men or women alone and single sports.57 59 60
Alongside injury, age, female sex and obesity61–63 are risk factors for the development of OA. Going forwards it may be important to understand if changes in body composition (eg, increasing BMI) in retired elite athletes influences longer-term musculoskeletal health outcomes.
Strengths and limitations
This is the first worldwide large-scale survey of injuries in retired Olympians. We invited responses in eight languages. The survey included questions about athletes’ behaviours during their injury, for example, what athletes did, and what pressures they felt, which is unique compared with previous geographical regional surveys. In addition, self-report of current health status provides information on Olympian’s recall of their general health during their Olympic career and their current symptoms of pain and limitations.
This cross-sectional study is limited by recall bias, given the range of ages and number of years retired, particularly regarding injury history for older Olympians (the oldest Olympian was 97 years), and there may be a differential effect of recalling injuries, for example, between London 1948 and PyeongChang 2018. To mitigate some recall bias, a significant, 1-month, injury definition was used whereby Olympians were asked to recall only significant injuries they had sustained, that is, injuries they were more likely to remember. Because minor injuries were not recorded due to the definition used, this study will overestimate the reported mean severity of injuries. Hence, it is important to consider this injury definition when both reporting and comparing injury rates and severity with other studies.
There is also a self-selection bias in the study sample, whereby Olympians who have a significant injury history may have had a greater propensity to participate and complete the survey. A prize draw was included as part of the study in an effort to incentivise those less inclined to participate, to provide a broader demographic. We cannot provide an accurate survey response rate as it was not possible to know how many retired Olympians were reached in the study promotion. There are an estimated 100 000 Olympians worldwide today (Wikipedia; ‘World Olympians Association’, n.d.) and based on recent Summer and Winter Games’ participation numbers it could be estimated there are around 20 000 current Olympians. Therefore the present sample represents around 4% of the total retired Olympian population and our conclusions are limited to this sample—they are not generalisable. The present descriptive study does not make any causal inferences.
Conclusion
In summary, 63% of retired Olympians who responded to the survey reported experiencing a significant injury during their Olympic career, with Olympians reporting injury also reporting a higher prevalence of depression during their Olympic careers. A third of Olympians attributed ongoing pain and functional limitation to injuries they sustained.
What are the findings?
Overall, 63% of a sample of retired Olympians reported at least one Olympic career-related significant injury, equating to 1.1 injuries per 10.4 years of participation.
Three-quarters of this sample of Olympians put pressure on themselves to return to sport and a quarter recalled that they continued to train/compete, while injured.
A third of Olympians experience current pain and functional limitation that they attributed to an Olympic-career injury.
How might it impact on clinical practice in the future?
Athletes continuing to train and compete with injury, including the pressures athletes feel to return to sport should be a matter for discussion within the athlete, medical and coaching team.
Approaches to athlete injuries should focus on facilitating full and complete rehabilitation particularly around significant joint injuries.
It is important to understand the factors associated with the longer-term consequences of Olympic-career injury in order to provide evidence-informed information for coaches and medical practitioners.
Acknowledgments
The authors acknowledge the contribution and support of the World Olympians Association administration team throughout the different stages of the study including study promotion and participant recruitment. They would like to offer sincere thanks to the study survey languages translation checkers, Francis Bougie, Gillian Cameron, Ayako Ito, Toshinobu Kawai, Juwon Kim, Natalia Salmina, Carlos Valiente Palazón, Ivory Wu and Valeriya Yanina. Finally, they would like to thank all the Olympians who participated for their time and effort in completing the survey, without whose help this study would not have been possible.
References
Footnotes
Twitter @DebbiePalmerOLY, @CarolynAEmery, @larsengebretsen, @malavshroff, @TSoligard, @jwhittak_physio
Contributors All authors contributed to the study conception and design, data collection and interpretation. DP analysed the data and drafted the paper. All authors provided revisions and contributed to the final manuscript. DP is the guarantor.
Funding The World Olympians Association funded the Retired Olympian Musculoskeletal Health Study (ROMHS) with a research grant from the IOC.
Competing interests TS works as Scientific Manager in the Medical and Scientific Department of the IOC. LE is Head of Scientific Activities in the Medical and Scientific Depart of the IOC, and Editor of the British Journal of Sports Medicine. RB is Director of the Medical and Scientific Department of the IOC.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval Ethical approval for the study was obtained from Edinburgh Napier University (UK) ethics committee (SAS/00011).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.