Article Text

Abstract
Objective We aimed to examine the risk of concussion in children with a previous history of concussion.
Design Systematic review and meta-analysis. The primary outcome was number of children with and without a previous lifetime history of concussion who sustained a diagnosed concussion within each study period. Risk of bias was assessed using the Newcastle-Ottawa Scale. A random effects model was used to estimate a pooled risk ratio (RR) with corresponding 95% CIs; results were summarised in forest plots.
Data sources Four electronic databases (MEDLINE, Embase, CINAHL, SPORTDiscus) and selected reference lists were searched (PROSPERO registration No CRD42019135462).
Eligibility criteria Original English language peer-reviewed publications that compared concussion risk in children aged 5–18 years with and without a previous concussion history in which risk estimates were reported or able to be calculated.
Results Of 732 identified studies, 7 studies representing 23 411 children (risk of bias range, 7–9; maximum possible score=9) were included for meta-analysis. Pooled risk of sustaining a concussion was more than three times greater in children with a previous concussion compared with those with no previous concussion (RR=3.64; 95% CI: 2.68 to 4.96; p<0.0001; I 2=90.55%). Unreported sex-stratified data precluded direct comparison of concussion risk in male versus female athletes.
Conclusion Previously concussed children have four times the risk of sustaining a concussion compared with those with no previous concussion history. This should be a consideration for clinicians in return to sport decision-making. Future studies examining subsequent recurrent concussion in youth sports must consider sex differences.
- concussion
- children
- risk factor
- sporting injuries
- recurrent
Statistics from Altmetric.com
Introduction
Widespread media attention on the impact of concussion in professional athletes has increased public concern about the sequelae and consequences of concussion.1 One to two million children under 18 years of age sustain a sport-related or recreation-related concussion in the USA every year.2 With over 30–45 million children participating in non-scholastic organised sports and 7.6 million adolescents participating in high-school athletics in the USA each year, youth represent the highest at-risk group for injury.3 4 The highest risk of sustaining a concussion is in collision sports such as rugby, ice hockey and American football, with incidence rates ranging from 0.5 to 4.2 concussions per 1000 athlete exposures.5–7 In sex-comparable sports, adolescent females may be at a greater risk of both sustaining a concussion8–10 and experiencing higher symptom burden,9 11 delayed symptom recovery12–14 and greater impairments in reaction time, processing speed and executive function9 10 compared with their male counterparts.
Compared with college and professional athletes, adolescents appear more vulnerable to concussion and take longer to recover due to neurological immaturity, thinner cortical skull bones and weaker supportive neck musculature.15–19 This is particularly concerning given the preventable nature of the injury in a critical period of neurological development. Furthermore, adolescents are more susceptible to the rare, but catastrophic, effects of second impact syndrome if they return to high-risk activities prematurely and sustain an exacerbation while still symptomatic from the initial concussion.20 Although the majority of concussion research involves college and professional athletes, existing return to sport (RTS) guidelines developed to reduce risk of subsequent injury assume recommendations apply equally to all ages.21 These guidelines allow return to physical activity (eg, walking, low-risk activities) early on, but require medical clearance for RTS (eg, unrestricted contact, competition, high-risk activities), only once the athletes are asymptomatic.
A previous history of concussion has been associated with an increased risk of any injury,22 risk of concussion15 22 and risk of lower extremity musculoskeletal injury22–24 compared with those without a previous history of concussion. However, existing systematic reviews have either focused on adult populations (college football and hockey athletes, and military personnel),22 or did not present adult and paediatric results separately,15 limiting applicability to children. The primary objective of this systematic review was to examine the risk of concussion in children aged 5–18 years who had experienced a previous history of concussion compared with those with no previous lifetime history of concussion. Our secondary objective was to compare the risk of concussion in children with a previous history of concussion compared with no previous history of concussion, stratified by sex.
Methods
Study identification: data sources and search strategy
This systematic review was registered a priori with PROSPERO (No CRD42019135462) at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=135462 and was reported according to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.25 We focused on risk of concussion exclusively as there was only one identified study that examined risk of (lower extremity) musculoskeletal injury following concussion. Four electronic databases were searched: MEDLINE including Epub Ahead of Print, In-Process & Other Non-Indexed Citations (1946 to 21 May 2019) and Embase (1947 to 21 May 2019) using the Ovid interface. CINAHL and SPORTDiscus were searched 22 May 2019 using the EbscoHost interface (database dates not provided). Database-specific search terms for the concept of concussion were peer reviewed as part of an earlier systematic review.26 We updated our search in MEDLINE and Embase to include the term *exacerb*.mp to be comprehensive and advance consistency of terminology adopted by the International Consensus Statement on Methods for Recording and Reporting of Epidemiological Data on Injury and Illness in Sport 2020 that was published after our original literature search.27 Search strategies are presented in online supplemental appendix 1. Searches were designed and conducted by a librarian experienced in systematic reviews, using a method designed to optimise term selection.28 References of included studies and relevant systematic reviews were manually searched and newly identified records were integrated into the set for screening.
Supplemental material
Study selection criteria
Studies were included if they were original peer-reviewed English publications that reported risk of concussion in children aged 5–18 years with a previous history of concussion compared with those with no previous lifetime history of concussion and reported effect estimates routinely used as measures of injury risk (ie, risk ratio (RR), OR, HR, incidence rate ratio)29 that provided sufficient data for RRs to be calculated. As per consensus recommendations, a recurrent concussion was considered a subsequent injury ‘to the same location and tissue as the index injury’, where the ‘index injury was healed/fully recovered’.(p375).27
Studies were excluded for the following reasons: (1) history of moderate-to-severe traumatic brain injury; (2) no documented, self-reported, or parent-reported head trauma; (3) non-sports-related injury; (4) evidence of structural injury or intracranial bleeding on neurodiagnostic imaging (if available); (5) head and orthopaedic injuries not reported separately; (6) child and adult data not reported separately in a mixed-age cohort; and (7) case reports, case series with n<10, letters to the editor, abstracts or conference proceedings.
Duplicate records were removed online. Records were downloaded and imported into a Reference Manager database where a second deduplication process was undertaken, and then uploaded to InsightScope. Records were appraised against the inclusion criteria using a three-step approach. Two independent reviewers screened titles/abstracts of citations resulting from the search strategy to identify potentially relevant studies. In the event that no abstract was available, the full text was reviewed to ensure relevant studies were not missed. Full texts were then assessed for eligibility by two independent reviewers according to pre-established inclusion/exclusion criteria. When there was disagreement, the two reviewers reached consensus through collaborative discussion without the need for a third reviewer.
Data extraction
Two independent reviewers extracted the following information into a standardised data extraction form: author, year of publication, study design, country, length of exposure, study population (age, sex, sport, recruitment source), sample size, outcome measured and injury definition. We extracted data count and both unadjusted and adjusted measures of association with 95% CIs. Effect estimates were reported based on describing increased risk of concussion. Where sex-stratified results were not published, we contacted the authors to obtain the raw data needed to make the calculations.
Assessment of risk of bias
Risk of bias was independently assessed by two reviewers using the Newcastle-Ottawa Scale (NOS).30 The NOS comprises eight criteria across three categories (maximum score nine stars) assessing selection criteria, comparability and exposure for case–control studies, and selection criteria, comparability and outcome for cohort studies. A high score indicates a low risk of bias. Discrepancies in scoring were resolved by discussion and consensus obtained between the two reviewers.
Data synthesis and meta-analysis
We performed a random effects meta-analysis to pool RRs across the studies and the results are summarised in a forest plot. When data (event count and sample size) were available, we calculated the RR for the studies before pooling, otherwise, we used the RR and its CI reported in the study. If both adjusted and unadjusted RRs were provided, we used the unadjusted values. When ORs were reported, we converted ORs to RR, where the control event rate was imputed from studies that provided data for the control group (no previous history of concussion). Statistical heterogeneity across studies was estimated using the I2 statistic, with 25%, 50% and 75% considered low, medium and high heterogeneity, respectively.31 Analysis was performed using the metafor Package in the R Statistical Software.32 33 An RR >1 indicated that the risk of subsequent injury is higher in children with a previous concussion. Statistical significance was determined at a level α=0.05.
Sensitivity analysis
To address our secondary objective, we intended a priori to calculate sex-stratified risk estimates (RR (95% CI)) to compare with our overall estimate of risk of concussion.
Results
Study identification
The search strategy identified 911 studies, of which 732 titles and abstracts were screened (level one screening) after duplicates were removed. We assessed 34 full texts (level two screening) for eligibility and retained seven studies for meta-analysis (figure 1).

PRISMA 2009 flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses
Risk of bias assessment
Based on the NOS, the risk of bias was low for all studies (range, 7–9; maximum possible score=9, table 1). A single (14%) study34 described using structured injury data to ascertain risk exposure and 6 (86%) studies34–39 demonstrated that participants were not concussed at the start of the study. Although several cohort studies adjusted for multiple potential confounders, including age, 5 (71%) studies37–40 did not adjust for previous history of mental health in their analysis. One retrospective cohort study36 lacked a systematic method for tracking concussion injuries.
Risk of bias for cohort studies as assessed with the NOS
Characteristics of included studies
The seven retained studies represented 23 411 children. Six (86%) were prospective cohort studies (n=1359 children with a previous concussion; n=11 762 children with no previous concussion), and 1 (14%) was a retrospective cohort study (n=1710 children with a previous concussion; n=8580 children with no previous concussion, table 2). The number of participants in a study ranged from 15837 to 10 290.36 Two (29%) studies37 40 included males only and 4 (57%) studies34 35 38 39 included at least 96% male athletes. None of the studies reported sex-stratified results. None of the authors provided the raw data after being contacted. Participants were recruited from American football (n=3; 43%),35 37 40 middle and high-school sports (n=1; 14%)36 and (hockey (n=3; 43%).34 38 39 Length of follow-up ranged from 1 to 2 sport seasons.
Study characteristics
Risk of concussion
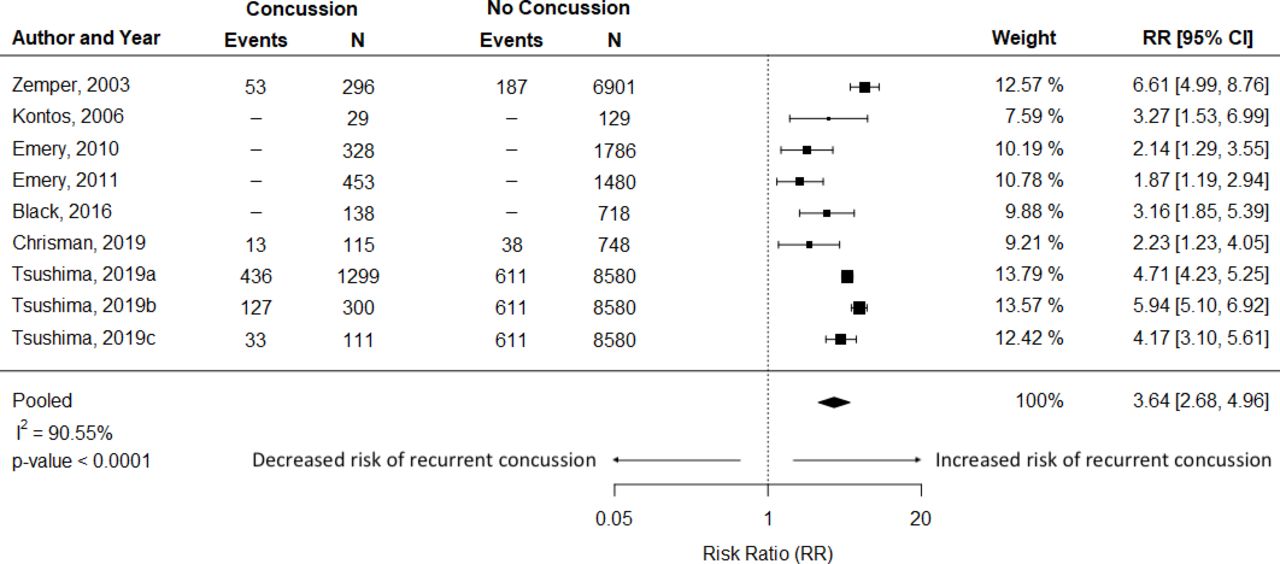
Overall pooled risk of sustaining a concussion was four times greater in children with a previous concussion compared with those with no history of concussion (RR=3.64; 95% CI: 2.68 to 4.96; p<0.0001; I 2=90.55%, figure 2). All studies showed a statistically significant increase in risk of concussion among previously concussed athletes (RR (95% CI)) ranging from 1.87 (1.19, 2.94) to 6.61 (4.99,8.76). Despite high statistical heterogeneity (I 2=90.55%), we decided to proceed with performing a meta-analysis since six of the seven concussion studies utilised the same study design (ie, prospective cohort studies), applied similar validated diagnostic criteria for concussion (ie, Fourth International Consensus Conference on Concussion in Sport or American Academy of Neurology),41 42 assessed primarily American Academy of Pediatrics defined contact or collisions sports43 shown to have a high risk of concussion (eg, football, hockey),6 7 and followed children for one or two seasons.

Forest plot of RR of recurrent concussion following index concussion for all included studies. The RR(95% CI) from individual studies and the pooled data are shown. Box size represents the relative weight each study contributes to the pooled estimate. RR >1 indicates greater risk of recurrent concussion for children with a previous lifetime history of concussion compared with those without a previous concussion. Tsushima 2019a presents the RR for youth with one previous concussion; Tsushima 2019b presents the RR for youth with two previous concussions; and Tsushima 2019c presents the RR for youth with three plus previous concussions. RR, risk ratio.
Based on the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework,44 there is a low level of certainty that the true risk of concussion is close to the estimated effect. However, several studies included large sample sizes with large numbers of events (concussions) and included studies were deemed to have a low risk of bias with similar point estimates and overlapping 95% CIs, which demonstrates consistency of findings. Confidence in the evidence may likewise be increased as Tsushima et al 36 reported a greater risk of recurrent concussion following two previous concussions than after a single concussion, suggesting there may be a dose response.
Risk of concussion, stratified by sex
Sex-specific results were not reported in any of the studies, and authors were unable to provide the requested raw data, therefore we performed a post-hoc meta-analysis consisting of studies with 96% or more male participants.35 37–40
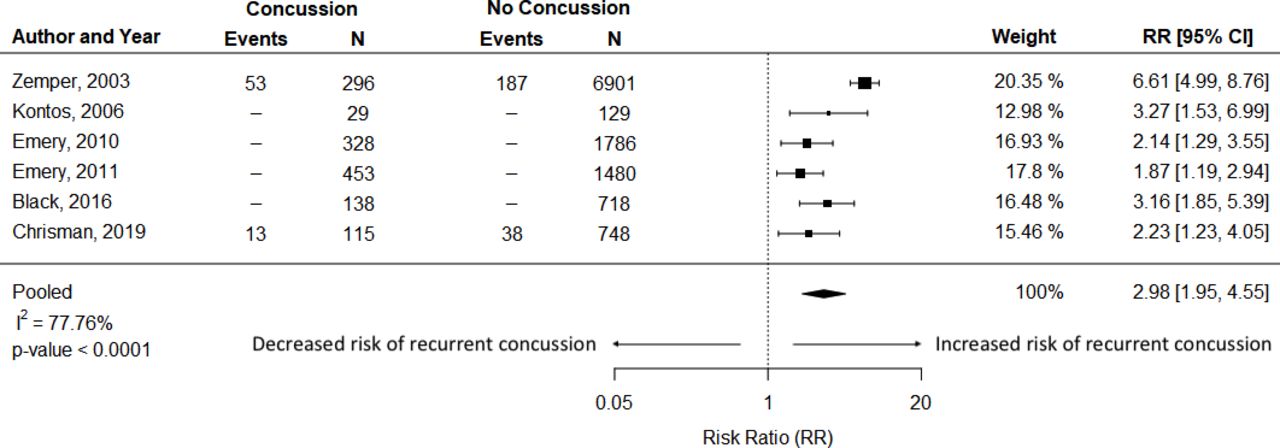
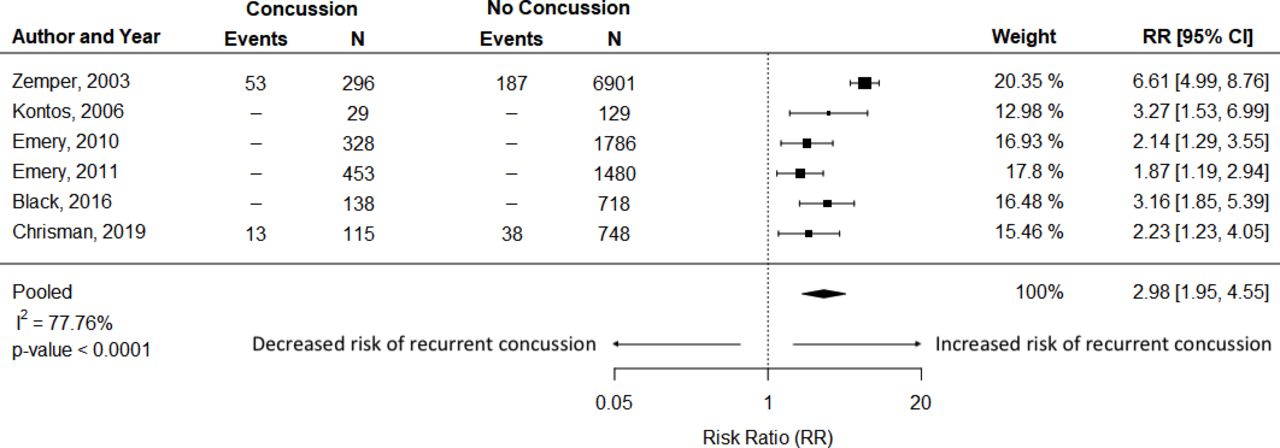
In a sensitivity analysis of a predominantly male population of youth athletes with and without a previous history of concussion, the point estimate for risk of concussion was lower (RR=2.98; 95% CI: 1.95 to 4.55; p<0.0001; I 2=77.76%, figure 3) when compared with our overall estimate (RR=3.64; 95% CI: 2.68 to 4.96; p<0.0001; I 2=90.55%). However, the considerable overlap in the CIs with our overall estimate limits interpretation of the findings regarding risk differences. Furthermore, although the sensitivity analysis lowered the statistical heterogeneity of the pooled estimate, it still remained high.
{kind=link}
{kind=link}
{kind=link}
Forest plot of RR of recurrent concussion following index concussion for predominantly male studies (≥96% male). The RR (95% CI) from individual studies and the pooled data are shown. Box size represents the relative weight each study contributes to the pooled estimate. RR >1 indicates greater risk of recurrent concussion for children with a previous lifetime history of concussion compared with those without a previous concussion. RR, risk ratio.
Discussion
This systematic review of high-quality studies, that included more than 3000 children under 18 years of age with a previous concussion and more than 20 000 children with no previous concussion, demonstrated that children who RTS following concussion are at nearly four times greater risk of sustaining a concussion relative to those with no previous concussion.
These findings extend previous systematic reviews that concluded previous concussion is a risk factor for sustaining a concussion across a wide range of ages and populations.15 22 In a predominantly adult population that included athletes and military personnel, the pooled odds of sustaining a concussion were 3.73 times higher in those with a previous concussion. A single narrative review of sport-related concussions concluded there was a high level of certainty that previous concussion increases concussion risk, but no pooled estimate was calculated.15 Although the estimated concussion risk was similar in our study, youth athletes have a higher overall incidence of concussion compared with college athletes. In a large prospective cohort study45 with over 1000 reported concussions, high-school football players had twice the rate of concussions per 1000 total athlete exposure as Division I college players (1.03 vs 0.49).
Possible factors to explore in future research to study this difference may include rule changes, equipment standards, concussion assessment techniques, reduced practice contact and awareness of concussion protocols. Furthermore, the incidence of recurrent concussion is likely underestimated, as approximately 50% of all concussions in youth may be unreported as a result of fear of being removed from a game, not wanting to let down teammates, lack of knowledge around common concussion signs and symptoms or not thinking they were serious enough to seek medical attention.46 47
Our data suggesting a threefold to fourfold greater risk of concussion among previously concussed children may be an underestimate. Some previously concussed children may not have returned to their sport within the study periods due to persistent symptoms and these athletes would be more vulnerable to repetitive head trauma on RTS, especially if physiological recovery is delayed beyond recovery of self-reported symptoms.48
Increased cerebral vulnerability may lead to either an exacerbation of symptoms from the index concussion or a reinjury. This is concerning, as recurrent concussions in adolescents have been associated with a greater severity of on-field signs and symptoms (loss of consciousness, anterograde amnesia, confusion),49 prolonged symptom recovery14 50 and higher baseline symptom reporting,51–54 and dynamic motor function deficits.55 It is unclear whether this represents a cumulative effect of multiple concussions, incomplete physiological recovery or neurological predisposition to injury. The high annual incidence of paediatric concussions sustained yearly translates into preventable morbidity for a substantial number of youths. Our findings suggest children have an increased vulnerability to recurrent concussion. We highlight the importance of establishing age-specific timelines for progression through established RTS medical clearance protocols to mitigate the risk.
Sex-specific differences
Understanding sex-specific differences in concussion risk was an important secondary objective of this study. It is noteworthy that few studies in this review included a meaningful number of females. Regrettably, none of the included studies provided sex-specific concussion rates, therefore we cannot determine whether differences in concussion risk exist between previously concussed male and female athletes compared with same-sex athletes with no previous concussion. Although we calculated a lower point estimate of concussion risk in a predominantly male population, further research is needed to determine whether sex-specific differences account for a variance in the RR given the significant overlap in CIs and high percentage of males (81%) in the overall population. Similar to previous reviews7 56 57 exploring a wide range of outcomes associated with concussion, a general lack of reported differences in risk between males and females precluded inference and represents a critical gap in the literature.
Possible sex differences that might account for these findings include lower injury thresholds,58 neck strength,59 injury biomechanics,60 women report more symptoms11 61 and hormones.58 62 Given high levels of female sport participation and a 6.3-fold increase in rate of overall child and adolescent concussion from 2003 to 2013,63 large prospective cohort studies reporting point estimates and associated 95% CIs comparing males and females with a previous concussion to non-concussed counterparts are needed to understand the effect of sex on concussion risk.
Explanations for increased susceptibility to concussion in youth
Although evidence suggests that a previous concussion increases the risk of concussion, our understanding of the underlying physiology behind this continues to evolve. Possible explanations include residual physiological effects from the primary concussion, microstructural injury, structural factors, genetic predisposition, impaired neuromotor control and sensorimotor deficits.7 17 24 55 64–71 A neurometabolic cascade of events that include ionic shifts, metabolic energy deficits, cytoskeletal damage, axonal dysfunction, altered neurotransmission, altered blood flow and inflammation has been associated with increased vulnerability to recurrent concussion.66 67 Animal models and human studies suggest allowing increased time for recovery following concussion reduces metabolic vulnerability and severity of neurocognitive dysfunction.66 67 While this aligns with current clinical guidelines for immediate removal from play following a concussion and a graduated exercise strategy to allow for physiologic recovery, age-specific and sex-specific timelines for safe RTS are still unclear.
Impaired neuromotor control and cognitive processing have also been cited as potential risk factors23 with possible cumulative effects.55 Lingering deficits may impair an athlete’s ability to simultaneously integrate cognitive demands with postural strategies required to safely react to their environment during sport.55 Preliminary evidence that concussion risk can be reduced with a neuromuscular training programme offers promise as a potential prevention strategy.71 Additionally, deficits in cervical spine proprioception, vestibular–ocular function and visual systems following concussion can reduce postural stability.64 65 Persistent impairments in dynamic postural stability months following concussion may result in altered movement strategies that increase recurrent concussion risk.24 Individualised cervical and vestibular physiotherapy have been shown to decrease time to RTS medical clearance following concussion; further research is needed to determine any protective effect against recurrent concussion.70
This study has several strengths that bolster the validity of our findings. To our knowledge, this is the first systematic review of risk of concussion following paediatric concussion. Multiple databases were searched along with reference lists of relevant studies. Study selection and data extraction were done independently. Additionally, all included studies were rated as high quality of evidence and study populations were large for most studies. All studies show substantial effects with evidence of some dose–response relationship.
These results should be considered in the context of the following limitations. First, as with all systemic reviews, the risk of publication bias must be considered, which may have overestimated the estimated risk of concussion. Second, there was significant heterogeneity between studies when calculating our pooled estimate. Some of the heterogeneity may be explained by sex differences, as heterogeneity (I2 ) fell when we calculated the risk estimate for male-dominant studies. We also calculated an unadjusted risk estimate due to wide variations between studies in controlling for relevant covariates, which may explain some of the heterogeneity.72 For example, Kontos et al 37 controlled for learning disabilities and attention-deficit/hyperactivity disorder in the study design, whereas Emery et al 38 39 and Black et al 34 controlled for year of play, player size, level of play and body checking attitude in their analysis; Tsushima et al 35 36 and Chrisman controlled for sex. Age of participants may also have contributed to heterogeneity, as those studies that included children aged 5–12 years had a lower RR (range, 2.14–2.23) than three out of four studies that included adolescents aged 13–18 (range, 3.27–6.61). The heterogeneity may also be associated with calculating the unadjusted RR using count data in studies where either ORs35 37 or incidence rate ratios34 38 39 were reported. However, these studies were sufficiently similar in design, diagnostic criteria, sport type and follow-up period to be reasonably confident in our findings. Third, selection bias may have been introduced due to the small number of female athletes (n=4491; 19% of total sample) included in the overall meta-analysis, almost exclusively from the only retrospective study (n=4396; 98% of total females), thereby limiting the generalisability of the results to females. Furthermore, our sensitivity analysis precluded definitive conclusions regarding sex-specific differences in concussion risk. Fourth, risk of concussion may differ based on time since previous concussion or clinical markers of recovery, however we were unable to study that as several studies failed to report clearly defined RTS clearance criteria or time interval between first and recurrent concussions. Fifth, measurement bias may have been introduced related to concussion exposure, potentially leading to substantial bias in the risk estimate. Despite rigorous injury surveillance systems used across all studies, differences in type of athlete exposures were not consistently reported or included in statistical modelling, despite the higher risk of concussion in competition than in practice.73 Sex-specific differences in concussion rates during games versus practices should be considered in future research. Similarly, although athletes with a suspected concussion were assessed using a standard definition of concussion, the lack of objective diagnostic biomarker raises the possibility of misclassification or non-detection.
Finally, given the small number of studies found, we could not further explore important facets of this topic including sex differences (males dominated), differences across sport, geography and culture (most studies were done in the North American context and focused on football and ice hockey) or age groups (only one study examined effects in children under 10, who may be experiencing rapid neurodevelopmental changes), making it unclear whether our results are generalisable. Despite these limitations, statistical agreement across all studies based on individual point estimates and 95% CIs (although varied in size) and high quality of included studies support our finding of increased risk of concussion in youth with a previous concussion.
Clinical and research relevance
Clinicians must consider previous concussion history when making RTS clearance decisions and educate families regarding the increased risk of concussion in youth. Although timelines for safe RTS following paediatric concussion have not yet been determined, current international guidelines recommend that once athletes are symptom-free, they should complete a six-stage graded exercise strategy to allow for fuller recovery before returning to at-risk activities.21 Efficacy of this strategy in reducing recurrent concussions has not been investigated. As per expert consensus, medical clearance decisions rely primarily on symptom reporting, which has been shown to resolve before neurocognitive status and functional balance. This highlights the need for further research to identify modifiable risk factors that can be assessed, mediated through intervention and required for medical clearance. There is also a strong need to identify objective biomarkers of recovery and their role in predicting recurrent concussion. Identification of ongoing functional disturbances and microstructural injury within advanced neuroimaging and fluid biomarker research appears promising; however, clinical application requires further validation before implementation in concussion management.74 In the meantime, clinicians should consider managing children with concussion more conservatively than adults as the increased risk of concussion is even more concerning given children’s previously established potentially increased vulnerability to concussion, potentially longer recovery times and potential for adverse long-term consequences during a sensitive period of neurodevelopment growth.15–19 Since current management of paediatric concussion is based on evidence from animal and adult human research, future consensus guidelines need to consider evidence-based age-specific and sex-specific recommendations for RTS following paediatric concussion.
Conclusion
Children with a previous concussion are at a greater risk of concussion after returning to sport compared with children with no history of concussion. Understanding the cause and timeline of increased risk is essential in order to inform age-specific RTS guidelines. Future studies examining concussion risk in youth sports must consider sex-specific differences. Further research is needed to determine objective markers of physiological recovery, identify clinical risk factors for recurrent concussion in children, evaluate evidence-based prevention strategies to mitigate concussion risk, inform medical clearance decision-making following concussion and reduce the long-term sequelae of multiple concussions.
What is already known?
Incidence of youth diagnosed with concussion has quadrupled in the last decade.
College athletes with a history of concussion are at an increased risk of subsequent injury, including recurrent concussion and lower extremity injury.
What are the new findings?
Having a lifetime history of concussion is associated with a four times greater risk of concussion in children.
A paucity of evidence on risk of concussion in girls aged 5–18 years is a major shortcoming in existing research.
Acknowledgments
We thank Katie O'Hearn, Msc, (Children’s Hospital of Eastern Ontario Research Institute) for methodological assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JvI, MS and RZ contributed to the conception or design of the work. JvI, MO and JH collected the data. JvI, MO and JH contributed to the analysis and interpretation of the work. Jvl drafted the manuscript. MO, MS, JH and RZ critically reviewed the manuscript for important intellectual content. All authors approve of the final version and agree to be responsible for all aspects of the work ensuring accuracy and integrity.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Jvl reported receiving speaking honoraria and travel expenses for presentations at scientific meetings; and is founder and an instructor for R2P Concussion Management. RZ reported being a coapplicant on a competitively funded grant administered by the National Football League through the independent scientific advisory board to fund a prospective concussion study with the goal of preventing concussions; he does not personally receive any funding for this work; his institution receives the operating funds to conduct the research; he has received honoraria from Parachute Canada (a Canadian non-profit for injury prevention) for his role on the Concussion Expert Advisory board.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.