Article Text

Abstract
Objectives To report COVID-19 illness pattern, symptom duration and time loss in UK elite athletes.
Methods Observational, clinical and database review of athletes with symptomatic COVID-19 illness managed within the UK Sports Institutes. Athletes were classified as confirmed (positive SARS-CoV-2 PCR or antibody tests) or probable (consistent clinical features) COVID-19. Clinical presentation was characterised by the predominant symptom focus (eg, upper or lower respiratory illness). Time loss was defined as days unavailable for full sport participation and comparison was made with a 2016–2019 respiratory illness dataset from the same surveillance system.
Results Between 24 February 2020 and 18 January 2021, 147 athletes (25 Paralympic (17%)) with mean (SD) age 24.7 (5.2) years, 37% female, were diagnosed with COVID-19 (76 probable, 71 confirmed). Fatigue was the most prevalent symptom (57%), followed by dry cough (50%) and headache (46%). The median (IQR) symptom duration was 10 (6–17) days but 14% reported symptoms >28 days. Median time loss was 18 (12–30) days, with 27% not fully available >28 days from initial date of infection. This was greater than our historical non-COVID respiratory illness comparator; 6 days, 0–7 days (p<0.001) and 4% unavailable at 28 days. A lower respiratory phenotype (ie, including dyspnoea±chest pain±cough±fever) was present in 18% and associated with a higher relative risk of prolonged symptoms risk ratio 3.0 (95% CI: 1.4 to 6.5) and time loss 2.1 (95% CI: 1.2 to 3.5).
Conclusions In this cohort, COVID-19 largely resulted in a mild, self-limiting illness. The presence of lower respiratory tract features was associated with prolonged illness and a delayed return to sport.
- athletes
- COVID-19
- infection
- sport
- illness
Data availability statement
No data are available. No additional data are available.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Acute infection with the novel coronavirus, SARS-CoV-2, causing COVID-19 illness, results in a broad range of clinical manifestations in the general adult population.1 Direct pulmonary involvement, with an inflammatory pneumonitis, is the most common reason for hospitalisation; however, other clinical presentations, such as those focused on the upper respiratory (UR) tract, are now widely recognised.2 Studies in the UK general population have now revealed that approximately 10% of individuals with COVID-19 exhibit symptoms lasting more than 28 days and approximately 5% for 84 days or longer.3 The reason an individual may develop a protracted illness course, with delayed recovery, currently remains unclear, but the type of symptoms and/or number of symptoms at presentation, may be indicative. Likewise, while a high level of physical fitness may be protective against the risk of severe disease requiring hospitalisation, it is unclear if this modulates disease course and recovery patterns in mild COVID-19.4 5
In the context of athlete health, a key focus for sporting organisations and their support personnel is the ability to guide an athlete safely to return to high-intensity training and competition following illness or injury.6A successful return to play (RTP) plan acts to inform recovery strategy and manage expectations of the athlete and coaching staff. It is particularly relevant for athletic populations at the elite, international or professional level, where uninterrupted preparation for sporting competition is a key component of athletic and career progression. In this context, RTP decision-making arises from the need to balance the impact of a period of recommended exercise restriction, against the risk of an adverse outcome from infection-related sequelae, including injury risk, following any period of relative rest.7 8
A number of organisations and academic groups have published recommendations regarding RTP following COVID-19,9 10 however there are little data describing the clinical pattern, symptom time course and impact of this illness in elite athletes. Shumacher and colleagues11 reported that in a small cohort of professional footballers (n=15), COVID-19 caused only mild symptoms, lasting less than a week, with no need for hospital care. Similarly, in the questionnaire-based AWARE-I Study, Schwellnus and colleagues12 reported that in athletes with a broad range of athletic capability, COVID-19 was associated with a mild illness lasting approximately 10 days.
The aim of this report was to extend these findings by describing our experience managing COVID-19 in a cohort of international-level Paralympic and Olympic athletes, many of whom were preparing to compete in the 2020 Tokyo Games, using a clinical dataset from the UK Sports Institutes (of England, Scotland, Wales and Northern Ireland). Our primary aim was to report the type and duration of symptoms and their impact on full training and competition participation, and to compare time loss with our historical illness surveillance data for non-COVID-19 acute respiratory illness. A secondary aim was to characterise the COVID-19 clinical presentation that may be indicative of protracted athletic recovery from COVID-19.
Methodology
Study design and subjects
This study was a retrospective case review of all elite athletes diagnosed with symptomatic COVID-19 between 24 February 2020 and 18 January 2021 who received medical care recorded on the electronic medical records systems used by the sports and exercise medicine physicians of the UK Sports Institutes of England, Northern Ireland, Scotland and Wales. The cases are from the population of approximately 2500 athletes who were competing in Olympic, Paralympic or Commonwealth Games sports at a senior international level for their home nation, or Great Britain and Northern Ireland. The study period was split into two waves for analysis to align with the first and second waves of the UK epidemic: the 6 months prior to August 2020 and the subsequent 6 months through January 2021.
Data collection
Athlete demographics, sporting discipline and relevant medical comorbidity data were obtained. The COVID-19 case medical record of all athletes was reviewed by a sports and exercise medicine physician until the end of the study follow-up period (11 March 2021) and the following key variables collected were:
COVID-19 diagnostic criteria; including clinical features and when available, diagnostic test results, that is, PCR from upper airway swabs, or SARS-CoV-2 antibody testing.
Nature and severity of initial symptoms experienced.
Time from symptom onset to resolution (symptom duration).
Time loss was the number of days from symptom onset to full training and competition participation. This included days when athletes were either completely unavailable, or had training modified due to illness.
Investigations, treatment and hospital care required for illness.
All data were anonymised in accordance with the privacy notices associated with the Sports Institutes’ electronic medical records systems, whereby prior informed consent was obtained from all athletes.
COVID-19 case and symptom definitions
Athletes were classified as having either (1) confirmed COVID-19 based on the presence of consistent clinical features and a positive SARS-CoV-2 PCR test or antibody test, or (2) probable COVID-19 based on consistent clinical features alone and diagnosed at a time of heightened community exposure risk in line with Public Health England guidance at this time1 (figure 1). Notably, SARS-CoV-2 antigen or antibody testing was not available in the UK for non-hospitalised individuals during the UK epidemic first wave.

Athlete numbers with COVID-19, with UK new case data overlaid from the UK government’s coronavirus dashboard (downloaded on 25 February 2021).22
Symptomatic presentation was classified into five clinical phenotypic groups, based on the predominant anatomical focus:
UR: sore throat±change in smell or taste or sinus problems reported±a cough±fever.
Lower respiratory (LR) illness: presence of dyspnoea±chest pain±cough±fever±other LR tract symptoms (eg, wheeze).
Cough only: cough as the predominant symptom recorded and in the absence of coexisting dyspnoea and without other UR symptoms.
Gastrointestinal (GI): with predominant symptoms being diarrhoea±nausea±abdominal pain.
Non-specific: main clinical feature was fever, fatigue±headache±myalgia but a lack of any prominent respiratory or GI symptoms.
The COVID-19 symptom and time loss duration was grouped as short (≤28 days) or prolonged (>28 days) in a similar manner to Sudre and colleagues.3
A historical acute respiratory illness comparator dataset was obtained from the English Institute of Sport (EIS) Performance Data Management System from 1 January 2016 to 31 December 2019. This dataset consisted of all cases with the diagnostic code of ‘respiratory tract infection’ and was the same electronic medical records and health surveillance system that was used to identify the COVID-19 diagnoses.
Data and statistical analysis
Data are reported as mean (SD) or median (IQR or range). Symptom duration and time loss were not normally distributed and were compared using the non-parametric Mann-Whitney U test. Χ2 tests, or Fisher’s exact test when expected cell counts were below five, were used to compare subgroups of the population to see whether they shared the same proportion of probable versus confirmed cases, prolonged symptom duration or time loss. Χ2 tests and risk ratio calculations were performed using a series of 2×2 tables splitting the data into presence/absence of the feature being tested. A Haldane-Anscombe correction of 0.5 was automatically applied to any tables that contained a zero-cell count. All CIs are at 95%. For all analyses, a p value of <0.05 was considered significant. Analyses were performed using Python V.3.8 with Pandas (V.1.0.5), statsmodels (V.0.11.1) and SciPy (V.1.5) packages. Graphics were produced using Python V.3.8 with Matplotlib (V.3.2.2) and Seaborn (V.0.11.1) packages.
Results
Athlete characteristics
A total of 147 athletes (92 male; 63%) were diagnosed with COVID-19, with a similar proportion of confirmed (n=71; 58 antigen confirmed, 13 antibody confirmed) and probable (n=76) cases (table 1). A similar number of athletes developed COVID-19 during the first and second waves of the UK epidemic, at 80 and 67, respectively (figure 1); and characteristics of athletes with confirmed and probable cases were similar (online supplemental table 1).
Supplemental material
Athlete characteristics and COVID-19 symptom patterns
The majority of athletes were preparing for summer sports (93%) and in able-bodied sport (83%), with the overall general demographic characteristics (ie, age and gender distribution) of athletes with COVID-19 considered representative of the UK Sports Institutes’ athlete pool (data not presented). The majority of athletes (77%) had no medical comorbidities, although, when present, asthma was the most common condition reported (18%).
COVID-19 symptom pattern and clinical phenotypes
A broad range of symptoms were reported (table 2) at presentation with fatigue, cough and headache being most prevalent, in 57%, 50% and 46% of athletes, respectively. Dyspnoea was reported in 18% of athletes. GI symptomology was the least prevalent presentation, apparent in only three athletes (2%). The presence of multiple symptoms (ie, ≥3) was apparent in 38% of athletes and 18% reported five or more symptoms at presentation. The most prevalent clinical phenotype was UR, classified in 37% of athletes. Symptom and phenotype pattern was comparable between male and female athletes and between confirmed and probable cases (online supplemental table 1).
The majority of athletes reported mild symptoms (n=140, 95%), that did not limit their ability to perform activities of daily living (eg, self-care). No athletes required hospital care or specific COVID-19 treatment (eg, oxygen or dexamethasone).
COVID-19 symptom duration and time loss
The median (IQR, range) between symptom onset and resolution was 10 days (6–17 days, 0–148 days) (figure 2) with female athletes having a slightly longer median symptom duration than male athletes at 12 days (8–18 days, 3–138 days) vs 9 days (5–16 days, 0–148 days), respectively (p=0.006). Of the total cohort, 21 athletes (14%) had symptoms >28 days and 5 (3% of total) had symptoms lasting >90 days. Symptom duration was similar between able-bodied and Paralympic athletes (p=0.46) and in those with and without asthma (p=0.95).

COVID-19 symptom duration.
Symptom duration was shorter in those presenting with a UR versus LR phenotype, at 10 (IQR 7–15, 2–148) and 18 (IQR 10–33, 4–121) days, respectively (p=0.01) (figure 3).
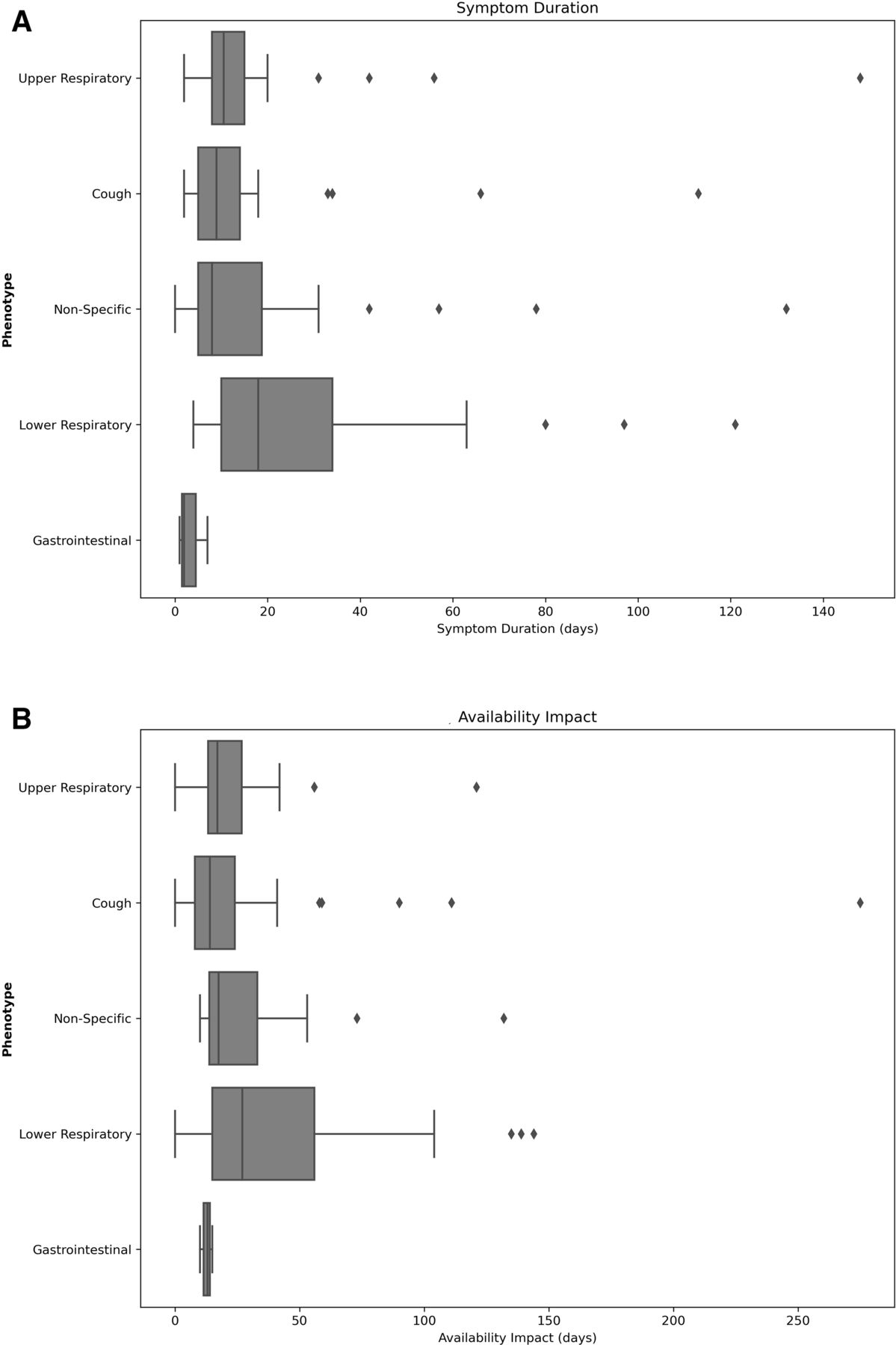
(A) Symptom duration based on COVID-19 clinical phenotype, and (B) time loss based on COVID-19 clinical phenotype.
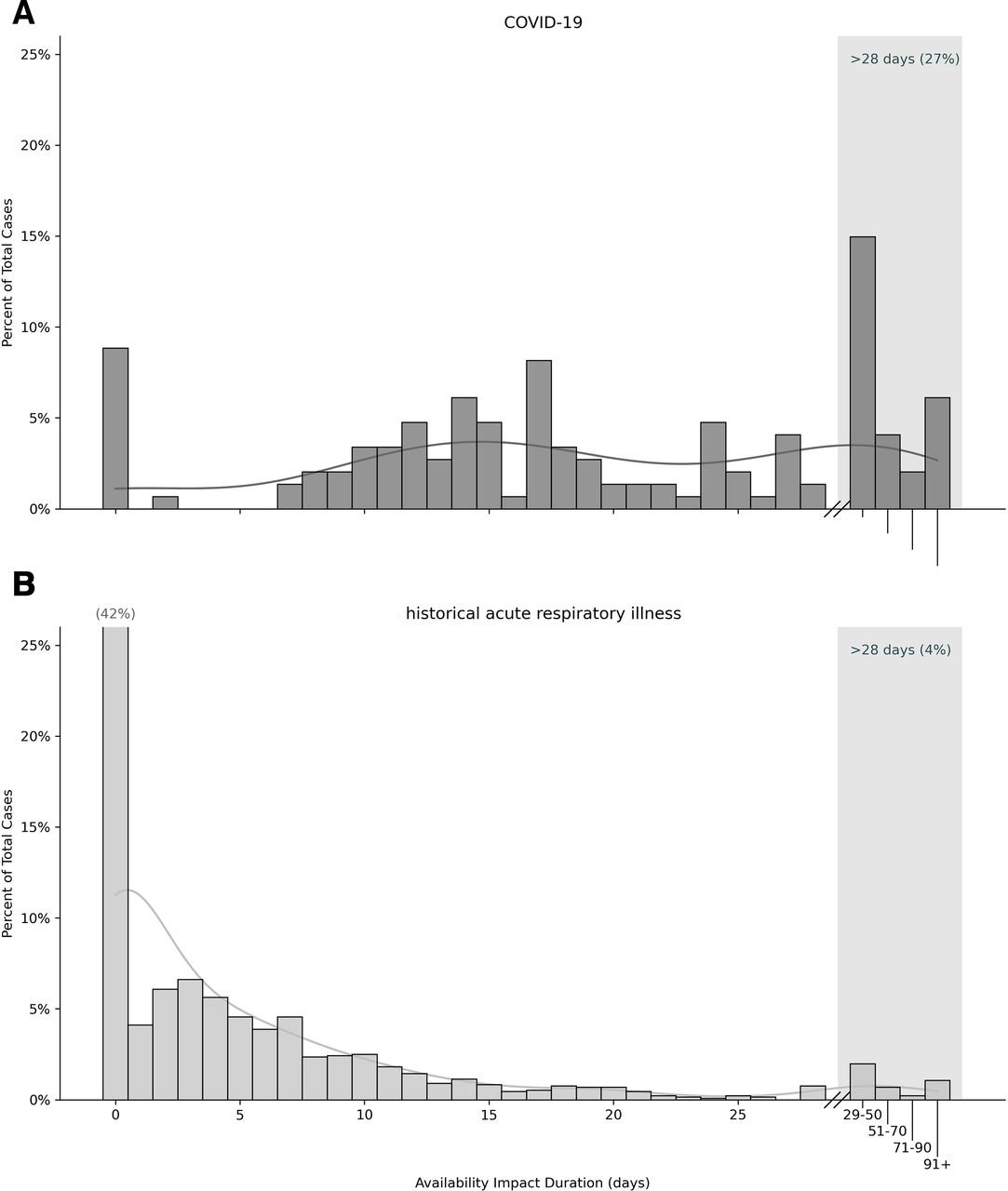
The median (IQR, range) time loss was 18 (12–30 days, 0–275 days) (figure 4). Of the total cohort, 75 (51%) athletes had more than 17 days of time loss, of whom 40 (27%) athletes were still not fully available >28 days and 9 (6%) >90 days. Seventy-one per cent of athletes with >28-day symptoms also had >28-day time loss.

Time loss from (A) COVID-19 (B) historical data for acute respiratory illness in the UK Sports Institute system.
Characteristics of athletes with prolonged (>28 days) time loss
The presence of chest pain at presentation was associated with a higher likelihood of prolonged time loss (>28 days), with no other single symptom indicative of prolonged return to full sport participation (table 2 and figure 5). The presence of five or more symptoms was also not associated with prolonged time loss (p=1.0).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk ratio of (A) >28-day symptom duration versus individual symptoms at presentation and (B) >28-day time loss versus individual symptoms at presentation.
Athletes with LR symptoms were 2.1 (CI 1.2 to 3.5) times more likely to have a prolonged time loss (>28 days). The sensitivity of LR to detect this was 0.30 (CI 0.17 to 0.47) and the specificity was 0.88 (CI 0.80 to 0.93). Thus, in this cohort, the negative predictive value of LR (probability of not having prolonged time loss without LR phenotype) was 77% (CI 73% to 81%), whereas the positive predictive value (probability of having prolonged time loss given LR phenotype) was 48% (CI 32% to 65%). There were no other predictive factors (tables 2 and 3, figure 3).
Association of athlete characteristics and symptom patterns with symptom duration
Athlete characteristics and symptom patterns associated with prolonged time loss (>28 days)
Comparison of time loss for historical EIS acute respiratory illness data
Our review of historical illness surveillance data revealed a shorter duration time loss period for acute respiratory illness with a median of 6 days (IQR 0–7 days, 0–224) (p<0.001) (figure 4). The prevalence of a prolonged time loss was also lower at 4% for acute respiratory illness vs 27% for COVID-19 (p<0.001).
Discussion
The primary aim of this study was to report the clinical characteristics, disease course and impact of COVID-19 on full sport participation, in a cohort of very closely monitored and supported international athletes, many of whom were in the preparatory phase for the 2020 Tokyo Olympic and Paralympic Games. Our analysis included athletes who developed COVID-19 in both the first and second UK epidemic waves, representing approximately 6% of the UK Sports Institutes’ athlete pool. Respiratory tract-focused symptomatology was the most common presentation; with fatigue, cough and headache being the most prevalent symptoms; GI issues were uncommon.
In keeping with the findings reported in an age-matched demographic of the general population with COVID-19,3 in the vast majority of cases, COVID-19 was a self-limiting illness, with symptoms lasting a median of 10 days and with no cases requiring specific targeted treatment (eg, oxygen or dexamethasone) or acute hospital care. Further, COVID-19 illness did not appear to be associated with protracted symptoms in the majority of athletes; that is, at 1 month following the onset of symptoms, only approximately 1 in 10 athletes remained symptomatic, again broadly aligning with the general population findings.
In contrast, however, COVID-19 does appear to have a more pronounced impact on full athletic recovery with over a quarter of athletes in this cohort not returned to full sport participation at 1 month following their initial infection date. Moreover, 6% of athletes were still limited at 3 months. This delayed return to full sport participation has profound implications for competition preparation, particularly given the close proximity to the Tokyo Olympic and Paralympic Games. It also compares unfavourably with our historical data, monitoring the impact of respiratory tract ‘infection’ time loss in this population of internationally competitive athletes. In the vast majority of our historical case series, an infective pathogen was not identified, and thus it is not possible to reliably compare the impact of SARS-CoV-2 infection with other specific viral pathogens.
It is important to note that, at the time of study, UK Sports Institute COVID-19 RTP guidance7 recommended a minimum of 7 days of graded return with training modification and thus this and a conservative approach to RTP in the context of this novel pathogen may have influenced the calculation of short-term (ie, <1 month) time loss.
An associated aim of this evaluation was thus to determine if there were factors that could help clinicians when trying to assess and predict the development of protracted COVID-19 recovery. Historically, the ‘neck check’ rule has been used to aid RTP in athletic individuals with respiratory symptoms.13 Specifically, it has been proposed that if respiratory symptoms localise to the UR tract (eg, sore throat and/or coryzal symptoms), then these are unlikely to impact training and it would be feasible to allow an athlete to continue with some form of exercise; whereas for those with symptoms below the neck, a period of full exercise cessation is recommended. This approach has, however, never been robustly evaluated in a prospective randomised trial and thus although widely used, remains contentious. Data from the recent AWARE-1 Study challenge this approach and indeed promoted the value of identifying a ‘symptom cluster’ that was associated with prolonged RTP, in symptomatic athletes with acute respiratory illness (including COVID-19). In addition, that study revealed that excessive fatigue was a key symptom associated with protracted RTP, with 70% of athletes with this symptom demonstrating an RTP greater than 40 days following infection,12 a finding that aligns with data from a general population symptom-tracker study in the UK from Sudre and colleagues3 who reported that fatigue at presentation was associated with an almost threefold likelihood of an individual developing long COVID-19.
In the current study, reporting data from an elite athlete cohort, we found that the presence of an LR pattern (ie, including features such as dyspnoea, chest pain and cough) was most indicative of a prolonged return to full training and was associated with almost three times the likelihood of a prolonged time loss (>28 days). This was a relatively arbitrary division, based on the presence of clinical features alone, and thus without confirmatory radiological or laboratory investigations, but may be indicative of likely low-grade pulmonary inflammation and potentially a more pronounced systemic response.
However, even based on clinical report, we found that a presentation confined to the UR tract was associated with a shorter duration of illness (median symptom duration of 10 days for the UR phenotype compared with 18 days for the LR phenotype) and a shorter return to full sport participation (median time loss of 17 days for the UR phenotype compared with 27 days for the LR phenotype). The reason this differs from the AWARE-1 findings may relate to differences in the study population (ie, elite vs broader athletic capability) and methodology (ie, medical records vs self-reported questionnaire data). Regardless, an approach that identifies the pattern of symptom localisation may be helpful in managing expectations regarding symptom duration and full sporting participation in elite athletes and now needs to be assessed and further validated in a broad range of athletic cohorts.
Several guidelines have now been published regarding protocols for RTP for athletes recovering from mild-moderate COVID-19 illness.7 14 The most widely used guidance, that appeared early in the first wave of the global pandemic, recommended at least 10 days between symptom onset and the start of graduated exercise progression over a further 7 days. This 17-day minimum graduated RTP (GRTP) was advocated to mitigate any risk of vigorous exercise early in the illness heightening susceptibility to more serious complications (eg, pneumonia or cardiac inflammation). Data since that time indicate a very low overall incidence of these types of complications15 and thus on the basis of a risk analysis a recommendation for shorter duration of exercise cessation may be appropriate, certainly in athletic individuals with relatively short-lived symptoms that are confined to the UR tract. It is noteworthy that data from two recent studies, enrolling a significant number of elite athletes, reveal cardiac inflammatory sequelae from COVID-19 in only a small proportion of athletes (approximately 0.6%).16 17
The reason why an athlete may suffer from protracted symptoms and a delayed return to sport has not been systematically evaluated or presented in this report. Several mechanisms have been proposed (eg, autonomic dysfunction) and several are potentially relevant in the context of a delayed return to full sport participation.18 19 Indeed, while ongoing detailed clinical evaluations are being conducted to establish relevant factors in Home Nation Sports Institutes (HSNI) athletes with protracted illness, this was not an aim of the current work, and we did not continue to prospectively track the intensity of persisting symptoms and limited exercise tolerance. This work is clearly needed in studies evaluating the pathophysiological mechanisms (including cardiac involvement) underpinning protracted COVID-19 recovery in both the general and athletic population.
Methodological considerations
Several methodological limitations are worthy of consideration. In the UK first wave, there was no community-based access to SARS-CoV-2 antigen testing. In this work, we therefore had to characterise the cohort, based on a classification as either a probable or confirmed diagnosis. It is therefore possible that some of the cases could have been classified incorrectly. Our comparison of these groups however shows similar clinical characteristics (online supplemental file 1) and we used the Public Health England diagnostic guidance at that time to evaluate cases in at time with very heightened background infection rate and avoidance strategies in place in the UK.1 While dyspnoea was more prevalent in the probable versus confirmed cases, dyspnoea alone was not independently associated with a longer time loss. Notably, the prevalence of chest pain which was associated with longer time loss was similar between probable and confirmed cases. Additionally, in contrast with general population, this cohort of individuals are closely monitored from a health point of view and have regular and detailed contact with Sport and Exercise Medicine (SEM) professionals. Overall, it therefore seems likely that these cases do represent true SARS CoV-2 infection.
In this respect, it is also noteworthy that, when compared with the background case rate in the UK, there appears to be a reduced prevalence or potential ‘infection rate’ during the second wave (figure 1). This pattern may reflect the paucity of community-based tests in the first wave in the UK, or indeed the fact that more robust infection avoidance strategies were in place for the second wave. Certainly, within the HSNI, COVID-19 risk mitigation and testing systems improved considerably between the first and second waves. It is likely that illness behaviour will continue to be dramatically altered by global vaccination strategies, when they are widely available in athletic populations.20
Ideally, we would have wished to use a prospective design to track athlete symptoms and to use a validated scoring system to record and characterise disease severity. However, the data collection system used at that time did not permit this type of analysis. Our definition of ‘time loss’ is one employed in the UK Sports Institutes and thus allowed direct comparison with our historical surveillance database. This is based on clinicians’ assessment of whether athletes are fully available to train and compete, and given the same systems were used for both historical monitoring and during the COVID-19 pandemic, provides methodological rigour. However, whether return to being ‘available’ is actually indicative of a full athletic recovery is likely to be more accurately determined by detailed physiological and psychological assessment. It is also possible that heightened clinical scrutiny, quarantine and GRTP requirements, in the context of this novel pathogen and an evolving understanding of COVID-19, may have influenced athlete symptom reporting or indeed prompted caution with respect to the acute RTP advice afforded to an athlete. Although this is likely to be relevant in some cases, it is worth noting that this cohort of athletes were highly motivated to continue uninterrupted training, given uncertainty regarding the timeline for the Tokyo 2020 Olympic Games and other international selection events. Overall, therefore, we feel that it is unlikely that a conservative approach to RTP significantly influenced the data reported of time loss at 28 days following the onset of infection.
A final limitation is that this study may suffer from sparse data bias21 due to the low occurrences of various combinations of case characteristics (eg, summer vs winter sports, or clinical symptoms such as chest pain) as can be seen in tables 2 and 3. As such, the risk ratio estimates and CIs may be biased upwards if above 1, or downwards if below 1, and this should be considered in the interpretation and potential application of the data presented.
Conclusion
In a cohort of elite athletes, COVID-19 was associated with a mild, self-limiting illness, lasting on average 10 days, but causing prolonged impact on full sport participation, longer than a month, in a quarter of athletes. Delayed RTP was associated with LR tract symptoms, specifically chest pain, at presentation and therefore consideration might be given to expediting RTP in athletes presenting with mild, short-lived COVD-19 symptoms confined to the UR tract. Further work is needed to determine the mechanisms associated with prolonged time loss following COVID-19 illness.
What are the findings?
In a cohort of elite athletes, preparing for international competition, COVID-19 illness largely resulted in a mild, self-limiting illness, not requiring hospital care.
The pattern and duration of COVID-19-related symptoms was similar to that reported in the UK general population; however, approximately a quarter of athletes had not returned to full sport participation at 28 days after symptom onset.
The presence of clinical features implicating lower respiratory tract involvement was associated with prolonged illness and delayed return to full sport participation.
How might it impact on clinical practice in the future?
Insight regarding the clinical course and time loss following COVID-19 illness in elite athletes informs recovery management and athlete counselling.
Consideration could be given to expediting return to full sporting participation for those who present with symptoms primarily confined to the upper respiratory tract.
Further work is needed to determine the factors underpinning a delayed return to full sport participation following COVID-19 in some athletes.
Data availability statement
No data are available. No additional data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was then approved by a UK Sports Institutes medical group, as a clinical audit, and therefore not requiring ethical approval.
Acknowledgments
The authors would like to thank Faye Hodson for administrative assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Breathe_to_win, @neilSportDoc, @EmilWalsted, @dundeesportsmed, @craig_ranson
Contributors JHH and CR designed and developed the protocol, assisted with data analysis, and drafted, edited and approved the manuscript. MW performed all data analyses and acts as the guarantor for data. ESW provided statistical analysis and review of the manuscript. MM, NH, RM, AB, ML and NE contributed to the methods and data collection, and assisted production of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.