Article Text

Abstract
Objective Public life restrictions associated with the COVID-19 pandemic caused reductions in physical activity (PA) and decreases in mental and somatic health. Considering the interplay between these factors, we investigated the effects of digital home exercise (DHE) during government-enforced lockdowns.
Methods A multicentre randomised controlled trial was performed allocating healthy individuals from nine countries (N=763; 523 female) to a DHE or an inactive control group. During the 4-week main intervention, DHE members engaged in live-streamed multicomponent home exercise. Subsequently, both groups had access to prerecorded workouts for an additional 4 weeks. Outcomes, assessed weekly, included PA level (Nordic Physical Activity Questionnaire-Short), anxiety (Generalized Anxiety Disorder Scale-7), mental well-being (WHO-5 Questionnaire), sleep quality (Medical Outcome Study Sleep Scale), pain/disability (Chronic Pain Grade Scale) and exercise motivation (Self-Concordance Scale). Mixed models were used for analysis.
Results Live-streamed DHE consistently increased moderate PA (eg, week 1: 1.65 times more minutes per week, 95% CI 1.40 to 1.94) and vigorous PA (eg, week 1: 1.31 times more minutes per week, 95% CI 1.08 to 1.61), although the effects decreased over time. In addition, exercise motivation, sleep quality and anxiety were slightly improved for DHE in the 4-week live streaming period. The same applied to mental well-being (mean difference at week 4: +0.99, 95% CI 0.13 to 1.86), but an inverted trend was observed after live streaming was substituted by prerecorded exercise.
Conclusions Live-streamed DHE represents an efficacious method to enhance PA and selected markers of health during pandemic-related public life restrictions. However, research on implementation is warranted to reduce dropout rates.
Trial Registration number DRKS00021273.
- well-being
- COVID-19
- exercise
- preventive medicine
- randomised controlled trial
Data availability statement
Data are available upon reasonable request if permitted by the respective ethics vote.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
In March 2020, the WHO classified the global spread of the novel coronavirus (SARS-CoV-2) as a pandemic. To control the contagion, governments used a variety of strategies, inter alia including stay-at-home orders, social distancing, business closures and banning of mass events.1 Although related measures have proven effective in reducing viral transmission,1 restricted access to sports clubs, gyms and parks caused massive declines in physical activity (PA). According to a multinational survey with 13 503 participants from 14 countries, individual movement at both moderate and vigorous intensity decreased by more than 40% during lockdowns2 and the portion of individuals achieving recommended PA levels (ie, 150 min of moderate PA or 75 min of vigorous PA per week) dropped by 19%.2 These self-reported findings align with objectively measured data. Tison et al 3 analysed daily step counts measured with smartphone applications before and during the pandemic. One month after the WHO declaration, step counts (averaged for 187 countries) had decreased by more than a quarter.
Physical inactivity causes 8%–9% of all premature deaths4 5 and furthermore is associated with the occurrence of coronary heart disease and type 2 diabetes, as well as different forms of cancer.4 Being physically active, on the other hand, entails a myriad of somatic benefits, such as reducing mortality6 as well as decreasing the risk of musculoskeletal6 7 and non-communicable6 diseases. In addition to the general importance of PA in health, it seems to confer some protection against COVID-19.8 Sallis et al 9 analysed health data from 48 440 adults diagnosed with COVID-19. Inactive individuals had a higher risk of hospitalisation (OR 2.3), intensive care unit admission (OR 1.7) and death (OR 2.5) compared with persons meeting the PA guidelines.
Public life restrictions may also compromise mental well-being. According to survey data, the share of general population members meeting cut-off screening scores for depression tripled when compared with prerestriction periods.10 A systematic review of other self-reports, furthermore, identified high rates of stress (up to 82%), post-traumatic stress (up to 54%), anxiety (up to 51%) and psychological distress (up to 38%) in countries affected by COVID-19.11 Generally, regular PA is known to avert and improve anxiety and symptoms of depression12–14 while being significantly associated with positive affect and life satisfaction.15
In view of the paramount importance of movement for both somatic and mental health, researchers have called for the development of specifically tailored programmes aimed at maintaining PA during public life restrictions.16–20 Digital home exercise represents an opportunity to be physically active while still supporting viral containment efforts by means of social distancing. According to multinational data, 7 out of 10 persons would be willing to participate in related programmes.16 Against this background, the present study investigated the efficacy of a ‘virtual gym’ providing digital live-streamed home exercise on PA and markers of mental and somatic health during the COVID-19 pandemic.
Methods
Study design
This article reports data from the ‘Move ASAP’ (Activity and health during the SARS-CoV-2 Pandemic) project.21 A two-armed randomised controlled multicentre trial was performed in nine countries with active public life restrictions (Argentina, Austria, Brazil, Chile, Germany, Italy, Ireland, South Africa and Spain). In the main 4-week study phase, all involved centres assigned healthy adults to either a live-streamed digital home exercise group (DHE) or an inactive control group (CON). After the actual 4-week intervention, both groups had access to an online archive with prerecorded workouts for an additional 4 weeks. Proxies of somatic and mental health, as well as PA, were assessed using online questionnaires weekly. All enrolled individuals provided digital informed consent.
Public involvement
Feedback of target population members (healthy adults, see the Sample section) was used during the planning of the study. The formulation of the research question and the choice of assessed outcomes were based on previous surveys.2 10 The questionnaires used were additionally pilot-tested for clarity and comprehension by non-academic volunteers. With regard to the design of the intervention, we draw on reported preferences for DHE.16
Sample
Participants were recruited by means of online and newspaper advertising as well as via social media promotion. To verify the absence of contraindications to exercise, each participant completed the Physical Activity Readiness Questionnaire22 and only healthy adults without reported complaints were enrolled. Exclusion criteria encompassed severe orthopaedic, neurological, cardiovascular, metabolic, endocrine or psychiatric diseases, intake of drugs modifying pain perception, and pregnancy.
Randomisation
We used stratified (strata variable: centre) urn randomisation for group assignment.23 To allow concealed allocation and to prevent selection bias, randomisation was automatically performed by means of the software for survey delivery (Soscisurvey, Soscisurvey, Munich, Germany). In detail, after having completed the outcome assessments of the baseline questionnaire, the digital algorithm assigned the participants to the two groups, in the end generating balanced group sizes for each centre stratum.
Intervention
Individuals randomised to DHE participated in a 4-week tele-exercise programme provided via video live streaming (ie, synchronous approach). A ‘virtual gym’ schedule (example in online supplemental figure 1) was created, offering multicomponent workouts with different focuses, such as strength, endurance, flexibility, stability, balance, relaxation and cognition. The intensity of most sessions was moderate, although a few workouts also included vigorous exercise activities. Using camera and microphone, the instructors carefully monitored the participants, and if necessary provided advice regarding correct exercise execution or adjustments of training intensity. Participants could participate in the workouts ad libitum and without prior registration. While each country developed its own schedule depending on the availability of instructors (see also online supplemental table 1), the following criteria were uniform to ensure standardisation: training sessions were offered for a minimum of 5 days per week; individual workout durations ranged between 30 and 60 min; and instructors held, as a minimum requirement, a bachelor’s degree in sports science, movement science or a related discipline. Instructors received standardised training, modifiable demonstration workouts and a video archive containing a large pool of sample exercises. During the workouts, both the instructors and the participants could activate a camera and microphone to receive feedback on exercise execution, ask questions or interact with the group (online supplemental figure 2). The software used for video transmission (VidyoConnect, Vidyo, Hackensack, USA; Zoom, Zoom Video Communications, San Jose, California, USA; Skype, Microsoft Corporation, Redmond, USA; Microsoft Teams, Microsoft Corporation, Redmond, USA; BlackBoard, Blackboard, Washington, DC, USA) varied between centres, depending on local licensing and requirements thereof. The CON members did not receive an intervention and completed only outcome assessments (see the Outcomes section) during the main intervention period. However, to create an incentive for participation, members of both groups (DHE and CON) received unlimited access to an online archive with prerecorded workouts for an additional 4 weeks after the end of the main study phase.
Supplemental material
Supplemental material
Supplemental material
Outcomes
Blinded assessment of health markers and PA was performed each 7 days using digital questionnaires. The study thus had nine measurements: at baseline and weekly during the two 4-week part periods (T1–T8). The applied scales were selected based on psychometric validation and, where possible, the availability of translations and cross-cultural adaptations for each centre. Instruments employed included the Nordic Physical Activity Questionnaire-Short (NPAQ-Short24) for PA, WHO-5 Scale for Mental Well-Being,25 Generalized Anxiety Disorder Scale-7 (GAD-726) for impulsiveness and anxiety levels, the Medical Outcome Study (MOS) Sleep Scale (12-item version) for sleep quality,27 the Self-Concordance Scale (SKK)28 for exercise motivation, and the Chronic Pain Grade Scale (CPGS) for pain and disability levels.29 In addition to the intervention effects, adherence to exercise was checked by documenting attendance at each workout session offered.
Data processing and analysis
We performed an a priori sample size calculation using an algorithm to account for between-site variance in multicentre trials aimed to be analysed with linear mixed models.30 As a result, 544 participants had to be included in the present study (dropout rate: 20%, power: 80.3%, α=0.05, d=0.25). All analyses were performed using standard statistical software packages (eg, R and SPSS V.22). The two-sided significance level for all analyses was set to α=0.05.
We conducted three types of analysis in this study31 32: (1) intention-to-treat (ITT), which was the main analysis; (2) complier average causal effect (CACE); and (3) dose–response analysis. The ITT analysis was aimed at estimating the population average causal effect by considering the randomised allocation regardless of whether the participants in each group complied or not with their allocation condition (ie, intervention or control32 33). The CACE analysis was aimed at estimating the local average causal effect within the compliers. ‘Compliers’ were considered those randomly allocated to the DHE group who adhered to at least two workouts per week throughout the study and those randomly allocated to CON who did not receive the live-streamed DHE during the 4-week main period and who adhered to at least two workouts per week during the additional 4 weeks when access to an online archive with prerecorded workouts was granted. For each analysis and outcome, a three-level mixed model with restricted maximum likelihood estimation was implemented. Initially, a linear mixed model was fit. An exponential (log-linear) mixed model was considered in case of evidence for violations of assumptions, although linear mixed models are rather robust in regard to this.34 The results of the linear models were presented as mean difference (MD), while ratios of means (RoM) were presented for exponential models. Uncertainty around the average estimates was expressed as 95% CI.35 36
The fixed effect term of the mixed models was composed of dummy variables indicating the follow-up time points 1–8, and the interaction terms were composed of group and time (ie, ‘group × time’, where 0 is for CON and 1 is for DHE, and weeks 1–8). This strategy was implemented in order to adjust for possible differences between groups at baseline and in turn to correct the analyses for possible bias related to regression to the mean.37 Two random effect terms were included in the mixed models in order to adjust the analysis for centres and for repeated measurements: (1) a correlated random intercept and slope varying the intercept for the respective centres and varying the slope for the time points; and (2) a correlated random intercept and slope varying the intercept for the repeated measurements within each centre and varying the slope for the time points. Both random effect terms were assumed to follow a multivariate normal distribution with the following hyperparameters: a k-dimensional mean vector composed of zeros and a ‘k × k’ covariance matrix composed of random intercept, slope and intercept–slope covariances. The models were adjusted for the following observed prognostic variables at baseline that could possibly affect missing outcome data in our data set: age, sex, living environment, employment and university degree.
We used instrumental variable (IV) analysis to estimate CACE. The IV was considered the randomised allocation assignment. We assumed the exclusion restriction and monotonicity assumptions for the IV analysis.31 32 38 The IV analysis was conducted in two stages. In stage 1, we regressed a binary variable indicating the compliers on the IV using a logistic mixed model. Time and the interaction term composed of the IV and time were also included in the fixed effect term of the model. From this model, we estimated the predicted probabilities of performing at least two workouts per week for each participant. In stage 2, CACE was estimated using mixed models regressing the outcomes of the study on the predicted probabilities estimated in stage 1. The random terms and the prognostic variables at baseline previously described were also included in stage 1 and 2 models.
A dose–response relationship analysis was performed using mixed models to investigate the influence of exercise dose (adherence) on the possible effects of the DHE programme. The dose–response models were adjusted for age, sex, living environment, employment, university degree and study part (ie, part 1: first 4 weeks; part 2: last 4 weeks). The random effect terms were the same as previously described.
Results
A total of 763 individuals volunteered to participate (online supplemental figure 3). Both groups (CON: n=377, DHE: n=386) were comparable with regard to age, sex, educational level, living environment and employment status (table 1). The main 4-week study part (live-streamed DHE vs CON) was completed by 350 participants, corresponding to a dropout rate of 54%. Slightly more dropouts were recorded in the CON (CON: 57% vs DHE: 51%). From the 350 participants, 228 finished the second 4-week study part (prerecorded workouts), which further increased the total dropout to 70% (CON: 71% vs DHE: 68%) at the end of the 8-week period. No adverse or serious adverse events were reported.
Supplemental material
Sample characteristics at baseline
The evaluation of the linear mixed model assumptions revealed violations in the models including the following five outcome variables: GAD-7, NPAQ (moderate PA), NPAQ (vigorous PA), CPGS (pain) and CPGS (disability). Therefore, exponential (log-linear) mixed models were implemented for these five outcome variables. Linear mixed models were implemented for the remaining three outcome variables: exercise motivation (SKK), sleep quality (MOS) and WHO-5 Scale for Mental Well-Being.
ITT analysis
Overall, the ITT analysis (table 2) revealed small to moderate MDs or RoMs for DHE versus CON (figures 1–4). DHE consistently increased moderate PA (eg, week 1: 1.65 times more minutes per week, 95% CI 1.40 to 1.94) and vigorous PA (eg, week 1: 1.31 times more minutes per week, 95% CI 1.08 to 1.61) during the main study part using live streaming (figure 1). These effects, however, became smaller over time and comparisons did no longer include the null value after replacing live exercise by prerecorded workouts (now offered in both groups).

Differences between the control and digital home exercise group in moderate (left) and vigorous (right) physical activity. The figure shows the ratios of means and 95% CI.

Differences between the control and digital home exercise group in well-being (left) and anxiety (right). The figure shows adjusted means (WHO-5) or ratios of means (GAD-7) and 95% CI. GAD-7, Generalized Anxiety Disorder Scale-7; WHO-5, WHO-5 Questionnaire.
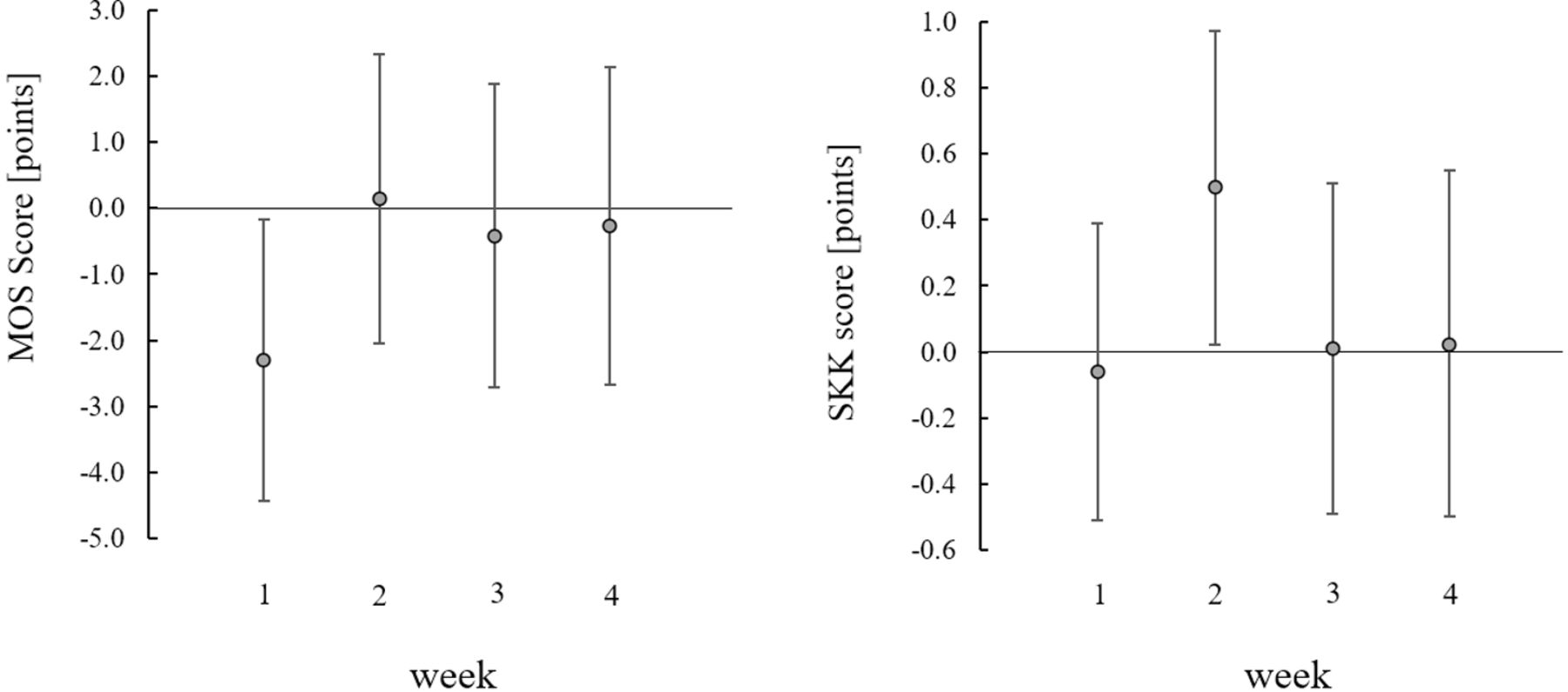
Differences between the control and digital home exercise group in sleep quality (left) and exercise motivation (right). The figure shows adjusted means and 95% CI. MOS, Medical Outcome Study; SKK, Self-Concordance Scale.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Differences between the control and digital home exercise group in pain (left) and disability (right). The figure shows ratios of means and 95% CI. CPGS, Chronic Pain Grade Scale.
Results of the causal effects (efficacy) analyses
Although with lower consistence, mental well-being (WHO-5) was slightly higher for DHE during the live streaming period (ie, week 4: MD 0.99, 95% CI 0.13 to 1.86) and showed an inverted (ie, lower compared with CON) trend during the additional 4 weeks when live streaming was interrupted and both groups had access to prerecorded workouts (figure 2). However, the 95% CI of the group comparisons contained the null value during these additional 4 weeks. Also, sleep problems (MOS) were initially reduced for the DHE group (week 1: MD −2.30, 95% CI −4.43 to −0.17; figure 3). Similarly, in week 2, anxiety was lower (RoM 0.87, 95% CI 0.77 to 0.98; figure 2) and exercise motivation was higher (MD 0.50, 95% CI 0.02 to 0.97; figure 3) for the DHE group compared with CON.
CACE analysis
The results of the CACE analysis (table 2) were largely similar to the ITT results. However, the uncertainty around the CACE estimates was higher with wider 95% CIs and more frequent inclusions of the null value. Only two exceptions were found: sleep problems (MOS) were higher for the DHE group at the end of the prerecorded workout phase (week 8: MD 7.69, 95% CI 1.30 to 14.08) and pain (CPGS) was up to 1.48 times higher (95% CI 1.10 to 2.01) for the DHE group during the 4-week live-streamed period compared with CON.
Dose–response analysis
The number of workout participations per week did not affect exercise motivation (SKK), sleep quality (MOS), anxiety (GAD-7), pain intensity and pain-related disability (CPGS). However, the exercise dose was predictive of changes in mental well-being (a 1-point increase in workout participation per week was associated with a 0.10 absolute increase in WHO-5 Scale; 95% CI 0.02 to 0.18), moderate PA (a 1-point increase in workout participation per week was associated with 1.07 times higher minutes of moderate PA per week; 95% CI 1.05 to 1.08) and vigorous PA (a 1-point increase in workout participation per week was associated with 1.04 times higher minutes of vigorous PA per week; 95% CI 1.02 to 1.06).
Discussion
Public life restrictions instituted during the COVID-19 pandemic substantially reduced the opportunities to engage in health-enhancing PA2 3 and there have been several calls to action requesting the development of novel ways to exercise.39 40 To the best of our knowledge, the present multicentre trial with participants from nine countries and four continents was the first to examine the effects of live-streamed home exercise conforming to the demand for social distancing.
From a population average causal effect perspective (ie, ITT), two key findings were made. First, DHE substantively enhanced PA, with population means markedly and consistently exceeding the WHO recommendation of at least 150 min of moderate PA or 75 min of vigorous PA per week. This is of particular importance because the worldwide confinements caused an almost 20% drop in PA guideline compliance2 and because sufficient activity is not only related to reduced mortality in general but also to a lower risk of hospitalisation, intensive care unit admission and death due to COVID-19.9 Second, live-streamed DHE had small beneficial effects on mental well-being, anxiety, sleep quality and exercise motivation. The positive impact of DHE on well-being was initially observed during all 4 weeks of the main intervention part. However, interestingly, this effect was not sustained during the subsequent 4 weeks, when the live streaming was interrupted and prerecorded workouts were available to both groups. This finding may be explained by the fact that the formerly inactive control group now received an intervention too and because the prerecorded workouts could have been less attractive to the DHE group.
Since the sample of our study was composed of healthy individuals, we did not expect large effects on physical and mental health indicators. However, even small changes as those observed could be relevant for several reasons. Effect sizes of previously tested interventions aiming to improve markers of mental well-being were small or moderate at best,41–44 meaning that our intervention performed at least similar. Additionally, exercise was offered during a pandemic with concomitant restrictions to public life. As these may be expected to adversely affect health, maintaining the status quo could already be seen as a success. Finally, if achieved changes, even if small, could be maintained over time, they could still result in an increased quality of life and/or cumulative and latent preventive effects regarding undesired health conditions. DHE, executed regularly, could thus be a promising option to protect health both during and in the absence of a pandemic. The challenge, however, would be to maintain adherence to tele-exercise as our study showed that the effects (ie, on mental well-being) ceased with the switch from live-streamed to prerecorded exercise.
Our CACE (ie, local average causal effect) analysis of the DHE programme was consistent with the ITT results, although the uncertainty around the estimates was higher. Of note, the DHE participants reported higher pain (CPGS) levels especially during the first 4-week period of live-streamed exercise intervention, although they did not report adverse events. Two non-mutually exclusive explanations are plausible. First, CPGS pain was higher in DHE than in CON at baseline. Although group allocation was randomised preventing selection bias, randomisation does not guarantee that groups are equivalent at baseline.33 This is why we adjusted the analyses for possible between-group differences at baseline. Second, there is an increased probability of delayed onset muscle soreness (DOMS) in individuals who increase exercise levels or those who initiate the practice of a new exercise type or regimen, and pain is one of the most common symptoms of DOMS.45 46
Prior to study initiation, in a very similar sample, we found that more than two-thirds of the respondents were ready to engage in DHE.16 This and the fact that individuals complying with the live-streamed exercise programme achieved potentially relevant improvements in PA levels and mental well-being are promising. However, despite meeting our predetermined sample size at baseline, only 46% (main study, part 1) or 30% respectively (unlimited database access, part 2) of the participants completed the study and a considerable share completed the questionnaires without attending workouts. Due to the substantial missing outcome data and possible violations of the ‘missing at random’ assumption of mixed models, the main ITT analyses in this study may be considered pseudo-ITT restricted to participants with complete data, although we adjusted the analyses for possible prognostic factors at baseline that could possibly affect missing data in our study.38
Dropout is a general problem in many longitudinal trials involving exercise interventions. Pooling data from 37 studies in patients with cancer, Czosnek et al 47 reported a mean attrition rate of 38% with a range of 22%–56%. Joseph et al 48 systematically reviewed internet-based PA interventions, reporting a mean attrition rate of 22.3% with a range between 0% and 69%. Comparing these data with our trial, it needs to be acknowledged that our dropout rate is rather at the upper margin. Three issues may particularly explain this finding. First, to obtain as much data as possible despite the rapidly changing situation related to the pandemic (eg, end of local restrictions and subsequent dropouts before terminal outcome measurements), we used weekly questionnaires. Possibly, this rather high frequency represented an obstacle for a share of the sample. Second, we removed participants from the study as soon as they did not complete the weekly assessments. However, some individuals who failed to answer the questionnaires initially may have continued to participate in the study later, if they would have been allowed to. Third, the duration and severity of public life restrictions varied, depending on many factors, inter alia local incidence, mortality and intensive care availability. While restrictions were still in place in all countries during the study, local relaxing of some measures (eg, partial opening of gyms) could have prompted participants to drop out. Irrespective, our study reinforces the importance of successful implementation. It is known that exercising in a group,49 being supervised by a healthcare professional50 and having a choice of contents51 represent important features ensuring adherence to exercise interventions. Using a virtual gym schedule and the live streaming format helped to satisfy these needs. Future studies, however, should aim to identify other decisive barriers and facilitators for participation.
As mentioned, the participants of our study were classified as healthy. Compelling evidence shows that, even in this group, mental and physical well-being were substantially decreased during social restrictions.10 The development of newly tailored interventions is hence paramount to prevent long-term increases of disease prevalence in most of the population. Notwithstanding, no assumptions can be made as to how the investigated exercise programme can be of help to individuals with chronic diseases. As PA and sports may improve not only general health parameters such as well-being, but also disease-specific outcomes (eg, insulin sensitivity in persons with diabetes), patients may be substantially more affected by the pandemic. It would therefore be intriguing to elucidate the potential as well as the risks of live-streamed exercise in related populations.
Conclusions
Live-streamed DHE is efficacious in consistently enhancing PA and, to a smaller degree, in improving mental well-being, anxiety, sleep quality and exercise motivation during pandemic-related public life restrictions. A dose–response relationship seems to exist, with a higher number of workouts per week being predictive of increases in mental well-being and PA levels. However, observed dropout rates, reaching about 50% after the 4-week main intervention, are worrisome. Future research should hence be geared towards refining and enhancing implementation.
What is already known on this topic?
Public life restrictions issued to contain the COVID-19 pandemic have caused significant reductions in physical activity levels and mental well-being.
What are the findings?
Live-streamed digital home exercise (DHE) increases physical activity and, to a minor degree, improves mental well-being, anxiety, sleep quality and exercise motivation.
The use of prerecorded workouts may not be associated with such health benefits.
Dropout proportion in DHE is high, making it a challenge for implementation.
How might it impact on clinical practice in the future?
If barriers to participation are reduced, live-streamed DHE can help counteract the mental and somatic adverse effects of social distancing and stay-at-home regulations during a pandemic.
Data availability statement
Data are available upon reasonable request if permitted by the respective ethics vote.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of the Faculty of Psychology and Sports Sciences of Goethe University Frankfurt (protocol no 2020-25); Ethics Committee of Karl Franzens University Graz (no 39/66/63 ex 2019/20); Comitato di Ateneo per la Ricerca, Università degli Studi di Roma "Foro Italico" (no CAR 45/2020); Research Ethics Committee of the Universidade Cidade de São Paulo (no 31216720.2.000.0064); Institutional Research Ethics Committee of Durban University of Technology (no IREC 090/20); Institutional Ethics Committee of the University of Santiago of Chile (no 207/2020); Research Ethics Committee of Fundación Instituto Superior de Ciencias de la Salud (no DEPINV12/20); Research Ethics Committee of Waterford Institute of Technology (no WIT2020REC100); and Ethics Committee of Universidad Politécnica de Madrid. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Chiara Fossati (Italian study centre) and Mireille van Poppel (Austrian study centre) provided valuable administrative support. Furthermore, the authors thank Patricia Sheehan and Annalouise Muldoon (Ireland), Lisandra Almeida, Rafael Olivera and Henrique Martins Ungri (Brazil), Jose Daniel Jiménez-García (Spain), and Marie Wilke and Leander Sielaff (Germany) for their assistance in conducting the exercise sessions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ItsJanWilke, @David Jimenez-Pavón, @fernandoalainio, @LucaHespanhol
Correction notice This article has been corrected since it published Online First. The results section of the abstract has been revised for clarity.
Contributors JW: concept/design, data collection, data analysis, manuscript draft, critical revision. LM, LH: data collection, data analysis, critical revision. AKB, DJ-P, FL, NM, BN, SN, SO-G, JP, FR, LR, CS, DU, LV: data collection, critical revision. Guarantor: JW
Funding LH received Young Investigator Grant from the Sao Paulo Research Foundation (FAPESP; grant 2016/09220-1). GY received a grant from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. Support from the Biomedical Research Networking Center on Frailty and Healthy Aging (CIBERFES) and FEDER funds from the European Union (CB16/10/00477) was provided.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.