Article Text

Abstract
Objective To determine the incidence of acute respiratory illness (ARill) in athletes and by method of diagnosis, anatomical classification, ages, levels of performance and seasons.
Design Systematic review and meta-analysis.
Data sources Electronic databases: PubMed-Medline, EbscoHost and Web of Science.
Eligibility criteria Original research articles published between January 1990 and July 2020 in English reporting the incidence of ARill in athletes, at any level of performance (elite/non-elite), aged 15–65 years.
Results Across all 124 studies (n=1 28 360 athletes), the incidence of ARill, estimated by dividing the number of cases by the total number of athlete days, was 4.7 (95% CI 3.9 to 5.7) per 1000 athlete days. In studies reporting acute respiratory infections (ARinf; suspected and confirmed) the incidence was 4.9 (95% CI 4.0 to 6.0), which was similar in studies reporting undiagnosed ARill (3.7; 95% CI 2.1 to 6.7). Incidences of 5.9 (95% CI 4.8 to 7.2) and 2.8 (95% CI 1.8 to 4.5) were found for studies reporting upper ARinf and general ARinf (upper or lower), respectively. The incidence of ARinf was similar across the different methods to diagnose ARinf. A higher incidence of ARinf was found in non-elite (8.7; 95% CI 6.1 to 12.5) vs elite athletes (4.2; 95% CI 3.3 to 5.3).
Summary/conclusions These findings suggest: (1) the incidence of ARill equates to approximately 4.7 per athlete per year; (2) the incidence of upper ARinf was significantly higher than general (upper/lower) ARinf; (3) elite athletes have a lower incidence of ARinf than non-elite athletes; (4) if pathogen identification is not available, physicians can confidently use validated questionnaires and checklists to screen athletes for suspected ARinf. For future studies, we recommend that a clear diagnosis of ARill is reported.
PROSPERO registration number CRD42020160472.
- respiratory system
- athletes
- sports
- exercise
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A significant proportion of all medical consultations (~50%) at international single sport1–8 and multisport events such as the Olympic,9–13 Paralympic14–16 and Youth Olympic Games17 18 are due to acute illness in athletes, of which the respiratory system is consistently the most common organ system affected.3 6 7 10 11 19 20 Acute respiratory illness (ARill) was the most common medical condition affecting athletes at both Summer and Winter Olympic and Paralympic Games,11 13 20 21 as well as other major events and tournaments.22 23 ARill in athletes can be broadly classified by an anatomical classification of ARill (predominantly affecting the upper or lower airways), and a pathological classification (non-infective ARill or acute respiratory infections (ARinf)). An athlete can present with a variety of symptoms of ARill, including upper ARill symptoms (blocked nose, runny nose, sore throat, swollen glands), lower ARill symptoms (cough, wheeze, chest pain) and in some cases ARill can be associated with systemic symptoms (fever, general fatigue and myalgia). While some symptoms indicate that the ARill is more likely to be due to ARinf (sore throat, swollen cervical lymph, fever) there is considerable overlap in the clinical presentation of non-infective ARill and ARinf. In most studies to date on ARill in athletes, the diagnosis was based on history and clinical assessment without laboratory confirmation of an infection, or the identification of a specific pathogen. Therefore, in the published literature on ARill in athletes it is not always possible to determine if athletes had a non-infective ARill or a suspected/confirmed ARinf. In these studies, the ARill was reported without a specific diagnosis because the ARill could not be attributed to an infective or non-infective cause.
ARill may occur at various stages of training and competition including the precompetition period (preparation training period), competition period (intracompetition) and/or postcompetition recovery period.24 25 ARill, in particular ARinf and can interrupt training and impact competition performance.26 27 While most ARill may be easily managed by the team physician, some may have systemic sequalae which can constitute a serious threat to the health of the athlete. Thus, it is important for clinicians to know how many ARill can be expected to occur in their team, over what period and which athletes may be more susceptible to ARill. Different factors may influence susceptibility to ARill in athletes, such as intensity and duration of exercise,28 participating in events and/or tournaments,21 gender29 and season of training and competition.30 Spence et al31 observed substantially higher incidence rates of ARill in elite athletes compared with recreationally competitive athletes.
Numerous studies have investigated the incidence of ARill in athletes participating in different sports, including runners,23 32 33 cyclists,34 cross-country skiers,35 swimmers,36–38 rowers39 and in athletes from other team sports such as rugby players40 and wheelchair athletes.41 Previous studies investigated ARill in different levels of performance, different types of ARill (infective vs non-infective) and using different types of diagnostic methodologies.42 To our knowledge, no previously conducted epidemiological studies have convincingly determined the overall incidence rates of ARill in athletes, nor has it been determined whether the incidence of ARill is affected by level of performance or age of the athlete. Thus, the primary aim of this systematic review and meta-analysis was to determine overall the incidence of ARill, including subgroups categorised by pathology (ARinf vs undiagnosed ARill), predominant anatomical region affected (upper vs lower respiratory tract or general), different levels of athletic performance (elite vs non-elite athletes), age groups (15–35 years vs >35 years) and season (summer vs winter).
Methods
Protocol and registration
A protocol was developed according to the guidelines outlined in the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.43
Study selection and eligibility criteria
Eligibility criteria were established and agreed on by all authors based on the concepts of population, intervention/indicator, comparator/control and outcome. Studies that met the following inclusion criteria were considered eligible to be included in this systematic review and meta-analysis:
Participants, both male and female, aged 15–65 years, who are athletes at any level (recreational to elite) engaged in training.
Participants had self-reported, physician or laboratory diagnosed ARill.
Studies reported ARill during events, tournaments, multistages of events and those that are reported directly after an event.
Studies reported the number of ARill among the participants as well as documented the study period.
Journal article with full-text original prospective and/or retrospective studies published in English between 1 January 1990 and 31 July 2020.
Exclusion criteria were set as:
Studies conducted in animals or human cells expressed in rodents.
Conducted with a heterogeneous sample (ie, mixed sample of athletic and non-athletic populations) without reporting individual group findings separately.
Studies available as an abstract only (ie, conference presentations), qualitative or case series, discussion paper, commentary or literature review.
Studies not available in English.
Studies specifically investigating only known non-infective ARill, including asthma, airway allergies or cold air injury (studies reporting ARill that could include both ARinf and non-infective causes were included and categorised as undiagnosed ARill).
Search strategy
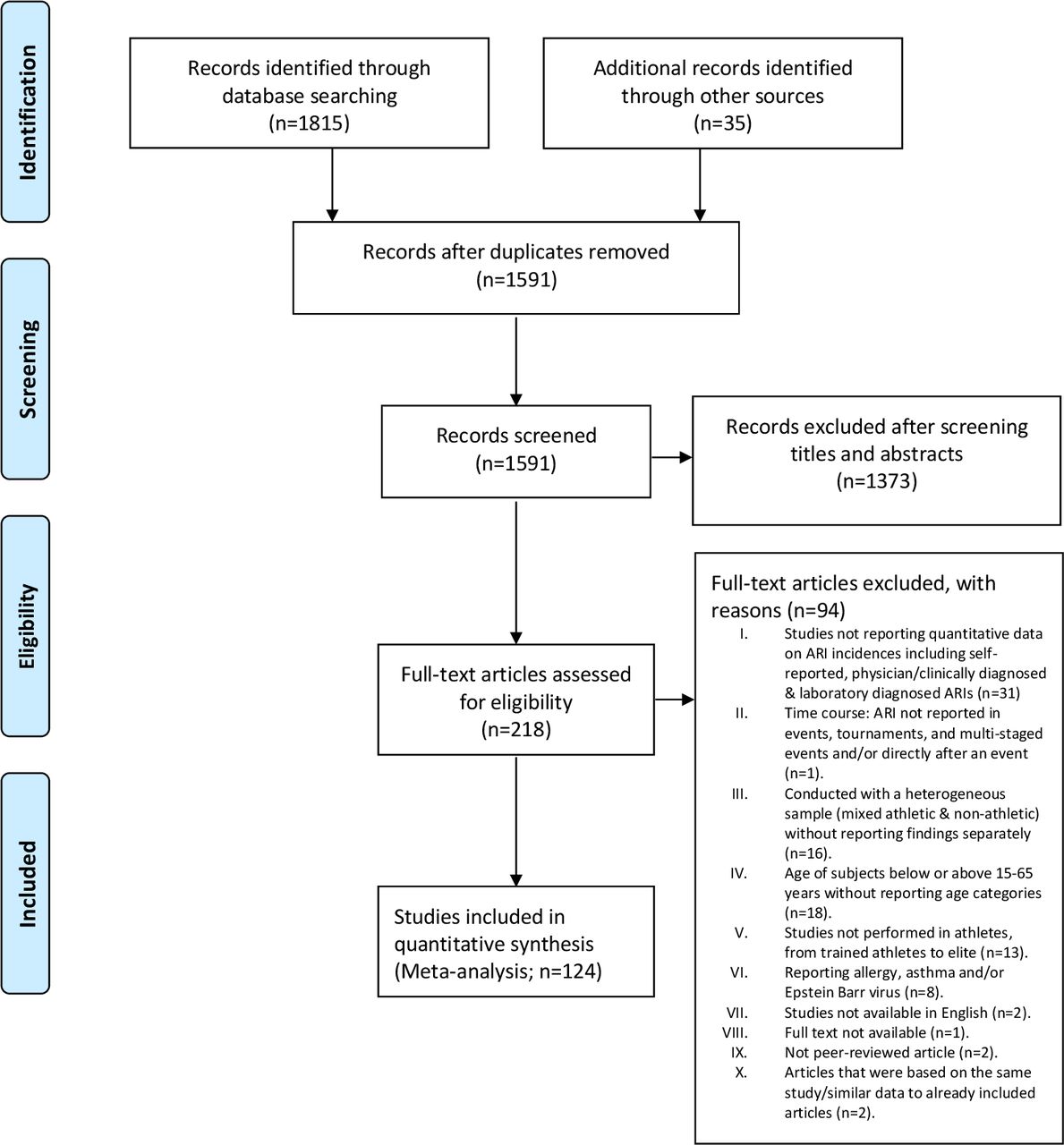
PubMed-Medline, EbscoHost and Web of Science (core collection) databases were searched for published articles from 1 January 1990 to 31 July 2020. Medical subject heading (MeSH) terms included a combination of search terms relating to (acute respiratory illness AND athlet* AND prevalence/incidence) and relevant exclusions (for full search string for each database, see online supplemental file S1). Studies including the terms ‘allergy’ and ‘asthma’ were excluded from the search, as these terms are covered in separate comprehensive assessments of asthma and allergy in athletes (IOC consensus statement subgroups; under review). A secondary search of the reference lists of included articles, and an additional search in Google Scholar were conducted, as well as addition of other articles identified by the authors, that were not captured in the original search. The results of these searches were combined, and duplicate articles removed (figure 1).
Supplemental material

{kind=link}
PRISMA flow diagram visualising the selection process of identified, screened and included articles following assessment of the eligibility criteria. ARI, acute respiratory illness; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Article screening and selection were performed using the online platform Central Access Database for IMpact Assessment (CADIMA).44 Articles were initially screened by title and abstract independently by two reviewers (LK and MB) using the selected inclusion/exclusion criteria. After this initial screening, the full texts of the articles were retrieved, and a second screening was undertaken by independent reviewers (MM, MG, LK and ME). Any conflicts were resolved through discussion and consensus was achieved between the reviewers.
Data extraction
The following data were extracted from the included articles by two independent reviewers (LK and MB) and checked by another author (ME): Participants (number, age, gender), study design, method used to diagnose illness, illness classification (pathological and anatomical), level of performance (professional/elite or amateur/trained/competitive/recreational), sport type, length of surveillance period and the number of ARill.
Definitions and classification of subgroups of ARill
We recognise that the methods used to diagnose an ARill, and specifically an ARinf can vary and include symptoms only, additional findings on clinical examination, and the use of special investigations to identify a specific pathogen. The methods used to diagnose ARill in each study were classified as follows: (1) self-reported symptoms of ARill only and (2) self-reported symptoms but with an algorithm indicative that was validated for ARinf. The validated questionnaires that were used included the Wisconsin Upper Respiratory Symptom Survey-2145 or the Jackson Cold Scale46 or other questionnaires in which the severity of the symptoms were scored to provide a quantitative assessment according to Fricker et al28 and Matthews et al (AIS Symptom log),47 (3) self-reported symptoms of an ARinf reviewed by a physician, but without clinical or laboratory evaluation, (4) clinical diagnosis of an ARinf by a physician, based on history and clinical examination, (5) diagnosis of ARinf by a physician that was confirmed by laboratory investigation to identify a specific pathogen as follows: PCR testing on specimens, culture of an organism from specimens, or serology (eg, rise in antibody titres). Data were extracted for each study, and this was agreed on by consensus (WD, MM, MG, JF, KM and NS). Once studies were classified by the five methods of diagnosis, all ARill studies were included in one of the following main and subgroups of ARill, based on a pathological classification (table 1).
Pathological classification (main and subgroups) of acute respiratory illness (ARill) and infections (ARinf) by diagnostic method
We acknowledge that ARill, including ARinf, frequently presents with both upper and lower respiratory tract symptoms/signs and it is not always possible to clearly distinguish between these main anatomical regions when classifying ARill. A limitation of this anatomical classification is that several pathogens that cause predominantly upper ARinf can, in some cases, present with lower respiratory and/or systemic symptoms. However, from a clinical/pragmatic point of view, and the fact that a clear distinction is made in many studies, we felt that it is relevant to include this anatomical classification in the review. Upper ARinf (suspected or confirmed) is the most common acute illness in athletes. We classified all studies of into the following subgroups, based on the predominant anatomical region affected:
Upper (ARill or ARinf): Studies where the predominant symptoms, signs, or confirmed pathology was clearly related to the upper respiratory tract (ie, above the larynx), or if the study specifically referred to athletes with upper respiratory illness. A few studies referred to clinical syndromes of ARinf using non-specific terms such as ‘influenza’, ‘influenza symptoms’, ‘common cold’, ‘symptoms suggestive of influenza’, ‘influenza symptoms’ or ‘influenza like’. Studies referring to these clinical syndromes were also included in this broad anatomical classification because they are caused by pathogens that all present with predominantly upper respiratory tract symptoms.48–51 Notably, this includes influenza viruses, which also predominantly present with upper respiratory tract symptoms52 and are listed as a cause of upper respiratory tract infections.48–50
Lower (ARill or ARinf): Studies where the predominant symptoms were below the larynx (including chest symptoms that is, cough, chest pain), or if the diagnosis specifically referred to athlete with lower respiratory illness (tracheal, bronchial or lung pathology for example, pneumonia).
General (upper/lower) (ARill or ARinf): Studies where it was not possible from the methods or results to distinguish between predominantly upper or lower respiratory tract ARill or ARinf, and could therefore include upper, lower or both.
Performance level
The athlete’s level of performance was categorised as follows: (1) Professional athletes (member of a professional league), (2) elite (international competition), (3) amateur athletes (largely or entirely engaged in sports without remuneration,53 (4) competitive (collegiate or regional) athletes, (5) trained athletes (undertaking daily exercise engaged in similar volumes of training as competitive athletes) and (6) recreational athletes (physically active but who does not train for competition at the same level of intensity and focus as competitive athlete.54 For subgroup analyses, the professional and elite athletes were combined and referred to as ‘elite’ athletes. There were five studies where athletes were classified as recreational, and these were included in the analysis with the combined amateur, competitive and trained athletes. This subgroup was referred to as ‘non-elite’ athletes.
Age groups
The age groups of athletes that were included in the studies were categorised as: (1) 15–35 years or (2) older than 35 years. The age threshold of 35 years was chosen based on the International Masters categorisation.55
Quality assessment and risk of bias
A modified Downs-and-Black tool was used to determine the quality of the articles.56 The tool consisted of items as follow: reporting, external validity, internal validity (bias and selection bias). Each item was scored as ‘yes’ (score=1), ‘no’ (score=0) or ‘undetermined’ (score=0). Four reviewers (LK/ME/MM/MG) performed the independent quality assessment of the studies. The same reviewers determined the level of evidence using the 2009 Oxford Centre for Evidence Based Medicine (OCEBM).57 The studies fell into two main categories: (1) Observational studies of symptoms of ARill in populations; (2) Intervention studies where the incidences of ARill were determined in response to an intervention. The observational studies were graded using the OCEBM ‘Symptom Prevalence Study’ levels of evidence, and the Intervention studies were graded using the ‘Therapy/Prevention Studies’ levels of evidence for randomised controlled trials.
Data analysis
The estimated pooled incidence of ARill and ARinf (determined by dividing the number of new cases of ARill and ARinf observed, by the total number of athlete days, per 1000 athlete days) were estimated using the DerSimonian Laird Random effects model58 to account for the heterogeneity in the cohorts (eg, differences in diagnostic technique, performance level of athlete) and weighting of studies. The estimations for ARill and ARinf were based on the number of studies in the individual categories, hence they have different denominators to calculate the IR. Heterogeneity was measured using I2 and Cochran’s Q statistics.59 Forest plots were produced to illustrate the results. All meta-analyses were conducted by using MetaXL.60 A significance level of 0.05 was accepted, and all statistical tests were two tailed. Differences between subgroups were determined by comparing 95% CIs.
Analyses of the following subcategories were also performed (only subcategories with more than three articles) based on the following: (A) methods to diagnose ARill, (B) pathological classification and (C) the anatomical classification (table 1).
A further analysis was done based on subgroups of ARinf, including studies that could confirm an infection (ARinf confirmed) and studies that used various methods to diagnose an infection (ARinf suspected) as follows:
The athlete’s performance level: Elite (including elite and professional athletes) or non-elite (including trained, amateur, competitive and recreational athletes).
Age group: 15–35 years or older than 35 years.
Season: Summer or Winter.
Quality of the study, based on modified Downs-and-Black tool: Excellent, good, fair or poor.
Results
Study selection
A total of 1583 studies were identified in the databases and additional sources for screening. Figure 1 summarises the study selection process and reasons for excluding studies. The full texts of 218 articles were assessed for eligibility, 94 were excluded and 124 were used for data extraction. All articles that passed the inclusion criteria (n=124) were included in the meta-analysis for the pooled incidence of ARill, as well as for the illness diagnosis sub analysis. For the remainder of the subanalyses, only studies that investigated ARinf (‘Infective confirmed’ or ‘Infective suspected’) in the anatomical classification of ‘upper’ or ‘general (upper/lower)’ were included (n=107). ARill in the ‘undiagnosed’ subcategory (n=17) were excluded from this subanalysis.
Level of evidence and quality assessment
Of the total studies assessed, 47 studies (38%) were rated using the 2009 OCEBM scale57 as 1b level of evidence, 21 studies (17%) were rated as 2b level of evidence and 56 studies (45%) were rated as 3b level of evidence (online supplemental table 2).
Supplemental material
The results of the quality assessment, using the modified Downs and Black scores, are presented in online supplemental table 3. The majority of studies were rated either excellent or good (n=104; 89%). The studies that were rated as fair (n=5; 4%) or poor (n=9; 7%) were mostly based on failing to meet the internal and external validity requirements, not reporting actual probability values, not describing characteristics of participants lost to follow-up, not providing estimates of random variability in the data for the main outcomes and not describing findings in the main outcomes. Studies rated as ‘poor’ were not excluded from analyses.
Study characteristics
The data extracted from the studies included in the present analysis are presented in online supplemental table 2A. The 124 studies had a total of 128360 (study range: 4–53 906) participants, including 74 860 males, 53 500 females and 9862 athletes with non-specified gender. Studies were conducted across 41 different sports, of which the majority included athletes participating in swimming (12 studies), endurance running (13 studies), rugby (9 studies), soccer (8 studies), athletics (7 studies) and studies who included athletes practicing mixed endurance sports, such as runners, cyclists, triathletes or swimmers (10 studies), mixed Winter Olympic (7 studies) and Paralympic sports (5 studies), and mixed Summer Olympic (5 studies) and Paralympic sports (3 studies).
Number of studies by pathological and anatomical classification of ARill
The number of studies by pathological and anatomical classification, as well as the specific study references, are presented in table 2. Of all studies included in the meta-analysis, the majority (73%) reported on upper ARill. In addition, 86% of all studies investigated ARinf, of which most studies reported on upper ARinf (82/107=77%). With regards to the methods used to diagnose ARinf, most of the studies report suspected ARinf (104/107=97%), of which the majority used either self-reported symptoms with an algorithm (51/104=49%) or clinical diagnosis by a physician, based on history and examination (41/104=39%). In only three studies (3%) was ARinf confirmed by means of special investigations described above.
Number of studies and % (of all studies) by pathological and anatomical classification and method of diagnosis of ARill and ARinf
Incidence of any ARill
Across all studies, the estimated pooled overall incidence (per 1000 athlete days) of any ARill was 4.7 (95% CI 3.9 to 5.7).
Incidence of undiagnosed ARill
Across the studies the estimated pooled incidence of undiagnosed ARill (n=17) was 3.7 (95% CI 2.1 to 6.7). In all these studies, the specific cause of the ARill could not be determined and could include illnesses that are due to either infective or non-infective causes. In 8/17 (47%) of these studies the ARill was assessed by a physician (history and examination) and in 7/17 (41%) the ARill was classified using self-reported symptoms only. The sample size in this subgroup (n=17) was too small to conduct further analysis by level of performance, age group and season.
Incidence of ARinf
In studies reporting ARinf the incidence (per 1000 athlete days; 95% CIs) of ARinf by pathological and anatomical classification and by method of diagnosis is presented in table 3 (Forest plots are presented in online supplemental file 4).
Supplemental material
The incidence (per 1000 athlete days; 95% CI) of acute respiratory infection (ARinf) by pathological and anatomical classification and by method of diagnosis
Incidence of ARinf by pathological and anatomical classification and by method of diagnosis
Across all studies reporting ARinf, an incidence of 4.9 (95% CI 4.0 to 6.0) was found. For studies including upper ARinf, an incidence of 5.9 (95% CI 4.8 to 7.2) was found, while for studies that reported on general ARinf (upper or lower) the incidence was 2.8 (95% CI 1.8 to 4.5).
Subgroup analysis of suspected ARinf, which included most studies (79 studies), showed an incidence of 5.7 (95% CI 4.6 to 6.9). The three studies of confirmed ARinf showed an incidence of 18 (95% CI 5.7 to 56.8). The incidence was 2.8 (95% CI 2.1 to 3.8) if the diagnosis was made by a physician based on history and clinical examination only; and if the diagnosis was made based on self-reported symptoms utilising a checklist and algorithms, the incidence was 7.4 (95% CI 5.9 to 9.4). Furthermore, an incidence of 5.1 (95% CI 2.6 to 10.2) was found if the diagnosis was made using self-reported symptoms reviewed by a physician, yet without clinical examination.
Incidence of ARinf in subgroups by level of performance, age group and season
The incidence of ARinf for the further subgroup analyses are presented in table 4. A higher incidence of ARinf was found in non-elite athletes (8.7; 95% CI 6.1 to 12.5) than in elite athletes (4.2; 95% CI 3.3 to 5.3). The incidence of ARinf was similar in older athletes (>35 years) (9.1; 95% CI 5.2 to 16.0) and younger athletes (5.9; 95% CI 4.3 to 7.9). Across the studies that were conducted during summer, the incidence of ARinf was similar (3.5; 95% CI 2.5 to 4.9) to that during winter (5.8; 95% CI 4.6 to 7.8).
The incidence (per 1000 athlete days; 95% CI) of ARinf by age group, performance level, season and quality of study subcategories
Incidence of ARinf by quality assessment of studies
The incidence of ARinf was similar by quality assessment of studies as follows: excellent (4.9; 95% CI 3.9 to 6.3), good (6.3; 95% CI 4.7 to 8.6), fair (2.1; 95% CI 0.8 to 5.6) and poor (5.2; 95% CI 0.8 to 35.3).
Discussion
The aim of this systematic review and meta-analysis was to determine the overall incidence of ARill, including subgroups categorised by pathology (undiagnosed ARill vs ARinf and subgroups of ARinf), predominant anatomical region affected (upper vs unclassified upper/lower), different levels of athletic performance, age groups, season and quality of study. We also sought to determine outcomes in subgroups of ARill in athletes based on the method that was used for the diagnosis of ARill.
Incidence of ARill in athletes
The first main observation was that the estimated overall pooled incidence (per 1000 athlete days) of ARill in athletes was 4.7 (95% CI 3.9 to 5.7) and there was no significant difference in the incidence of undiagnosed ARill (3.7; 95% CI 2.1 to 6.7) vs all ARinf (suspected and confirmed) (4.9; 95% CI 4.0 to 6.0). The reasons why the incidence of undiagnosed ARill is similar to that of ARinf is likely because most ARill in athletes are due to infection and that non-infective ARill (eg, allergic rhinitis) is a predisposing factor for ARinf.61 Another explanation could be that studies that specifically investigated only known acute non-infective ARill, including acute asthma, allergies or cold air injury, were excluded. However, these reasons are speculative, and we encourage that a precise diagnosis of all ARill is reported in future studies.
Incidence of ARinf in subgroups by pathological classification
The incidence of suspected ARinf was not different by method of diagnosis. Earlier research showed that self-reported symptoms of ARill agree with physician-based diagnosis, suggesting that individuals are capable of adequately reporting symptoms.45 The practical application of these data is that sport and exercise medicine (SEM) physicians can confidently use validated questionnaires and checklists to screen athletes for suspected ARinf.42 These findings may have important considerations for choices around data collection methods in future large epidemiological studies. Research showed that patient-reported data can complement clinician-reported data to achieve more reliable measurements of clinical outcomes.62
Laboratory-based identification of a pathogen is the most accurate method for confirming the diagnosis of ARinf.42 The results of this analysis showed an apparent high incidence of confirmed ARinf (18; 95% CI 5.7 to 56.8). These data must be interpreted with caution because they are based on only three studies in which only two studies report very high incidences of confirmed ARinf (as visible in the forest plots, presented in online supplemental file 4). In one of these studies, there was a Streptococcal outbreak in 23 athletes over 15 days (IR of 40.6/1000 athlete days).63 In another study, seven clusters of different respiratory viral infections were recorded, with a ‘common cold’ in 44 athletes over 21 days, resulting in an IR of 26.7/1000 athlete days,64 which could have been caused by different risk factors such as the competition, international air travel and time difference.65 A large outbreak of infections from one pathogen in a small number of athletes is unusual and contrasts to the other study in this group.66
Pathogen identification is an important part of clinical practice42 and for the SEM physician this will allow for identification of more pathogens causing more serious ARinf. More serious ARinf may be associated with multiorgan involvement, higher risk of serious medical complications during exercise, and prolonged return to play (eg, for COVID-19).67 As a consequence of the COVID-19 pandemic, laboratory testing, such as PCR tests, might be more accessible, although we acknowledge that in some sports medicine settings laboratory testing may still not be feasible due to cost or inaccessibility. In these settings, our results confirm that a clinical diagnosis by a physician through history and physical examination, as well as use of self-reported symptoms using validated questionnaires or checklists or even symptom review by a physician without clinical or laboratory evaluation, can be used to diagnose ARinf.
Incidence of ARinf in subgroups by anatomical classification
For subgroups by anatomical classification, the incidence of upper ARinf was significantly higher than general (upper/lower) ARinf. This finding is not surprising and is in keeping with results from several studies reporting that upper ARinf is the most common non-injury related health problem in athletes and in the general primary care setting.68 Lower ARinf seem to be very rare in athletes. The incidence of ARinf in athletes was 4.9 (95% CI 4.0 to 6.0), and for upper ARinf was 5.9 (95% CI 4.8 to 7.2). This equates to an incidence of approximately 1.8 ARinf per athlete per year. In the general adult population, the incidence of ARinf is approximately 2–3 per person per year,69 70 yet it is unclear from the literature if the statistic in the general population is only upper ARinf or all ARinf. Thus, the annual incidence of ARinf in athletes appears similar or marginally lower than the general adult population. It is important to note that in most studies the incidence of ARinf in athletes has been reported over short observation periods (during a competition or in a season) and not over a 1-year period. These shorter observation periods are typically associated with the increased physical and emotional load associated with competition as well as international travel, all of which can increase the incidence of ARinf.71 72 Therefore, the true annual incidence of ARinf in athletes might be even lower. Based on the findings of this review, if a team physician is looking after the health of 100 athletes over a competition that lasts 3 weeks, it was estimated that medical teams will have to manage approximately 10 acute respiratory tract infections.
Incidence of ARinf in subgroups by level of athlete performance, age groups, seasons and quality assessment of studies
The incidence of ARinf in studies in elite athletes was significantly lower (4.2; 95% CI 3.3 to 5.3) compared with non-elite athletes (8.7; 95% CI 6.1 to 12.5). Although a higher training load is a general risk factor or for ARill (J-shaped curve),67 73 there are data to suggest that elite athletes, compared with non-elite athletes have a lower susceptibility to ARill (S-shaped curve).67 A further explanation could be that elite athletes have more access to a team physician and preventative support from allied health professionals, while non-elite athletes are less likely to have access to such medical support teams. Significant differences with respect to age of athlete and seasonal variation were not observed in this meta-analysis.
Although, the incidence of ARinf varied in subgroups by the quality assessment of the studies, this was not significantly different. As most studies were rated as either excellent or good (88%), the quality of the studies did not have a major influence on the overall incidence for ARinf.
Strengths and limitations
To our knowledge, this is the first systematic review to determine the incidence of ARill in athletes. We registered the review with PROSPERO and followed a systematic approach using an online tool, CADIMA. Furthermore, we developed a classification system, based on methods to differentiate between ARill and ARinf, and performed our subgroup analyses using a pathological and anatomical classification. This was important to address heterogeneity across studies in definitions and nomenclature of ARill, upper ARinf, and undiagnosed ARill. We believe this approach provides a more comprehensive clinical picture to inform clinical assessment and practice. This review has clinical importance and relevance given that ARill are the most common illnesses affecting athletes.
There are a number of limitations. A first possible limitation is that we excluded specific studies where only non-infective ARill, such as asthma, airway allergies or cold air injury to the airways were reported. These conditions are an important cause of respiratory symptomatology in athletes, which can be confused with ARinf.74 In our study, we grouped undiagnosed ARill as those where a study population with ARill could include infective or non-infective ARill. It is possible that some of these conditions might have been present in that group. It is for this reason that we analysed undiagnosed ARill as a specific subgroup and did not include these studies in the ARinf group. Therefore, a strength of this meta-analysis was that, in the subgroup analyses we focused on ARinf, therefore removing other non-infective causes of airway symptomatology as best as possible. We did not perform further analyses of subgroups (by level of athlete performance, age groups, seasons and quality assessment of studies) of the undiagnosed ARill group because the sample size of these studies was too small. Although not a limitation, this resulted in most of the review and meta-analysis focusing on ARinf.
Second, this review considered research published only in the English language, such that relevant studies conducted in non-English language were not included. We also excluded qualitative studies, reviews, commentary and discussion as well as case studies, which can be a rich source of information regarding the prevalence and incidence of ARill. Nevertheless, the broad search strategy utilised in this review ensured a degree of confidence that, within the inclusion criteria for incidence and/or prevalence of ARill from original studies were identified and appraised.
Third, the number of participants used to calculate the overall incidence could be biased or skewed, due to the high number of elite (Olympic/Paralympic) athletes in some of the studies.
Fourth, the incidence of less or more severe ARill or ARinf could not be determined in this systematic review. In most studies, severity of ARill was not reported as there is no consistent definition of severity of ARill.
Fifth, there was also a high degree of heterogeneity between studies. This was evident, as the I2 for all analyses was >90%, and therefore, the results should be interpreted with caution.
Finally, the number of studies included in some subgroup analyses was relatively small and this limits the interpretation of findings across subgroups. Specifically, the number of studies in which ARinf was confirmed by pathogen identification the sub-analysis was small (n=3) compared with the number of studies where ARinf was suspected (based on history and clinical examination) (n=44).
Summary and clinical implications
This systematic review and meta-analysis demonstrated that the overall incidence of ARill among athletes was 4.7 per 1000 athlete days (95% CI 3.9 to 5.7). The overall incidence of ARinf (suspected and confirmed) was 4.9 (95% CI 4.0 to 6.0) and similar to the incidence of ARill in studies reporting undiagnosed ARill (3.7; 95% CI 2.1 to 6.7). The highest incidence, by anatomical classification, was for upper ARinf at 5.9 (95% CI 4.8 to 7.2), which translates to approximately 1.8 ARinf per athlete per year. The incidence of ARinf in studies in elite athletes was significantly lower (4.2; 95% CI 3.3 to 5.3) compared with non-elite athletes (8.7; 95% CI 6.1 to 12.5). In the other subgroup analyses, there was no difference in the incidence of ARinf in subgroups by methods to diagnose ARinf, age groups, seasons or quality assessment of studies. We recommend the diagnosis of ARinf be based on physician clinical assessment, but include laboratory confirmation of the pathogen, if indicated and possible. Pathogen confirmation is the most definitive diagnostic method.42 In cases where laboratory testing is not feasible, we recommend using self-reported symptoms using validated questionnaires or checklists to diagnose ARinf. However, specific pathogen identification to refine the diagnosis of ARinf in athletes is likely to become more important in future. It is known that some pathogens that cause very mild ARinf with minimal risk of medical complications during exercise or interruption of training, while other pathogens (eg, SARS-CoV-2) can cause more severe disease, potentially with cardiac and other multi-organ involvement resulting in prolonged return to training.67 The classification system that has been published in this study may serve as an important and useful tool for physicians and researchers to distinguish between ARill and ARinf. We recommend that a clear diagnosis of ARill is reported in future studies.
What are the findings?
Acute respiratory illness (ARill) is the most common illness affecting athletes, and these are mostly acute respiratory infections (ARinf).
ARill can result in time loss from training and competition.
How might it impact on clinical practice in the future?
The overall incidence of ARinf in athletes is 4.9/1000 athlete days, which translates to approximately 1.8 ARinf per athlete per year.
Upper ARinf were the most common respiratory tract illnesses.
A higher incidence of ARinf was found in non-elite athletes than in elite athletes.
The incidence of ARinf is similar in older and younger athletes and across studies conducted in summer and winter.
The incidence of ARinf across different methods of diagnosis are similar.
In clinical practice the diagnosis of ARinf should be based on physician clinical assessment including laboratory confirmation of the pathogen where possible.
Self-reported symptoms using validated questionnaires or checklist could be used for screening of ARinf and in cases where physician diagnosis or laboratory testing is not feasible.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @wderman, @goipergormance, @sportsdocaus, @margo.mountjoy
Contributors WD, NS and MS conceived the study idea. MB, ME and LK completed the search. WD, MB, ME, JF, MG, LK, KM, MM and NS extracted and reviewed data from the studies included in the meta-analysis. NS performed the data analysis and data visualisation. All authors interpreted the data analysis, contributed to writing of the draft of the manuscript and approved the submitted version.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.