Article Text

Abstract
Objective To evaluate the effectiveness of motor control training (MCT) compared with other physical therapist-led interventions, minimal/no intervention or surgery in patients with symptomatic lumbar disc herniation (LDH).
Design Systematic review and meta-analysis.
Data sources Eight databases and the ClinicalTrials.gov were searched from inception to April 2021.
Eligibility criteria We included clinical trial studies with concurrent comparison groups which examined the effectiveness of MCT in patients with symptomatic LDH. Primary outcomes were pain intensity and functional status which were expressed as mean difference (MD) and standardised mean difference (SMD), respectively.
Results We screened 6695 articles, of which 16 clinical trials (861 participants) were eligible. Fourteen studies were judged to have high risk of bias and two studies had some risk of bias. In patients who did not undergo surgery, MCT resulted in clinically meaningful pain reduction compared with other physical therapist-led interventions (ie, transcutaneous electrical nerve stimulation (TENS)) at short-term (MD –28.85, –40.04 to −17.66, n=69, studies=2). However, the robustness of the finding was poor. For functional status, a large and statistically significant treatment effect was found in favour of MCT compared with traditional/classic general exercises at long-term (SMD −0.83 to –1.35 to −0.31, n=63, studies=1) and other physical therapist-led interventions (ie, TENS) at short-term (SMD −1.43 to –2.41 to −0.46, n=69, studies=2). No studies compared MCT with surgery. In patients who had undergone surgery, large SMDs were seen. In favour of MCT compared with traditional/classic general exercises (SMD −0.95 to –1.32 to −0.58, n=124, studies=3), other physical therapist-led interventions (ie, conventional treatments; SMD −2.30 to –2.96 to −1.64, n=60, studies=1), and minimal intervention (SMD −1.34 to –1.87 to −0.81, n=68, studies=2) for functional improvement at short-term. The overall certainty of evidence was very low to low.
Conclusion At short-term, MCT improved pain and function compared with TENS in patients with symptomatic LDH who did not have surgery. MCT improved function compared with traditional/classic general exercises at long-term in patients who had undergone surgery. However, the results should be interpreted with caution because of the high risk of bias in the majority of studies.
PROSPERO registration number CRD42016038166.
- physical therapy specialty
- rehabilitation
- back
- exercise therapy
- exercise training
Statistics from Altmetric.com
Introduction
Lumbar disc herniation (LDH) is one of the most common spinal pathologies, which can be associated with debilitating pain1 and neurological dysfunction.2 A herniated disc is diagnosed when the nucleus pulposus extends beyond the normal barrier of the annulus fibrosus.3 It is estimated that LDH has a 1-year incidence of 0.1%–0.5% and a lifetime incidence of approximately 1%–2%.4 In many high-income and low-income and middle-income countries, the increased prevalence of LDH has led to a socioeconomic and healthcare burden affecting the quality of life of patients with LDH. Stewart et al 5 estimated an average of 5.3 hours of lost productive time at work per week, which makes patients vulnerable to reduced performance. Therefore, adequate management of LDH is important for patients, clinicians and healthcare policy makers.
Conservative care options include motor control training (MCT), motor control exercise (MCE), stabilisation and core stability exercises for patients with symptomatic LDH.6 The overarching principle of exercise is to strengthen core muscles. For example, an MCT programme includes low-level sustained isometric contraction of the deeper muscles of the trunk such as multifidus, transversus abdominis and pelvic floor muscles that are typically affected in the presence of pain.6 The intervention focuses on the correction of motor control ‘faults’, such as optimisation of muscle activation or optimisation of posture and movement to modify loading of the lumbar spine and adjacent structures (eg, hip, thoracic spine).7–9
MCT involves individualisation of treatment using a clinical reasoning approach.8 A main advantage of MCT over general exercise is that MCT comprises therapeutic exercise to improve specific motor control features for a broad, multidimensional view incorporating psychosocial aspects of low back pain (LBP).7 Moreover, MCT may help to improve flexibility, posture, ease of movement, enhance body awareness, balance and coordination in patients suffering from LBP.10
To date, no systematic review with meta-analysis has been published on MCT for treatment of LBP in patients with LDH. MCT is routinely recommended by therapists to alleviate pain and symptoms in patients with LDH. Thus, a well-designed systematic review can inform clinicians, therapists, healthcare policy makers and patients. Our objective was to examine the effectiveness of MCT in comparison with other common comparisons, that is, physical therapist-led interventions, surgery and placebo/sham treatment in patients with symptomatic LDH.
Methods
The study methodology followed systematic review methods proposed by the Cochrane Handbook,11 and reported findings following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement12 and the recently published Prisma in Exercise, Rehabilitation, Sport medicine and SporTs science guide.13 The protocol of this systematic review has been registered in the international prospective register of systematic reviews (PROSPERO; #CRD42016038166; http://www.crd.york.ac.uk/PROSPERO) and published in a peer-reviewed academic journal.6 Any amendments to the protocol were made and are described in the relevant sections.
Information sources and search strategy
An extension to the PRISMA statement was used for reporting the literature search in this study.14 We performed an exhaustive search in MEDLINE via PubMed, Scopus, PEDro, EBSCO (SPORTDiscus and CINAHL), the Cochrane Central Register of Controlled Trials, the Web of Science and Embase. We added the Web of Science database to the databases listed in the protocol to improve the inclusiveness of the search strategy. A comprehensive search of databases from each database’s earliest inclusive dates to 30 April 2019 was conducted; a subsequent updated search (to 30 April 2021) was also conducted. No restrictions to language or publication status were applied. Given the interchangeable use of various terms in the literature including MCT, MCE, core stability, specific stabilisation exercise and Pilates, all search terms were used. Proper Boolean operators and database filters were applied to optimise the search (online supplemental appendix 1). The strategies were peer reviewed by another author (AK) prior to execution using the Peer Review of Electronic Search Strategies Checklist.15 AA did the search while MP adjudicated. The reference lists of relevant reviews16 17 and included studies were screened for additional references. Google Scholar and ClinicalTrials.gov were also searched in April 2021 to identify any registered yet unpublished or ongoing clinical trials. Finally, we contacted subject-area experts for information about ongoing studies.
Supplemental material
Eligibility criteria
The MCT programme was defined as exercise aiming to facilitate, activate, restore, train or improve the function of the deep musculature of the spine.6 We included clinical trials with concurrent comparison groups in adult patients (≥18 years) with referred leg symptoms, with or without LBP which assessed the effect of MCT compared with other physical therapy interventions, surgery or placebo/sham treatment. Only those studies which defined LDH as displacement of the nucleus and/or annulus fibrosus through a tear of the annulus fibrosus were included.18 Synonymous terms such as prolapse, protrusion and sequestration were used, but the term disc bulging was not sufficient to be considered as an alternative term of LDH.16 18 We did not impose any restriction on lumbar spinal level of disc herniation. Studies which examined specific pathologies, such as systemic inflammatory diseases, fractures, spondylolysis, spondylolisthesis, scoliosis, infections, tumours and osteoporosis, were excluded. To be eligible for inclusion, MCT had to be used as the main intervention, not as a co-intervention to other treatment programmes in trials. Furthermore, when MCT was used in addition to other treatments in primary studies, they had to represent at least 50% of the total treatment programme to be included. Full details of the eligibility criteria and our PICO format19 can be found in the published protocol.6
The prespecified primary outcomes were pain intensity and functional status,6 measured at the time point closest to the end of predefined time intervals (ie, short-term, intermediate-term or long-term). For pain intensity, data of visual analogue scale (VAS), numeric pain rating scale (NPRS) and McGill Pain Questionnaire, and for functional status, data of Roland Morris Disability Questionnaire, Oswestry Disability Index (ODI), modified ODI and ODI-2 were extracted from the included studies. For articles to be included, they had to have at least one of the primary outcomes of this study. The secondary outcomes were muscle endurance, muscle thickness, quality of life, functional tests, return to work and adverse events.6
Selection process
The selection of studies was a three-stage process, with the identified citations independently assessed for inclusion by two authors (MP and MA). The first stage was evaluation of titles retrieved with systematic searches reported above. The article was included in this first screen if the title identified MCT and/or LDH. We then reviewed the abstracts of all potentially eligible articles. Full-text articles meeting the criteria were selected and reviewed independently by both authors and assessed for inclusion in the study. Any disagreement between the two authors was resolved by discussion or by consulting another author (JAH/SMR). In the case of multiple publications (eg, poster, published paper in a peer-review journal, etc), we included only the published paper.
Data extraction
Data on the characteristics of the eligible studies were extracted independently by pairs of authors (MP and SD, MP and MA). We used a Microsoft Excel 365 spreadsheet (Microsoft, Redmond, Washington, USA) which was designed a priori (online supplemental appendix 2). A third author (AK) checked the extracted data for any errors.
Risk of bias assessment
Two authors (MP and SD) independently assessed the risk of bias of each included study. Any disagreements were discussed between the two authors, and a third author (AK) was consulted for final assessment if no consensus could be reached. The risk of bias assessment in the primary studies was performed using V.2 of the Cochrane risk of bias tool for randomised trials (Cochrane RoB 2 tool).20 The Cochrane RoB 2 tool evaluates five domains of bias: (1) selection bias; (2) performance bias; (3) attrition bias; (4) detection bias; (5) selective outcome reporting bias20 21 (online supplemental appendix 3). Contrary to what was stated in the protocol, the assessment tool was changed to the Cochrane RoB 2 tool, since it is more comprehensive and recommended by the Cochrane Handbook.22
Data synthesis and analysis
Pain outcomes were converted to a 100-point scale and examined as a mean difference (MD) since all studies used similar instruments (eg, NPRS, VAS), while functional status was evaluated as a standardised mean difference (SMD) in the plots. SMD was calculated using Cohen’s d and was also interpreted according to Cohen’s rule of thumb: <0.2=no/trivial effect; 0.2 to 0.5=small effect; >0.5 to 0.8=medium effect; >0.8=large effect.23 When medians and IQRs were provided, means and SD were calculated by the method described by Wan et al.24 In the present meta-analysis, most mean/SD ratios were <2, suggesting skewness.25 However, non-normality was not a major issue, since most studies had a relatively sufficient sample size (ie, ≥30 in each subgroup) and so the normality of MD and SMD estimates was justified using the central limit theorem.26 Forest plots were used to depict the effect sizes based on follow-up data and their respective CIs for each study grouping. A negative effect size indicates that MCT is more beneficial than the comparison therapy, meaning that participants have less pain or less functional limitations. Random-effects model was used for all meta-analyses based on the DerSimonian and Laird model, because of expected considerable heterogeneity between studies (eg, different exercises parameters, different co-interventions). Additionally, mean differences in pain score and functional status score were used to compare them with the absolute minimal clinically important difference (MCID) for pain and functional status.27–29 We used a reference MCID of 15 for pain and 10 for functional status based on previous findings.30–32 Furthermore, the MCID for the Biering-Sorensen test was 5.3 s as reported by Cruz-Montecinos et al.33 The number needed to treat was also calculated using the Psychometrica online calculator (http://www.psychometrica.de/effect_size.html) as an estimate of the clinical benefit for the primary outcomes.
Meta-analyses were conducted using the ‘metan’ package in Stata MP V.16.0 (StataCorp, College Station, Texas, USA). If data were not available in numerical format, we estimated it from figures using WebPlotDigitizer V.4.2 (https://automeris.io/WebPlotDigitizer/index.html). Whenever possible, we also calculated the power of each meta-analysis using the ‘power.analysis’ function from the ‘dmetar’ package34 (RStudio V.4.0.0; RStudio Team, 2020).
For the secondary outcomes, we calculated MD with 95% CI between the intervention and comparison groups for each continuous variable. The secondary outcomes were not pooled for meta-analysis, as it was expected that not many studies were available for the secondary outcomes. Additionally, we reported potential conflicts of interest as well as the funding source.
Subgroup analysis
After several team meetings, the authors decided to stratify the analyses according to (1) those who had not yet undergone surgery and (2) those who had undergone surgery and subsequently examined the effect of MCT for three to four different comparisons (ie, other forms of exercises; minimal intervention, self-management or no intervention; other physical therapist-led interventions, including electrotherapy,35 36 mixed physical therapy techniques37 or conventional physical therapy38 39 and surgery) and performed meta-analyses separately for each stratum. Sensitivity analysis is presented in online supplemental appendix 4.
Unit of analysis issues
Where a study was defined as a crossover trial, data were extracted only up to the point of crossover. Moreover, the unit of analysis was based on aggregated outcome data for treatment groups reported in the trial publication. Thus, we did not obtain individual participant data to carry out meta-analysis.
Assessment and investigation of heterogeneity
Between-study statistical heterogeneity among the included studies was quantified by the I2 statistic and Q test (χ2) with a significance level at p≤0.050.40 The interpretation of I2 values was as follows: 0%–40%: heterogeneity may not be important; 30%–60%: may represent moderate heterogeneity; 50%–90%: may represent substantial heterogeneity and 75%–100%: considerable heterogeneity.11
Assessment of publication bias
Although the number of studies was not sufficient for most comparisons, the possibility of publication bias for two comparisons was preliminary assessed by the Egger’s graphs.41 If the 95% CI for the slope of the linear regression included zero, then no publication bias was indicated.
Certainty of evidence
We examined the certainty of evidence for the primary outcomes using the Grading of Recommendations, Assessment, Development and Evaluations approach42 (online supplemental appendix 5).
Patient and public involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for design or implementation of the study.
Results
Study characteristics
After removing duplicates from 22 418 citations, 6695 unique citations were identified and 16 clinical trials with concurrent comparison groups for our systematic review from 11 countries across 3 continents were included (figure 1 and online supplemental eTable 1 for the reasons of exclusion). Of the 16 included trials, 4 eligible studies (25%) were conducted in Turkey43–46; 2 (12.5%) in Sweden47 48 and Brazil,35 36 and one each in Iran,49 Norway,50 Belgium,39 Switzerland,37 Wales,51 China,52 Korea53 and Pakistan.38 All trials were published in English. The 16 studies were published between 2003 and 2019, and 861 participants were examined in total. Study sample sizes (at the level of randomisation) ranged from 25 to 159 (median 57.5, IQR 35.5–60). Study period was reported by 8 studies,36 38 44 46 47 50 52 53 with a median (IQR) of 10 (7.5–19.5) months.
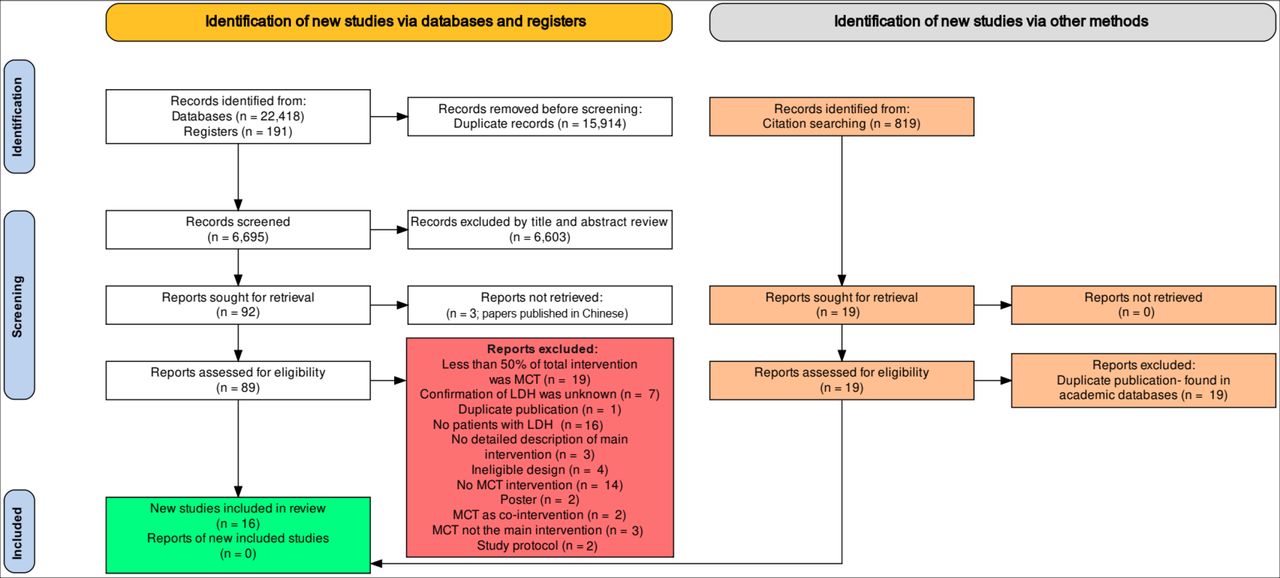
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram (2020) of search process for studies examining the efficacy of motor control training (MCT) in patients with lumbar disc herniation (LDH).
Study population
Seven of the studies enrolled participants with LDH who did not undergo surgery35 36 43 49 51–53 and nine studies included patients with LBP and previous surgery for disc herniation.37–39 44–48 50 The age range of included participants at baseline was 29–65 years with a mean (SD) of 54.38 (9.81) years. In total (n=16), 25% of the studies did not specify the sex/gender of the study population.39 49 51 53 Sixty-nine per cent reported including both male and female participants, and 6% included male participants only.52 Most studies (87.5%; n=14) delivered the intervention programme to participants in outpatient clinics,35–38 44–53 and in the remainder it was unclear.39 43 The level of disc herniation was reported as L4–L5 in four studies (25%),46 48–50 L4–S1 in one study (6%),52 L2–S1 in one study (6%)47 and L3–S1 in one study (6%).44 In the remainder, the level of disc herniation was unknown or unclear. Online supplemental eTables 2 and 3 summarise the characteristics of the included studies and LDH definition of each eligible study.
Primary investigators
In 11 studies, the primary investigators were affiliated with a department of physical therapy, physical medicine, rehabilitation or similar within a university/hospital setting,35 36 38 39 43 45 46 48 49 51 53 in 4 department of orthopaedic44 47 50 52 and in 1 department of anatomy.37
In nine studies, the primary investigators were trained as physical therapist,35 36 38 39 43 48 49 51 53 in three as orthopaedist,47 50 52 and physiatrist,44–46 and in one as physiologist.37 Moreover, in two studies, it was explicitly reported that the primary investigator was involved in treatment,35 36 in five not involved,37 46 47 50 52 and it was unclear or unknown in the other nine studies.
In 14 studies, treatment was delivered by a physical therapist only,35–39 43 46–53 in two by a physiatrist only.44 45
Funding and conflicts of interest
Ten studies were funded by university or professional foundations.35–37 47–53 One study did not receive funds,43 and in the remainder it was unclear.38 39 44–46
The authors of four studies declared no conflicts of interest,35 36 43 52 and in the remainder no official disclosure of conflict of interest was reported.37–39 44–51 53
MCT, clinician and comparison interventions
Nine of the studies implemented MCT as a stand-alone intervention,35–38 46 48 49 51 53 whereas seven studies implemented MCT with other physiotherapist-led treatments, including mobility/warm-up exercises,43 47 52 back education,45 cognitive intervention,50 home exercise44 and ergonomic advice.39 In 10 studies the MCT exercise was supervised,35–37 43 44 46–48 50 52 in 1 study unsupervised49 and in the remainder it was unknown or unclear.38 39 45 51 53 In three trials,36 37 43 MCT focused on trunk muscles (eg, transverse abdominis and lumbar multifidus) according to the protocol proposed by Richardson et al.54 55 Two studies44 48 used Saal approach,56 57 one study50 used O’Sullivan et al approach,58 another study52 used Akuthota et al approach,59 one study35 used Hides et al approach60 and one study53 used Kwon et al approach.61 The remaining studies did not specify which protocols were used.38 39 45–47 49 51 Comparison intervention of each included study is presented in online supplemental eTable 2.
Risk of bias in included studies
The majority of studies (87.5%; n=14) were classified as ‘high risk of bias’,35–39 43–46 48 49 51–53 while only two studies (12.5%) were judged as having ‘some concern’.47 50 No single study was found to have a low risk of bias. Most studies (95%) did not adequately balance baseline covariates between groups, according to the method recommended by Imbens and Rubin.62 Fourteen studies did not perform or report multiple eligible analyses of the data.35–39 43–46 48–53 Furthermore, only two studies (12.5%) registered their protocol, and the analyses were in accordance with a prespecified analysis plan.36 50 A summary of the risk of bias for each included study and each domain is given in table 1. Answers to the signalling questions in each domain for all included studies are also provided in online supplemental appendix 3.
Risk of bias assessment of included studies using V.2 of the Cochrane risk of bias tool
Effects of interventions
Table 2 summarises the treatment effects and the certainty of evidence for all comparisons.
Summary of treatment effects, 95% weighted mean difference, 95% standardised mean difference (SMD), clinical relevance, number needed to treat (NNT) and GRADE summary of findings among studies included in systematic review of MCT for symptomatic LDH
Primary outcomes
Figures 2 and 3 show the results of meta-analyses for the primary outcomes. Those studies that did not report required data for meta-analyses were excluded from the figures and table 2.
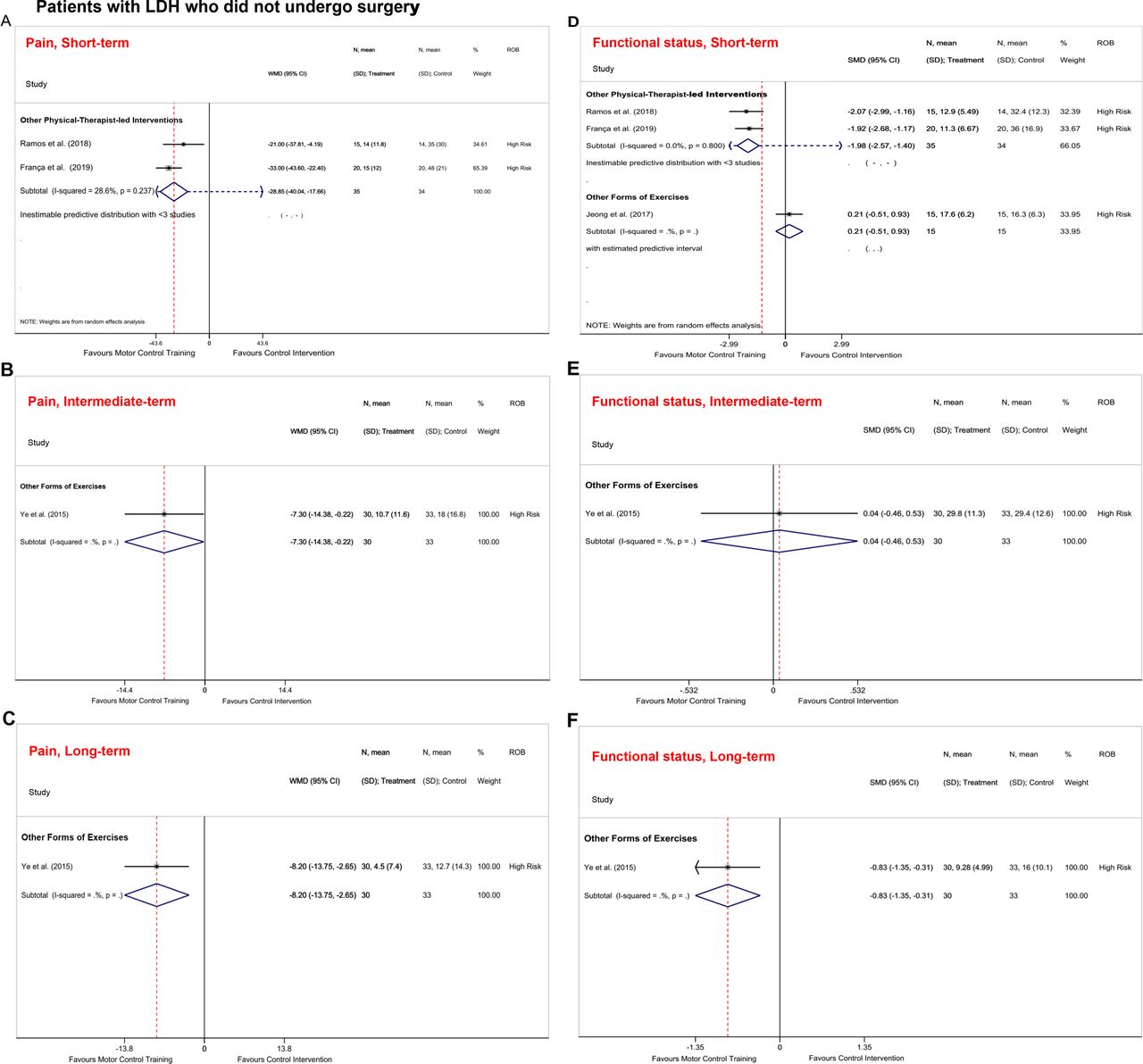
Forest plots of comparisons in patients with lumbar disc herniation (LDH) who did not undergo surgery. (A) Pain at short-term, (B) pain at intermediate-term, (C) pain at long-term, (D) functional status at short-term, (E) functional status at intermediate-term and (F) functional status at long-term. Pain is presented as weighted mean difference (WMD) and functional status is expressed as standardised mean difference (SMD). Whenever a minimum of three studies were available for each comparison, the 95% prediction intervals were also estimated.

{kind=link}
{kind=link}
{kind=link}
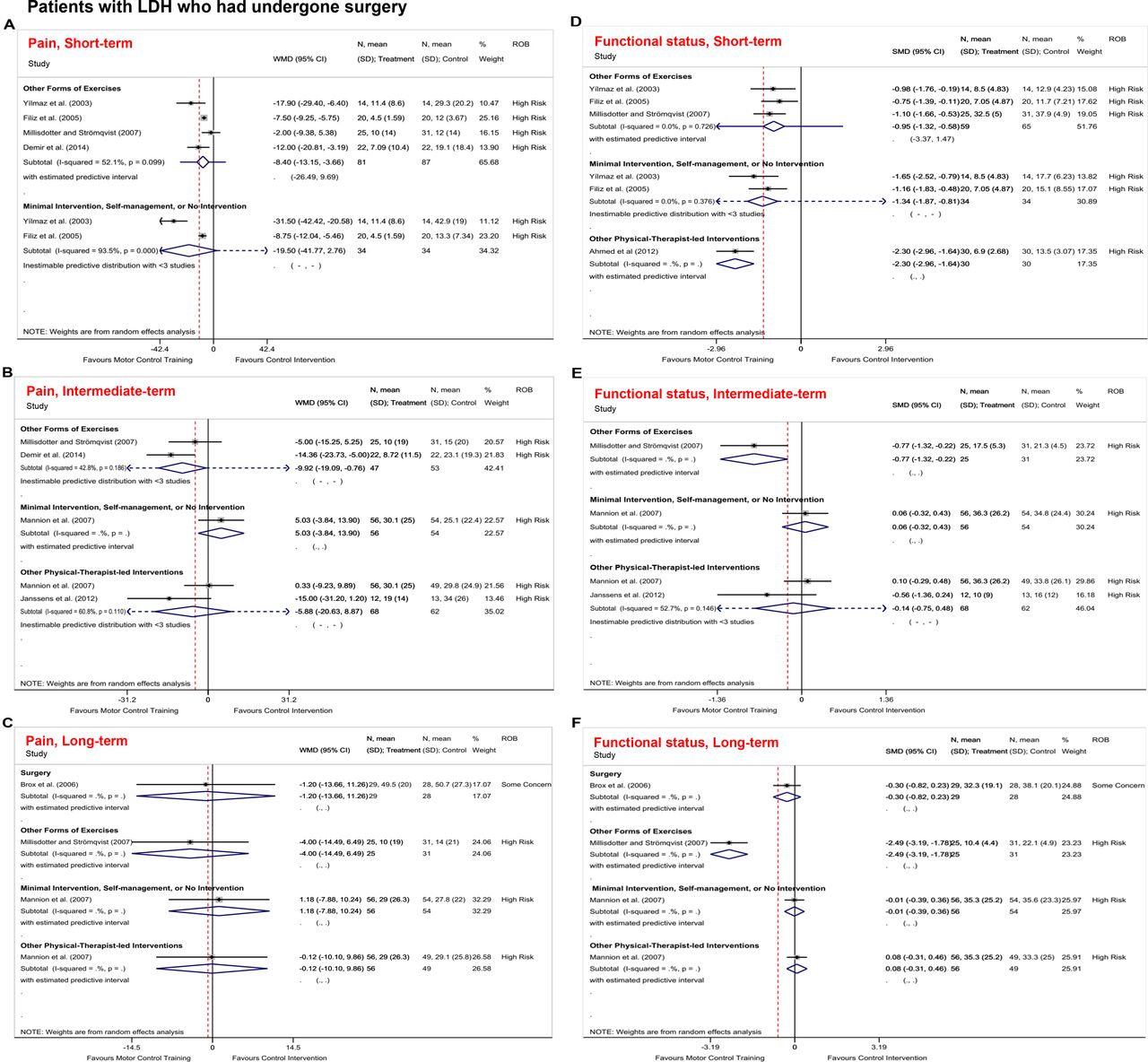
Forest plots of comparisons in patients with lumbar disc herniation (LDH) who had undergone surgery. (A) Pain at short-term, (B) pain at intermediate-term, (C) pain at long-term, (D) functional status at short-term, (E) functional status at intermediate-term and (F) functional status at long-term. Pain is presented as weighted mean difference (WMD) and functional status is expressed as standardised mean difference (SMD). Whenever a minimum of three studies were available for each comparison, the 95% prediction intervals were also estimated.
Patients who did not undergo surgery
MCT versus other physical therapist-led interventions
Pain (n=2)—at short-term, low-certainty evidence from two trials35 36 suggested that MCT produces large, clinically and statistically significant pain relief than electrotherapy (ie, transcutaneous electrical nerve stimulation) in patients with symptomatic (MD −28.85, 95% CI −40.04 to −17.66, participants=69; figure 2A and table 2).
Back-specific functional status (n=2)—low-certainty evidence suggested that MCT results in a large statistically and clinically better effect than transcutaneous electrical nerve stimulation (TENS) at short-term (SMD −1.98, 95% CI −2.57 to −1.40, participants=69; figure 2D and table 2).35 36
MCT versus other forms of exercises
Pain (n=3)—one high risk of bias study43 indicated that land-based MCT does not result in greater pain relief during activity than water-based MCT at short-term (MD 22.33, 95% CI −6.36 to 51.02, participants=23). At intermediate-term and long-term, another study52 found statistically significant but not clinically meaningful differences between MCT and general exercise for pain intensity in patients with symptomatic LDH (intermediate-term: MD −7.30, 95% CI −14.38 to −0.22, participants=63, figure 2B and table 2; long-term: MD −8.20, 95% CI −13.75 to −2.65, participants=63; figure 2C and table 2).
Back-specific functional status (n=3)—at short-term, intermediate-term and long-term, high risk-of-bias two studies52 53 reported that MCT results in not clinically meaningful effect compared with other forms of exercises (short-term: SMD 0.21, 95% CI −0.51 to 0.93, participants=30, figure 2D and table 2 53; intermediate-term: SMD 0.04, 95% CI −0.46 to 0.53, participants=63, figure 2E and table 2 52; long-term: SMD −0.83, 95% CI −1.35 to −0.31, participants=63, figure 2F and table 2).52 In addition, one study43 suggests that land-based MCT does not provide greater clinically meaningful improvement in back-specific functional status than water-based MCT at the short-term (SMD 0.37, 95% CI −0.46 to 1.20, participants=23).
MCT versus surgery (n=0)
No studies were identified which examined this comparison.
MCT versus minimal intervention, self-management or no intervention (n=0)
No studies were identified which examined this comparison.
None of the differences were found to be clinically relevant with the exception of MCT versus other TENS for pain and functional status at short-term.
Patients who had undergone surgery
MCT versus other forms of exercises
Pain (n=4)—very low-certainty evidence suggested that MCT compared with other forms of exercises significantly improves pain intensity at short-term (MD −8.40, 95% CI −13.15 to −3.66, participants=168; figure 3A and table 2).44–46 48 However, the results were clinically inconclusive at intermediate-term (MD −9.92, 95% CI −19.09 to −0.76, participants=100; figure 3B and table 2)44 48 and long-term (MD −4.00, 95% CI −14.49 to 6.49, participants=56; figure 3C and table 2).48
Back-specific functional status (n=3)—at short-term and intermediate-term, low-certainty evidence suggested that MCT was better than other forms of exercises, but the results were clinically inconclusive (short-term: SMD −0.95, 95% CI −1.32 to −0.58, participants=124, figure 3D and table 2 45 46 48; intermediate-term: SMD −0.77, 95% CI −1.32 to −0.22, participants=56; figure 3E and table 2).45 46 48 However, one study48 reported that MCT results in clinically significant effect at long-term (SMD −2.49, 95% CI −3.19 to −1.78, participants=56; figure 3F and table 2).
MCT versus other physical therapist-led interventions
Pain (n=2)—at intermediate-term, very low-certainty evidence suggested MCT has a similar benefit to other physical therapist-led interventions (ie, mixed techniques; MD −5.88, 95% CI −20.63 to 8.87, participants=130; figure 3B and table 2).37 39 However, the authors did not present their treatment protocols in detail. Moreover, one high risk of bias study37 showed that MCT does not provide clinically and statistically significant improvement compared with other physical therapist-led interventions at long-term (MD −0.12, 95% CI −7.88 to 10.24, participants=105; figure 3C and table 2).
Back-specific functional status (n=3)—one high risk of bias study38 showed that MCT results in a large statistically and clinically functional improvement than other physical therapist-led interventions at short-term (SMD −2.30, 95% CI −2.96 to −1.64, participants=60; figure 3D and table 2). Inconclusive results regarding functional improvement were found at intermediate-term (SMD −0.14, 95% CI −0.75 to 0.48, participants=130; figure 3E and table 2)37 39 and long-term (SMD 0.08, 95% CI −0.31 to 0.46, participants=105; figure 3F and table 2).37
MCT versus surgery
Pain (n=1)—one risk of bias study50 reported that surgery does not provide greater pain relief compared with MCT at long-term in patients with a history of previous surgery for disc herniation (MD −1.20, 95% CI −13.66 to 11.26, participants=57; figure 3C and table 2).
Back-specific functional status (n=1)—at long-term, one some concern risk-of-bias study50 reported that surgery does not have clinically significant improvement in functional status compared with MCT (SMD −0.30, 95% CI −0.82 to 0.23, participants=57; figure 3F and table 2).
MCT versus minimal intervention, self-management or no intervention
Pain (n=3)—very low-certainty evidence suggested that at short-term, MCT results in clinically important pain relief compared with minimal intervention, self-management or no intervention; however, the results were inconclusive (MD −19.50, 95% CI −41.77 to 2.76, participants=68; figure 3A and table 2).45 46 However, at intermediate-term and long-term, the findings demonstrated that MCT results in non-meaningful pain reduction compared with minimal intervention, self-management or no intervention (intermediate-term: MD 5.03, 95% CI −3.84 to 13.90, participants=110, figure 3B and table 2 37; long-term: MD 1.18, 95% CI −7.88 to 10.24, participants=110; figure 3C and table 2).37
Back-specific functional status (n=3)—very low-certainty evidence suggested that MCT provides statistically and meaningfully better improvement in functional status compared with minimal intervention, self-management or no intervention at short-term (SMD −1.34, 95% CI −1.87 to −0.81, participants=68; figure 3D and table 2).45 46 No meaningful functional improvement was found in favour of MCT at intermediate-term (SMD 0.06, 95% CI −0.32 to 0.43, participants=110; figure 3E and table 2).37
Secondary outcomes
Muscle endurance was assessed in two studies,43 45 quality of life in three studies,43 44 47 functional tests in three studies47 49 50 and return to work in three studies.44 45 50 The results for the secondary outcomes suggest considerable controversy about the effectiveness of MCT compared with control intervention in patients with LDH (online supplemental appendix 6). Moreover, at short-term, three studies,35 36 48 and at intermediate-term and long-term one study48 reported that no adverse events related to MCT were observed within the period studied. Other studies did not report MCT-related adverse events. For comparison interventions, only one study reported two wound infections among 23 patients who had undergone surgery.50
Publication bias
It was not possible to examine publication bias for most of the comparisons owing to the paucity of data. The preliminary analyses using Egger’s graphs do not suggest considerable publication bias among the selected comparisons, but this cannot be ruled out (online supplemental appendix 8).
Discussion
We investigated the effectiveness of MCT compared with other interventions in patients with symptomatic LDH. The certainty of the evidence was low that MCT can decrease pain and improve functional status compared with TENS at short-term. However, the robustness of the findings was not confirmed through the sensitivity analysis (online supplemental appendix 7). MCT can clinically beneficially improve functional status compared with traditional/classic general exercises at long-term in patients who had undergone surgery. Compared with minimal intervention, self-management or no intervention, MCT can also lead to clinically meaningful reduction in pain at short-term in patients with LDH and surgery. However, the certainty of the evidence was very low, so we have very little confidence in these effect estimates. Therefore, future clinical trials are likely to have an important impact. Most, if not all, clinical trials included had major methodological pitfalls.
It is important to mention that the included studies used various forms of MCT in those patients with LDH. For instance, the number of treatment sessions, frequency and the number of muscles which were trained were significantly different across the selected studies. In addition, many studies did not progress their training programmes to more functional and complex activities involving the muscles of the trunk and limbs, which is fundamental in a complete MCT programme. Therefore, it is questionable whether the effect of MCT might not be different if applied and examined in a uniform manner, not to mention that this introduced a large degree of clinical heterogeneity among the included studies. Ideally, we would have liked to have conducted subgroup analyses to explore the differences between the different types of comparisons; however, there were too few studies in order to allow for a meaningful comparison. Nevertheless, while caution should be urged in drawing conclusions from indirect comparisons, the magnitude of the effect would appear to be similar for the different types of comparisons, suggesting no significant difference between the results of studies included in each subgroup. Moreover, for ‘other forms of exercises’, similar conclusions can be drawn.
Comparison with other reviews
The finding of this study agrees with the previous reviews63–65 which showed that non-surgical treatments did not yield better effects than surgical treatments in patients with LDH, especially at long-term follow-up. However, we should bear in mind that our study focused on MCT only to provide a thorough understanding of the effectiveness of this exercise and the small number of homogeneous studies did not permit us to collate conclusive evidence about MCT for patients with symptomatic LDH. Furthermore, notwithstanding a published review16 reporting that MCT is more effective than no treatment for reducing pain intensity at short-term follow-up, our meta-analysis suggests that MCT did not produce greater pain relief in patients who had undergone surgery than minimal intervention, self-management or no intervention (online supplemental appendix 9).
Implications for clinicians
Our findings suggest that MCT as a stand-alone treatment may not produce satisfactorily meaningful pain relief and improved function, which is consistent with previous clinical guidelines.66 In that regard, it is important to consider adverse events, which were evaluated in only two trials and used unclear methodology. In general, it would appear that exercise for LBP may result in mild increase in back pain and muscle soreness, but is essentially safe67 (online supplemental appendix 10). Therefore, clinicians treating patients with LDH can safely prioritise exercise such as MCT and expect short-term improvements in pain and function if patients have not had surgery, and long-term gains in patients who have had surgery. MCT should be done in five steps including segmental spinal stabilisation exercise (eg, abdominal drawing-in manoeuvre in supine), non-functional spinal dissociation exercise (eg, abdominal drawing-in manoeuvre in quadruped with alternative arm and leg raises), functional spinal dissociation exercise (eg, wall squatting with abdominal drawing-in manoeuvre), segmental movement control exercise (eg, half circle in side-lying with abdominal drawing-in manoeuvre) and whole-body coordination (eg, standing wood chop/chop and lift with abdominal drawing-in manoeuvre).68
Limitations
First, the most important limitation is the limited number of high-quality trials for each comparison and the uncertainty about the impact of publication bias. Therefore, these results are inconclusive and should be interpreted with caution. Moreover, extraction of effect data was not possible for several trials.47 49 51 Second, since the number of studies in each subgroup was too small, we did not use quantile-quantile plots, and kurtosis and skewness coefficients of the extracted data to assess the normality assumption. Hence, we only calculated the mean/SD ratio25 and justified the normality assumption by the central limit theorem.
Recommendations for future research
Larger and high-quality trials are necessary to improve the certainty of evidence for using MCT in adults with LDH. Future trials should consider an adequate strategy to balance baseline covariates and a detailed description of random sequence generation and allocation concealment. Furthermore, the sample size in most of the included trials was not defined a priori, so future studies require calculating sample size based on the primary outcome(s) and the probability of attrition rate. Finally, it is highly desirable that future studies provide a full description of the MCT programme and its progression protocol using a valid reporting exercise intervention guideline, such as the 16-item Consensus on Exercise Reporting Template in order to evaluate its external validity.69
Conclusion
In patients with symptomatic LDH, there is very low evidence suggesting that MCT produces clinically meaningful improvement in pain and function compared with TENS in clinical practice at short-term in patients with LDH and no surgery. However, the robustness of the findings for pain relief was not confirmed. MCT improved function compared with traditional/classic general exercises at long-term in patients who had undergone surgery. Qualitative synthesis of the results showed that MCT may result in a faster return to daily activities compared with classical exercises and no exercise at short-term in patients who have had surgery. Future high-quality trials may change the certainty of evidence and estimates of each primary outcome’s effect.
What is already known
Motor control training is an active intervention programme that focuses on the recruitment and control of key muscles involved in protection of the lumbopelvic region.
Motor control training is more effective than no treatment for reducing pain intensity at short-term follow-up.
The quality of evidence related to the effectiveness of motor control training compared with other interventions has not been investigated in patients with symptomatic lumbar disc herniation.
What are the new findings
In patients who have symptomatic lumbar disc herniation and no surgery, motor control training is not statistically or clinically better than traditional/classic general exercises to improve function in the short-term.
There is low-certainty evidence suggesting that motor control training may be better than transcutaneous electrical nerve stimulation to improve pain and function in patients who have lumbar disc herniation and no surgery at short-term; however, the robustness of the results for pain was not confirmed in the sensitivity analysis.
In patients who have had surgery, motor control training is better than traditional/classic general exercises in the long-term for function, although studies have a high risk of bias.
At short-term, motor control training may result in a faster return to daily activities compared with classical exercises and no exercise in patients who have had surgery.
It seems unlikely that serious adverse events due to the intervention will occur.
Ethics statements
Patient consent for publication
Ethics approval
This systematic review was approved by the Institutional Review Board of Iran University of Medical Sciences with the support of the Iran national committee for ethics in biomedical research (IRB protocol number: IR.IUMS.REC.1400.880; https://ethics.research.ac.ir/EthicsProposalView.php?id=238210).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MP, SD, AK and MAM conceived and designed the study. AA conducted the search while MP adjudicated. MP, SD and MA performed the screening, study selection and data extraction. MP and SD analysed and interpreted the data with input from JAH and SMR. MP drafted the manuscript with input from JAH, SMR, MN and MAM. All authors have read and approved the final version.
Funding This study received funding from Iran University of Medical Sciences (grant number #1400-2-99-21936).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.