Article Text

Abstract
Objective To compare the effectiveness of progressive tendon-loading exercises (PTLE) with eccentric exercise therapy (EET) in patients with patellar tendinopathy (PT).
Methods In a stratified, investigator-blinded, block-randomised trial, 76 patients with clinically diagnosed and ultrasound-confirmed PT were randomly assigned in a 1:1 ratio to receive either PTLE or EET. The primary end point was clinical outcome after 24 weeks following an intention-to-treat analysis, as assessed with the validated Victorian Institute of Sports Assessment for patellar tendons (VISA-P) questionnaire measuring pain, function and ability to play sports. Secondary outcomes included the return to sports rate, subjective patient satisfaction and exercise adherence.
Results Patients were randomised between January 2017 and July 2019. The intention-to-treat population (mean age, 24 years, SD 4); 58 (76%) male) consisted of patients with mostly chronic PT (median symptom duration 2 years). Most patients (82%) underwent prior treatment for PT but failed to recover fully. 38 patients were randomised to the PTLE group and 38 patients to the EET group. The improvement in VISA-P score was significantly better for PTLE than for EET after 24 weeks (28 vs 18 points, adjusted mean between-group difference, 9 (95% CI 1 to 16); p=0.023). There was a trend towards a higher return to sports rate in the PTLE group (43% vs 27%, p=0.13). No significant between-group difference was found for subjective patient satisfaction (81% vs 83%, p=0.54) and exercise adherence between the PTLE group and EET group after 24 weeks (40% vs 49%, p=0.33).
Conclusions In patients with PT, PTLE resulted in a significantly better clinical outcome after 24 weeks than EET. PTLE are superior to EET and are therefore recommended as initial conservative treatment for PT.
- overuse injury
- exercise rehabilitation
- randomised controlled trial
- sports rehabilitation programs
- tendinopathy
Data availability statement
Data are available on reasonable request. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- overuse injury
- exercise rehabilitation
- randomised controlled trial
- sports rehabilitation programs
- tendinopathy
Introduction
Patellar tendinopathy (PT) is a common chronic tendon injury that is characterised by load-related pain in the patellar tendon.1 As many as 45% of elite athletes in jumping sports like basketball and volleyball suffer from PT.2 This often results in prolonged sport absence, which hampers an individual’s athletic performance and the health-related benefits of physical activity.3 It also has been shown that 58% of the patients with PT encounter problems with participation in physically demanding work.4
Despite the fact that many risk factors in the aetiology and pathogenesis of PT have been suggested, a direct cause–effect relationship is currently unknown.5 The nomenclature ‘tendinitis’ has been replaced by ‘tendinopathy’,1 since histopathological studies confirm structural degenerative changes of the tendon tissue as the key feature, with minimal presence of inflammatory cells.6 7 Anti-inflammatory treatment options are, therefore, discouraged and these have proven ineffective for tendinopathy.8
Eccentric exercise therapy (EET) has strong evidence of effectiveness for PT and is also supported in guidelines by the National Institute for Health and Care Excellence (NICE), London, UK.9 10 However, EET is pain-provoking and the therapeutic effects on pain and functional outcome are debated when applied during the competitive season.11 A recent review proposed an alternative exercise therapy for PT consisting of progressive tendon-loading exercises (PTLE) within the limits of acceptable pain.3 To date, it is unknown how the effectiveness of PTLE compares to EET.
The aim of our stratified, single-blinded, block-randomised controlled trial was to compare PTLE and EET based on clinical outcome after 24 weeks in patients with PT.
Methods
Trial design
The JUMPER study was a stratified, investigator-blinded, block-randomised controlled trial that included recreational, competitive and professional athletes with PT. The trial was conducted at a university medical centre in The Netherlands. The study protocol was registered on ClinicalTrials.gov (ID: NCT02938143) prior to recruitment. All patients provided written informed consent.
Patient involvement
Patients and public were not involved in the trial design and conduct of the study or the choice of outcome measures. Several national sports federations announced the study with additional advertisements in local sport organisations. Healthcare providers were alerted to the study with conference announcements, information on websites, newsletters and emails.
Patients
Inclusion criteria were: age 18–35 years old; history of knee pain localised in the region of the patellar tendon in association with training and competition; performing sports at least three times a week; tenderness on palpation of the corresponding area on the proximal patellar tendon; structural tendon changes on grey scale ultrasound and/or increased tendon vascularity on power Doppler; and Victorian Institute of Sports Assessment for Patellar Tendons (VISA-P) score <80 out of 100 points.12 13
Exclusion criteria were: acute knee or patellar tendon injuries, prior knee surgery without full rehabilitation, known presence of inflammatory joint diseases or familial hypercholesterolaemia, daily use of drugs with a putative effect on the patellar tendon in the preceding 12 months (eg, fluoroquinolones), local injection therapy with corticosteroids in the preceding 12 months, previous patellar tendon rupture, daily exercise therapy with a minimum duration of 4 weeks in total in the preceding 12 months, inability to perform an exercise programme, participation in other concomitant treatment programmes, signs or symptoms of other coexisting knee pathology on physical examination or ultrasound/MRI and contraindications for MRI.
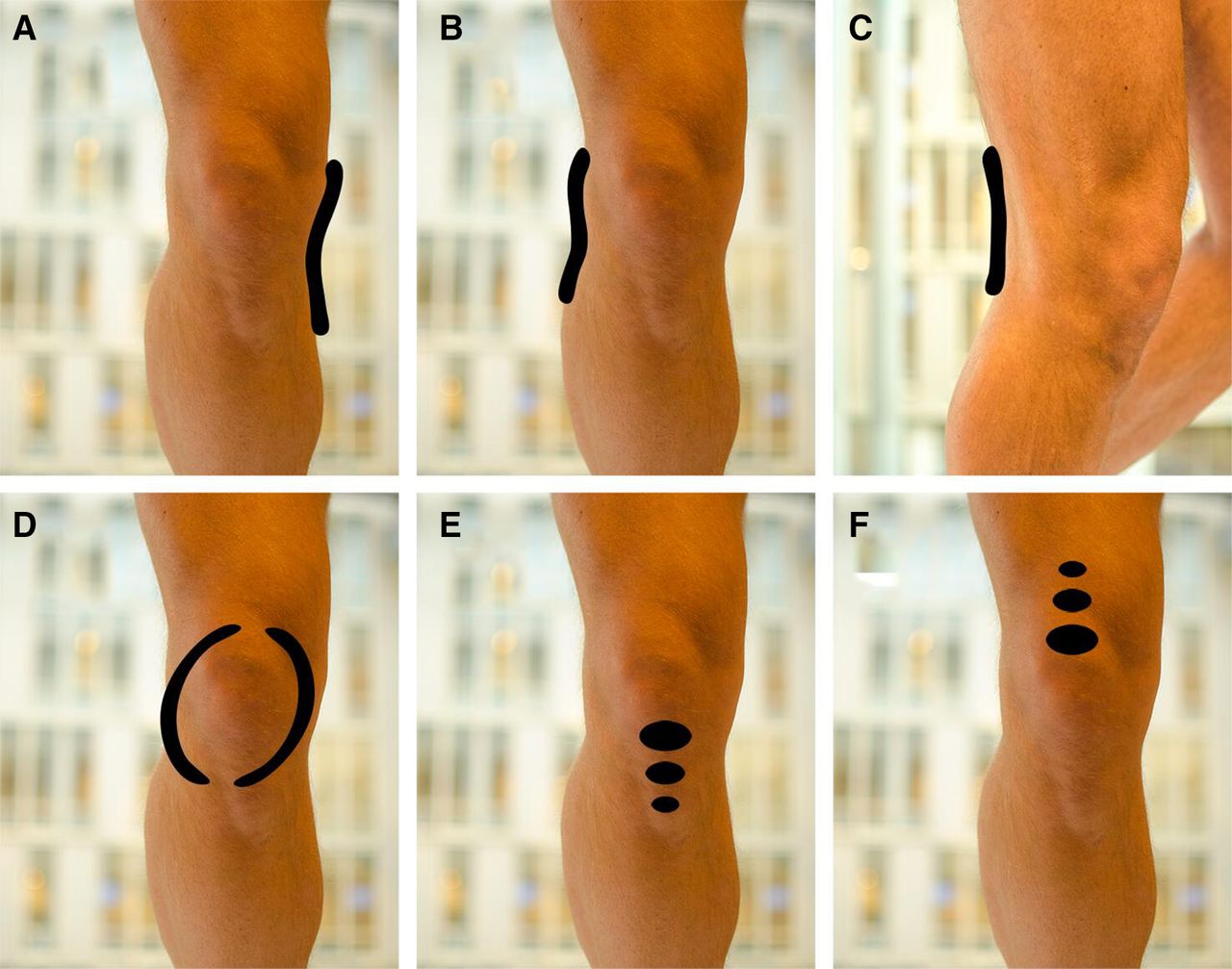
Applicant eligibility was assessed with an initial online screening, including the VISA-P questionnaire and a self-reported pain map to assess the location of pain (figure 1).14 The screening criteria that needed to be fulfilled were VISA-P score <80 points and the reporting of pain exclusively at the inferior pole of the patella or anywhere along the course of the patellar tendon (figure 1E) in association with physical load. The final eligibility assessment in our hospital to confirm eligibility included first, history taking, completing the VISA-P questionnaire and physical examination performed by one sports physician (R-JdV) with 10 years experience. Activity level was measured using the Cincinnati Sports Activity Scale (CSAS).15 The clinical examination was regarded positive if tenderness at the inferior patellar pole or patellar tendon could be reproduced on palpation and a single-leg squat. Provocation tests according to the patellofemoral pain consensus statement were performed to exclude patellofemoral pain.16 Second, eligibility was confirmed by using grey scale ultrasound and power Doppler to increase the likelihood of the clinical diagnosis, performed by a radiologist-in-training with 5 years experience (SJB) under supervision of a senior musculoskeletal radiologist with 16 years experience (EHGO). The ultrasound examination was regarded positive if there was presence of structural and/or hypoechoic changes and/or tendon thickening (anterior–posterior diameter >6 mm) and/or the presence of intratendinous power Doppler flow.17

Knee pain map for pain localisation. For the initial eligibility assessment, patients were asked to select one picture describing the location of pain most correctly; either (A) Pain on the medial side of the knee, (B) Pain on the lateral side of the knee, (C) Pain on the backside of the knee, (D) Pain behind and around the patella, (E) Pain directly under the patella or along the course of the patellar tendon or (F) Pain directly above the patella.
Randomisation and blinding
Centralised computer-based randomisation was performed in a 1:1 ratio to PTLE (interventional treatment) or EET (control treatment), using computer-generated block randomisation with a variable block size ranging from 4 to 10. Allocation concealment was ensured by keeping the randomisation list in the care of the sports physician (R-JdV) who was not involved in the follow-up measurements. The allocation sequence was concealed until patients were enrolled and assigned to interventions. The main investigator (SJB) was blinded for the allocated treatment during the entire period of data collection. During the study, patients were requested not to discuss their treatment exercises with the main investigator or the sports physician who instructed the exercise programme. Instead, patients were instructed to consult an independent second sports physician (JZ) if they had any questions regarding the therapy. Stratification was performed to divide the number of patients with early PT (≤6 weeks of symptom duration) from patients with longstanding PT, because it is suggested that early PT has a better prognosis.18
Interventions
Patients were randomly assigned to PTLE within the limits of acceptable pain (interventional treatment) or pain-provoking EET (control treatment) during 24 weeks (figure 2). We have provided detailed information regarding the unsupervised exercise programmes in the patient information brochures (online supplemental appendix). Patients could access our dedicated website (http://www.jumperstudie.nl/) with instructional videos that we created in collaboration with a sports physiotherapist (EV).
Supplemental material

Exercise therapy performed in the PLTE group (intervention) and EET group (control). The exercises illustrated are exemplary images. The complete exercise programme is available in online supplemental appendix. EET, eccentric exercise therapy; PTLE, progressive tendon-loading exercises.
Patients in the intervention group performed daily isometric (static), isotonic (dynamic), energy-storage (explosive) and sport-specific exercises consecutively, within the limits of acceptable pain (online supplemental appendix). Progressive load was administered based on the individual pain response (Visual Analogue Scale, VAS score ≤3 points on a scale 0–10). This PTLE programme contained four stages, where stage 1 consisted of daily isometric exercises (single-leg leg-press or leg-extension, 5 repetitions of 45 s mid-range (60° knee flexion) quadriceps isometric hold at 70% of maximum voluntary contraction). Stage 2 consisted of the isometric exercises of stage 1 on every first day, and new isotonic exercises performed on every second day. The isotonic exercises were also performed as a single-leg leg-press or leg-extension, and started with 4 sets of 15 repetitions between 10° and 60° of knee flexion and slowly progressed to 4 sets of 6 repetitions with increasing load and knee angles between almost full extension and 90° flexion. Stage 3 consisted of plyometric (energy storage) loading and running exercises (jump squats, box jumps and cutting manoeuvers) on every third day, starting with 3 sets of 10 repetitions using both legs and slowly progressed to 6 sets of 10 repetitions using one leg. Isometric and isotonic exercises were continued on every first and second day, respectively. Stage 4 consisted of sport-specific exercises, which were characteristic for the type of sport (eg, basketball, volleyball). Patients were instructed to gradually return to sport-specific training, performed every 2–3 days to allow for recovery from high tendon-loading exercises. In this stage, the isometric exercises of stage 1 were continued on days that the sport-specific exercises were not performed. Progression to each subsequent stage was defined using individualised progression criteria, based on the level of pain experienced during a pain provocation test that consisted of one single-leg squat. If the VAS-score was 3 or less and exercises of the stage were performed for at least 1 week, progression to the next stage was advised. When all the exercises in stage 4 were performed within the limits of acceptable pain (VAS score ≤3 points), return to competition was recommended. In this phase, stage 1 and 2 maintenance exercises were advised twice per week. The fastest possible time to return to sports was after 4 weeks, according to this PTLE programme. Patients who were allocated to PTLE were financially compensated for a subscription at the gym.
The control treatment was pain-provoking EET, performed twice daily for a duration of 12 weeks (first stage). The eccentric exercises were performed on a decline board with a 25° slope, as described previously.19 Stage 1 of the EET consisted of a single-leg decline squat, where the downward component (eccentric phase) was performed with the symptomatic leg and the upward component (concentric phase) mainly performed using the contralateral leg. Patients were instructed to perform the exercises with pain (VAS score ≥5 points on a scale 0–10 during the exercises).11 Additional load in a backpack was advised to increase the intensity of the exercise if no or only minimal pain was experienced when performing the exercises. Stage 2 was initiated if there was complete adherence to stage 1 exercises and when there was acceptable pain during eccentric exercises with additional weights (VAS score ≤3 points on a scale 0–10, the amount of weights was not specified). Stage 2 exercises consisted of sport-specific exercises, which were characteristic for the type of sport. Maintenance exercises consisted of stage 1 exercises twice a week. Patients in the EET group were allowed to return to sports after 4 weeks. We advised to do this if a single-leg squat could be performed within the limits of acceptable pain (VAS score ≤3 points on a scale 0–10). The decline board with a 25° slope was provided for patients allocated to EET.
Patients in both study arms were instructed to perform exercises targeting risk factors for PT in addition to the allocated tendon-specific exercises.20 21 These exercises targeting risk factors included flexibility exercises of quadriceps, hamstrings, gastrocnemius and soleus muscles, strength exercises for the hip abductor muscles and hip extensor muscles using an elastic resistance band, calf-muscle strengthening exercises and core-stability exercises. The resistance band was provided to each participant. All patients with bilateral symptoms were motivated to perform the exercises for both legs.
All patients received detailed advice and education on tendon care by a sports physician (R-JdV). This included explanation of the condition, expected management, the positive influence of exercise therapy and the positive effects of a gradual return to sports. Specific attention was given to the relation between load and pain using the pain-monitoring model.22 Modification of all athletic activity (intensity, duration, frequency and type of load) was advised for activities that result in considerable patellar tendon pain, namely either significantly reduced or even avoided for at least 4 weeks. We stimulated to perform (sports) activities within the limits of acceptable pain (VAS score ≤3 points on a scale 0–10).
Outcomes
The primary outcome was the VISA-P questionnaire.12 This validated and injury-specific questionnaire incorporates pain, function and ability to play sports. A VISA-P score of 100 indicates no pain, maximum function and unrestricted ability to play sports. The VISA-P questionnaire was self-administered without assistance at baseline, 12 weeks and 24 weeks, after a brief explanation of the questionnaire by the main investigator (SJB).
Secondary outcomes were the return to sports rate, subjective patient satisfaction and exercise adherence. Return to sports was designated as return to desired sports at pre-injury level; return to desired sports, but not at preinjury level; return to sports, but not to desired sport; and no return to sports.23 Subjective patient satisfaction was categorised into excellent, good, moderate and poor.23 Exercise adherence was reported descriptively as a percentage of the total number of prescribed training sessions completed. Additional secondary outcomes included the reasons for not performing the tendon-specific exercises and exercises targeting risk factors, number of registered training or match days, pain scores, questionnaires, functional tests and commonly used and advanced imaging methods (online supplemental appendix). All outcomes were collected by one trained examiner (SJB).
At baseline, patients with bilateral symptoms were asked to choose the most painful knee for reporting pain scores. In these cases, all clinical and radiological outcome parameters were obtained for this specific side. At each follow-up visit, patients were reminded to report outcome measures for this initially chosen side. Adverse events were monitored during the trial period. Any adverse events that occurred were discussed at the follow-up visits, and patients were requested to report any adverse events that occurred in-between the follow-up visits by telephone or email to the main investigator (SJB). The use of cointerventions during the study period was discouraged.
Statistical methods
The statistical analysis plan was uploaded on ClinicalTrials.gov before completion of the study. The sample size was calculated at 76 patients to detect a predefined minimum clinically important difference (MCID) of 13 points for the VISA-P questionnaire (power 0.80, two-sided significance level 0.05, and accounting for 10% lost to follow-up).24 Statistical analyses following an intention-to-treat approach were performed by the main investigator (SJB) under supervision of a biomedical statistician (JZ). Normality of the data was checked visually with Q-Q plots and tested statistically using the Shapiro-Wilk test. Longitudinal data were analysed using generalised estimating equations (GEE), to test for between-group differences in primary and secondary outcomes. In order to test for these between-group differences in relation to the time course of the dependent variables, we included the interaction term ‘study arm*visit’ in the GEE-model. The visit variable defined the time point at which the measurements were performed (baseline, 12 weeks, 24 weeks). Predefined adjustments were made for baseline variables age, sex, body mass index, symptom duration and CSAS. Bonferroni adjustment was applied for multiple comparisons to reduce the chance of obtaining false-positive results. We performed an additional analysis of the percentage of patients that achieved the MCID of 13 points or better for the VISA-P.24 Categorical variables were analysed using Fisher’s exact test. Return to sports was dichotomised into return to desired sports at preinjury level and no return to desired sports at preinjury level.23 The influence of symptom duration prior to intervention on the dichotomised return to sports and subjective patient satisfaction was investigated using adjusted binary logistic regression analysis. Patient satisfaction was dichotomised into satisfied (excellent/good) and dissatisfied (moderate/poor).23 Adherence to the tendon-specific exercises and exercises targeting risk factors were registered using a weekly online questionnaire. The daily adherence to the tendon-specific exercises and exercises targeting risk factors of the preceding week was registered as a percentage. Imputation of missing data was not performed, because the missingness of data was assumed to occur not at random. Namely, missingness in the outcome depends on the difference between the pain-provoking EET group and the PTLE exercises within the limits of pain, and is related to the true value of the outcome.25 Instead, post hoc sensitivity analyses were performed following three scenarios (online supplemental appendix). In the worst-case scenario for PTLE, the single missing participant from the PTLE group was assigned the worst outcome of this treatment group (VISA-P score of 43 points and 49 points at 12 weeks and 24 weeks, respectively) while all missing patients from the EET group were assigned the best outcome of their treatment group (VISA-P score of 91 points and 100 points at 12 weeks and 24 weeks, respectively). Statistical analysis was performed using IBM SPSS software V.25 (IBM). Statistical significance was defined as a p<0.05.
Results
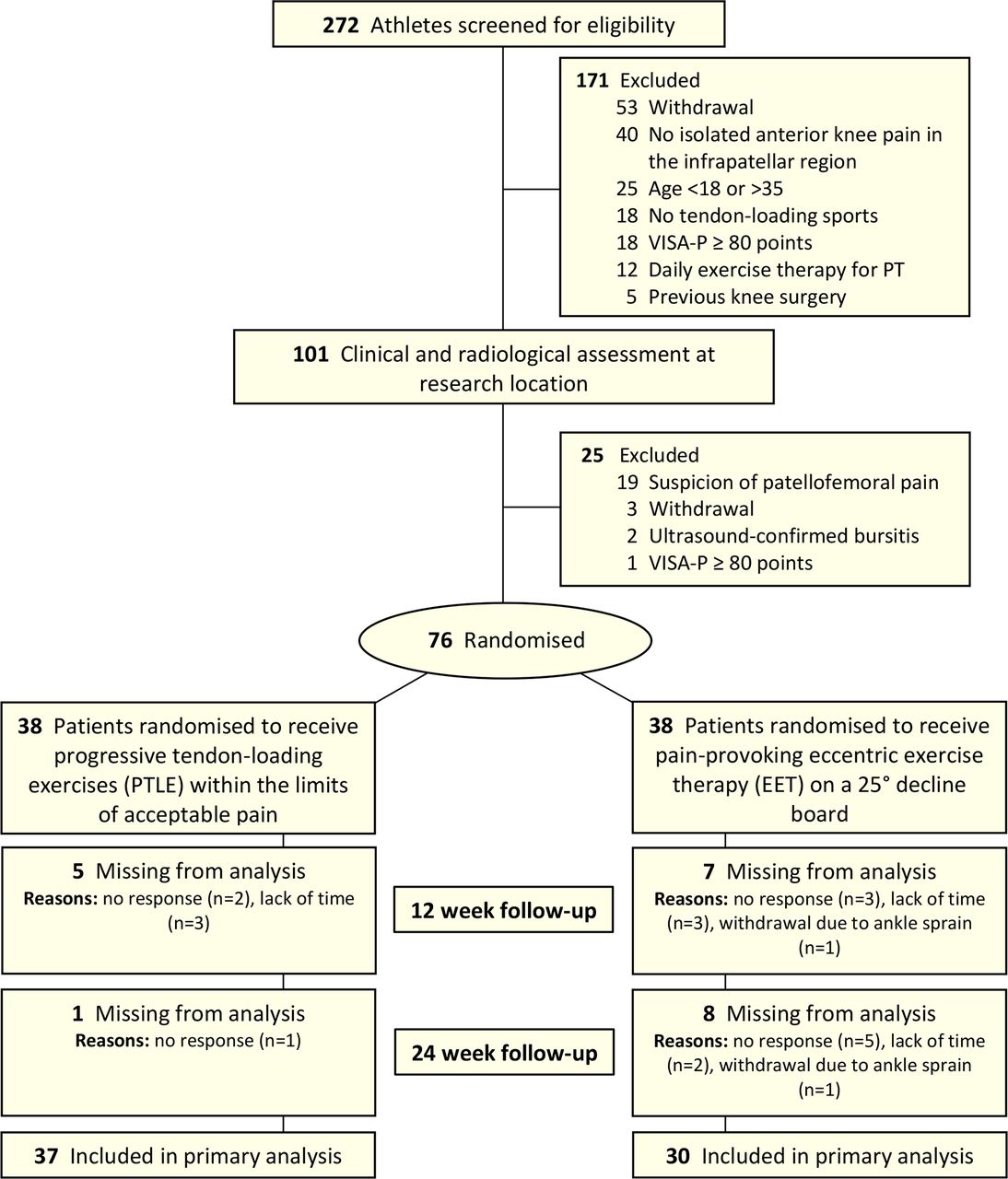
Between January 2017 and July 2019, a total of 272 applications from potentially eligible athletes with suspected PT were screened, of which 101 athletes were invited for eligibility assessment. Twenty-seven of these athletes were excluded, leaving 76 eligible patients remaining for inclusion (figure 3). The intention-to-treat population consisted of patients with a median (IQR) symptom duration of 2 years (1-4) and 42% had bilateral symptoms. Most patients (82%) underwent prior treatment for PT but failed to recover fully. There were no between-group differences in baseline characteristics, except for a longer symptom duration in the intervention group (119 vs 78 weeks) and more ultrasound-assessed erosions of the inferior patellar border (45% vs 18%) in the intervention group (table 1). An equal majority of the patients (82% in both groups) received therapy prior to the time of study commencement, of which physical therapy was part of the prior therapy in 74% of patients in both groups. Nine patients (12%) were lost to follow-up; 1 in the intervention group and 8 in the control group. Only one of the patients was included for the stratum early tendinopathy (≤6 weeks of symptom duration).

The CONSORT flow diagram. CONSORT, Consolidated Standards of Reporting Trials; PT, patellar tendinopathy; VISA-P, Victorian Institute of Sports Assessment for Patellar Tendons.
Baseline characteristics of the progressive tendon-loading exercise (PTLE) and eccentric exercise therapy (EET) groups*
Primary outcome
The estimated mean VISA-P score improved significantly from 56 (95% CI 52 to 61) at baseline to 84 (95% CI 79 to 89); p<0.001 at 24 weeks in the PTLE group and from 57 (95% CI 53 to 62) to 75 (95% CI 69 to 82); p<0.001 in the EET group (figure 4). The parameter estimate for the ‘study arm*visit’ interaction using GEE was statistically significant (p=0.023), indicating a different course over time of the VISA-P score between both study arms. The adjusted mean between-group difference in VISA-P score was not significant at 12 weeks (1 (95% CI −6 to 8); p=0.69) and significant at 24 weeks (9 (95% CI 1 to 16); p=0.023), in favour of the PTLE group. Unadjusted VISA-P scores are listed in table 2 and the individual data points of the VISA-P scores are illustrated in figure 5. After performing sensitivity analyses to assess the influence of missing data, except from the worst case scenario, the findings were consistent with those from the primary analysis and thus, leading to a similar conclusion on the treatment effect (online supplemental table S2). After 12 weeks, 16 patients (49%) in the PTLE group and 17 patients (55%) in the EET group achieved the previously reported MCID of 13 points or better for the VISA-P score.24 After 24 weeks, 32 patients (87%) in the PTLE group and 23 patients (77%) in the EET group achieved the MCID or better. The between-group difference for patients achieving the MCID or better was not statistically different at both 12 weeks (p=0.40) and 24 weeks (p=0.24).

The UNADJUSTED time course of mean VISA-P score in the PTLE group (intervention) and EET group (control). Abbreviations: PTLE, progressive tendon-loading exercises; EET, eccentric exercise therapy. The error bars represent ±1 SE.
Main outcome measures at 12 and 24 weeks in the progressive tendon-loading exercise (PTLE) and eccentric exercise therapy (EET) groups

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual changes in the VISA-P score from baseline in patients in the PLTE group (intervention) and EET group (control). Unadjusted individual changes in VISA-P score are shown after 12 weeks and 24 weeks exercise therapy. Adjusted mean between-group differences from baseline to 12 and 24 weeks are shown with 95% CIs. EET, eccentric exercise therapy; PLTE, progressive tendon-loading exercise; VISA-P, Victorian Institute of Sports Assessment for Patellar Tendons.
Secondary outcomes
In the PTLE group, 21% (n=7) returned to the desired sports at preinjury level after 12 weeks and 43% (n=16) after 24 weeks. In the EET group, 7% (n=2) returned to the desired sports at preinjury level after 12 weeks and 27% (n=8) after 24 weeks. The dichotomised return to sports was not statistically different between both groups at 12 weeks (p=0.13) and 24 weeks (p=0.16). The return to sports rate after 12 weeks (p=0.12) and 24 weeks (p=0.25) was not influenced by the symptom duration prior to the interventions. After 12 weeks, 79% (n=26) of the patients were satisfied with the clinical outcome in the PTLE group and 63% (n=19) in the EET group. After 24 weeks, this was 81% (n=30) in the PTLE group and 83% (n=25) in the EET group. The dichotomised patient satisfaction was not statistically different between both groups at 12 weeks (p=0.18) and 24 weeks (p=0.81). The percentage of patients with an excellent satisfaction was significantly higher in the PTLE group (38%) than in the EET group (10%) (p=0.009). Subjective patient satisfaction after 12 weeks (p=0.58) and 24 weeks (p=0.14) was not influenced by the symptom duration prior to the interventions. Adherence to the tendon-specific exercises was not statistically different between the PTLE group and EET group after 12 weeks (p=0.54) and 24 weeks (p=0.33). Adherence to the exercises targeting risk factors was also not statistically different between the PTLE group and EET group after 12 weeks (p=0.91) and 24 weeks (p=0.97). The commonly used and advanced imaging outcomes are included in online supplemental appendix.
Adverse events
No serious adverse events occurred while performing the specific exercises of PTLE and EET during the trial. Two patients sustained ankle sprains while playing sports during the follow-up period. No patients reported using cointerventions during the study period.
Additional secondary outcomes
The additional secondary outcomes in the PTLE and EET groups are listed in online supplemental table S1. The VAS for pain (scale 0–10) related to tendon-specific exercises at 24 weeks was significantly lower in the PTLE group than in the EET group with an estimated mean of 2 vs 4 (adjusted mean between-group difference: 2 (95% CI 1 to 3); p=0.006). There were no significant between-group differences in any of the other additional secondary outcomes.
Discussion
In this randomised controlled clinical trial of patients with PT, PTLE provided superior clinical outcomes compared with EET after 24 weeks follow-up.
The improved performance of PTLE is important and clinically relevant as EET is commonly used in clinical practice and currently the recommended therapy in some guidelines (eg, NICE guidelines).9 Our findings also indicate that PTLE is still beneficial in patients who previously did not improve during prior treatment for PT. We, therefore, recommend a PTLE programme with additional exercises targeting risk factors, load management and patient education as the basis of treatment for physically active patients with PT.
Additional benefits of PTLE were that there was a trend towards a higher return to sports rate compared with EET (43% vs 27%) and that the exercises were significantly less painful to perform (VAS 2 vs 4). The percentage of patients with an excellent satisfaction was also significantly higher in the PTLE group (38% vs 10%). Both treatments involve performing rehabilitation exercises and in practice it would seem logical to opt for the most effective programme.
A suggested reason for the superiority of PTLE is the introduction of isometric exercises, which are considered to immediately reduce pain and facilitate muscle strengthening using isotonic exercises in the subsequent phase, due to an exercise-induced decrease in pain sensitivity.26 Yet, recent well-designed studies did not detect this supposed effect.27 In our study, the major between-group difference was found in the latter half of the exercise programme. This suggests that the phase of energy-storage loading is important to implement before starting the sport-specific exercises.
However, from a critical point of view, less than half of the patients returned to sports at preinjury level after performing PTLE for 24 weeks. Furthermore, despite the positive trend, the difference in return to sports rate with EET was not statistically significant. Also, the difference in patients achieving the predefined MCID after 12 weeks (49% vs 55%) and 24 weeks (87% vs 77%), was not statistically different between both groups. This implicates that there is room for improvement of the current unsupervised PTLE programme, for example, with guidance from a sports physiotherapist. Even with the substantial time investment for patients in both exercise groups, satisfaction after 24 weeks was fairly low. The possibility that a more rapid return to sports at preinjury level through a PTLE programme supervised by a physiotherapist should be investigated.
This is the largest clinical trial in patients with PT to date. Another strength is the comprehensive physical examination and ultrasound confirmation for the diagnosis of PT before enrolment. The outcome measures were extensive and included both clinically used and recently proposed advanced imaging methods.28 29 The interventions were provided using a single consultation with web-based support, making the intervention feasible and generalisable for future implementation.
This study has several limitations. First, inherent in the interventions, blinding of the intervention was not possible for the study patients. However, blinding of the main investigator for the allocated treatment and blinding of the sports physician, radiologist and biostatistician for the clinical outcome was performed. Second, the finding of a better clinical outcome in patients performing PTLE no longer holds if the worst case scenario of the sensitivity analysis of missing data was correct. However, because this worst-case scenario is unlikely, we are confident the advantage of PTLE over EET will be maintained. Third, according to our predefined protocol, we adhered to stratifying patients with early PT vs longstanding PT. We expected a large number of patients with early (short duration) PT who did not yet start exercise therapy. Most patients, however, had longstanding symptoms and had been treated with exercise therapy for either a short period or longer than 12 months ago. Fourth, we observed a substantial spread of individual data points regarding the clinical outcome, indicating that the results of the proposed exercise programme may vary between subjects. This emphasises the importance of an individualised treatment approach. Fifth, the study population consisted of a mix of recreational and competitive athletes, and results could be more specific to either population if the study was more uniform. Finally, this study involved unsupervised exercise therapy, and results may be improved by using a supervised programme.
This study emphasises the importance of exercise therapy for the conservative treatment of patients with PT. Despite the chronicity of symptoms in the patients included in this trial, the large number of patients with bilateral symptoms from PT (42%) and the failure of conservative treatment prior to the time of study commencement (82%), patients in both treatment groups demonstrated improvement in pain, function and ability to play sports. A majority of the patients achieved the MCID or better after 24 weeks, even despite a limited adherence to the exercise programmes (40% for PTLE and 49% for EET).
Conclusion
In this trial among patients with mostly chronic PT, treatment with PTLE is superior to EET, despite presence of chronic symptoms and the previous conservative treatment in the majority of patients. These findings support the use of PTLE in the conservative treatment of PT.
What are the findings?
In the largest clinical trial in patients with patellar tendinopathy (PT) to date, progressive tendon-loading exercises (PTLE) resulted in a clinically relevant benefit compared with pain-provoking eccentric exercise therapy (EET) after 24 weeks follow-up.
There was a trend towards a higher return to sports rate in the PTLE group (43% vs 27%, p=0.13).
No significant between-group differences were found for subjective patient satisfaction (81% vs 83%, p=0.54) and exercise adherence (40% vs 49%, p=0.33) between the PTLE group and EET group after 24 weeks.
The Visual Analogue Scale for pain (scale 0–10) related to the exercises at 24 weeks was significantly lower in the PTLE group than in the EET group with an estimated mean of 2 vs 4 (adjusted mean between-group difference: 2 (95% CI 1 to 3); p=0.006).
How might it impact on clinical practice in the future?
PTLE should be regarded as standard initial care for the treatment of patients with PT.
Data availability statement
Data are available on reasonable request. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Ethics approval
The study protocol for the JUMPER study was approved by the local ethics committee: The Medical Ethics Review Committee of the Erasmus MC University Medical Centre Rotterdam, The Netherlands (NL58512.078.016).
Acknowledgments
The authors thank the National Basketball Association (NBA) and GE Healthcare Orthopaedics and Sports Medicine Collaboration for providing the research grant and GE Healthcare for providing the ultrasound equipment. We also thank Jill Cook and Ebonie Rio for sharing their experience with PTLE during the design phase of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rj_devos
Contributors R-JdV is the guarantor for this study. R-JdV, EHGO, SJB and EV were involved in designing the trial. SJB was the main investigator and responsible for data collection, analyses and writing of the manuscript, while the remaining coauthors revised the manuscript for important intellectual content. R-JdV was responsible for the clinical eligibility assessment in this trial and final randomisation with treatment allocation. SJB and EHGO were responsible for the radiological eligibility assessment in this trial. EV was responsible for the exercise therapy performed in the trial. JZ was the dedicated contact person for participants in the trial after randomisation. JZ was responsible for the statistical analyses performed in this trial. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding Research grant from the National Basketball Association (NBA) and GE Healthcare Orthopaedics and Sports Medicine Collaboration. Ultrasound equipment for this study provided by GE Healthcare.
Disclaimer We plan to disseminate the results to study patients and or patient organisations.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: EHGO and R-JdV had financial support from the National Basketball Association (NBA) and GE Healthcare Orthopaedics and Sports Medicine Collaboration for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.