Article Text

Abstract
Objectives The aim of this study was to examine the effectiveness of an enhanced online injury prevention programme on the number of running-related injuries (RRIs) in recreational runners.
Methods We conducted a randomised-controlled trial in runners who registered for running events (distances: 10–42.195 km) in the Netherlands. Adult runners who provided informed consent were randomised into the intervention or control group. Participants in the intervention group received access to the online prevention programme, which included items to prevent RRIs. Participants in the control group followed their regular preparation for the running event. The primary outcome measure was the number of new RRIs from baseline to 1 month after the running event. To determine differences between injury proportions, univariate and multivariate logistic regression analyses were performed.
Results This study included 4050 recreational runners (63.5% males; mean (SD) age: 42.3 (12.1) years) for analyses. During follow-up, 35.5% (95% CI: 33.5 to 37.6) of the participants in the intervention group sustained a new RRI compared with 35.4% (95% CI: 33.3 to 37.5) of the participants in the control group, with no between-group difference (OR: 1.03; 95% CI: 0.90 to 1.17). There was a positive association between the number of items followed in the injury prevention programme and the number of RRIs (OR: 1.05; 95% CI: 1.00 to 1.11).
Conclusion The enhanced online injury prevention programme had no effect on the number of RRIs in recreational runners, and being compliant with the programme paradoxically was associated with a slightly higher injury rate. Future studies should focus on individual targeted prevention with emphasis on the timing and application of preventive measures.
Trial registration number NL7694.
- sporting injuries
- running
- athletes
- preventive medicine
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Running is a popular form of physical activity: it is easy to perform, easily accessible and has a range of health-related benefits.1–3 Unfortunately, running can also be associated with a high number of running-related injuries (RRIs) with a prevalence between 10% and 92%.4–6 This large range is likely due to a lack of consistency in defining an injury, heterogeneity of studied running populations and variable exposure times.4
As first steps towards prevention of RRIs, risk factors have been assessed in multiple studies. These studies identified several risk factors, including a previous RRI, no previous running experience, higher body mass index, higher age and a high weekly running distance.7–9 The large variety of risk factors indicates that the cause of RRIs is multifactorial.10 However, most prevention studies focused on modifying one single risk factor for RRIs, for example no previous running experience and increasing training load too fast.11 12 These studies found no effect on the number of RRIs, which may be due to the fact that they targeted only one single risk factor. In addition, literature shows that runners’ assumptions on RRI prevention is not supported by scientific evidence which demonstrates the need to inform runners on known risk factors.13 14 In 2017, we designed the INtervention Study on Prevention of Injuries in Runners at Erasmus MC (INSPIRE) trial, a randomised-controlled trial (RCT) in which the effect of a multifactorial online injury prevention programme on the number of RRIs was investigated.15 This programme did not decrease the number of RRIs in recreational runners. However, new insights were gained to enhance injury prevention in runners, including runners’ opinions, barriers and facilitators of injury prevention.16 17 We found indications that the prevention programme even increased the number of new RRIs in runners with no previous RRI.17 Therefore, we concluded that research on RRI prevention should target runners who previously reported injuries, because these runners seem to be more motivated to perform preventive measures than runners with no history of RRIs.16 Furthermore, runners reported that a website and application were the most preferred routes of information delivery. Last, participants indicated that ‘not knowing what to do’ was an important barrier for injury prevention.16 As shown by Hesphanol et al in trail runners, online tailored advice may have the potential to prevent RRIs.18 Specific potential educational content was earlier suggested by Murray et al and Blagrove et al in terms of registration and monitoring of weekly training load and the integration of running-specific strengthening exercises in training schedules.19 20 Runners clearly prefer practical and straight instructions with the use of animations and interactive tools, which can be integrated into their training sessions with great ease.
Therefore, we designed an enhanced online injury prevention programme entitled ‘10 steps 2 outrun injuries’. The aim of this study was to examine the effectiveness of this prevention programme on the number of RRIs in recreational runners.
Methods
Study design
The Shaping up Prevention of Running Injuries in the Netherlands using Ten steps (SPRINT) study is an RCT in recreational runners with a minimum follow-up of 3 months. A detailed study protocol of the SPRINT study has been published elsewhere.21 This study was funded by the Netherlands Organisation for Health Research and Development (ZonMW, grant number 50-53600-98-104) and was performed in collaboration with the Rotterdam Marathon Study Group of Golazo Sports, the organiser of large running events in the Netherlands.
Participants
Runners who registered for the DSW Bruggenloop Rotterdam 2019 (15 km), Nacht van Groningen 2020 (10, 16.1 and 21.1 km), NN CPC Loop The Hague 2020 (10 and 21.1 km) or NN Marathon Rotterdam 2020 (10.55 and 42.195 km) were asked to participate in this study through a question on the online registration form. Interested runners who met the inclusion criteria (18 years or older, registration at least 2 months before the running event, sufficient knowledge of the Dutch language, access to internet and email and no participation in the previous INSPIRE trial) received more information about the SPRINT study by email. If they were still interested, participants were asked to provide digital informed consent and complete the baseline questionnaire. For runners who registered for multiple selected running events only the first registration was taken into account.
Randomisation and follow-up
After completing the baseline questionnaire, participants were randomised into either the intervention or control group, using a computer-generated randomisation list (Microsoft Access) with block sizes of 40. The allocation was concealed, as the randomisation table was generated by an individual from outside the research group and was not accessible for the research team during the inclusion and data collection. The participants were informed on the outcome of the randomisation by a member of the research team. Participants in the intervention group received a personal login code to the website that included the prevention programme, to which they had unlimited access. Moreover, a Web App version was made available. Participants in the control group followed their regular preparation for the running event. During follow-up, all participants received three follow-up questionnaires to inform on new RRIs in the time frame between the last questionnaire and current questionnaire: 1 month and 1 week before the running event, and 1 month after the running event. In addition, all participants received every two weeks a newsletter with updates on the SPRINT study and a hyperlink to an online injury questionnaire with the question to actively register any new RRI. The newsletters for the intervention group additionally highlighted one of the items of the prevention programme.
The ‘10 steps 2 outrun injuries’ prevention programme
The prevention programme was based on literature, the expertise of clinicians and researchers and the results and knowledge gained through the INSPIRE trial.15–17 This programme included 10 items with specific advice and tools to prevent RRIs (online supplemental appendix A). More detailed information about the items can be found elsewhere.21
Supplemental material
Measurements
Items of the four sections (demographics, training, running events and previous RRI) collected through the baseline questionnaire are presented in online supplemental appendix B. Information on new RRIs was obtained with the follow-up questionnaires and the biweekly injury questionnaires (online supplemental appendix B).
Outcome measures
The primary outcome measure of this study is the difference in injury proportion between the intervention and control group from baseline to 1 month after the running event, based on participants with at least one new injury reported in the follow-up questionnaires and the injury questionnaires filled-in through the biweekly newsletters. An RRI was defined as a self-reported injury of the muscles, joints, tendons and/or bones in the lower back or lower extremities (hip, groin, thigh, knee, leg, ankle, foot and toes) that is caused by running (training or competition). The injury had to be severe enough to cause a reduction in running distance, speed, duration or frequency for at least seven days or three consecutive scheduled training sessions or the consultation of a physician or other health professional had to be necessary.22
Secondary outcome measures included the clustered injury location, severity of RRIs based on the OSTRC Overuse Injury Questionnaire, and medical consumption.
Sample size
Based on the INSPIRE trial, an injury incidence of 38% was expected in recreational runners who register for a running event (distance: 10–42.195 km) at least 2 months before the running event until 1 month after the running event.17 Since the prevention programme was focused on runners with a previous RRI, the sample size calculation was based on the subgroup analysis of runners with a previous RRI. With a risk difference of 5%, 0.05 significance level (two-sided testing and a power of 80%), a minimum of 1414 runners with a previous RRI had to be included in the analyses to detect a relevant difference in RRIs. Since the INSPIRE trial reported that 52.1% of the participants sustained a previous RRI, the sample size was doubled in order to obtain enough power for the primary analyses in the entire study population.15 Taking a loss to follow-up of 20% into account, at least 3394 runners had to be included in this study.
Statistical analyses
Descriptive statistics were used to describe all variables, expressed in frequency or mean and SDs. Participants in the intervention and control group were compared with independent sample t tests (continuous data), Mann-Whitney U tests (continuous data) and χ2 tests (dichotomous data). Consistent with the Consolidated Standards of Reporting Trials (CONSORT) statement, an intention-to-treat analysis was performed.23 Injury proportions with 95% CIs were calculated for all participants and for the intervention and control group separately, for which a difference in injury proportion was calculated. To correct for errors, we checked whether participants who reported an RRI filled in an RRI on the same location in the previous questionnaire. If not, the RRI was interpreted as a new RRI. If they did, this RRI was not regarded as a new RRI. Additionally, ORs with 95% CI were calculated using univariate logistic regression analysis. Potential confounders (age, body mass index (BMI) and previous RRI) and baseline characteristics with a significant difference between the intervention and control group were added one by one to the univariate regression model. If a potential confounder altered the unadjusted estimate effect by 10% or more, this confounder was added to the multivariate logistic regression model to calculate adjusted ORs and to the generalised linear models to calculate adjusted risk ratios. Predefined subgroup analyses were performed for distance of running event, sex, running experience (≤1 year/>1 year), previous RRI and reported RRI at baseline. Moreover, between-group differences in the clustered injury locations (lower back, hip/groin, upper leg/knee, lower leg (shin/calf/Achilles tendon/ankle), and foot/toe) were analysed. Based on the request of peer reviewers, we made a minor protocol deviation in the predefined subgroup analysis; we calculated the injury proportion and adjusted ORs for participants without an RRI at baseline. With the OSTRC Overuse Injury Questionnaire, the OSTRC severity score (0–100) of new RRIs was calculated and every new RRI was categorised into a substantial overuse injury (yes/no).24 Next, between-group differences in OSTRC severity score, substantial overuse injury, pain score (Numeric Rating Scale (0–10)), use of painkillers and/or non-steroidal anti-inflammatory drugs (NSAIDs), and medical attention were calculated. A sensitivity analysis was performed to compare the injury proportion of participants in the intervention group who were compliant with the prevention programme with the injury proportion of the control group. Participants were regarded compliant if they reported that they applied at least one item from the prevention programme to their training sessions. Last, an explorative additional analysis on the number of used items in relation to the injury risk was performed using univariate logistic regression analyses. All analyses were performed in SPPS Statistics V.25 and p values <0.05 were regarded as statistically significant. Missing data were not imputed and analyses were based on complete data.
Results
Participants
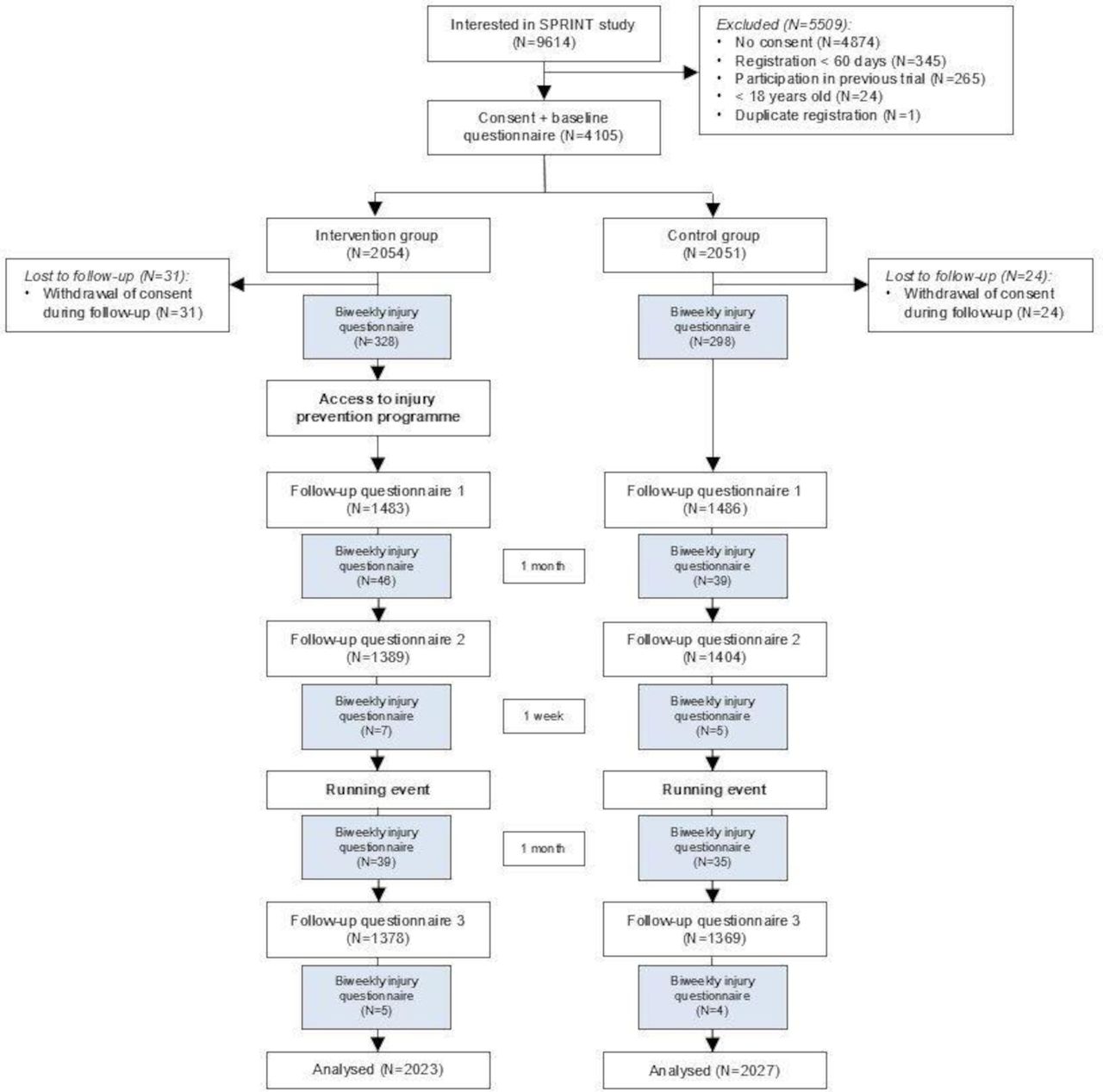
After registration for one of the selected running events, 9614 runners were interested in participation in the SPRINT study (figure 1). Of these, 4105 participants were included and randomised into either the intervention group (n=2054) or control group (n=2051). During follow-up, 55 participants were lost due to withdrawal of consent. A total of 2023 participants in the intervention group and 2027 participants in the control group were included for analyses. Compared with participants in the control group, participants in the intervention group were at baseline on average (SD) older (42.8 (12.4) vs 41.7 (11.9), p=0.01) and had a higher BMI (23.4 (SD: 2.6) vs 23.2 (SD: 2.6) p=0.01) (table 1). A total of 2000 (49.4%) participants reported a previous RRI in the last 12 months. Compared with participants in the control group, participants in the intervention group reported less RRIs at baseline (17.4% vs 20.3%, p=0.02).

Flowchart of the SPRINT study. SPRINT, Shaping up Prevention of Running Injuries in the Netherlands using Ten steps.
Baseline characteristics of the study population
Follow-up questionnaires
The mean follow-up duration was 5.0 (range: 3.0–7.8) months, with no between-group difference. A total of 3312 (81.8%) participants completed at least one of the follow-up questionnaires, while 2329 (57.5%) participants completed all follow-up questionnaires. Participants who did not complete any of the follow-up questionnaires were on average (SD) younger (37.8 (10.7) vs 43.3 (12.2), p<0.001), had less running experience (8.0 (8.6) vs 10.8 (10.3) years, p<0.001) and participated less often in a previous running event (89.8% vs 94.4%, p<0.001) compared with participants who completed at least one follow-up questionnaire (online supplemental appendix C).
Primary outcome measure
During follow-up, 1436 participants (35.5%, 95% CI: 34.0 to 36.9) sustained a new RRI, with a total of 2245 new injuries (1131 RRIs in the control group and 1114 RRIs in the intervention group) (table 2). The injury proportion for the intervention group was 35.5% (95% CI: 33.5 to 37.6) and for the control group 35.4% (95% CI: 33.3 to 37.5), with no differences between groups (adjusted OR: 1.03, 95% CI: 0.90 to 1.17).
Total number of injuries and per clustered injury location with differences between the intervention group and control group (n=4050)
Subgroup analyses and secondary outcome measures
In all participants, the most reported injured location was the knee (11.0% in the control group and 10.4% in the intervention group) (figure 2). There were no significant differences in the clustered injury locations between the intervention and control group (table 2). Subgroup analyses performed for the distance of running event registered for, sex, running experience, previous RRI, and reported RRI at baseline showed no significant differences in injury proportions between the intervention and control group either (table 3). In participants without an RRI at baseline, the injury proportion was 33.1% (95% CI: 30.8 to 35.3) in the intervention group and 32.6% (95% CI: 30.3 to 34.9) in the control group, with no differences between groups (adjusted OR: 1.03, 95% CI: 0.89 to 1.20) (online supplemental appendix D).

{kind=link}
{kind=link}
Number of injured runners per anatomical side. * statistically significant difference between intervention and control group (p<0.05).
Subgroup analyses of injury proportions for the intervention and control group
Data on RRI severity on 13 of the 2245 reported new RRIs were missing due to a questionnaire error. The OSTRC severity score was on average 53.2 (SD: 26.1) for all participants, with no difference between the intervention and control group (53.2 (SD: 25.9) vs 53.2 (SD: 26.4)). A total of 1441 (64.6%) RRIs were classified as a substantial overuse injury, with a significant difference between the intervention and control group (747 (66.6%) vs 694 (62.5%), p<0.05). Of the participants (n=1250) who reported a new RRI in the follow-up questionnaires, 198 (15.8%) participants used painkillers and/or NSAIDs and 548 (43.8%) participants received medical attention (table 4).
Severity and medical consumption of new RRIs reported in the follow-up questionnaires
Sensitivity analysis
Of the participants in the intervention group who completed the last follow-up questionnaire (n=1378), 922 (66.9%) participants reported that they read at least one item of the injury prevention programme, of whom 491 (53.3%) participants read at least five items and 256 (27.8%) participants read all 10 items. A total of 680 (49.3%) participants reported that they applied at least one item to their training sessions and were therefore compliant with the prevention programme. The most applied items were ‘take enough time for rest and recovery’ (n=351, 51.6%), ‘make sure there is variety in movement using specific exercises’ (n=343, 50.4%) and ‘do not train too much’ (n=333, 49.0%). The injury proportion of the participants in the intervention group who were compliant was 44.0% (95% CI: 40.2 to 47.7) compared with 35.4% (95% CI: 33.3 to 37.5) of the participants in the control group. Furthermore, there was a positive association between the number of items applied and the number of RRIs (OR: 1.05; 95% CI: 1.00 to 1.11)).
Discussion
The aim of this study was to investigate the effect of a specifically designed injury prevention programme on the number of RRIs in recreational runners. This enhanced online injury prevention programme did not decrease the number of RRIs. Neither were there any differences in the number of RRIs in any of the investigated subgroups of runners. Compliance with the injury prevention programme had a negative effect on injury proportion. Of the new RRIs, almost two third were classified as a substantial overuse injury and almost half of the participants with a new RRI needed medical attention.
The injury prevention programme did not decrease the overall number of RRIs in runners. Notably, we found that being compliant (applied at least one item) with the injury prevention programme negatively affected the injury proportion. Similar results were found in participants who applied at least five items of the intervention programme (injury proportion 47.9%, 95% CI: 40.8 to 55.1). Moreover, there was a positive association between the number of items applied and the number of RRIs. The negative effect of compliance might be due to the timing of applying the prevention programme: the prevention programme may have been initiated as a result of an RRI (tertiary prevention) and not proactively to prevent an RRI. Due to the design of this study, we were not able to determine the time frame between the occurrence of the RRI and the use of the programme. Furthermore, only 49.3% of the participants in the intervention group were complaint to the prevention programme which was only slightly higher compared with the INSPIRE trial (44.1%). Perhaps, more targeted educational interventions, as argued by Nielsen et al and Hespahanol et al may increase compliance.18 25 So future studies should focus on how to improve compliance and the timing and application of prevention programmes.
In step six of the prevention programme, runners were advised to stop running or adapt their training when they experienced discomfort or mild pain during running as this can be the first sign of an RRI. As a consequence, this may have interfered with the primary study outcome, since a reduction in running for more than seven days or three consecutive training sessions was considered as an injury according to our definition of an RRI. Of the 680 participants who were compliant to the prevention programme, 231 (34.0%) participants applied the information from step six in their training sessions. In these participants, the injury proportion was 56.3% (95% CI: 49.8 to 62.7). Given this high proportion, we analysed the injury proportion for participants in the intervention group who did not apply step six to their training sessions (n=1792), resulting in an overall injury proportion of 32.9% (95% CI: 30.7 to 35.1). As this injury proportion was 2.6% lower compared with the injury proportion of all participants in the intervention group, the impact of the advice of step six on the number of reported RRIs seemed relatively high. Furthermore, we expected that participants who applied step six to their training sessions reported less substantial overuse injuries. However, significantly more RRIs of the participants in the intervention group were classified as a substantial overuse injury compared with the RRIs of the participants in the control group (747 (66.6%) vs 694 (62.5%), p=0.05).
Because the INSPIRE trial indicated that running prevention advices should be directive and personalised, we aimed to make items more actionable (eg, if your step frequency is low, gradually build up your step frequency) and included animations, videos and interactive tools in the new prevention programme (online supplemental appendix A). Moreover, we removed the information on forefoot strike as this seemed to have a negative impact on the occurrence of lower limb injuries.17 The prevention programme used in the INSPIRE trial pointed to a negative effect on the occurrence of new RRIs in the subgroup of runners with no previous RRI.17 Therefore, runners without previous RRIs were advised not to change anything in their running behaviour in step one of the enhanced injury prevention programme (online supplemental appendix A). This prevention programme was especially focused on runners who had an RRI in the past. However, we did not detect any between-group differences in the subgroup of participants with a previous RRI. Therefore, the enhanced injury prevention programme did not decrease the number of RRIs in this subgroup.
Strengths and limitations
A strength of this study was the large sample size of 4105 participants. To our knowledge, this is the largest RCT on RRI prevention so far. We adhered to the criteria of the CONSORT statement. Furthermore, the loss to follow-up was relatively low since more than 80% of the participants completed at least one of the follow-up questionnaires. A limitation of this study was that participants who did not complete any of the follow-up questionnaires were on average younger and less experienced runners (online supplemental appendix C). However, these small differences between responders and non-responders are not expected to impact the primary study outcomes. A reported RRI during follow-up was not regarded as new injury if participants reported an RRI on the same location in the previous questionnaire, and if they had reported in that same previous questionnaire not yet to be recovered. Therefore, we may have missed new RRIs on the same location while the previous injury was still present. Hypothetically, this new RRI could have had a different origin than the previous reported RRI (eg, the first RRI may have been patellofemoral pain and the second additional RRI a meniscal tear). We expect that this may have occurred in the vast minority. Another potential limitation is the inclusion of participants with an RRI at baseline, since an existing injury may impact the risk of new injuries at other locations due to dysfunction of the kinetic chain. However, sensitivity analyses excluding those participants with an RRI at baseline showed similar results compared with analyses including all participants. Information on the injury severity and medical consumption was based on the follow-up questionnaires only since this information was not collected through the biweekly injury questionnaires. Therefore, information on the consequences of newly reported RRIs was missing for a total of 186 participants who reported a new RRI in the biweekly injury questionnaire only.
Conclusion
An educational online prevention programme had no effect on the number of RRIs in recreational runners. The prevention programme also had no impact on the occurrence of new RRIs in the subgroup of runners with a previous RRI even though it was specifically aimed at this subgroup of runners. Runners compliant to the programme reported more injuries compared with those in the control group. Therefore, future studies should consider focusing on individual targeted prevention with attention to the timing and application of the preventive measures.
Key messages
What is already known?
The large variety of risk factors indicates that the cause of running-related injuries (RRIs) is multifactorial. However, most prevention studies so far focused on modifying one single risk factor for RRIs and found no effect on the number of RRIs.
What are the findings?
An educational and multifactorial online injury prevention programme was not effective in the prevention of RRIs in recreational runners.
Even though the injury prevention programme was specifically aimed at runners with a previous (but not current) injury, it did not decrease the number of RRIs in this subgroup.
Being compliant with the injury prevention programme negatively affected the injury proportion.
How might it impact on clinical practice in the future?
An educational online injury prevention programme will not reduce the number of injuries in recreational runners.
Future studies should focus on how to improve injury prevention programmes, possibly by more targeted and individualised educational interventions.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Medical ethics approval was obtained by the Medical Ethical Committee of the Erasmus Medical Center Rotterdam, The Netherlands (MEC-2019-0136). Participants gave informed consent to participate in the study before taking part. The trial was prospectively registered (www.trialregister.nl; NL7694).
Acknowledgments
The authors would like to thank all runners that participated in the SPRINT study and running organisation Golazo Sports (Rotterdam Marathon Study Group) for their collaboration.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rj_devos, @mvanmiddelkoop
Contributors All authors made substantial intellectual contributions to the development of the study protocol, interpretation of the results and drafting of the manuscript. KLAC performed the data collection and data analysis and wrote the manuscript, under supervision of TF, MvM, and R-JdV. The trial was coordinated by MvM. All authors read and approved the final manuscript. MvM is the study guarantor.
Funding The SPRINT study was funded by the Netherlands Organisation for Health Research and Development (ZonMW), grant number 50-53600-98-104.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.