Article Text

Abstract
Elite athletes are particularly susceptible to sleep inadequacies, characterised by habitual short sleep (<7 hours/night) and poor sleep quality (eg, sleep fragmentation). Athletic performance is reduced by a night or more without sleep, but the influence on performance of partial sleep restriction over 1–3 nights, a more real-world scenario, remains unclear. Studies investigating sleep in athletes often suffer from inadequate experimental control, a lack of females and questions concerning the validity of the chosen sleep assessment tools. Research only scratches the surface on how sleep influences athlete health. Studies in the wider population show that habitually sleeping <7 hours/night increases susceptibility to respiratory infection. Fortunately, much is known about the salient risk factors for sleep inadequacy in athletes, enabling targeted interventions. For example, athlete sleep is influenced by sport-specific factors (relating to training, travel and competition) and non-sport factors (eg, female gender, stress and anxiety). This expert consensus culminates with a sleep toolbox for practitioners (eg, covering sleep education and screening) to mitigate these risk factors and optimise athlete sleep. A one-size-fits-all approach to athlete sleep recommendations (eg, 7–9 hours/night) is unlikely ideal for health and performance. We recommend an individualised approach that should consider the athlete’s perceived sleep needs. Research is needed into the benefits of napping and sleep extension (eg, banking sleep).
- sleep
- athlete
- health
- performance
- consensus
Statistics from Altmetric.com
PREAMBLE
An ever-growing volume of peer-reviewed publications speaks to the recent and rapid growth in scope and understanding of sleep for optimal athlete health and performance. More than 80% of all peer-reviewed publications on this topic have been published in the last 10 years (>1 000 papers using the search terms ‘sleep’ and ‘athlete’, Web of Science). Herein, a panel of international experts review the current knowledge on sleep and the athlete, briefly covering the background, exploring continued controversies, highlighting fruitful avenues for future research and providing practical recommendations.
The introduction section covers the need for sleep, including sleep architecture and the restorative benefits of sleep for the brain and body. Pitfalls and challenges measuring athlete sleep are reviewed, and practical recommendations provided. The following section, entitled sleep and the athlete, covers the influence of sleep inadequacy and sleep extension on athletic performance. We review the evidence that elite athletes are particularly susceptible to sleep inadequacy, for example, during intensified training and in those reporting symptoms of over-reaching and overtraining. The final section, entitled strategies to improve sleep, provides practical recommendations to alleviate the symptoms of jet lag, nutritional strategies to enhance sleep and a toolbox for practitioners to manage and optimise athlete sleep.
Introduction
The need for sleep
Normal human sleep comprises two main types—non-rapid eye movement sleep (non-REM) and REM sleep.1 Non-REM sleep is divided into three stages, representing a continuum from ‘light’ sleep in stages 1 and 2, through to ‘deep’ sleep in stage 3.2 The duration and composition of normal sleep changes across the life cycle. At the ages most relevant to aspiring and established athletes, a sleep of 8–10 hours for an adolescent (aged 15 years) contains approximately 57% light sleep, 22% deep sleep and 21% REM sleep; and a sleep of 7–9 hours for a young adult (aged 30 years) contains approximately 61% light sleep, 16% deep sleep and 23% REM sleep.3
Sleep is essential for the brain and the body. Protocols with one or two nights of total sleep deprivation or 1 or 2 weeks of partial sleep restriction have been used to demonstrate the importance of sleep for both mental and physical health. In particular, sleep loss impairs cognition,4 learning and memory consolidation5 and mental well-being6; it disrupts growth and repair of cells,7 metabolism of glucose8 and lowers the protective immune response to vaccination9 10 and resistance to respiratory infection (see online supplemental file 1 for more extensive review on the need for sleep).11
Supplemental material
Measuring sleep
With the increasing popularity of measuring sleep within both medical and consumer fields, unsurprisingly, the number of sleep measurement tools is rapidly increasing (table 1). Some of the more common measurements regarding sleep include: sleep architecture (sleep staging), sleep duration, measured or estimated sleep efficiency (quality), sleep-onset latency (SOL: time taken to fall asleep) and wake after sleep onset (WASO). Sleep can be measured both objectively (polysomnography, activity monitoring, smartphone applications and nearable devices placed on or near the bed) and subjectively (sleep diaries and questionnaires) and has been reviewed elsewhere (see online supplemental file 1 for more extensive review on measuring sleep).12
Evaluation of tools for sleep assessment in athletes
Polysomnography
Polysomnography is considered the gold standard of sleep monitoring and typically includes an assessment of eye movement, brain activity, heart rate, muscle activity, oxygen saturation, breathing rate and body movement.13 Polysomnography allows for the determination of REM and non-REM. As polysomnography can be an expensive, obtrusive and complex technique, it is typically used for the assessment of sleep disorders or in research studies.
Activity monitoring
Activity monitors are wearable devices that record movement,14 with most using a 3-axis accelerometer to determine sleep/wake based on a specific algorithm.15 Currently, there are generally two classifications of devices—those that are considered ‘research-grade’ (validated against polysomnography)16 and those that are considered ‘commercially available’. Both research-grade and commercially available activity monitors typically overestimate sleep duration relative to polysomnography (and underestimate relative to recall and sleep diary), underestimate awakenings and WASO relative to polysomnography (and overestimate relative to recall and sleep diary), and generally underestimate sleep latency relative to both polysomnography and sleep diary.17
Nearables and smartphone applications
One subset of nearable devices is placed on the mattress and measures movement and other physiological signals of the individual lying on the bed (typically using ballistocardiography).18 19 Currently, validation of available devices is sparse, little is known about the algorithms used, and these devices are not considered accurate for measuring sleep.20 In general, smartphone apps are poor at determining sleep stages and sleep parameters15 and researchers have little room to influence or access raw data.21 22
Sleep diaries and questionnaires
Sleep diaries can be a simple and cost-effective means of assessing sleep and typically include: bed and wake time, lights-out time, daytime napping, ratings of sleepiness and alertness, caffeine and alcohol intake, exercise and light emitting device use23 for a duration of at least 1 week. Questionnaires are often used for screening purposes or an initial assessment of sleep due to their ease of administration and low cost. Common questionnaires in insomnia research include: the Pittsburgh Sleep Quality Index (PSQI) to assess sleep quality,24 the Sleep Hygiene Index to assess sleep hygiene25 and the Epworth Sleepiness Scale26 to assess daytime sleepiness. However, these questionnaires have not been validated for athletes (table 1). Athlete-specific questionnaires include the Athlete Sleep Screening Questionnaire27 28 and the Athlete Sleep Behaviour Questionnaire.29 Similar to sleep diaries, while questionnaires may be time and cost effective, response biases may exist.
In summary, there are increasing options for scientists and athletes to monitor sleep, with some devices (primarily consumer sleep technology) having some limitations in their assessment of sleep and wakefulness. Consideration should be given to whether or not the devices are validated, and an assessment is required as to the usefulness and appropriateness of using unvalidated technology. Some devices may provide some basic level of sleep awareness and education; however, individuals should be cognisant of the limitations of available means of monitoring sleep (table 1).
Sleep and the athlete
Sleep and athletic performance
Sleep disturbance is a common occurrence prior to competition that may impact athletic performance.30 Discerning the effects of sleep disturbance on athletic performance is difficult across studies, given the wide variety in study designs, populations, conditions, measuring tools and reported outcomes. To best ascertain the quality of evidence for studies investigating the relationship between sleep and athletic performance, it is recommended to separate experimental outcomes between partial (ie, partial restriction or acute improvement in sleep for 1–3 nights) and complete (ie, sleep deprivation/loss) changes in sleep quality or quantity.
The effect of sleep restriction and acute sleep improvement on athletic performance
The effect of sleep restriction and acute sleep improvement on performance is equivocal for strength31 and exercise performance.32 Such mixed results may be a result of differences in sleep protocols,33 as well as the time of testing. For example, if performance is assessed towards the end of the day (eg, 17:00–19:00 hours) the circadian drive for alertness/performance may limit the effect of sleep restriction on performance.34 In addition, the time of sleep restriction (eg, prolonged wake vs early rising) can vary between studies,33 35 with collective evidence suggesting that sports-specific skill execution, submaximal strength and anaerobic power can decline, however, there are many instances in which performance is maintained (eg, maximal aerobic or strength efforts).33 Few studies have assessed the effect of acute sleep enhancement on athletic performance,36 with preliminary evidence showing positive benefits for strategies such as sleep hygiene. For example, strategies that focus on improving the sleep environment (removal of light, technology and noise, 17°C–22°C temperature) have shown improvements in sleep duration, although most studies report limited benefits to sports performance.36 Comparatively, studies have shown sleep extension improves sport-specific skill execution,37 as well as sprint performance,38 however, these studies often lack objective measures of sleep or a control group. From a practical perspective, naps offer a suitable strategy to supplement lost sleep, with 20–30 min naps improving sprint39 and peak jump velocity performance.40
Sleep deprivation, chronic sleep improvement and athletic performance
There is sufficient evidence to suggest a detrimental effect of sleep deprivation (a night or more without any sleep) and a beneficial effect of chronic sleep improvement (repeated exposure of strategies that improve sleep over weeks or months) on sport-specific and physical performance.33 36 41 Thus, avoiding situations that present large risks to sleep, and promoting long-term behaviours that improve sleep quantity and quality is encouraged (box 1). While study findings emphasise the importance of positive long-term sleep behaviour for sporting performance,42 43 there are concerns with the available evidence. For instance, it is uncommon for sleep studies to include a control group; as such, studies showing improvements in physical performance with sleep extension should be considered with caution. Large discrepancies in sleep protocol duration and timing make it difficult to determine the performance effect of sleep interventions. Of further note, it is debatable whether the findings of the detrimental effects of sleep deprivation on performance are applicable to elite athletic populations, given it would be rare for athletes to endure a night or more without any sleep. Other issues include an underrepresentation of female athletes, differences in quantification of performance and experimental environments, the inability to blind subjects and imprecision and/or lack of adequate description of the sleep intervention protocol.
Sleep and athletic performance: five key recommendations
Avoid situations that present ongoing risks to sleep; promote positive habitual sleep behaviour.
When incorporating strategies to enhance sleep or performance in the field setting, take account of other factors that may impact results (eg, ongoing illness).
Researchers are encouraged to take on the responsibility for improving the quality of evidence on sleep and athletic performance (eg, reporting of randomisation procedures, protocol adherence and handling of missing outcome data). We recommend a research methods consensus meeting be held.
We recommend researchers report baseline athlete sleep behaviour (eg, sleep inadequacies) to better characterise the effect of targeted sleep interventions on athletic performance. Practitioners are encouraged to target specific individuals in need of help and/or address specific situations for those at risk (ie, situations known to compromise sleep, for example, travel).
Future research needs to focus on: (1) sleep interventions that assess strength outcomes in athletic populations; (2) longer (eg, more repetitive) periods of sleep restriction and sport-specific measures of performance and (3) randomised controlled trials on sleep and (1) performance at differing times of the day (eg, early morning heats in Olympic swimming) and (2) differing tasks—meaning differing sports and different elements that contribute to sporting success.
Adequately controlled investigations are required to fully explore the influence of sleep extension on athletic performance and health. A recent study of a small group of trained cyclists and triathletes, showed better endurance performance after three consecutive nights of sleep extension (~8.4 hours sleep each night) compared with habitual sleep (~6.8 hours sleep each night); prompting the authors to recommend endurance athletes sleep >8 hours each night to optimise performance.44 The degree to which the ergogenic effect of sleep extension varies as a function of habitual sleep is important to determine (ie, repaying a recent sleep debt or a real effect of banking sleep?).45 Other unresolved questions include: whether sleep extension (eg, targeting >8 hours each night) should be recommended for all athletes, across all sports and event types (viz. ‘one-size-fits-all’); whether sleep extension increases sleep inertia (eg, grogginess on waking), with detrimental effects on postwaking performance46; whether there is a ceiling effect (eg, for total sleep time, slow-wave sleep or REM sleep) beyond which no further performance or health benefit is gained; or whether too much sleep can have negative effects on performance or health. Reductions in sleep efficiency and sleep quality with sleep extension44 might conceivably have detrimental effects on athlete immunity.47 48
From a practical perspective, there appears minimal harm in attempting to improve sleep or minimise situations which compromise sleep over long periods to improve performance outcomes. Our five recommendations (Box 1) also offer additional benefits on overall health and mental well-being,49 as discussed elsewhere in this review.
Sleep inadequacy and the athlete
The prevalence of sleep inadequacy has been reported to be high among elite athletic populations who often experience disruptive training and competition schedules that limit the opportunity for sleep. This is characterised by habitual sleep durations <7 hours,50 sleep dissatisfaction,51 unrefreshing sleep,52 long SOL,52 53 day-time sleepiness54 and day-time fatigue.55 Studies reporting global sleep quality show that 50%–78% of elite athletes experience sleep disturbance and 22%–26% suffer highly disturbed sleep.30 43 54
Definitive evidence that sleep inadequacy is more prevalent in elite athletes than the wider population is in short supply. Only a small handful of studies have included non-athletic controls to allow this comparison,56–58 and these controls were not always representative of sleep characteristics in the wider population.56 In addition, studies have tended to rely on subjective rather than objective measures of sleep (table 1).56 57 Using sleep questionnaires, one such study reported a higher prevalence of poor sleep quality and a greater proportion of morning types among elite Canadian athletes compared with non-athletic controls; although, the controls were selected from previous studies and screened to include only good sleepers (PSQI <5).56 Another study using sleep questionnaires reported no differences in chronotype distributions between elite Australian athletes and non-athletic controls.57 Notwithstanding, objective sleep assessment using actigraphy showed shorter sleep duration and poorer sleep quality (eg, sleep efficiency and sleep latency) in 47 British Olympic athletes compared with age and gender matched non-athletic controls.58 The empirical evidence also indicates that clinical sleep problems are prevalent in high level athletes. For example, a recent systematic review profiling sleep characteristics in elite athletes highlighted the prevalence of insomnia symptoms (eg, longer sleep latency, greater sleep fragmentation, non-restorative sleep and excessive day-time fatigue).30 Anecdotal evidence indicates that other sleep problems, such as sleep apnoea, are generally less common but do exist. The prevalence of obstructive sleep apnoea appears to be higher in strength and power athletes (eg, rugby players) than the non-athletic population. This is likely a consequence of large body mass and neck circumference, anatomical features consistent with sleep apnoea.54 59
Does participation in elite sport degrade sleep?
It remains to be shown whether a causal relationship exists between participation in elite sport and sleep inadequacy. Athlete sleep is influenced by various sport-specific factors and also by societal factors (eg, pervasive use of smart phones and social media in an ‘always connected’ society) (figure 1).30 60 Sport-specific risk factors for sleep inadequacy in athletes have broadly been identified as those pertaining to training, travel and competition (figure 1).30 61 More specifically, the risk factors include: high training loads62–64; short-haul and long-haul travel65 66; the night before competition67 68; evening competition (start times after 18:00)69 70 and early morning training (start times before 8:00).55
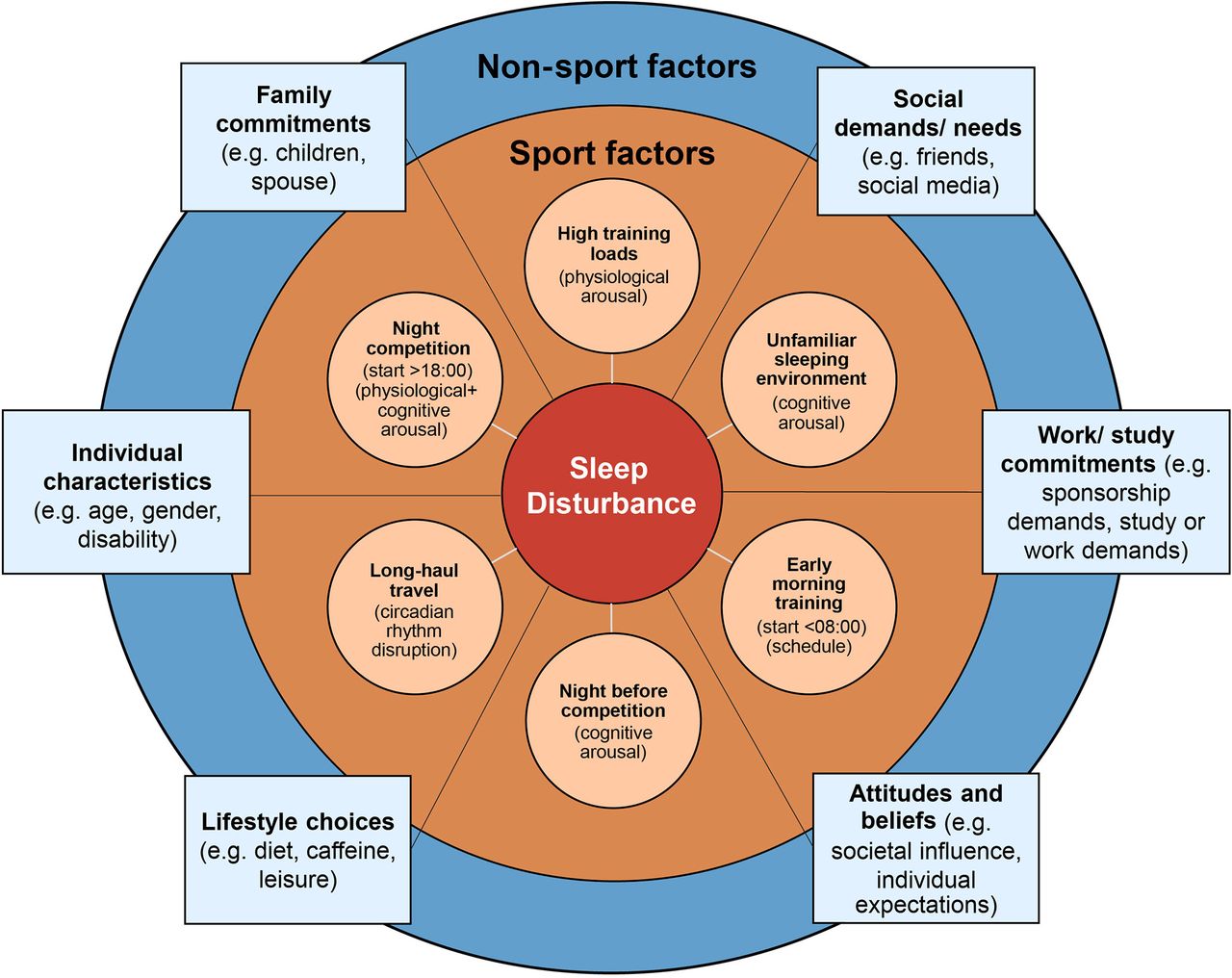
Contributory factors for sleep disturbance in athletes; including sport-specific factors (orange shading) and non-sport factors (blue shading).
Sport-specific risk factors for sleep inadequacy in athletes
The extent to which multiple factors challenge athlete sleep is unlikely to be uniform across all sports. Given both the specificity of athlete selection processes for different sports, and the different environmental and cultural constraints within different sports (eg, early morning training is engrained in swimming culture), it is reasonable to expect that athlete risk profiles and the challenges to athlete sleep vary between different sports.61 Although the available evidence is limited, one study reported that long-term sleep problems were particularly prominent in contact and combat sport athletes and in those participating in aesthetic sports.53 The underlying cause(s) of sleep problems in these athletes remains speculative but may include a history of concussion in contact and combat athletes71 72 and an influence of generalised anxiety disorder, negative perfectionism and low energy availability in aesthetic sport competitors.53 73 Energy restriction resulted in a hypometabolic state, affecting nocturnal body temperature and sleep patterns in overweight women.74 Studies are required to assess the influence of low energy availability on sleep patterns among athletes, particularly those participating in aesthetic and weight category sports. Research assessing actigraphy-derived sleep patterns in elite athletes has shown that individual sport athletes obtain less sleep than team sport athletes.75 Earlier training start times were proposed to account for shorter sleep duration in individual sport athletes, and retiring to bed earlier the night before early morning training does not appear to offset the reduction in sleep duration.35 Circumstantial evidence supports the notion that elite athletes tend to prevail in their chosen sport in part due to the matching of their chronotype with the sport-specific training schedules.57 An association between sport-type and chronotype distribution has been demonstrated in elite athletes, whereby a high proportion of morning types (72%) were involved in sports with early morning training schedules.57 Sport-type differences also become evident during high risk periods for sleep disruption, such as competition. For example, in a study of sleep habits in elite German athletes, precompetition sleep difficulties (eg, not being able to fall asleep) were more evident in individual compared with team sports.67
General risk factors for sleep inadequacy in athletes
Candidate risk factors for sleep inadequacy in elite athletes also include many of those factors commonly considered to influence sleep in non-athletic individuals. These include female gender,76–78 spinal cord injury,79 increasing age80 and poor mental health (eg, traits of neuroticism, maladaptive perfectionism and hyperarousal, and the pervasive influence of psychological stress and anxiety (rumination or worry)).81 Gender was identified as a risk factor for lifetime sleep problems in elite French athletes, with a greater incidence of sleep problems in female athletes.53 As is the case in non-athletic individuals, spinal cord injured athletes typically report poorer sleep quality than able-bodied athletes.30 79 Age has been shown to relate to the prevalence of poor sleep quality, with athletes>25 years of age reporting higher PSQI scores than those <20 years of age54; early parenthood could be a contributing factor.82 Athlete age was also identified as a risk factor for sleep disruption prior to a major competition, however normal sleep quality (eg, PSQI scores) was not.68 The latter finding indicates that athletes who typically report good sleep quality are not necessarily resilient against situational sleep disruption in the face of challenges, such as an important competition. Hyperarousal trait predicted actigraphy-derived reduction in sleep efficiency following a night game in elite netball players83; in the same way as non-athletes with hyperarousal trait are known to suffer reduced sleep quality in the face of psychosocial stressors.84 These recent findings in elite netball players83 indicate that the basal level of arousal may provide a risk factor for sleep disruption during competition. It is, therefore, possible to build ‘at-risk’ profiles and target subsequent sleep management at the individual athlete level.
In summary, current evidence indicates that elite athletes are particularly susceptible to sleep complaints.85 Nevertheless, the research evidence indicates that sleep inadequacy in elite sport can be predictable, enabling targeted sleep education and sleep management interventions.
Intensified training, over-reaching and overtraining
Elite athletes follow rigorous, carefully planned training regimens designed to optimise peak performance during the most important competitions of the season. Periods of intensified training are inherent to athletes’ training programmes and are intended to impose training stress to stimulate the physiological adaptations necessary to improve performance. However, when the balance between training stress and adequate recovery is disrupted, an abnormal training response may occur, and functional over-reaching and overtraining can develop.86 Overtraining is defined as a long-term decrement in performance capacity with or without related physiological and psychological signs and symptoms of maladaptation in which restoration of performance capacity may take several weeks or months.86
Over-reaching, overtraining and sleep disturbances
Sleep disturbances are frequently reported as one of the many symptoms of over-reaching/overtraining.86 87 This finding has been demonstrated through athlete self-reports of difficulties initiating sleep, restlessness and heavy legs during sleep88–91; but also via altered nocturnal wrist actigraphy in athletes with clear signs of over-reaching (ie, high perceived fatigue and decreased performance) during intensified training.63 92 93 Nevertheless, the reported magnitude of these sleep alterations with over-reaching/overtraining is quite modest in terms of both the reduction in sleep efficiency (<5%) and sleep duration (<30 min), particularly when compared with that observed in sleep disorder patients94 or even in athletes in response to jet lag95 or hypoxia.96 Of note, a case study reported larger sleep deficiency (<6 hours per night compared with 8–10 hours per night following full recovery) in a talented female sprint cyclist who developed signs of overtraining (ie, persistent fatigue and underperforming over months). This case indicates that more severe sleep impairments could be associated with overtraining syndrome, but more research is needed to confirm this hypothesis.89
Is sleep disturbance a symptom of over-reaching/overtraining or an aetiological mechanism?
It remains unclear whether sleep disturbance is an aetiological mechanism of over-reaching or merely a symptom. While the psychophysiological mechanism(s) underlying sleep disturbance during periods of over-reaching/overtraining remain unclear, several potential factors may contribute to the reported sleep disturbances and performance decline. During overload training periods, several aspects of innate and adaptive immunity are depressed (eg, marked reductions in neutrophil function, lymphocyte proliferation and circulating T cells).97 98 Over-reached athletes with objective signs of moderate sleep disturbance demonstrate a higher incidence of upper respiratory tract infections than non-over-reached athletes.63 Depressed immune response, often leading to infection, has been shown to impair sleep.99 However, given that lack of sleep itself also has a direct impact on immune function,100 further studies are needed to determine whether an altered immune function that may occur with over-reaching/overtraining leads to sleep disturbance. An additional confounder in determining this link is that over-reaching/overtraining can change mood and increase stress and anxiety, all of which can adversely impact sleep.101–104 These reciprocal relationships make it difficult to determine the direction of the relationships between sleep, immune function, stress, anxiety and mood, and how these may lead to or contribute to the development of over-reaching/overtraining.
Recently, Schaal et al reported that the daily use of whole-body cryostimulation during intensified training improved the quality of the swimmers’ recovery by preserving sleep quantity (measured by actigraphy) and preventing the development of over-reaching.93 Since cold exposure after intense exercise can induce a prompt postexercise parasympathetic reactivation,93 105 which may promote relaxation and the onset of sleepiness,106 the development of over-reaching and its related sleep disturbances may potentially be mediated by alterations of the autonomic nervous system balance. Further investigations are required to test this hypothesis.
The impact of training and competition schedules on sleep
Lastly, the increase in training load at the origin of over-reaching/overtraining development is often accompanied by changes in training and competition scheduling, which may influence the amount of time an athlete can spend in bed. The impact of training and competition schedules on athletes’ sleep is well established (see section ‘sleep inadequacy and the athlete’).55 75 107 108 Early morning training and competition reduce athletes’ sleep duration and increase pretraining fatigue levels.55 75 Similarly, intense training sessions and matches performed in the evening (18:00–21:00 hours) are commonly associated with later sleep onset time, shorter time in bed and less total sleep obtained (figure 1).69 109 As such, when designing training programmes, practitioners need to consider the upcoming competitive schedules and should also be aware of the implications of training timing on sleep duration and fatigue levels.55 Poorly designed training programmes may restrict the opportunity athletes have for sleep, which may limit recovery between training sessions and increase the risk of over-reaching/overtraining. Potential solutions (eg, naps) are provided in the sleep toolbox section at the end of this consensus.
Strategies to improve sleep
Circadian rhythms, jet lag and sleep
Humans possess a body clock situated in the suprachiasmatic nuclei in the hypothalamus. In the absence of external time cues (such as light/dark cycle), this master clock tends to run for about 24.3 hours.110 The clock becomes synchronised and in-tune with the environment and solar day (~24 hours ‘circadian rhythm’) by the coupling of cyclic changes in the external environment (‘zeitgebers’—time cues) with rhythmic signals from melatonin (originating from the pineal gland, an ‘internal zeitgeber’).111 112 The body clock is connected to networks of peripheral clocks, and has roles in increasing alertness, mental and physical activity in the daytime, and preparing the body in the evening for sleep. This ‘circadian rhythm’ enables consolidated sleep to take place at night and prepares the body towards the end of sleep for wakening to face the new day. The body clock does this via the rhythmic changes it produces in the autonomic nervous system, bloodborne hormones, core body temperature and the sleep-wake cycle.110
Chronotype is a genetically determined predisposition that modifies each individual’s preference to be most active in the morning (‘morningness’), the middle of the day (neither type) or in the evening (‘eveningness’).57 113 In relation to chronotype distribution, as defined by the ‘morningness–eveningness’ preference continuum,114 a skew towards ‘morningness’ has been reported in elite athletes.56 57 115
The ease of falling asleep, the ability to maintain sleep and the likelihood of waking up are associated with the rhythm of core body temperature. Getting to sleep and maintaining sleep are easiest when core body temperature is either falling or low (at and after the onset of melatonin secretion, ~21:00 hours), and most difficult when it is rising or high (and melatonin secretion has stopped).116 Further, when core body temperature is rising, spontaneous waking is most likely to occur. The timing of the body clock is stable and transient changes to a regular routine—for instance, waking in the middle of the night to feed a baby, or turn off a car alarm, or taking a nap in the daytime—result in no change in the phase of the body clock.117 In contrast, the normal synchrony between the body clock and the environment is transiently lost after rapid transmeridian travel, the associated negative feelings and symptoms of which are referred to as ‘jet lag’.118
Daily variations in components of sports performance before travel
Variations in human physiology that manifest over a 24-hour solar day (circadian) have been extensively reported.119 Before considering the consequences of jet lag for sporting performance, it is essential to note that there are specific times of day when rhythms associate with peak sporting performance. Tasks that require fine motor coordination (such as standing on a wobble board) or are related to learning game tactics may be achieved more easily in the morning (08:00–09:00 hours). This is probably because basal arousal levels are lower than the diurnal peak and closer to the optimum level for performance.117 119 Tasks requiring complex hand-eye-coordination skill, such as the accuracy of tennis or badminton serves, peak around 13:00–15:00 hours. They have two components to the rhythm, a circadian influence parallel to core body temperature, but also a time-awake effect where performance decreases with time awake and mental fatigue (synchronous with the sleep-wake cycle). Limited evidence indicates that self-paced endurance performance (total work done in 1 hour) is comparable in the morning (08:30 hours) and early evening (17:30 hours) in temperate conditions.120 Lastly, circadian rhythms in gross muscular tasks such as back and leg strength (daily variation of 3%–10%),121–123 repeated sprint performance and time-trial performance (daily variation of 3%–6%),124 125 exhibit maximum and minimum values in parallel to those of core body temperature (17:00–20:00 and ~05:00 hours, respectively).122 The most reported explanation as to why gross muscular performance is better in the evening than the morning centres around the causal relationship between core body temperature and muscle temperature and performance, from the observation of both profiles being in phase. Research in this area has shown this relationship is not simple and temperature does not fully explain the daily rhythm in strength.126–130
Jet lag after time zone transition
After a westward flight, for example, where local time is 8 hours behind ‘body time’, the individual feels tired at ~16:00 hours (new local time) and wakes up at a now inappropriate time in the local time zone (24:00 hours), when the local inhabitants are going to bed. After an eastward flight, destination time is ahead of an unadjusted ‘body time’. In this case the individual does not feel tired when it is time to go to bed (local midnight) because the body clock will indicate only 16:00 hours, but they feel tired (24:00 hours, body time) when the local inhabitants are waking for the next day (08:00 hours, local time). In these circumstances where there is a mismatch between the endogenous and exogenous rhythms, the symptoms of ‘jet lag’ arise. As adjustment of the body clock to the new time zone occurs, nocturnal sleep improves and symptoms of daytime fatigue, poorer motivation and poorer mental performance subside.116
Jet lag and sporting performance
Empirical evidence that jet lag affects athletic performance directly is sparse. Three main lines of evidence underpin the rationale for the adjustment strategies recommended for sports persons crossing multiple time zones (see online supplemental table 1 for bright light avoidance and exposure).116–118 131 132 First, the evidence that the body clock influences sporting performance, hence an endogenous component34; second, the observed negative effects while adjusting the body clock to the new time zone; including, nocturnal sleep loss, daytime fatigue, poorer motivation and poorer mental performance, which in turn can affect training and physical performance; and third, the findings of meta-analyses of win-loss records of basketball, hockey and American football teams travelling across time zones before matches.133 134 Although limited to the level of association, these meta-analyses predictably show advantages, hence a better chance of winning, if the team plays at a time coinciding with daytime in the time zone left (closest to peak core body temperature). For example, after eastward flights, local afternoon or evening matches are preferable to morning; whereas, after westward flights, morning or early afternoon matches are preferable to late afternoons or evenings: we know that teams travelling westward for evening matches have a disadvantage.133 134 When the advice presented in online supplemental table 1 is delivered through a formal educational programme to athletes it works well in regard to preparation prior to, during and after arrival at the destination to help alleviate the symptoms of jet lag.118 132 135
Supplemental material
Travel fatigue and jet lag: guidelines and research recommendations
Travel fatigue associated with high frequency travel and jet lag associated with time zone displacement are downsides of elite competition. The symptoms of travel fatigue and jet lag may present themselves in a similar manner, but different aspects of travel cause them. Travel fatigue associated with the disruption and demands of travel, such as getting to the plane and poor prior sleep, can become an enduring problem for elite competitors in sports such as basketball (National Basketball Association) and hockey (National Hockey League), who endure high frequency domestic flights for matches each season.136 Jet lag is associated with the resynchronisation of the body clock to the new environment and resolves at a rate of about 1 day per time zone crossed.118 132 Much effort has gone into assessing the responsible factors for jet lag135 137 and the time course of recovery while staying in the new time zone. The severity of symptoms and adjustment of an individual depend on the direction of the flight and interindividual variation.135 There have been several investigations on chronobiotics, agents that can cause phase adjustment of the body clock (eg, light (250–10 000 lux), exercise or melatonin), employed with various levels of success.138 Either preflight,139 after arrival using melatonin,140 141 bright light,142 143 or exercise144; or, a combination of prearrival and postarrival melatonin.140 141 145 Readers are directed elsewhere for a review of interventions to minimise jet lag after westward and eastward flights.145 146 There is a pressing need for real-world and robust studies to support the proposed strategies for adjusting the body clock after time zone transitions, for example, randomised controlled trials are required to assess the efficacy of melatonin and the advice on the use of bright light (online supplemental table 1).
Nutritional strategies to enhance sleep
The role that nutrition may play in enhancing the quality and/or quantity of sleep has become of interest to many people working not only in sport, but in other areas of health and disease. The notion that a nutritional intervention may improve athlete sleep and potentially enhance muscle recovery and repair, hormonal status, overnight protein synthesis or muscle glycogen stores has stoked commercial interest in nutritional supplements for sleep. The rationale behind the potential influence of nutrition on sleep relates to a number of neurotransmitters being associated with the sleep-wake cycle (eg, serotonin), that have potential to be influenced by nutrition.147 However, unfortunately the research in this area is in its infancy and definitive conclusions are currently difficult to formulate. The limited research in the area provides some evidence that dietary intake prior to sleep, specifically carbohydrate intake and the timing of ingestion, has the potential to influence sleep.148 149 Afaghi et al 148 compared low and high Glycaemic Index (GI) carbohydrate-rich meals eaten 4 hours before bedtime with a high GI meal eaten 1 hour prior to bedtime, finding that the earlier consumed high GI meal reduced SOL (the time taken to fall asleep). Further information on the influence of dietary macronutrients on sleep is found in recent reviews.42 150
Caffeine and sleep
The impact of caffeine on sleep has been extensively investigated. Caffeine is found in various foods and beverages including coffee, chocolate and tea, with coffee being the primary source of dietary caffeine, although preworkout and energy drinks are becoming increasingly popular sources.151 Caffeine antagonises adenosine receptors in the brain: these receptors are associated with arousal regulation and stimulation of these receptors promotes wakefulness. Normal dietary caffeine consumption is sufficient to antagonise up to 50% of the inhibitory A1 and facilitatory A2A receptors.152 A recent systematic review of 58 publications highlighted the negative effects of caffeine on sleep.151 Results of this analysis indicate that caffeine typically increases SOL and decreases sleep duration, sleep efficiency and perceived sleep quality. When examining the influence of caffeine on sleep architecture, slow wave sleep and slow wave activity were reduced, while stage one sleep, wakefulness and arousal were increased. The magnitude of these effects of caffeine was modulated to some extent by age, gender, body mass and genetic predisposition; nevertheless, the typical consumption of 1–2 double espressos up to 16 hours before sleep induced consistent negative effects on sleep.151
The above-mentioned review151 presented results mainly from studies involving healthy, non-athletic males; relatively little is known about the effects of caffeine on sleep in athletes. Caffeine is frequently used by athletes to enhance performance and as a fatigue countermeasure prior to training (doses of 3–6 mg/kg body mass appear to be effective).153 One study has investigated the effects of caffeine consumption on sleep in elite rugby union players and found that caffeine consumption before an evening game was common and resulted in an increase in postgame salivary caffeine levels.154 Similar to the data from the previously mentioned systematic review,151 salivary caffeine concentrations were associated with increased SOL, a decrease in sleep efficiency and tended to be related to a decrease in sleep duration. This may partially explain some of the difficulties with sleep post game that many elite team sport athletes report.155 Further research is required to be able to provide guidance around optimising timing and doses of caffeine in relation to effects on sleep architecture. It is likely this will be required on an in individual basis, with present evidence suggesting a judicious approach to the use of caffeine in athletes.
In summary, there are very few high-quality, randomised controlled trials on nutrition and athlete sleep. Limitations include the type, timing and dosages of macronutrients and other nutritional interventions given (eg, herbal products), as well as the variable means by which sleep quantity and quality are measured in studies (table 1).42 Athletes should be wary of unsubstantiated claims regarding sleep-boosting supplements and aware of the risks of a doping violation for supplements not tested by an established quality assurance programme.153
A ‘sleep toolbox’ for practitioners: evidence-based practice
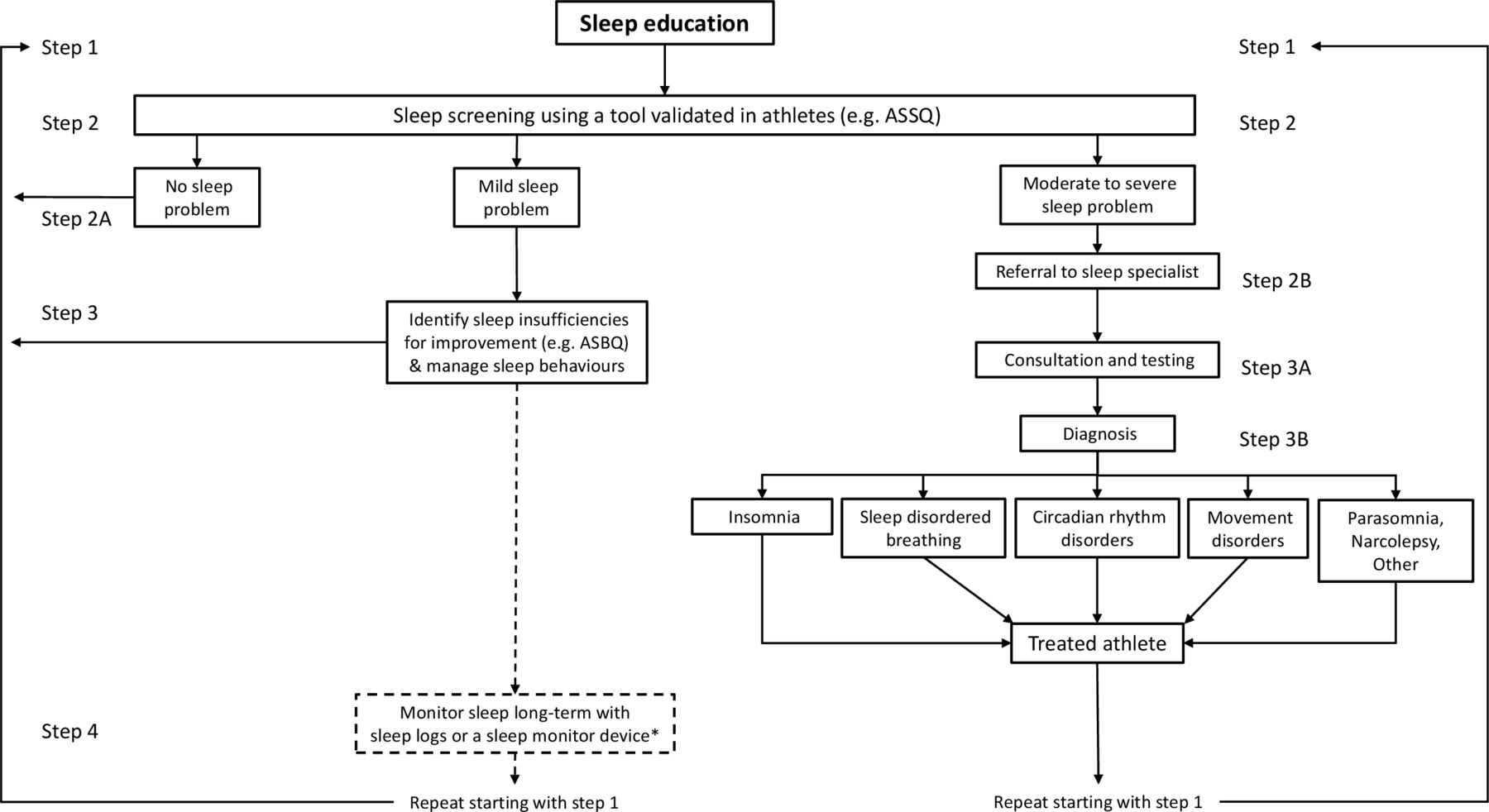
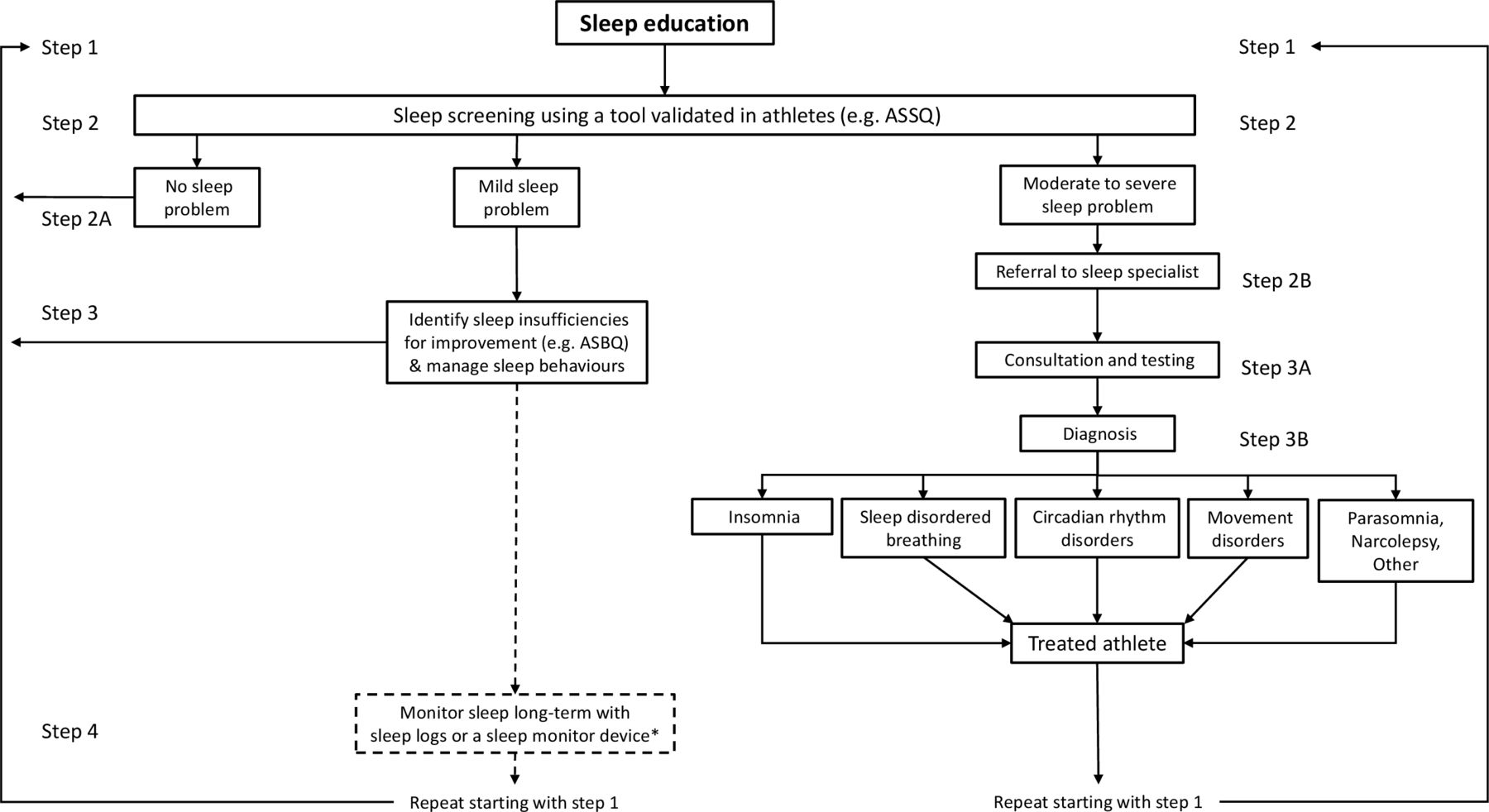
Sleep management in athletes can be challenging for practitioners for many different reasons; not least, the lack of knowledge relating to sleep-wake cycles and the prevalence of common sleep myths.156 157 These issues are amplified when sleep disturbance and consequent daytime dysfunction are more common among athletes compared with healthy non-athletes.56 Practitioners need to be equipped with tools to overcome these challenges to optimise sleep in athletes for better athlete health, well-being and success (box 2). Figure 2 describes a pathway for practitioners to follow in order to manage and optimise sleep for athletes.
{kind=link}
{kind=link}
A flow diagram for practitioners to help optimise and manage sleep for athletes. Step 1 – Sleep education should occur multiple times throughout the season and can be in the form of presentations, informal sessions, and information sheets. Step 2 – Use questionnaire-based sleep screening initially during pre- and post-season evaluations and on an as needed basis during the season. The Athlete Sleep Screening Questionnaire (ASSQ) is a validated clinical tool to flag athletes who need further help from a sleep specialist. Step 2A – The questionnaire you use should identify athletes with sleep problems using validated cut-points. For example, the ASSQ categorises athletes into no, mild, moderate, and severe clinical sleep problem. Athletes with no sleep problem can go back to Step 1 (Sleep Education) to determine what areas to focus on. Step 2B – If the athlete has a moderate to severe sleep problem, referral to a sleep professional is recommended right away due to the potential duration of treatment and potential wait times. Step 3 – Identify sleep improvement and optimisation strategies based on the athlete’s sleep insufficiencies and/or poor sleep habits. The Athlete Sleep Behaviour Questionnaire (ASBQ) identifies maladaptive sleep behaviours and has been validated in an athlete sample. For athletes who have moderate to severe sleep problems, caution is warranted as identifying sleep insufficiencies can make the problem worse (eg, recommending more sleep when the athlete has insomnia). Proper judgement is required. Step 3A – Ideally the moderate to severe clinical sleep problem athlete should have a sleep consultation with a sleep medicine physician specialising in working with athletes. Step 3B – Once a diagnosis has been established, different treatments are available and can help the athlete optimise sleep. Step 4 – Tracking sleep with sleep logs or a sleep monitor in those with a mild sleep problem (broken arrows) may not be necessary but can be used for feedback to the athlete to help modify behaviour change. The practitioner must be able to properly interpret the data and understand the limitations of the sleep logs or the sleep monitor which should be validated against polysomnography. *See table 1 for monitoring tools.
Summary of the sleep toolbox for practitioners
Provide sleep education for athletes—Sleep education sessions for athletes have been shown to improve sleep. Sleep education could cover topics related to sleep quantity, quality, timing, and sleep monitors. Education should focus on how sleep relates to performance in their sport to create buy-in for further sleep interventions (see tool #1).
Screen athletes for sleep problems—All the best sleep advice could undermine an athlete’s sleep if they have an underlying sleep problem (eg, bank sleep for an athlete with insomnia). Start with a questionnaire-based tool validated in athletes as athletes can be quickly identified and seek help from a sleep specialist in a timely manner (see tool #2, figure 2).
Encourage naps—With late or early training times, travel and balancing life outside of sport, athletes may not have enough sleep opportunity at night so supplementing with a nap is key. Even short naps of <30 min can enhance mood, alertness and cognitive performance in those who get sufficient night-time sleep. Time naps from 13:00 to 16:00 hours when there is a dip in alertness (the ‘postlunch dip’) and consider a ‘coffee-nap’ (see tool #3).
Bank sleep—Sleep extension has potential to improve athlete performance and mood and reduce stress levels. This tool may be a good way to ease anxiety leading into an important competition. By getting more sleep prior to an important competition, athletes can have confidence knowing that a poor night’s sleep the night before competition should not affect their performance. The period of banking sleep does not have to be months, even just 1 week has been shown to improve performance (see tool #4).
Tool #1: provide sleep education for athletes
Less than half of a sample of 86 coaches and sports science support staff had promoted sleep hygiene, with one of the main barriers being lack of sleep knowledge.157 It is important for practitioners to seek out and access accurate sleep information specific to athletes in the form of seminars, manuscripts and other evidence-based modes when preparing athlete sleep education. Promoting sleep information specific to the athlete’s sport such as sleep need, adjusting to training times and emphasis on the impact of sleep on performance is key to create buy-in and behavioural change. Encouragingly, sleep education presentations ranging in duration from 30 to 60 min have been shown to increase sleep duration by an average of 20–90 min.158–160 However, the improvements in sleep were not maintained at follow-up 1 month later.159 More frequent sleep education sessions throughout the season, along with frequent check-ins with the athlete about their sleep, may be required to maintain the benefit (box 3).
Athlete sleep education—five tips to educate athletes on the importance of sleep
Night-time sleep quantity—a range of 7–9 hours is appropriate for healthy adults and 8–10 hours for teenagers166; however, experts speculate that athletes need more to recover from the physical and psychological demands of the sport.167 The amount of sleep athletes get may need to increase depending on the training load of the sport and the age of the athlete.
Daytime sleep quantity (naps)—when schedule changes are not possible, napping can supplement insufficient night-time sleep. But a nap can also be beneficial for those just wanting a boost in alertness. See tool #3 for more information.
Good sleep hygiene—sleep hygiene includes the habits necessary to have good sleep quality and daytime alertness. Research has shown that having good sleep hygiene can improve sleep quality.168 Common sleep hygiene habits include avoiding stimulants (eg, caffeine), alcohol, and heavy meals too close to bedtime, adequate exposure to natural light in the morning, not lying in bed awake for long periods of time, having a relaxing bedtime routine and having a sleep environment conducive to sleep which is cool, dark and quiet.
Sleep and train in-line with chronotype—adolescents are more likely to be evening chronotypes (‘night owls’) due to later melatonin release. The research shows athletes are more likely to be morning chronotypes (‘larks’) but those who are night owls struggle more with their sleep.56 When possible, avoiding training times early in the morning and late at night allows ample opportunity for sleep and recovery.
Caution when using sleep monitors—see table 1 for strengths and weaknesses of sleep monitors. Caution must be taken to understand the impact of the feedback from the device to the individual athlete. Some athletes may become preoccupied with their sleep monitor data, which may increase anxiety around sleep and result in worse sleep.169 Another important consideration is privacy, as sleep monitoring device apps may contain personal and sensitive information; it is important to consider who has access to this information.170 Practitioners must weigh both the pros and cons of using sleep monitoring technology for the athletes they are working with.
Tool #2: sleep screen athletes and refer for help when needed
Sleep screening has become an integral part of managing athlete health, allowing practitioners to identify sleep problems and refer athletes to a sleep specialist for clinical diagnosis, when necessary (figure 2 and table 1). This is an important step because any sleep-focused strategies will likely be ineffective in the presence of untreated sleep disorders.
Tool #3: encourage nap opportunities
A nap is considered daytime sleep and purported benefits include improvements in alertness, concentration, motor performance and mood.161 For those athletes who may have rigid early morning training times and cannot get enough night-time sleep, a nap during the day can supplement limited night-time sleep.162 Naps have even been shown to enhance mood, alertness and cognitive performance for those who typically get the amount of sleep they need on a nightly basis,161 so taking a nap may still be beneficial if the athlete is getting a sufficient amount of night-time sleep. When athletes have a shorter window to nap, durations of <30 min are recommended so they do not have sleep inertia (ie, grogginess) from getting into the deeper stages of sleep. Athletes should consider the benefits of taking a 15–20 min ‘coffee-nap’ in the mid-afternoon. Caffeine consumed in doses of 150–200 mg just prior to a mid-afternoon nap (hence ‘coffee-nap’) has been shown to be an effective countermeasure to mid-afternoon sleepiness (the ‘postlunch dip’).163 164 On wakening, exposure to bright light and face washing are also recommended additions to the nap routine.164 Athletes can set an alarm about 10 min longer than the duration of the nap in order to factor in the amount of time to fall asleep. Relaxation and breathing techniques can help the athlete to fall asleep. Athletes should avoid naps altogether if they have problems falling asleep at night.
Tool #4: banking sleep and sleep extension
Getting more sleep (‘banking sleep’) before a period of anticipated sleep loss may benefit performance.45 165 The sleep extension approach involves scheduling a longer sleep opportunity than normal, usually a window of 9–10 hours where there is a protected time for sleep. One study in collegiate basketball players showed that sleep extension, comprising a 10-hour time in bed each night over a time frame of 5–7 weeks, improved reaction time, sprint times, mood and free-throw shooting accuracy.38 Research is required to determine whether the purported benefits of sleep extension can be realised with shorter additional nightly sleep and/or over a shorter time frame, particularly in athletes identified with sleep insufficiency.
Conclusion
The available evidence indicates that elite athletes are particularly susceptible to sleep inadequacies that are characterised by habitual short sleep duration (<7 hours each night) and poor sleep quality (eg, fragmented sleep). These observations have sparked a recent explosion of research targeted towards understanding the relationship of sleep to recovery, training and performance in elite athletes. Unfortunately, the quality of much of the available research evidence is poor, largely due to inconsistent, unreliable and invalid research methods. A key recommendation from this narrative review and expert consensus is for researchers to collaborate and employ better, more consistent research methods to improve the quality of the evidence and responsibly inform practitioners. Based on the best available evidence, a sleep toolbox is provided (figure 2 and Box 2), offering standardised interventions and screening tools to address the problem of sleep health in elite athletes.
What is already known?
Sleep disruption affects recovery, training and performance in elite athletes and elite athletes do not get enough sleep. The primary risk factors for chronic sleep disturbance include high training loads, travel and stress associated with competition. Other risk factors include individual versus team sports, female vs male athletes and the type of sport.
While there is a growing interest in understanding the relationship of sleep to recovery, training and performance, to date, the quality of the evidence is poor largely due to inconsistent, unreliable and invalid research methods. Researchers should collaborate and employ more consistent research methods to improve the quality of the evidence.
What are the new findings?
Our five recommendations (box 3) and the sleep toolbox (box 2) are based on best evidence to provide clinicians and practitioners with standardised interventions and tools to address the problem of sleep health in elite athletes. The toolbox also provides researchers with valid, reliable and standardised methods for future research.
Future research should focus on the role and impact of sleep extension and napping on sleep health and performance in elite athletes. In addition, with more accurate, valid and reliable research methods, future research should explore the relationship of sleep to immune function and the effect of nutritional manipulation on sleep.
Supplemental material
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ProfNeilWalsh, @shonahalson, @CBTmin, @lukegup86, @HughFullagar, @aaronjcoutts, @YLMSportScience, @sleep4sport
Contributors All authors have made substantial contributions to the drafting and revision of this consensus statementand have seen and given final approval for the submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AMB and CH have received grant funding from Own the Podium and Mitacs. MAG has received grant funding from Kemin Foods, Nexalin Technology and Jazz Pharmaceuticals; he has performed consulting activities for Fitbit, Natrol, Casper Sleep, Curaegis Technologies, Smartypants, Thrive Global, Pharmavite and Merck.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.