Article Text

Abstract
Objective Compare the effectiveness of primarily surgical versus primarily rehabilitative management for anterior cruciate ligament (ACL) rupture.
Design Living systematic review and meta-analysis.
Data sources Six databases, six trial registries and prior systematic reviews. Forward and backward citation tracking was employed.
Eligibility criteria Randomised controlled trials that compared primary reconstructive surgery and primary rehabilitative treatment with or without optional reconstructive surgery.
Data synthesis Bayesian random effects meta-analysis with empirical priors for the OR and standardised mean difference and 95% credible intervals (CrI), Cochrane RoB2, and the Grading of Recommendations Assessment, Development and Evaluation approach to judge the certainty of evidence.
Results Of 9514 records, 9 reports of three studies (320 participants in total) were included. No clinically important differences were observed at any follow-up for self-reported knee function (low to very low certainty of evidence). For radiological knee osteoarthritis, we found no effect at very low certainty of evidence in the long term (OR (95% CrI): 1.45 (0.30 to 5.17), two studies). Meniscal damage showed no effect at low certainty of evidence (OR: 0.85 (95% CI 0.45 to 1.62); one study) in the long term. No differences were observed between treatments for any other secondary outcome. Three ongoing randomised controlled trials were identified.
Conclusions There is low to very low certainty of evidence that primary rehabilitation with optional surgical reconstruction results in similar outcome measures as early surgical reconstruction for ACL rupture. The findings challenge a historical paradigm that anatomic instability should be addressed with primary surgical stabilisation to provide optimal outcomes.
PROSPERO registration number CRD42021256537.
- rupture
- systematic review
- rehabilitation
- anterior cruciate ligament
- randomized controlled trial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is uncertainty whether early surgical reconstruction or rehabilitation with optional surgical reconstruction of ACL rupture yields better functional and clinical outcomes.
Observational studies do not offer clear information whether early surgical reconstruction or primary rehabilitation with optional surgical reconstruction leads to better outcomes.
WHAT THIS STUDY ADDS
Through systematic review and meta-analysis, we found primary rehabilitation with optional surgical reconstruction results in similar patient-reported outcomes for ACL rupture as early surgical reconstruction.
Primary rehabilitation with optional surgical reconstruction showed a positive trend for better radiological knee osteoarthritis outcomes, albeit with very low certainty of evidence. Early surgical reconstruction showed a positive trend for better meniscal outcomes, but with a low certainty of evidence.
This ‘living’ systematic review will update on a yearly basis as the evidence develops.
HOW MIGHT THIS STUDY AFFECT RESEARCH, PRACTICE OR POLICY
Current treatment recommendations and guidelines regarding ACL patients without serious concomitant injuries should be revised to a ‘stepped care approach’ with a primarily rehabilitation focused treatment approach as first line treatment.
Randomised controlled trials with longer follow-ups are necessary to reach firm conclusions about the development of adverse outcomes, such as posttraumatic joint damage. Recent advancements in ACL surgical techniques need to be tested in high-quality randomised controlled trials.
Introduction
Anterior cruciate ligament (ACL) injury is one of the most common and serious knee injuries, with an annual incidence of 0.03% in the general population and 0.15–3.67% in professional athletes.1–3 ACL injuries are associated with marked individual4–12 and socioeconomic burden13–16; optimising recovery is pertinent. The patient and/or clinician stand point determines the outcome of interest.17 This may be prevention of joint osteoarthritis and secondary meniscal damage, return to sport rate and time to return, athletic performance, improvement of quality of life and cost-effectiveness as all have their relevance and this spectrum needs to be considered in clinical practice and research.
There has been debate on whether management should be primarily surgical (ie, surgical reconstruction soon after injury) versus primarily rehabilitative (with the option of later reconstruction in the case of persistent instability).17–20 To date, this debate has not been informed by high-quality systematic review. Accordingly, the quality of evidence in the underlying randomised controlled trials (RCTs) available to previous reviews of the topic21–25 could not document a superiority of one approach versus another. Furthermore, new RCT data will come to light over time to add to the evidence base for specific outcomes and subgroups. Living systematic reviews26 are a relevant methodological approach for when one can expect the evidence based for a spectrum of outcomes to mature over time.
The aim of this living systematic review is to examine the comparative effectiveness of primarily surgical versus primarily rehabilitative treatment strategy after ACL rupture. To comprehensively capture the multidimensional facets of this question, we consider patient-reported outcome measures and other outcome measures in different individual, social and economic dimensions.
Methods
This review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines27 28 and was prospectively registered in PROSPERO. Data and statistical code are found in an online repository (https://doi.org/10.17605/OSF.IO/Q69UV).
Patient involvement
There was no patient or public involvement in creating this systematic review.
Administration, dissemination and updating the living systematic review
This review is hosted on the website of the Hochschule für Gesundheit (University of Applied Sciences), Bochum, Germany. We plan to update this living systematic review every year for a minimum of 6 years. We will screen the literature every year to identify new data that may alter our conclusions and recommendations. When new data become available, we will update the analysis and present the updated findings at the website of the Hochschule für Gesundheit (University of Applied Sciences), Bochum, Germany (https://bit.ly/3ogGYIe).
Search strategy
An electronic database search of MEDLINE, EMBASE, CINAHL, Web of Science Core Collection, CENTRAL, SPORTDiscus was conducted (online supplemental appendix 1). Searches were performed from their inception to June 2022. The search terms were identified after preliminary searches of the literature and by comparing them against a previous systematic review.21 No language or any other restrictions were applied to the database searches.
Supplemental material
Unpublished and ongoing studies were searched via the US National Institutes of Health (https://clinicaltrials.gov/), EU Clinical Trial Register (https://www.clinicaltrialsregister.eu/), DRKS—German Clinical Trials Register (https://www.drks.de), ISRCTN registry (https://www.isrctn.com/), Australian New Zealand Clinical Trials Registry (https://www.anzctr.org.au) and the Netherlands Trial Register (https://www.trialregister.nl/).
A search for prior systematic reviews published was completed via the Cochrane Database of Systematic Reviews (search terms: ‘anterior cruciate ligament’; limits: none) and GoogleScholar (search terms: ‘anterior cruciate ligament’ ‘systematic review; limits: first 10 pages). Forward and backward citation tracking of included articles was performed (TS and TB). Two independent reviewers (NS and TB) evaluated all trials against prespecified inclusion/exclusion criteria based on title/abstract and subsequently full text. Disagreements were settled through discussion among the reviewers (NS and TB). A third reviewer (TS) adjudicated any disagreement.
Inclusion and exclusion criteria
Inclusion criteria followed the Participants, Interventions, Comparators, Outcomes, Study design framework.27 Participants were those with ACL rupture of any age. We excluded studies that included patients with inflammatory arthropathy or end-stage osteoarthritis (grade 4 Kellgren and Lawrence)29 as well as studies that focused on the management of ACL injuries with unstable longitudinal meniscus tears. Interventions were reconstructive surgery of the ACL with any method of reconstruction or type of reconstruction technique. Comparators were any type of rehabilitation (eg, physiotherapy, exercise training, bracing, education) with or without optional delayed reconstruction of the ACL. Primary outcome measures were self-reported knee function, radiological osteoarthritis and meniscal injuries at all follow-ups. Secondary outcomes were adverse events, health-related quality of life, return to activity or level of sports participation, functional assessments, knee stability and objective measures of muscle strength. Study designs were required to be parallel randomised (individual, cross-over or cluster design) controlled trials (RCTs). Quasi-RCTs and non-RCTs were excluded given they do not offer an unbiased estimate of the effect size.30
Data extraction
Study information was extracted independently by two authors (NS and TS), with disagreement settled via discussion. If disagreement could not be settled, a third adjudicator (JZ) decided. Reviewers were not blinded to information regarding the authors, journal or outcomes for each article reviewed. The following information was extracted: author, year, journal, funding, conflict of interest, study type, sample size, age, sex, type of intervention, body mass index, sports participation while injured, setting, description of intervention and comparator, follow-up time points and outcome measure scores. We used the following categories to characterise the different follow-up time points: short-term (≤1 year), medium-term (>1–3 years) and long-term (>3 years). If multiple follow-ups existed within each timeframe, we extracted the follow-up closest to 1 year for short term, 3 years for intermediate term and 10 years for long term. When two time points were equally close to these follow-ups, we extracted the one that was furthest from baseline. Data for the main results were extracted either as mean and SD (post-treatment) or the number of events (n) and non-events (N) where applicable. If a study report did not report relevant data for extraction, the corresponding author was contacted on two occasions over a 2-week period.
Risk of bias assessment and GRADE
Risk of bias (RoB) was assessed via the Cochrane Risk of Bias Tool V.2.0.31 An overall RoB judgement was made for one subjective outcome (patient-reported knee score) and one objective outcome (meniscal surgery or radiological confirmed knee osteoarthritis). Assessment of RoB was based on results of the last follow-up time point of the individual study. Two independent assessors (MH and TS) performed the assessment. Disagreements were resolved through discussion or by a third reviewer (JZ).
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of evidence (online supplemental appendix 4).32 33 Indirectness was judged by the approach by Schüneman.5 RoB was graded the following way: down grade 1 level: 50% high RoB and down grade 2 levels if 75% high RoB. We used the criteria from Confidence in Network Meta-Analysis (CINeMA)4 to evaluate imprecision, inconsistency and publication bias. We chose these criteria because the use of CIs, prediction intervals (PI) and a ‘region of equivalence’ provide a more clinically informative and robust approach to heterogeneity.32 33 Notably, CINeMA is not restricted to network meta-analysis and overcomes a number of the limitations of other approaches, such as, for example, the assessment of inconsistency: many authors rely solely on an I2 value to assess heterogeneity, yet this is incorrect .34 The assessment of publication bias based solely on statistical techniques or assessment of funnel plots is another fallacy that is still often done.32 35 For the imprecision and inconsistency, we downgraded by one level if there were some concerns and two levels if there were major concerns. Indirectness was downgraded by one level if deemed serious and two levels if deemed very serious. We downgraded one level if publication bias was suspected. As-treated-comparisons started with a rating of ‘low’ as we deemed this data as observational and not as randomised.32 The evaluation of all ratings started at a high level of certainty given guidelines for meta-analyses, including RCTs only. Two authors (TS and MH) performed the GRADE assessment.
Statistical analysis
For data analysis, we created two categories of comparators: (early) reconstructive surgery of the ACL with postoperative rehabilitation (‘early surgery’) and rehabilitation with or without elective reconstructive surgery of the ACL (‘primary rehabilitation’). We also analysed the ‘as treated’ (ie, per protocol) data in three groups: ‘early surgery’, ‘delayed surgery’ and ‘non-operative’. If more than one outcome measure was reported for each type of outcome in the same study, only one was considered for further analysis. We prioritised scales if they measured the primary outcome in the trial to maximise statistical power. Data transformations are described in online supplemental appendix 5.
Effect size measures were standardised mean difference (SMD)32 or mean difference for continuous outcomes and OR with corresponding 95% shortest credible intervals (CrI) for meta analyses or 95% frequentist CIs for dichotomous outcomes.36 SMD effect size was interpreted as: small (0.2), medium (0.5) or large (0.8).37 We used the International Knee Documentation Committee questionnaire (IKDC) for patient-reported knee scores as a measure of the minimally clinically important difference (MCID). We used the following values for the follow-up time points38: short- (MCID: 16.7 points), medium term (MCID: 17.0 points), long term (MCID: 17.0 points). Back-transformation of SMDs was performed to a common scale.32 We also backtransformed the OR by using the median comparator group risk as the assumed comparator risk.32 We also created synthetic effect sizes for all available time points to compute a summary measure for all time points combined if permissible by the data.39 We performed our analysis with a correlational value of ρ=0.5 and sensitivity analysis with ρ=(0.6, 0.7).
For meta-analysis, we used pairwise Bayesian random effects meta-analysis. Bayesian meta-analysis can be more efficient than frequentist methods if the number of studies is small (≤5 studies) and heterogeneity is present.40–43 This is the case if empirical prior distributions for variance of the true effects (τ²) are available, as this allows a better estimation of τ² when few studies are available.43 Prespecified prior distributions are described in online supplemental appendix 5. As treated data were analysed via Bayesian random effects network meta-analysis . For estimation details, please see online supplemental appendix 5.
Publication bias and small study effects were assessed statistically via funnel plots if at least 10 studies were included in the meta-analysis.44 Non-statistical assessment of publication bias was performed as described by our GRADE criteria (online supplemental appendix 4). Pending the number of available studies (≥10 trials required for meta-regression), we performed subgroup analysis based on prespecified covariates.39 We performed sensitivity analysis for all prior distributions and for self-reported return to activity (long term), as the latter was reported in both studies with medians.45 All calculations and graphics were performed with the R statistical computing environment,46 and the R packages Meta,47 Bayesmeta,48 Metafor,49 Netmeta,50 metamedian and gemtc.51
Results
We identified 9514 reports through database searching and manual search of reference lists of relevant literature reviews. After removing duplicates and screening titles and abstracts of all remaining unique reports, 104 full-text reports were assessed for eligibility. We included three studies52–54 with nine study reports (figure 1).52–60 Literature sources and reasons for exclusion of ineligible studies/reports are reported in online supplemental appendix 2.

PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Unpublished and ongoing trials
We identified three ongoing trials potentially relevant for this review.13 61 62 We provide further information concerning these trials in online supplemental appendix 3.
Study characteristics
The characteristics of the three included studies are shown in table 1. Sample size ranged from 32 to 167 participants (mean: n=106; total: n=320). Mean (SD) age of all participants was 29.5 (7.05) years, whereas body mass index was 24.4 (3.4) kg/m² based on two studies.53 54 On average, 93% injured their ACL while performing their chosen sport. This result is based on two studies.53 54 All trials employed active rehabilitation. One trial54 employed evidence-based, progressive rehabilitation, one trial53 based its rehabilitation on Dutch rehabilitation guidelines and one trial used52 a progressive rehabilitation programme.
Study characteristics
RoB and GRADE assessment
Two study outcomes were rated as low RoB overall. The other study outcomes were either rated with some concerns or a high RoB overall (online supplemental appendix 6). The certainty of the evidence was rated for meta-analytic outcomes as low or very low overall and as high to very low for individual study outcomes (online supplemental appendices 7 and 8). Main reasons for downgrading the evidence were RoB, inconsistency and imprecision. We did not grade down due to publication bias in accordance to our prespecified criteria. Indirectness was not downgraded as this review followed strict population, intervention, comparator and outcome eligibility criteria.
Data handling and synthesis
Three reports (two studies)53–55 only reported precision of the estimates as 95% CIs, which we converted to SD with established formulae. Two studies52 54 reported return to activity data as median (IQR), which we transformed to mean (SD). Two reports (one study)54 55 reported primary outcomes as mean difference (95% CI). The authors of the study provided the data for this outcome. The authors of one report56 confirmed our queries regarding sample size. All outcomes are reported for meta-analytic summaries and individual study outcomes in tables 2 and 3 and figures 2–4. The secondary outcome muscle strength could not be assessed as this was not reported in any trial. All data, calculated effect sizes and as-treated analyses are reported in online supplemental appendices 9, 10 and 12.

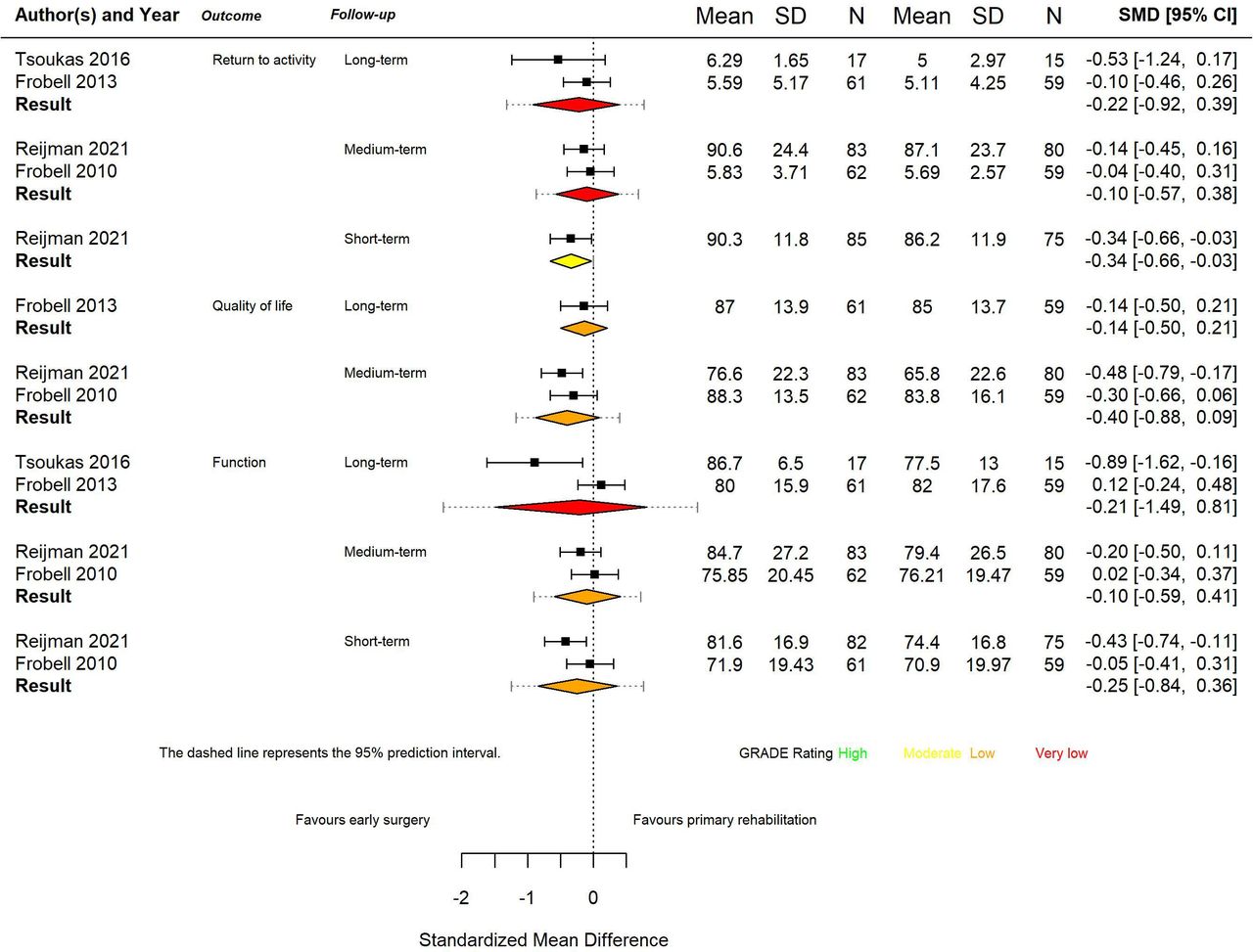
Overview of continuous outcomes for the comparison early surgery versus rehabilitation with optional surgery. The used software sets the limit automatically to the 95% CrIs and not the 95% prediction intervals (dashed lines). As the highest value of a 95% CrI is 0.81 it sets the positive limit to 1.0 although the prediction interval goes further than that. CrI, credible interval.

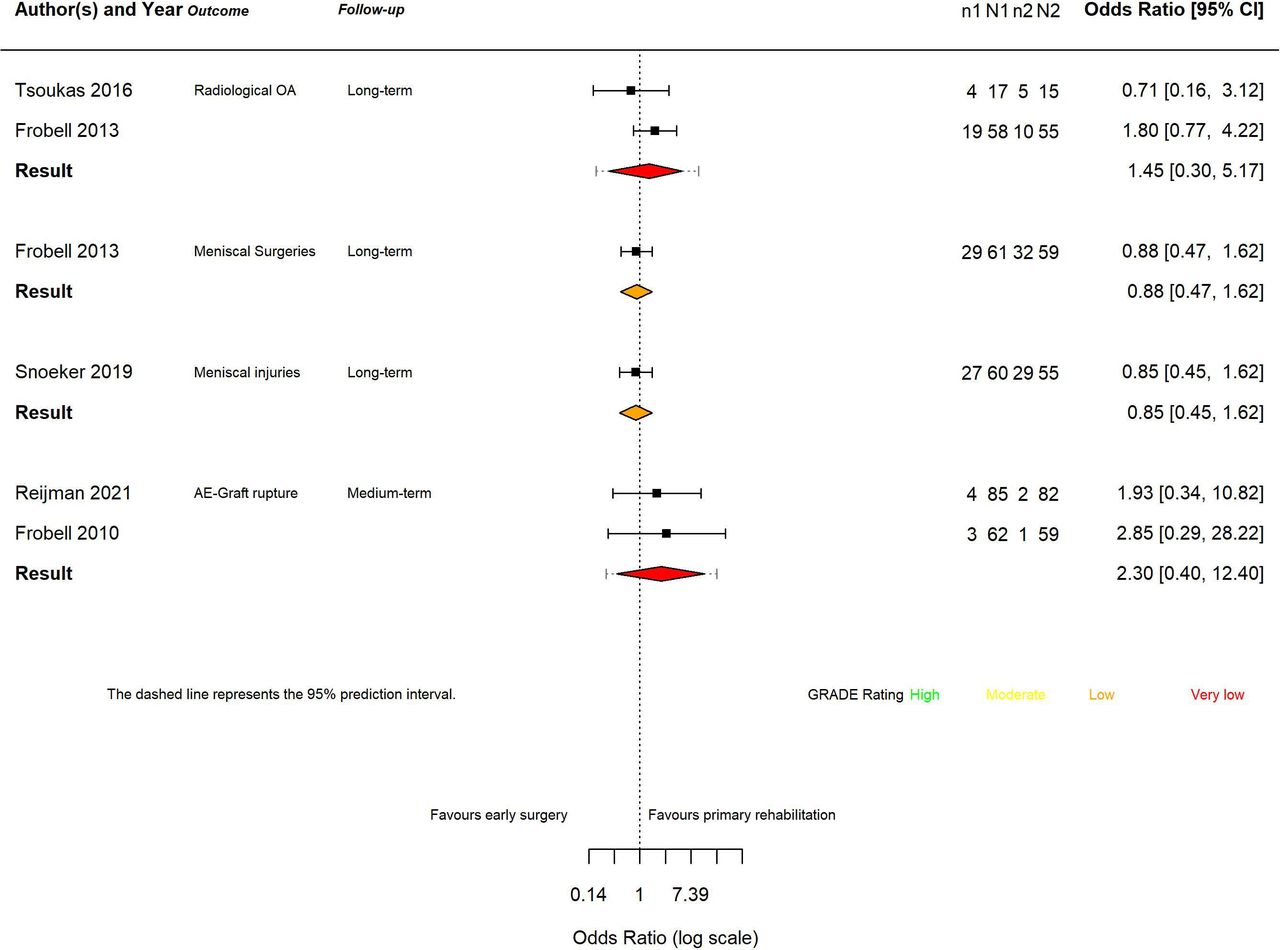
Overview of dichotomous outcomes for the comparison early surgery vs rehabilitation with optional surgery.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
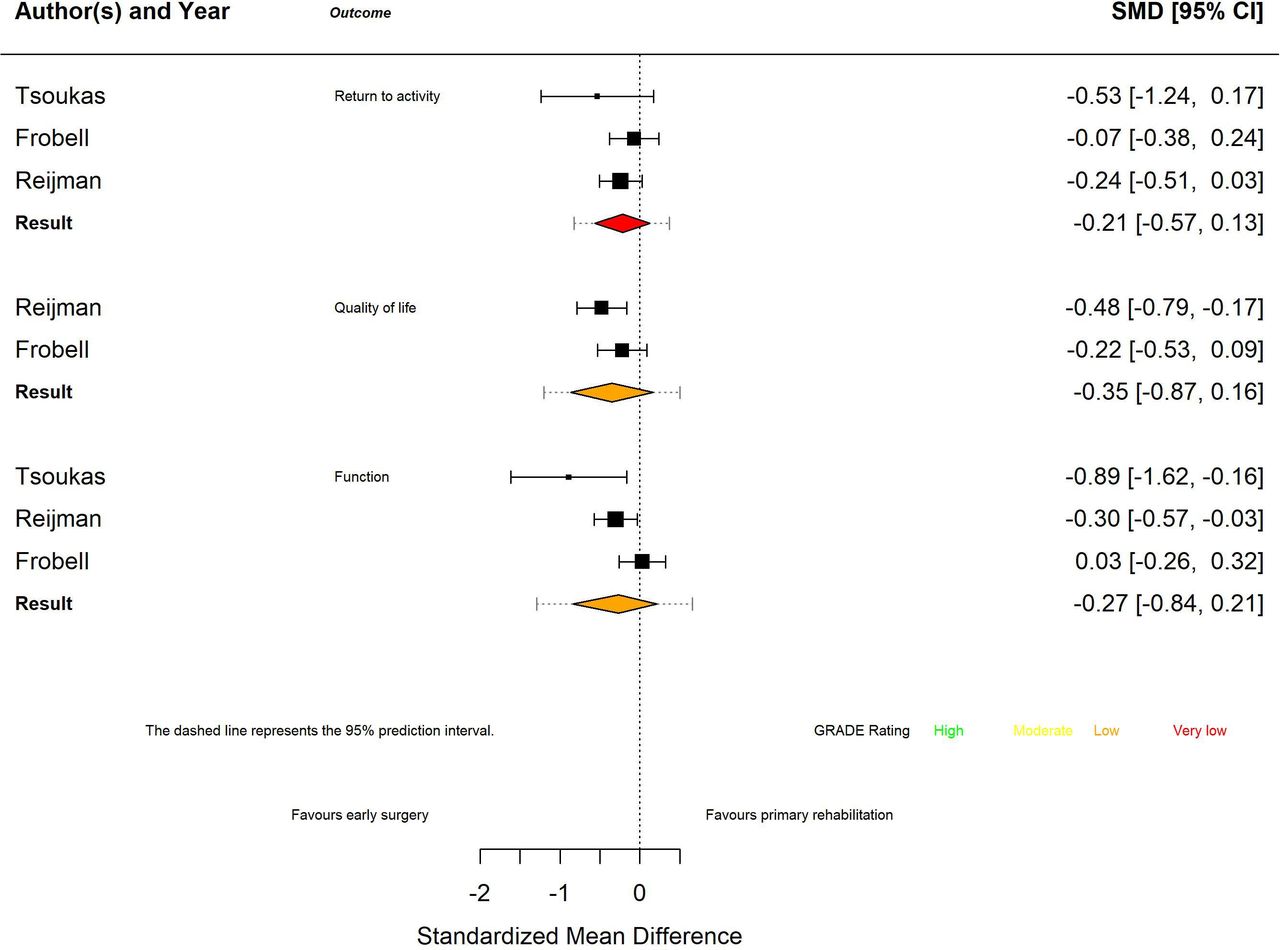
Overview of continuous outcomes for the comparison early surgery versus rehabilitation with optional surgery for all time points combined. SMD, standardised mean difference.
Certainty of Evidence (GRADE approach) of meta-analytic outcomes
Certainty of evidence (GRADE approach) of individual study outcomes
Self-reported knee function
Three studies with four reports52–55 were included. Meta-analysis was performed for short-term,53 54 medium-term53 54 and long-term follow-up.52 55 In the short-term (SMD: −0.25; 95% CrI −0.84 to 0.36; 95% PI −1.25 to 0.76; two studies; n=288; GRADE: low) and medium-term (SMD: −0.10; 95% CrI −0.59 to 0.41; 95% PI −0.91 to 0.72; two studies; n=288; GRADE: low) showed no statistical difference between the two groups with low certainty of evidence. Estimated raw mean difference was −4.21 (95% CrI −14.27 to 6.07) and −2.65 (95% CrI −15.94 to 10.89) points on the IKDC scale (0–100 points), which did not reach clinical meaningfulness (MCID: 16.7 points and 17 points). For long-term follow-up (SMD: −0.21; 95% CrI −1.49 to 0.81; 95% PI −2.28 to 1.58; two studies; n=152; GRADE: very low), there was no statistical between group difference for self-reported knee function with very low certainty of evidence. Estimated raw mean difference was −0.96 (95% CrI −5.79 to 3.95) points on the IKDC scale, which did not reach clinical meaningfulness (MCID: 17 points). Sensitivity analyses using as-treated data for the non-operative control group from Frobell et al 55 revealed similar effects (online supplemental appendix 12). Analysis of all time points combined yielded also no difference between groups with low certainty of evidence (SMD: −0.27; 95% CrI −0.84 to 0.21; 95% PI −1.29 to 0.66; three studies; n=309; GRADE: low). The estimated raw mean difference was −5.07 (95% CrI −15.70 to 3.99) points on the IKDC scale and was not clinical meaningful (MCID: 17 points).
Meniscal injury
Only one report examined this outcome.63
Results from single studies
One study report63 reported on development of new (or worsening) meniscal damage after baseline or index surgery via MRI. Early surgery showed no effect compared with primary rehabilitation at long-term follow-up (OR: 0.85; 95% CI 0.45 to 1.62; GRADE: low) with a low level of certainty.
Radiological knee osteoarthritis
Two studies52 55 were included. We estimated no statistical effect at long-term follow-up (OR: 1.45; 95% CrI 0.30 to 5.17; 95% PI 0.18 to 10; two studies; n=152; GRADE: very low) with a very low level of certainty. Transformation of the OR into a risk difference with an assumed prevalence of 25% in the rehabilitation group gives a number fewer than 1000 of −72 (95% CrI (144 to −384)) at a very low level of certainty. Assuming that 250 (25%) patients of 1000 patients develop knee osteoarthritis (OA) after being treated with primary rehabilitation then 72 more patients (322 patients) treated with early surgery will develop knee osteoarthritis with a 95% CrI (144 patients less, 384 patients more) with a very low level of certainty. Sensitivity analyses using as-treated data for the non-operative control group from Frobell et al 55 revealed similar effects (online supplemental appendix 12).
Health-related quality of life
Two studies53 54 were included. We estimated no effect for early surgery compared with primary rehabilitation at medium-term follow-up (SMD: −0.40; 95% CrI −0.88 to 0.09; 95%PI −1.18 to 0.40; two studies; n=288; GRADE: low) with a low level of certainty. The converted raw mean difference of −5.91 (95% CrI −13.05 to 1.32) points on the SF-36 (mental health score, 0–100 points) was likely not clinically meaningful (≥ 10 points).64 Analysis of all time points combined gave evidence of no effect (SMD: −0.35; 95% CrI −0.87 to 0.16; 95% PI −1.20 to 0.50; two studies; n=288; GRADE: low) with a low level of certainty. The converted raw mean difference of −5.01 (95% CrI −12.37 to 2.34) points on the SF-36 (mental health score, 0–100 points) was likely not clinically meaningful (≥ 10 points).
Results from single studies
One study55 reported no effect on health-related quality of life at long-term follow-up (SMD: −0.14; 95% CI −0.50 to 0.21; GRADE: low) with low level of certainty.
Self-reported return to activity
Four reports of three studies52–55 were included. Meta-analysis was performed for medium-term53 54 and long-term follow-up for postinjury activity level at the specific follow-up time points.52 55 At medium-term follow-up, there was no effect (SMD: −0.10; 95% CrI −0.57 to 0.38; 95% PI −0.87 to 0.68; studies=2; n=288, GRADE: very low) with very low certainty of evidence. Raw mean difference on the Tegner Scale (0–10 points) was −0.31 (95% CrI −1.80 to 1.19) points, which was not clinically meaningful (MCID: 1 point).65 No effect with very low certainty of evidence was also estimated for long-term follow-up (SMD: −0.22; 95% CrI −0.92 to 0.39; 95% PI −1.32 to 0.77; studies=2, n=152, GRADE: very low). Raw mean difference on the Tegner Scale was −0.75 (95% CrI −2.92 to 1.23) and cannot be considered clinically meaningful. Sensitivity analyses using as-treated data for the non-operative control group from Frobell et al 55 yielded no effect for early surgery in comparison to the non-operative group (SMD: −0.84; 95% CrI −2.56 to 0.87; 95% PI−3.36 to 1.67; studies=2; n=152, GRADE: very low) with a very low level of certainty. Raw mean difference on the Tegner Scale was 2.61 (95% CrI −2.67 to 7.90) and can likely be considered clinically meaningful but only with a very low degree of certainty. One should note that a sensitivity analysis with a meta-analysis of medians yielded lower values (median: 1.18, 95% CI −0.75 to 3.20) on the Tegner scale. Analysis of self-reported activity for all time points resulted in no effect (SMD: −0.21; 95% CrI −0.57 to 0.13; 95% PI −0.82 to 0.37; studies=2; n=152, GRADE: very low) between groups with a very low level of certainty. Raw mean difference on the Tegner Scale was −0.72 (95% CrI −1.92 to 0.42) and cannot be considered clinically meaningful.
Results from single studies
One study53 reported no effect at short-term on return to activity (SMD: −0.34; 95% CI −0.66 to –0.03; GRADE: moderate) with a moderate level of certainty.
Meniscal surgeries
Results from single studies
One study report55 reported on the number of patients with any meniscal surgery during the study, including those performed at baseline concomitant with index ACL reconstruction, and during follow-up up to 5 years, which showed no effect for primary surgery versus primary rehabilitation with a low level of certainty (OR: 0.88; 95% CI 0.47 to 1.62; GRADE: low). Transformation of the OR into a risk difference with an assumed prevalence of 51% in the rehabilitation group gives a number fewer than 1000 of 32 (95% CrI 181 to–119) with a low level of certainty. Assuming that 510 (51%) patients of 1000 patients develop or have a meniscal injury when undergoing primary rehabilitation then 32 less patients (478 patients) treated with early surgery will develop or have a meniscal injury with a 95% CrI (181 patients more, 119 patients less) with a low level of certainty.
Secondary outcomes
The secondary outcomes: adverse event (graft rupture), knee stability, patellofemoral cartilage thickness, leg hop–limb symmetry index and economic resource are displayed in tables 2 and 3 and in online supplemental appendix 9.
Funding and conflict of interest
One study53 was funded by a professional organisation. Another study54 had mixed funding of private or professional and governmental organisations. One study52 did not report their funding source. The authors declared no conflict of interest in two studies,52 53 whereas one study54 reported a conflict of interest.
Small study effects and publication bias
We did not suspect publication bias according to our criteria for GRADE. Small study effects and publication bias could not be statistically assessed because the number of studies were fewer than 10 studies.44
Subgroup analysis and meta-regression
Subgroup analysis and meta-regression were not feasible due to the low number of studies (ie, n<10).32
Sensitivity analyses
We performed sensitivity analyses with different priors for the between study variance (τ²) for meta-analytic outcomes (online supplemental appendices 12 and 13). This was done to check how sensitive the results were to different priors (prior beliefs about the distribution of τ²) for the between study variance. The findings did not change when different priors for τ² were used. The meta-analysis of medians led to markedly different outcomes for self-reported return to activity for the comparison early reconstruction versus non-operative treatment in the long term. Transformed raw mean differences were 2.61, (95% CrI −2.67 to 7.90) versus 1.18, (95% CI −0.75 to 3.20) points on the Tegner scale (0–10) for the sensitivity analysis.
Protocol deviations compared with PROSPERO registration
We added a meta-analysis of medians as a sensitivity analysis and added a meta-analysis of all timepoints combined to this work. We removed the outcome treatment failure (graft rupture vs surgical reconstruction) due to recommendations made by the reviewers as a graft rupture is an obvious and ‘unexpected/unwanted’ adverse event (or failure), while delayed ACL reconstruction in the rehabilitation group (in both studies) was an a priori expected and planned part of the treatment strategy.
Discussion
This is the first living systematic review and meta-analysis investigating the effects of primarily surgical versus primarily rehabilitative management for ACL injuries based on RCTs. Our analysis showed that there are no clinically relevant differences in most outcomes between early surgical reconstruction and primary rehabilitation with optional reconstruction. Radiological knee osteoarthritis showed a trend to slightly favour primarily rehabilitative treatment although at very low certainty of evidence. Meniscal damage showed a favourable trend for primary surgery in the long-term but at a low level of evidence.
Improving function
From IKDC or Knee Injury and Osteoarthritis Outcome Score (KOOS) scales, a highly clinically relevant improvement in function was shown for both treatments. Regardless of treatment modality examined, more than 90% of patients achieve MCID on the KOOS scale after 2 years.66 Furthermore, the mean values of the function scores excluding the KOOS-QoL value reach the threshold for the Patient Accepted Symptom State at the longest follow-up.66 67 Current evidence suggests that both early surgery and primary rehabilitation result in clinically meaningful improvements in long-term subjective knee function. Overall, our analysis showed that early ACL reconstruction did not result in improvements in function versus primary rehabilitation management with a low level of certainty.
Radiological osteoarthritis
Early reconstruction showed no protective effect on the development of post-traumatic osteoarthritis in either the primary or as-treated analysis at a very low level of certainty. Our estimates showed a trend with very low certainty of evidence, for primary rehabilitative therapy and/or delayed reconstruction to result in less cartilage loss. A result that is confirmed by Swedish ACL registry (cohort) data in a registry evaluation of 64 614 patients with ACL rupture.68 Overall, the protective effect on the development of knee osteoarthritis of an ACL reconstruction remains a point of debate.10 23 25 65 69 Prior authors reported no differences in knee osteoarthritis,24 70 or differences in rates of osteoarthritis development, depending on the degree of osteoarthritis71 or the length of the follow-up period,72 but these results are only based on observational studies. Fundamentally, our findings from RCTs challenge a historical paradigm73–75 that anatomic instability must be stabilised with surgery to prevent knee osteoarthritis.
The following mechanisms may in part explain these observations: (1) increased inflammation from the surgical procedure,76–78 (2) failure to accurately restore the exact contact points between the tibia and femur,79–82 (3) kinematic differences of ACL patients, which can be interpreted as avoidance behaviour83–88 (4) and premature early sports participation by patients who have undergone reconstructive surgery.89–91 Collectively, these mechanisms highlight that the development of post-traumatic osteoarthritis is a multifactorial complex process of interacting risk factors and thus prevention of degenerative cartilage damage by surgical or conservative treatment seems neither realistic nor possible.
Meniscal status and meniscal surgery
There is no statistical difference between early surgery and primary rehabilitation but with low certainty of evidence. Our analysis indicated that the observed differences were particularly due to the inferior results of the patients with delayed ACL reconstruction. Similar results with a low degree of certainty are found in the literature.12 23 An early ACL reconstruction in patients with functional instability might be recommended following the ‘as treated’ analysis results, especially as the ‘delayed surgery’ group showed a less favourable meniscal situation. There is no direct RCT evidence that patients with functional instability need to be stabilised. But it is a best practice recommendation92 to operate on these instable patients and it was a prespecified criterion in the investigated RCT. We suggest that in the case of functional instability of the knee, a surgical reconstruction of the knee is warranted.
Improving return to activity
In the medium term and long term, patients reported no effect between groups, but the certainty of evidence for these results is very low. The effect sizes were also not clinically meaningful. Widespread expert recommendations are that athletes with a high functional demand should undergo surgical treatment.92–94 However, the quality of evidence for such recommendations is very low according to our results. What is not currently available is RCT-level information on an extreme high level of sports participation (Tegner Score of 10). A return to knee-loading sports, even those with high rotational loads, is also described after a treatment approach of primary rehabilitation in a larger group of patients.95 96 Notably, although competitive athletes are successful in returning to their sport after ACL reconstruction,8 many of these athletes do not reach their preinjury level of performance.97 According to our analysis, one cannot unequivocally conclude that athletes are required to undergo early ACL reconstruction. Further RCTs need to be conducted to answer this question for an athletic population.
Patient-centred care
We observed no clinically meaningful differences between treatment approaches, and, thus, propose an individualised and patient-centred form of care. Depending on a patient’s medical situation (eg, concomitant injuries such as repairable meniscal tears, relevant cartilage injuries, other higher grade ligamentous injuries),53 54 98 individual anatomical differences (eg, the tibial slope, femoral morphology, alignment),92 99 100 functional demands in daily life or sports,92 an individualised primary treatment strategy should be determined as a ‘shared decision process’.101–103 For many patients with ACL injuries without serious concomitant injuries, a ‘stepped care approach’ with a primarily rehabilitation focused treatment approach seems appropriate, especially pertaining to cost-effectiveness57 58 and the avoidance of surgical risks.103 Functional instability, despite a high-quality exercise-based approach, determines the need for subsequent surgical treatment to minimise secondary joint damage.86 91 97 101 103 104 The task of future research will be to define valid predictors for an individual’s success or failure with primary non-surgical care to enable an evidence-based clinical decision-making process. One such example is the decision-making and treatment algorithm based on the Delaware-Oslo ACL Cohort Study, which certainly requires confirmatory studies.98 104 105 Furthermore, such a stepped approach requires health systems to provide the necessary financial resource for an adequate primary rehabilitative care.106 107
Limitations
This study is not without limitations. The low number of included studies still left uncertainties regarding the best approach for dealing with ACL ruptures. Furthermore, only one trial was of low RoB, which further undermined the certainty in the estimates. All RCTs included patients with complete ACL injuries, but the inclusion criteria regarding concomitant injuries were somewhat different in the individual trials. The applied surgical techniques were also different across the included trials, depending on the surgeon’s preference. Furthermore, the current data do not permit conclusions in favour or against primary surgical management for professional athletes. We also did not prespecify different MCIDs for other outcomes beyond self-reported knee function. The use of MCID for interpretation of outcomes is debated because it varies based on analytic methods, study populations, type of disease, baseline status, change in values and treatments and patient demographics. It should be interpreted with caution.38
Future directions
RCTs with longer follow-ups are necessary to allow robust conclusions about the development of adverse outcomes, such as post-traumatic joint damage. In the context of ACL surgery, anatomic surgical techniques (eg, double-bundle technique, anteromedial femoral tunnel drilling technique), extra-articular reconstructions such as those of the anterolateral ligament or even slope-reducing tibial osteotomies have become particularly established in recent years and need to be evaluated in RCTs in the future.108–110 Initial reviews here show partial benefits for individual outcomes, for example, of anatomical versus non-anatomical techniques.111 112 The same can be said for rehabilitation programmes as a lot of these do not follow current best practice recommendations.113 Future studies will need to address how these new surgical procedures (eg, slope reducing tibial osteotomies) compare to contemporary primary rehabilitation.17 106
Conclusion
We found very low to low certainty of evidence of no clinically relevant differences in most outcomes between early surgical reconstruction and primary rehabilitation with optional reconstruction. Early surgery showed a positive trend pertaining to a better meniscal status but with a low level of certainty of evidence. Rehabilitation with optional surgery showed a trend for an advantage regarding the avoidance of the development of radiological knee osteoarthritis. On the weight of the current evidence, indicating that early surgical ACL reconstruction is not beneficial for all patients, we propose an individualised, patient-centred form of care that discusses the potential treatment options with the patient.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank Dr. Clare Ardern for comments on the methodological approach in this work
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @PhysioMeScience, @PatrickOwenPhD, @belavyprof
Contributors Conceptualisation: TS, JZ, FD; data curation: TS, NS; formal analysis: TS; funding acquisition: NA. Investigation: TS, JZ, FD; methodology: TS, DB, TB, NS, MH; project administration: TS; resources: TS; software: TS; supervision: DB, PO, TB, WZ; validation: NA. Visualisation: TS; writing—original draft: TS, JZ, FD; writing—review and editing: all. Approved final manuscript: all.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. No funding was received to support this work.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.