Article Text

Abstract
Objective To investigate the underlying causes and regional patterns of sudden death in football (soccer) players worldwide to inform and improve existing screening and prevention measures.
Methods From 2014 to 2018 cases of sudden cardiac death (SCD), survived sudden cardiac arrest (SCA) and traumatic sudden death were recorded by media monitoring (Meltwater), a confidential web-based data platform and data synchronisation with existing national Sudden Death Registries (n=16). Inclusion criteria were met when sudden death occurred during football-specific activity or up to 1 hour afterwards. Death during other activities was excluded.
Results A total of 617 players (mean age 34±16 years, 96% men) with sudden death were reported from 67 countries; 142 players (23%) survived. A diagnosis by autopsy or definite medical reports was established in 211 cases (34%). The leading cause in players >35 years was coronary artery disease (76%) and in players ≤35 years was sudden unexplained death (SUD, 22%). In players ≤35 years the leading cause of SCD varied by region: cardiomyopathy in South America (42%), coronary artery anomaly in North America (33%) and SUD in Europe (26%). Traumatic sudden death including commotio cordis occurred infrequently (6%). Cardiopulmonary resuscitation (CPR) resulted in a survival rate of 85% with the use of an automated external defibrillator (AED) compared with 35% without.
Conclusions Regional variation in SCD aetiology should be verified by expansion of national registries and uniform autopsy protocols. Immediate access to an AED at training and competition sites, as well as CPR training for players, coaches and staff members, is needed to improve survival from SCA.
- football
- prevention
- death
- resuscitation
- heart disease
Data availability statement
No data are available.
Statistics from Altmetric.com
Introduction
According to the FIFA Big Count in 2006, there were 265 million football (soccer) players worldwide, a number with increasing tendency (10% per 6 years). Sudden cardiac death (SCD) is a tragic, but rare event in different sports.1 2 In adolescent high-level football players, the incidence of SCD has recently been shown to be 6.8/100.000 athletes per year.3 Nevertheless, the burden of exercise-related SCD in football players at different ages and levels remains unclear due to the lack of football-specific studies.4 However, football is the sport, which has taken the problem of SCD most seriously and has initiated several activities.5
Large population-based studies about SCD and survived sudden cardiac arrest (SCA) in athletes from the USA and Europe indicate regional differences in the underlying causes of death.6–9 A different ethnic and genetic mix between these regions may lead to such a heterogeneous distribution. It is therefore of great relevance to investigate such regional patterns to possibly optimise existing screening and prevention procedures, and reduce fatalities.
Although football players are at lower risk of traumatic sudden death compared with other sports such as baseball, hockey or skiing,6 10 football-specific circumstances, which may potentially lead to death,11 have not been investigated yet. Furthermore, prospective, football-specific data of secondary prevention measures of SCD, such as cardiopulmonary resuscitation (CPR) and use of an automated external defibrillator (AED), have not been systematically examined. This registry aims to investigate the underlying causes of sudden death (SCD), survived SCA and traumatic sudden death in football players worldwide, both at professional and amateur level to provide an improved basis for prevention strategies and the emergency treatment (rescue chain) in the respective regions.
Methods
This prospective observation study started in 2014.
Definitions
SCD was defined as death occurring during football-specific exercise (warm up, training, match) or within 1 hour after cessation of activity. Survival due to successful defibrillation and/or CPR was defined as SCA. The playing level of football players was divided into three categories: (1) elite football players were specified as subjects younger than 40 years who compete for a first or second division team at national or professional level with regular training; (2) competitive football players were defined as subjects of any age who compete for an amateur league team (including youth, academy and college teams) and regularly participate in training; and (3) recreational football players were characterised as individuals of any age who play football either on a regular or irregular basis (kick-around with friends, recreational tournaments) without the pressure to win against others.
Inclusion and exclusion criteria
We included football players at any age. Furthermore, codes of football such as futsal, beach soccer or walking football were included as they represent elements of five-a-side-football, which is played throughout the world. All sudden death events occurring during or within 1 hour after training (all organised sports activities for football players) and competitions were included. Sudden death without relation to football-specific exercise was excluded from the study, in particular during activities other than football or, during rest or sleep. Furthermore, related sports with common characteristics and key elements of football (other ‘codes of football’) such as rugby, Australian rules, American or Gaelic football, were not considered.
Case detection
In 2014, an online reporting form on a web-based data platform (https://www.uni-saarland.de/fifa) became operative under the auspices of FIFA. An open access online questionnaire allowed coaches, players, physicians, family members, referees and other people involved to report a case of sudden death. Data collection was enabled in an anonymised manner (except contact details) and besides basic information (age, gender, ethnicity, date, country) the questionnaire focused on the circumstances of sudden death of a football player (https://www.uni-saarland.de/en/faculty-hw/fifa/en/report.html). Translations into many relevant languages in worldwide football (English, French, Spanish, Portuguese, German, Italian, Arabic, Japanese, Greek, Turkish, Russian) were provided by FIFA or cooperating researchers in the respective countries.
Additionally, a professional press monitoring application by the Meltwater company (global market leader, covering 238 countries, crawling on 3.1 million articles per day) was used. A daily systematic, reporter-independent media search in four corresponding languages of FIFA (English, French, Spanish, German) was performed by a physician using a combination of keywords and operators to produce accurate search results (Boolean search type): “football”, “football player”, “soccer”, “soccer player”, “national player” OR “goalkeeper” AND “death”, “deathly”, “fatal”, “dead”, “stroke”, “heart failure”, “heart attack”, “sudden death”, “cardiac death”, “cardiac arrest”, “infarction”, “lifeless”, “collapse”, “resuscitation”, “resuscitate”, “CPR revival”, “resuscitation”, “revitalization”, “revivification”, “reanimation”, “reactivation” OR “revivalism”.
Furthermore, data synchronisation with other institutions recording sudden death cases (19 FIFA Medical Centers of Excellence (hospitals, outpatient clinics), 16 national Sudden Death Registries (SDRs), 2 sudden death foundations) was carried out.
Once a case was submitted, contact with the reporting person to conduct an orienting interview was attempted. Systematic tracking of each case was always based on descendants’ agreement and release from medical confidentiality for the attending physicians. Subsequently, precise medical information was requested including autopsy reports, clinical and demographic details. Whenever necessary, pathological findings were verified by direct communication with the medical examiner. Clear findings were considered as ‘confirmed causes’ and slightly ambiguous results in combination with a positive (family) history, pre-existing cardiovascular diseases or risk profiles as ‘suspected causes’.
Circumstances of CPR were analysed for moment, first responders and availability of an AED at the scene. Furthermore, the onset of CPR was distinguished between ‘prompt’ (on-site bystanders or attending team physicians of elite players) and ‘delayed’ (inactivity until the arrival of paramedics or first responders) according to the respective reports. Cases were assigned to different racial and ethnic groups (ie, white, black, Hispanic, Asian) on the basis of medical reports, autopsy reports or published photos.
Statistics
For this observational study descriptive statistics were used mainly. Normally scaled variables were grouped together into categories. For each category the frequency or percentage was calculated. Data were expressed as means±SD. Differences in survival rates were analysed using a two-sided Χ2 test. Analysis was performed using Statistica V.10 software (Statsoft, Tulsa, Oklahoma, USA). The significance level for the alpha error was set at p<0.05.
Results
Over a 5-year period, a total of 617 cases of sudden death (607 football players, 4 futsal players, 4 beach soccer players and 2 walking football players) from 67 countries were reported to the registry. In 142 cases SCA was survived (23%). The mean age was 34±16 years (range 5–76 years) and gender distribution showed a strong predominance of men (n=594, 96%). The majority of all cases occurred at amateur level (95 %, n=584), which was further divided into recreational players (45%, n=279, age 40±16 years) and competitive players (50%, n=305, age 28±14 years). Elite players represented only a small fraction (5%, n=33, age 26±6 years). In 157 cases field position was reported showing 38 goalkeepers (24%), 45 defenders (29%), 43 midfielders (27%) and 31 strikers (20%). Cases were identified via press monitoring (58%, n=359), data synchronisation with 16 national SDRs (33%, n=201), online reporting system (6%, n=37) and reports by FIFA Medical Centers of Excellence (3%, n=20). After implementation of professional press monitoring in 2016, the number of captured cases increased each year by 7 in 2016, 18 in 2017 and 27 in 2018, respectively.
Causes of sudden death
A specific cause of sudden death could be documented in 211 cases (34% of all cases) of which 124 cases were identified by autopsy in 21 countries. In 101 cases autopsies were reported from the cooperating registries and reviewed in the respective language by medical professionals on a national level. Due to national data protection law, direct access to autopsy reports was limited (only 11 reports available). In 23 cases submitted via the online reporting form, autopsies were verified by phone interviews with the treating physician, medical examiner or coroner. In 87 SCA survivors a definite diagnosis was assigned on the basis of medical reports and clinical office evaluations. In 69 cases medical reports were considered reliable after discussion with medical professionals of the reporting national registries or FIFA Medical Centers of Excellence. Furthermore, after systematic tracking of 18 SCA survivors reported through media, a diagnosis was confirmed via direct interview with the attending physician (n=16) or the survived subject (n=2). However, aetiology tracking based on media reports (n=359) was generally difficult resulting in only 49 diagnoses (14%, including 31 suspected diagnoses).
Causes were divided into the following categories: cardiovascular (82%), trauma-related (11%) and non-traumatic (7%). An overview of confirmed and suspected diagnoses is presented in table 1.
Summary of 211 confirmed diagnoses and 51 suspected diagnoses of sudden death (including SCA with survival)
The most common finding ≤35 years was sudden unexplained death (SUD) with a structurally (gross and histologically) normal heart at autopsy or negative diagnostic findings after survival. Notably, in the age group ≤35 years 7 of 14 confirmed diagnoses of coronary artery anomaly were present in women. The age-dependent differences in causes of sudden death (including SCA with survival) are illustrated in figure 1.

(A) Causes of sudden death (including SCA) at any age (n=211). (B) Causes of sudden death (including SCA) ≤35 years (n=145). Trauma involves high-impact trauma (traumatic intracranial haemorrhage,carotid artery rupture, abdominal bleeding, neck fracture); others include non-traumatic causes, valvular heart disease,congenital heart disease, unspecified cardiovascular diseases, non-traumaticintracranial haemorrhage and electrical heart disease. CAA, coronary artery anomaly; CAD, coronary artery disease; CC, commotio cordis; CM, cardiomyopathy; MC, myocarditis; SCA, sudden cardiac arrest; SUD, sudden unexplained death.
Besides confirmed as well as 8% suspected diagnoses based on history and circumstances, the majority of all reported cases (58%; 309 SCDs and 46 SCAs) remained unclear owing to the following reasons: (1) autopsies were not performed (not being legally mandatory/permitted in many countries and due to family decision based on cultural differences); (2) disclosure of medical details was restricted due to confidentiality reasons or family decision (including 58 SCAs and the respective follow-up examinations).
Geographical distribution
A substantial part of all reports was received from Europe (n=354, 57%) followed by South America (n=74, 12%), North America (n=64, 10%), Asia (n=49, 8%), Africa (n=39, 7%) and Australia (n=37, 6%). A list of the case reports in the different countries is presented as online supplemental file 1. In North America and Australia survival rates of cardiac arrest (52% and 49%, respectively) appeared more favourable than in Europe (23%) and Asia (14%). Poor outcomes were observed in South America (4%, 1 survival per 25 SCDs) and Africa (3%, 1 survival per 39 SCDs).
Supplemental material
In players ≤35 years regional patterns of the leading causes were observed: cardiomyopathy in South America (42% of all cases on this continent), coronary artery anomaly in North America (33%) and SUD in Europe (26%). However, in the age group >35 years, in which coronary artery disease (CAD) prevailed by far (76%; 50 of 66 cases), no clear regional differences were observed. An overview of the geographical distribution of the most common causes of sudden death (including SCA with survival) is given in table 2.
Geographical distribution of the most frequent causes of sudden death (including SCA with survival) ≤35 years (n=145) and >35 years (n=66)
Moment of SCD/SCA and onset of CPR
Overall survival was 23% (142 of 617 players). In 84% of all cases SCD/SCA occurred during football-specific activity including match (n=431) or training (n=88) resulting in a survival rate of 24%. When the moment of SCD/SCA was within 1 hour after match (n=79) or training (n=9), only 17% survived. In 10 cases SCD/SCA happened during warm-up before a game and was survived in only one of them. Information about the circumstances of CPR was available in 471 cases (76%, figure 2).

Circumstances of out-of-hospital cardiopulmonary resuscitation (CPR) and the respective survival rates in 471 football players. Prompt, immediate CPR by on-site bystanders or attending team physicians of elite players; delayed, no CPR until the alarmed emergency medical services (EMS) arrived; lay persons, CPR performed by lay persons; professionals, CPR performed by professionals (physicians, paramedics, nurses, fireworkers, lifeguards) who happened to be at the scene; defib on-site, defibrillation by using an automated external defibrillator at the scene; defib EMS, defibrillation by the alarmed EMS.
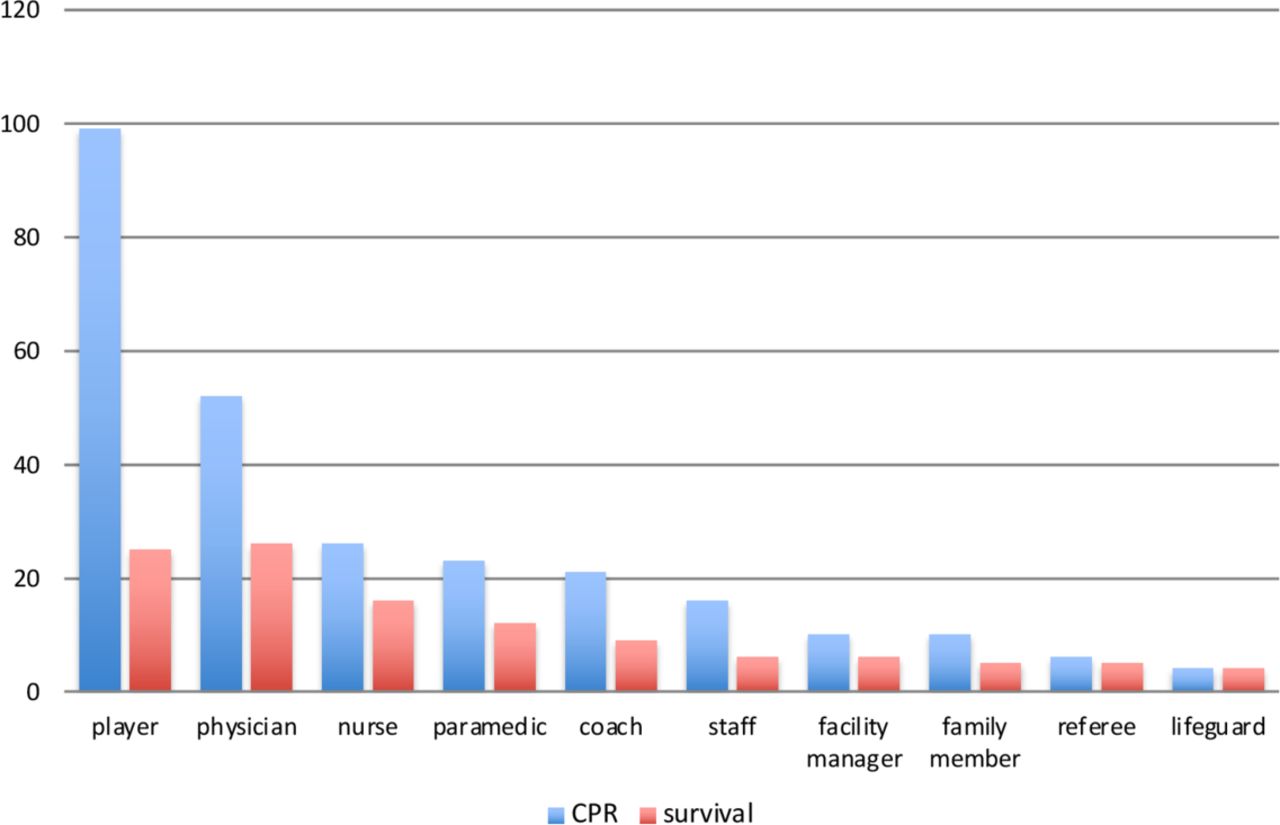
CPR was initiated promptly in 68% of these cases. Delayed CPR (inactivity until the arrival of paramedics or first responders) occurred according to the reports in 81% (121 of 149 cases with delayed CPR) due to misinterpretation of symptoms or unawareness. Prompt CPR was performed in 182 cases (57%) by lay persons resulting in a survival rate of 35%. When CPR-trained staff (physicians, nurses, firefighters, paramedics, lifeguards) happened to be at the scene, prompt CPR resulted in a survival rate of 50% (61 of 123 cases). Survival increased to 85% (35 of 41 cases) when CPR was initiated by trained staff and an AED was used (difference, 35%; 95% CI, 19% to 47%; p=0.001). On the contrary, survival rate was lower (20/43; 47%) after defibrillation by emergency medical services (difference, 38%; 95% CI, 19% to 55%; p=0.001). Notably, football players themselves performed prompt CPR most frequently before arrival of emergency medical services (36%; 99 of 273 cases; figure 3). The survival rates of elite players, competitive players and recreational players were 30%, 26% and 19%, respectively.
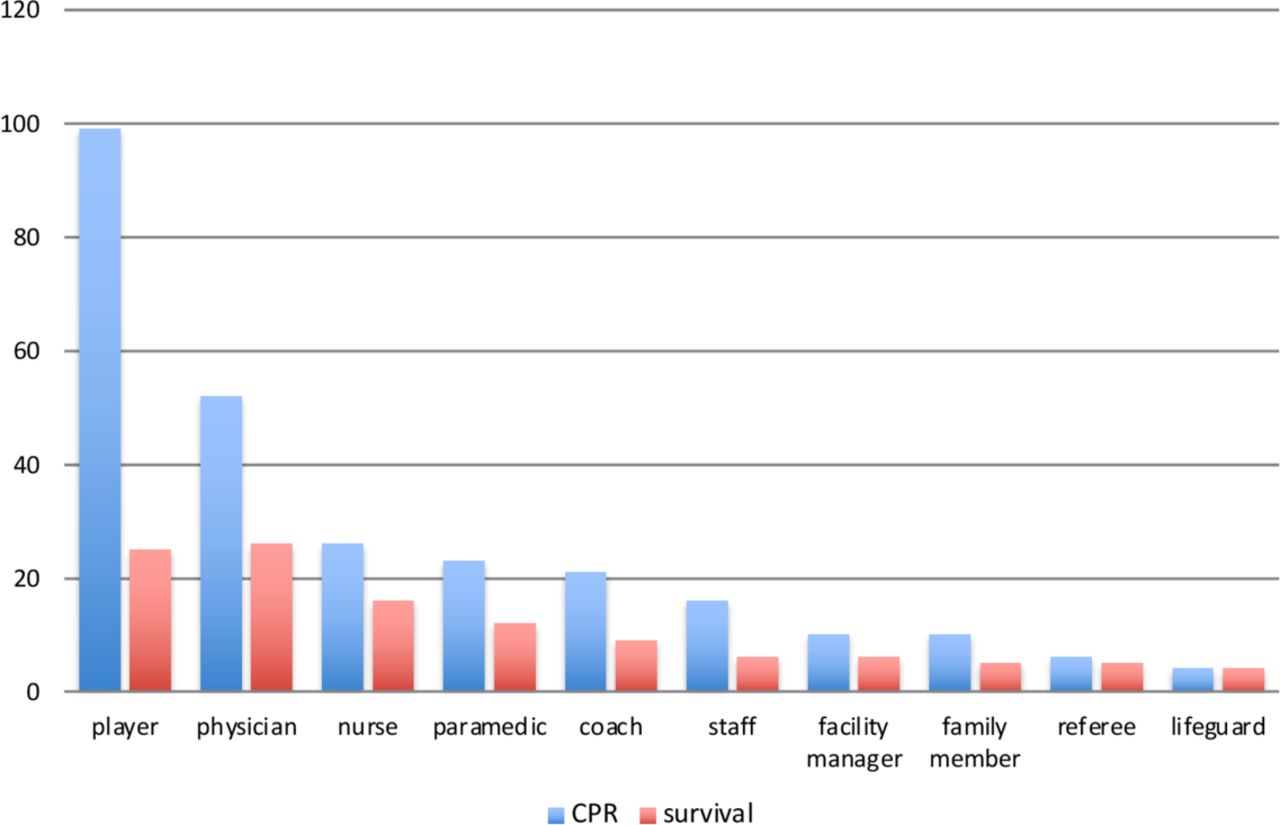
Out-of-hospital cardiopulmonary resuscitation (CPR) by different groups of first responders at the scene and the respective survival rates in 273 cases.
Pre-cardiac arrest symptoms and recognition of SCD/SCA
In 183 (30%) of all cases, symptoms directly preceding SCA were reported. Information was obtained from documented case history (online platform and national registries) and media (interviews with survivors or family members). Most frequently, the combination of nausea and general discomfort (58%, n=106)—often merging into each other—was observed. Second leading symptom was chest pain (24%, n=45), which predominated in the age group >35 years (23 of 76 cases, 30%), but was also present in the young ≤35 years (21 of 132 cases, 16%). Other symptoms were dyspnoea and dizziness accounting each for 9% (n=16) of cases with reported symptoms. In only 13 cases (6%) with pre-cardiac arrest symptoms, pre-existing diseases or similar symptoms were known. Apart from these warning symptoms, there were 24 cases reporting brief myoclonic jerks directly after the subject collapsed to the ground.
Race and ethnicity
Of the 211 cases with confirmed diagnoses, 204 cases (97%) could be assigned to the following ethnic groups: white (69%, n=141), black (16%, n=32), Hispanic (9%, n=19) and Asian (6%, n=12). The proportion of cardiomyopathy was 28% (n=9) in black, 26% (n=5) in Hispanic, 17% (n=2) in Asian and 7% (n=10) in white players. Hypertrophic cardiomyopathy (HCM) predominated in Hispanic (11%) and black (9%) players, and arrhythmogenic right ventricular cardiomyopathy (n=4) was exclusively observed in white players. In the young ≤35 years the proportion of coronary artery anomaly was 6/31 (19%) in black and 4/90 (4%) in white players.
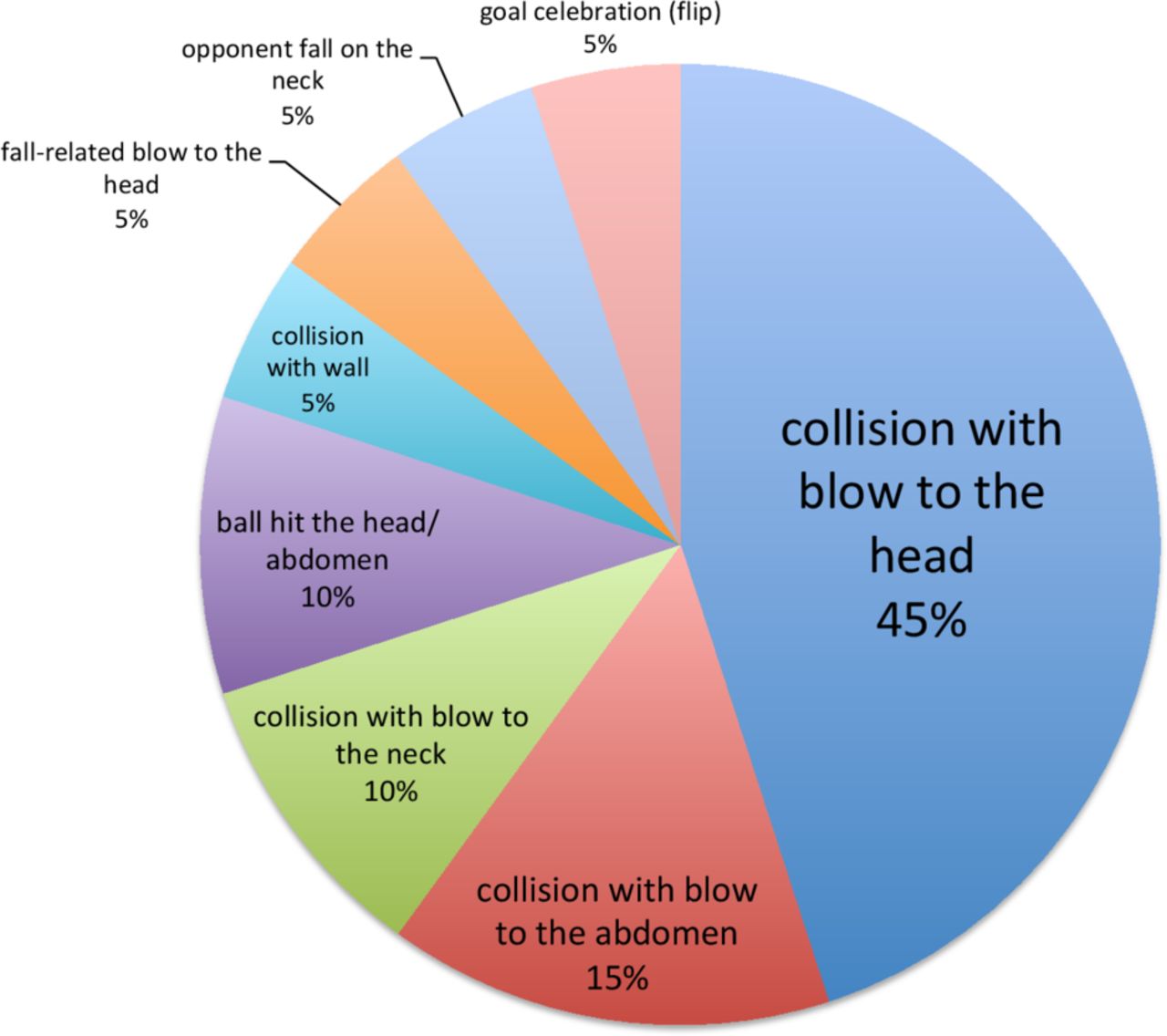
Traumatic sudden death and commotio cordis
Sudden death as a result of trauma occurred in 34 cases (6% of total, mean age 20±7 years). Causes of high-impact trauma were head injury (11 cases), neck trauma (5 cases) and blunt abdominal trauma (4 cases). The respective injury mechanisms implicated in traumatic sudden death and cardiac arrest are demonstrated in figure 4. Field position was reported in 12 cases (six goalkeepers, five midfielders and one striker). Commotio cordis was confirmed in seven cases and highly suspected in seven other cases as the most probable diagnosis based on history (innocent-appearing, low impact blow by a ball, fist or elbow to the precordium resulting in cardiac arrest) and the absence of other plausible causes. When adding the seven cases highly suggestive of commotio cordis to all confirmed sudden death cases in football players ≤35 years (n=145), commotio cordis constituted 9% of total (14 of 152 diagnoses, mean age 22±6 years). In 11 of 14 cases (79%) the ball hit the chest and in 3 cases (19%) there was a tackle, in which a blow by the opponent’s elbow or fist to the precordium was reported. Commotio cordis was survived in six cases (43%).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Injury mechanism related to high-impact trauma resulting in sudden death and cardiac arrest (n=20).
Discussion
In this worldwide observational study, regional and age-dependent distribution patterns of the underlying substrates of SCD/SCA in football were documented. Gender distribution showed a strong predominance of men (96%), which is in the upper range of earlier studies in athletes (81%–97%)9 12–14 and can only partly be explained by the preponderance of male players in this particular sport. The aetiology of SCD/SCA was mainly in accordance with expectations from regional studies.7 12 15–17 Some of the results should be regarded as preliminary because of very heterogeneous reporting from different countries and continents.
SCD/SCA in the young
Structurally normal heart
In the young ≤35 years a structurally normal heart (SUD) was the most frequent finding when autopsies were carried out. This raises the suspicion for primary arrhythmia syndromes. In line with previous studies in athletes SUD seems to predominate in Europe,15 16 although similar observations were also made on other continents.12 17
Cardiomyopathy
Cardiomyopathy was the second most leading cause ≤35 years and showed the highest proportion (5 of 12 cases, 42%) in South America. Notably, HCM was the most frequently reported form of cardiomyopathy ≤35 years and predominated not only in black athletes, as published previously,14 but also in Hispanic athletes. Furthermore, subtypes of cardiomyopathy might have been under-reported given the considerable number of cardiomyopathies not otherwise specified possibly reflecting a lack of international autopsy standards, even though European guidelines exist.18
Premature CAD and coronary artery anomaly
In Europe 13% (11 of 84 cases) of the football players suffered from premature CAD, a number, which is at the lower range when compared with other European athletes (6%–38%).7–9 19 Coronary artery anomaly, which is associated with the highest risk of sports-related deaths,9 predominated in North America and might be a greater risk factor for SCD in female football players. Furthermore, coronary artery anomaly was more common in black than white players, as observed previously.14
Myocarditis
Myocarditis was diagnosed infrequently (4%, eight cases). When adding three cases of suspected myocarditis and two cases of myocardial fibrosis (suggestive of prior myocardial infection), myocarditis accounted for 6%. This is consistent with previous observations in competitive athletes,8 19 although higher proportions up to 24% have been observed.7 12
SCD/SCA in football players >35 years
CAD prevailed by far in football players >35 years, as previously observed in competitive and recreational athletes.7 8 The spectrum of differential diagnosis for SCD/SCA in this age group seems to be smaller than in the young. No regional differences in the causes of SCD/SCA were observed.
Outcome of CPR on the field of play
The overall survival rate of 23% was higher when prompt CPR was performed by lay persons (35%) and CPR-trained staff (50%). Notably, the additional use of an AED by CPR-trained staff resulted in a survival rate of 85%. A similar rate has been previously demonstrated in student athletes and adults during physical activity.20 When the defibrillator was supplied by emergency medical services, the survival rate was lower,20 most likely because of delayed arrival of the emergency medical services staff. This calls undoubtedly for the presence of AEDs in amateur clubs and regular practice sessions for club players and staff on the features of an emergency action plan.
Emergency procedures and preventive measures
When comparing 10 different groups of first responders at the scene performing prompt CPR, the majority were football players themselves (36%). Therefore, CPR training with proper education should be strongly encouraged in players and not just staff. In general, staff, physiotherapists and athletic trainers should be trained to recognise SCA and be ready to implement prompt CPR and use of an AED.21 22 Since time from collapse to defibrillation is the most important determinant of survival,23 recognition of pre-cardiac arrest symptoms is crucial.21 22 Survival rate showed geographical differences with poor outcomes in South America and Africa (≤5%). In these regions the distribution of AEDs should be encouraged and supported to reach the more desirable rates of North America and Australia (survival approximates 50% in this study, consistent with a recent study in the USA).13
Specific circumstances of traumatic sudden death in football
Trauma constituted 6% of all sudden deaths. The most frequent injury mechanism was a collision with the opponent leading to intracerebral haemorrhage in more than half of all traumatic cases. Commotio cordis, which is often under-reported in young athletes as it occurs in a wide variety of circumstances,24 25 was observed in 9% of football players ≤35 years. Notably, previous studies on sudden death showed a slightly lower percentage of commotio cordis (4%–7%) in football.6 25 With regard to the football-specific circumstances of commotio cordis, 79% (11 of 14) were triggered by the ball. Although this is in contrast to previous data suggesting footballs (as projectiles) are rarely implicated in commotio cordis (1 of 87 projectiles),25 a recent study indicates a risk of ball sports.11
Limitations
Weaknesses and strengths of the registry
This study represents the first worldwide SDR of football players (and athletes). It is obvious that such an effort suffers from several shortcomings. Most importantly, many countries lack a duty to report cases of sudden death. Thus, cases of sudden death may have been missed which could have impacted the proportion of aetiologies described. Furthermore, the quality of diagnoses was reduced due to the lack of autopsy or medical reports in all cases, and in some cases relied on media reports only. Case detection was limited due to the lack of cooperating national SDRs (only n=16). A larger number of national registries may have the potential to better detect out-of-hospital cardiac arrests.26 This holds particularly true for ambulance-based registries on a national level aiming to investigate the incidence of sudden death. However, it was not our aim to calculate incidences, but rather to provide an initial overview of worldwide regional distribution of sudden death in football. Since accurate estimation of worldwide sudden death events (numerator; unknown number of under-reported cases) and football players at risk (denominator; lacking reliable data) remains a highly intractable task, multilingual media search was chosen as the best alternative source, knowing well the associated rate of under-reporting ranging from 5% to 70%.12 27–29 Nevertheless, some patterns are potentially less influenced from reporting inaccuracies, for example, disease distributions and possible survival rates (because there is no systematic influence to be expected from different reporting). Notably, 42% of our cases were not captured through media. Therefore, a strength of this registry was the double controlling with the cooperating registries and FIFA Medical Centers of Excellence resulting in the acquisition of detailed medical information.
Experiences in setting up a worldwide registry
Ideally to investigate sudden death in football, medical and autopsy records should be regarded as the primary source. To obtain such data, we regularly communicated with various medical specialists involved in national registries, which was a time-intensive but productive approach. In contrast, systematic tracking of cases reported via media was difficult. When planning a new registry on a national level, establishing automated access to ambulance-based records or in-hospital records would be considered the gold standard (not feasible in our worldwide study) to accurately determine aetiology and estimate sudden death incidence.26 Additionally, recommendations on uniform registration standards of sudden death in athletes should be implemented.30
Other limitations
Although three different data sources were used to build a comprehensive database, the cause of sudden death in this study remained unclear in 58% of all reported cases due to a lack of sufficient medical information. However, demographic data were available in the vast majority of these cases. Given the high rate of unexplained diagnoses, entities such as cardiac ion channelopathies, which were recently suspected in about 30% of autopsy-negative results,31 might have been underestimated in this study. Likewise, diagnosis of coronary artery anomaly was probably under-reported given the limitations of non-invasive imaging,32 which is not standard in the pre-competition medical assessment in most if not all FIFA member associations. Furthermore, it is quite conceivable that within the 61 unexplained SCAs observed in our study (15 SUDs, 46 unknown diagnoses), a specific pathological condition such as HCM remained undiagnosed. Recently it was demonstrated that diagnosis of early-stage HCM in young football players is challenging and close follow-up is recommended.3
Owing to the voluntary nature of reporting sudden death (no mandatory recording in any country) there is unavoidably a considerable under-reporting of cases, which is very difficult to estimate in its size based on available information. Likewise, time from collapse to CPR, which is in general rarely accurately measured or incomplete in out-of-hospital cardiac arrests,33 was described in simplified terms (‘prompt’ or ‘delayed’) based on the respective reports. Although inclusion of sudden death within 1 hour after sports-related activity is in accordance with convention, we probably underestimated the real figure of sudden death by excluding cases outside this time window during rest. Furthermore, we cannot exclude a potential reporting bias by region. First, most national registries (10 of 16) and participating FIFA Medical Centers of Excellence (12 of 19) are located in Europe, which might explain the dominance of reports from this continent. Second, potential under-reporting in South America might be due to the absence of national SDRs. Third, world languages such as Mandarin, Hindi or Arabic were not traffic languages of our searching tool. Furthermore, diagnostic accuracy was limited to healthcare structure, family decisions and national law (restrictions to perform autopsies). The specific aetiology of SCD/SCA could not be confirmed in the majority of cases, and thus the reported causes may be altered if more complete data were available. However, it seems unlikely that the general pattern of diseases has been altered because there are no stigmas associated to any one of the causes. In addition, regional differences in aetiology might have been influenced by variability in forensic experience. Therefore, a verification process and standardised pathological criteria across geographical regions might improve determination of the specific causes. Calculation of regional incidences was not feasible owing to the low number of national registries and lacking of precise information about exposure and participant data.
Conclusion
This is the first report from the FIFA-SDR after 5 years of data collection. We report sex, age and disease distributions with some inequalities between continents that may support decisions about primary prevention (diagnostic) measures. Heterogeneous reporting by country affected data reliability but some outcomes like survival rates are less prone to be influenced from reporting inaccuracies.
In terms of secondary prevention, regular CPR training of football players and staff with direct access to AEDs is a recommended measure to turn SCA into a more frequently survived event (up to 85% in this study). Therefore, a wide distribution and availability of AEDs in football clubs should be striven for and CPR training together with education strongly encouraged in players, staff, coaches and club members.
Setting up a worldwide SDR in football is challenging and needs further refinement. In this sense, it is a ‘work in progress’. It is evident that more systematic data collection about sudden death in football by national registries is needed to decrease the number of unreported cases and assist our ongoing prospective surveillance to better inform prevention measures in football.
Key messages
What are the findings?
Over a 5-year period, regional and age-dependent distribution patterns of the underlying substrates of sudden cardiac death (SCD) were found in worldwide football.
While definitive conclusions cannot be drawn, in players ≤35 years the leading causes were cardiomyopathy in South America (42%), coronary artery anomaly in North America (33%) and sudden unexplained death in Europe (26%). In players >35 years, coronary artery disease was the leading cause (76%) with no clear regional differences.
Compared with an overall survival rate of 23%, survival was better when prompt cardiopulmonary resuscitation (CPR) was performed by lay persons (35%), CPR-trained staff (50%) and the use of an automated external defibrillator (AED) by CPR-trained staff (85%).
How might it impact on clinical practice in the future?
More national registries should be installed to verify the observed distribution patterns in causes of SCD in football players before an adjustment of primary prevention measures can be recommended.
With regard to secondary prevention measures, regular CPR training of football players and staff with direct access to an AED at trainings and competitions is a strongly recommended standard to improve survival from sudden cardiac arrest.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethics committee and by the independent Data Protection Centers Saarland, Germany (approval number 172/11).
Acknowledgments
The authors thank the FIFA and the FIFA Medical Centers of Excellence for their operational support. Furthermore, our thanks are directed to the non-profit organisations 'Fondazione Giorgio Castelli Onlus' (Rome, Italy) and 'Heartbeat of Football Foundation' (Sydney, Australia) for their tireless work in reporting and tracking SCD cases.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ProfJiriDvorak
Contributors TM, JS and JD designed the study. FE, TM, JS, AK and PB collected data. FE analysed the data and drafted the manuscript. All authors contributed to the final manuscript.
Funding This work was funded by F-MARC (FIFA Medical Assessment and Research Centers). Financial support enabled Saarland University to cover the expenses for two main areas: (1) yearly subscription fees for the use of the media search application provided by the Meltwater company; (2) reasonable compensation for the work undertaken by a physician running this registry on a daily basis.
Disclaimer None of the authors were in any way employed by the funding institution. There was no ethical conflict or any unwanted guidance. All authors can take responsibility for the integrity of the data.
Competing interests TM is chairman of the Medical Committee of the German FA and UEFA. JD is former chairman of F-MARC. All authors declare that they have no competing interests regarding the aims of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.