Article Text

Abstract
Objective Synthesise evidence for effectiveness of rehabilitation interventions following ACL and/or meniscal tear on symptomatic, functional, clinical, psychosocial, quality of life and reinjury outcomes.
Design Overview of systematic reviews with Grading of Recommendations Assessment, Development and Evaluation certainty of evidence.
Data sources MEDLINE, EMBASE, CINAHL, SPORTDiscus and Cochrane Library.
Eligibility criteria Systematic reviews of randomised controlled trials investigating rehabilitation interventions following ACL and/or meniscal tears in young adults.
Results We included 22 systematic reviews (142 trials of mostly men) evaluating ACL-injured individuals and none evaluating isolated meniscal injuries. We synthesised data from 16 reviews evaluating 12 different interventions. Moderate-certainty evidence was observed for: (1) neuromuscular electrical stimulation to improve quadriceps strength; (2) open versus closed kinetic chain exercises to be similarly effective for quadriceps strength and self-reported function; (3) structured home-based versus structured in-person rehabilitation to be similarly effective for quadriceps and hamstring strength and self-reported function; and (4) postoperative knee bracing being ineffective for physical function and laxity. There was low-certainty evidence that: (1) preoperative exercise therapy improves self-reported and physical function postoperatively; (2) cryotherapy reduces pain and analgesic use; (3) psychological interventions improve anxiety/fear; and (4) whole body vibration improves quadriceps strength. There was very low-certainty evidence that: (1) protein-based supplements improve quadriceps size; (2) blood flow restriction training improves quadriceps size; (3) neuromuscular control exercises improve quadriceps and hamstring strength and self-reported function; and (4) continuous passive motion has no effect on range of motion.
Conclusion The general level of evidence for rehabilitation after ACL or meniscal tear was low. Moderate-certainty evidence indicates that several rehabilitation types can improve quadriceps strength, while brace use has no effect on knee function/laxity.
- knee
- anterior cruciate ligament
- rehabilitation
- exercise
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC?
ACL and meniscal injuries are often associated with a poor outcome—many fail to return to pre-injury level of sport and there is a high risk of reinjury, persistent symptoms and impaired quality of life.
There is little consensus regarding the optimal components of ACL and meniscal rehabilitation to achieve successful outcomes, leading to substantial heterogeneity in rehabilitation protocols.
WHAT THIS STUDY ADDS?
Despite 22 systematic reviews including 142 unique randomised clinical trials, there is mainly low level of evidence for the effectiveness of ACL rehabilitation interventions to improve symptomatic and functional outcomes.
The highest level of evidence for ACL rehabilitation in this review (moderate certainty) was observed for: (1) neuromuscular electrical stimulation to improve quadriceps strength; (2) open versus closed kinetic chain exercises to be similarly effective for improving quadriceps strength and self-reported function; (3) structured home-based rehabilitation to be similarly effective to structured in-person rehabilitation for improving quadriceps and hamstring strength and self-reported function; and (4) postoperative knee bracing being ineffective for physical function and knee laxity.
There is an urgent need for high-quality randomised clinical trials with sufficient sample size to improve the overall quality of evidence.
There was no evidence identified in this systematic review to inform the rehabilitation of isolated traumatic meniscal injuries in young adults.
Introduction
ACL and meniscal tears are the most common traumatic knee injuries in athletes and are expected to increase.1 2 Surgery to reconstruct the ACL or repair/partially remove a torn meniscus is often performed to restore mechanical stability, facilitate a return to competitive sport and prevent secondary injury.3 Yet, two-thirds of patients do not return to their pre-injury level of sport within the first year following ACL reconstruction (ACLR)4 and up to one-quarter sustain second ACL injuries.5 Young adults following meniscal surgery face a similar fate—although return to sport rates are higher (67%–89%),6 21% of repairs fail (ie, require secondary surgery).7 In the longer term, unacceptable knee symptoms, persistent functional deficits and impaired quality of life are common.8 9 Half of injured individuals will develop symptomatic osteoarthritis (OA) within 10 years, regardless of operative or non-operative treatment.10 11
Six different clinical practice guidelines emphasise the importance of active rehabilitation (ie, exercise therapy) following ACL injury (±meniscal injury) and reconstruction to restore muscle strength and lower limb function, reduce pain and symptoms, and safely return to competitive sport without reinjury.12 However, a systematic review focusing on ACL rehabilitation in clinical practice guidelines found conflicting recommendations and poor applicability—indicating barriers for clinicians to implement recommendations into practice.12 There is little consensus regarding the optimal components of ACL rehabilitation, reflecting a lack of evidence (and/or poor-quality evidence) underpinning these guidelines and leading to substantial heterogeneity in rehabilitation protocols.12 13 The same is true for traumatic meniscal injuries. The 2018 clinical practice guideline for meniscal lesion assessment and treatment overwhelmingly focuses on older adults with degenerative pathology associated with OA14 —a very different population (likely with distinct rehabilitation goals and expectations) to young adults with traumatic injuries.
Clinical practice decisions and policy are informed by reviews summarising the effectiveness of knee injury rehabilitation interventions. While systematic reviews of randomised controlled trials (RCTs) are considered the highest level of evidence, these vary greatly in scope and quality in knee injury research. An overview of systematic reviews allows the findings of separate reviews to be compared, providing clinical decision-makers with the strongest evidence available.15 The few systematic reviews of systematic reviews for the effectiveness of traumatic knee injury rehabilitation interventions have not focused on reviews of high-level (RCT) evidence and did not use the Grading of Recommendations Assessment, Development and Evaluation (GRADE) to evaluate the level of confidence of the estimated effect.16–18 Additionally, many new trials and reviews are available since the most recent overview was published in 2016.17
The aim of this systematic review was to critically appraise and synthesise systematic review evidence of RCTs assessing rehabilitation interventions following ACL or meniscal injury to improve symptomatic, functional, clinical, psychosocial or quality of life outcomes, and prevent reinjury. We aimed to provide an up-to-date overview and best-evidence synthesis of all review evidence for rehabilitation after ACL and meniscal injury to help maximise treatment outcomes for patients. This systematic review is one of several contributing to the development of evidence-based consensus recommendations for rehabilitation to optimise musculoskeletal health and prevent post-traumatic OA following knee trauma (OPTIKNEE).
Methods
This overview of systematic reviews followed Cochrane recommendations for reviews of systematic reviews and conforms to the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines.19 It was prospectively registered in Open Science Framework (https://osf.io/ue3wb/).
Search strategy, selection criteria and protocol deviations
We performed a systematic literature search in June 2020 and updated in June 2021 with no restriction on publication year or language in MEDLINE, EMBASE, CINAHL, SPORTDiscus and Cochrane Library. The search combined Medical Subject Headings and text words related to ACL/meniscal injury, rehabilitation and systematic review, and was developed in consultation with a health sciences librarian (online supplemental appendix 1). While we also included search terms for other knee injuries (eg, posterior cruciate ligament, collateral ligament and dislocation injuries) and did not specifically exclude these from the current review, we focused on ACL and meniscal injuries as no eligible systematic reviews on other traumatic injuries were identified, and ACL and meniscal injuries are the most common.20 Systematic reviews (with or without meta-analysis) of RCTs investigating non-surgical and non-pharmacological interventions (eg, exercise therapy, manual therapy, electrotherapy) in human participants following ACL and/or meniscal injury (with or without surgical management) were eligible (eg, open vs closed kinetic chain exercises in people following ACLR). Only full-text published systematic reviews were eligible (ie, conference abstracts and unpublished data were excluded). We had planned to also include systematic reviews of clinical practice guidelines but decided to only include reviews of RCTs, to reduce heterogeneity in study design and to ensure highest level of experimental evidence. For inclusion, systematic reviews needed to report on any outcome measurement related to pain, symptoms, function, reinjury, psychosocial factors, quality of life or adverse events. Physical measures, such as knee range of motion, proprioception, muscle strength, laxity, alignment and measures of adiposity, were also included. Although not specifically stated in the protocol, we also included measures of muscle size. Exclusion criteria were: (1) non-English language publication; (2) mean/median age of participants >30 years in studies following meniscal surgery (to minimise the effects of pre-existing OA and interventions being evaluated for degenerative disease); and (3) interventions following knee arthroplasty. While the research question described in our protocol focused on identifying the most effective rehabilitation interventions to reduce the risk of symptomatic post-traumatic OA, we identified no systematic reviews reporting symptomatic post-traumatic OA as an outcome. We therefore focused on the individual outcomes listed in the outcome section of the protocol (and above), which for some, when combined, have been previously used as a surrogate outcome for symptomatic OA.21
Supplemental material
Two authors (from AGC, BP or MH) independently screened all titles and abstracts for eligibility using a systematic review screening management application (covidence.org), and screened reference lists of all systematic reviews identified. Full texts of all potentially relevant studies were reviewed by two authors independently (AGC, MG) to determine final study selection. Disagreements between reviewers were discussed until consensus.22
Data extraction
The following data were extracted from the included studies by one author and cross-checked for accuracy by a second author (either AGC, MG) using a customised data extraction spreadsheet: databases listed in each systematic review used to identify relevant studies, date of search, inclusion/exclusion criteria listed by each systematic review, population and demographics, risk of bias/quality assessment tool, details of intervention and comparator, measures of effect, meta-analysis results (if applicable) and author conclusions. Details of primary RCTs were also extracted from summary tables of each review (group sizes, intervention/control details, outcomes, time points and summary results).
Risk of bias assessment
Two authors (AGC, MG) independently assessed risk of bias using the ROBIS (Risk of Bias In Systematic reviews) tool.23 The tool uses signalling questions (with accompanying rating guidance) to identify concerns (ie, high, low or unclear risk of bias) across four domains: (1) study eligibility criteria; (2) identification and selection of studies; (3) data collection and study appraisal; and (4) synthesis and findings (online supplemental appendix 2). A judgement of the overall risk of bias (ie, high, low, unclear) was then completed using the overall signalling questions. Disagreements in initial risk of bias ratings were discussed until consensus.
We also evaluated the quality of evidence pooled within the systematic reviews using a previously applied algorithm specifically developed to assign GRADE levels of evidence for overviews of systematic reviews.24 This algorithm incorporates the number of participants pooled, statistical heterogeneity, risk of bias and methodological quality of systematic reviews. Results are categorised as high, moderate, low or very low certainty of evidence (online supplemental appendix 3).
Data synthesis
We had planned to synthesise data quantitatively using meta-analyses; however, due to the large heterogeneity of the original RCTs and the lack of meta-analyses in the reviews (ie, only one review conducted a meta-analysis for each intervention type), we performed a best-evidence (narrative) synthesis. The synthesis incorporated the quantitatively pooled results from individual reviews and assigned GRADE certainty of evidence for each intervention type. We excluded systematic reviews with high (or an unclear) risk of bias across all four ROBIS domains (and an overall high risk of bias) from data synthesis to maximise the quality of evidence synthesised. We assessed the overlap of RCTs included in more than one systematic review and managed any overlap by providing GRADE levels of evidence for each systematic review (and not pooling effect estimates). We did not synthesise interventions that were only assessed in one RCT. We were unable to perform subgroup analysis to determine the optimal rehabilitation programme (eg, type, intensity, frequency, duration) as planned due to insufficient data preventing meaningful comparisons.
Patient and public involvement
Two individuals with lived experience of ACL injury and reconstruction (ACLR) and four clinicians (ie, physiotherapists, orthopaedic surgeons) contributed to the priority theme setting and outcomes of interest for this review at an in-person meeting alongside the 2019 World Congress of OA as part of the larger initiative to develop evidence-based consensus recommendations for rehabilitation to optimise musculoskeletal health and prevent post-traumatic OA following knee trauma (OPTIKNEE). In addition, a patient and clinician partner contributed to interpretation of findings by providing feedback on the manuscript for its clinical messaging (see the Acknowledgements section).
Results
Study characteristics
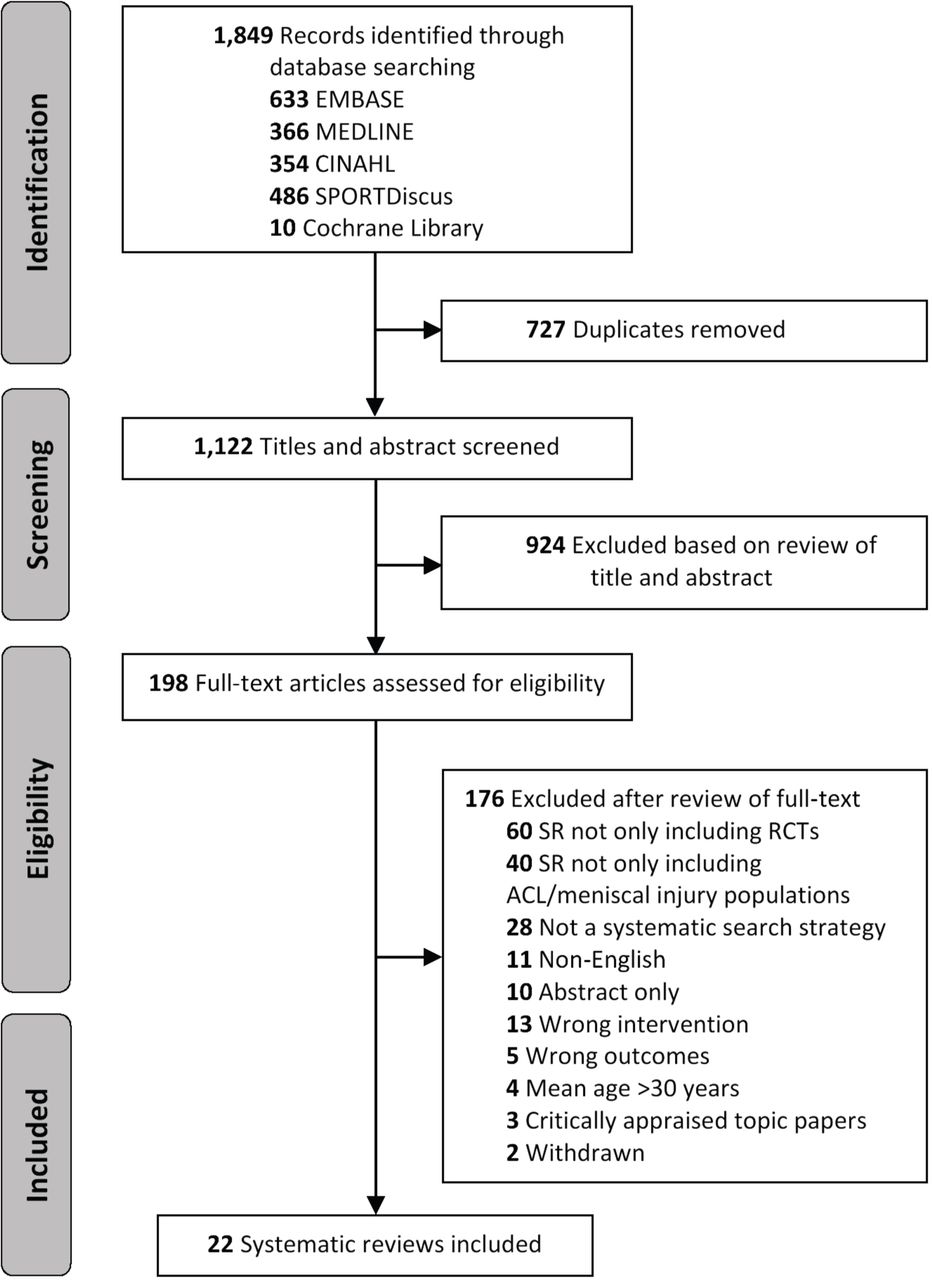
Twenty-two systematic reviews including 142 primary RCTs were included in this review (figure 1).25–46 These systematic reviews were published between 2004 and 2021, included mostly male participants (56%–95% men) and focused almost exclusively on ACLR populations (table 1). No systematic reviews evaluating interventions following isolated meniscal injury in persons with a mean age of ≤30 years were identified. The number of individual trials evaluating the same intervention in each systematic review ranged from 3 to 13, with the total number of participants randomised ranging from 98 to 789 (table 1).

Flow diagram of study selection. RCT, randomised controlled trial; SR, systematic review.
Study characteristics
Of the systematic reviews following ACL tear included in our data synthesis, the most common interventions evaluated were neuromuscular electrical stimulation (NMES) (n=4 reviews), open versus closed kinetic chain exercises (n=3), cryotherapy (n=2), structured in-person versus structured home-based rehabilitation (n=2), whole body vibration (n=2), neuromuscular control exercises (n=2), with single reviews evaluating the effect of: (1) preoperative rehabilitation; (2) psychological interventions; (3) blood flow restrictive training; (4) knee braces; (5) dietary supplements and (6) continuous passive motion (CPM). There was considerable overlap of trials included in the different systematic reviews used in data synthesis (67 of the 142 RCTs in ≥1 systematic review) (figure 2, online supplemental appendix 4). Interventions assessed in only one primary RCT (and not included in data synthesis) included electrocorporal shock wave therapy, hydrotherapy, stair climbing and duration of rehabilitation sessions.
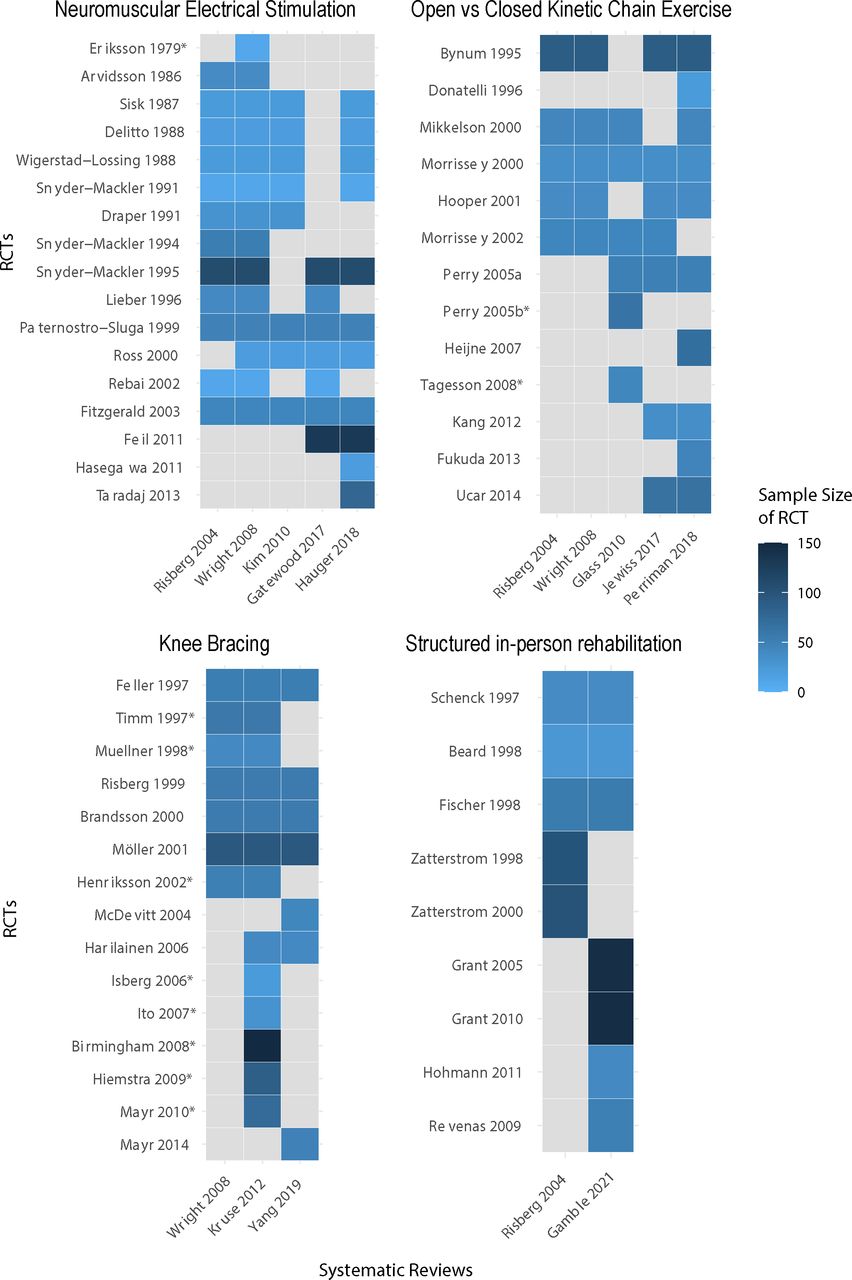
Heatmaps displaying the overlap of individual trials that evaluated interventions (with moderate-certainty evidence) included in more than one systematic review. Includes all eligible systematic reviews, irrespective of whether they were included or excluded from data synthesis. Grey boxes indicate that an RCT was not included in the respective systematic reviews. * indicates that an RCT was not included in our data synthesis because the systematic reviews that assessed it were excluded from our data synthesis due to high risk of bias. RCTs, randomised controlled trials.
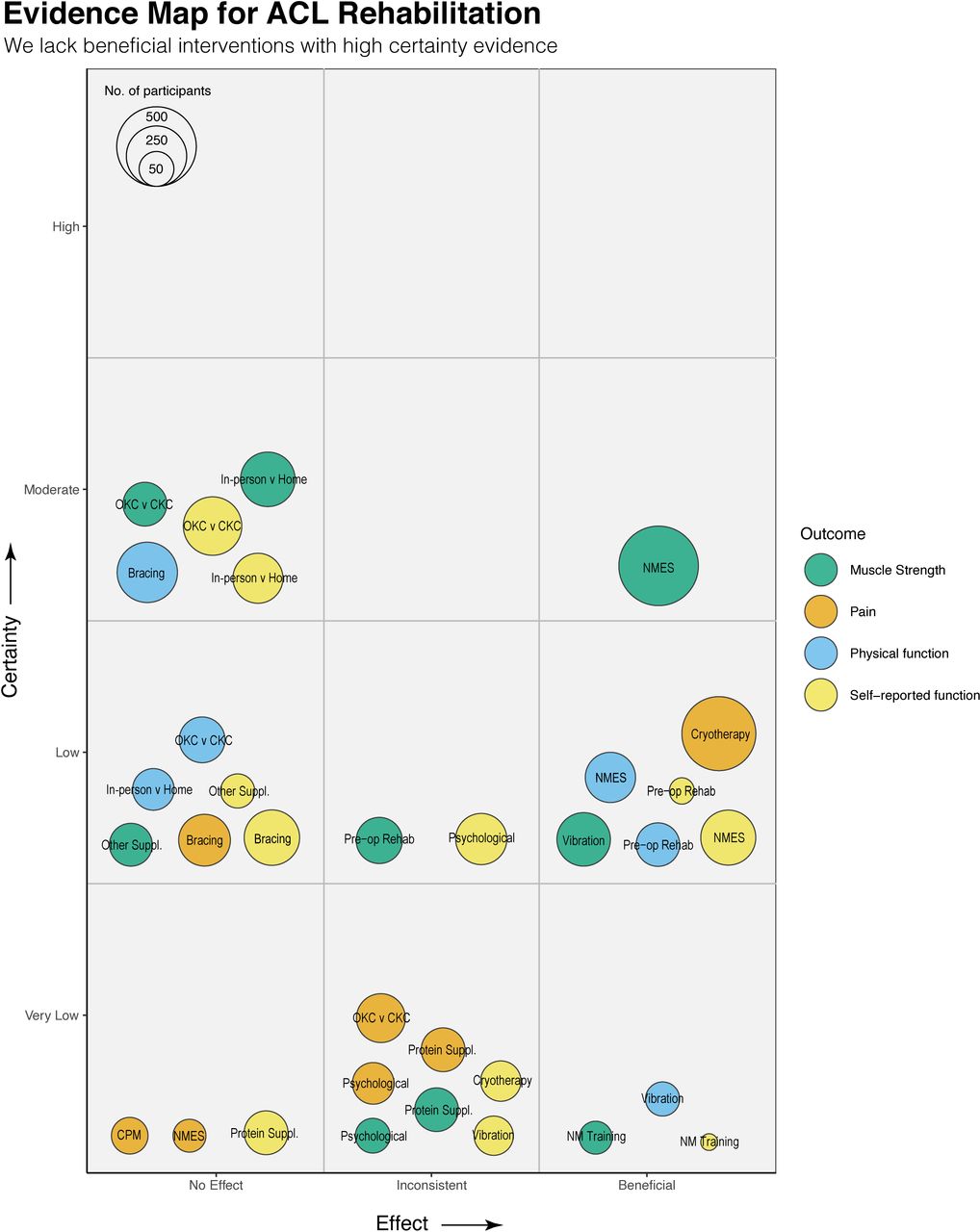
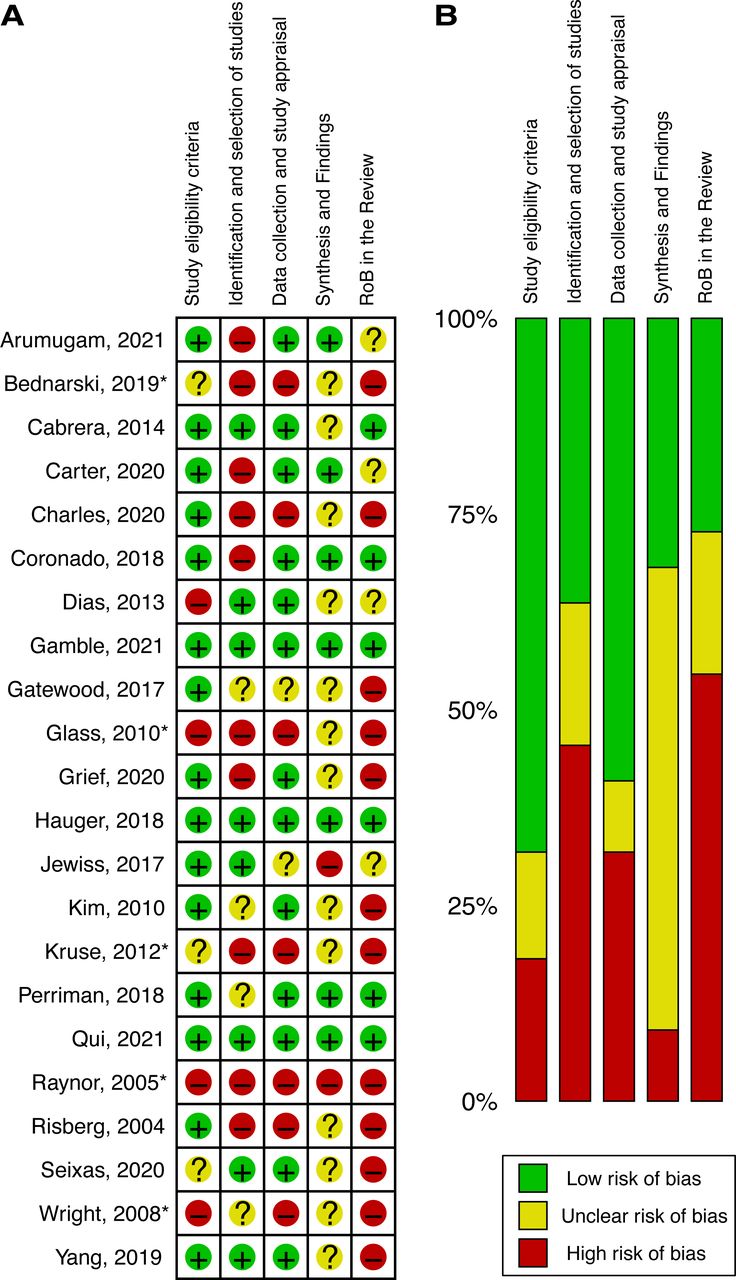
Six of the 22 reviews were rated as high or unclear risk of bias across all four domains and were subsequently excluded from data synthesis (figure 3). Across the remaining 16 reviews, 15 (94%) had low risk of bias for study eligibility criteria, 7 (44%) had low risk of bias for identification and selection of studies, 12 (75%) had low risk of bias for data collection and study appraisal, and 7 (44%) had low risk of bias for synthesis and findings (figure 3). Certainty of evidence for each intervention assessed using the adapted GRADE algorithm is detailed in online supplemental appendix 5online supplemental appendix 5 and an evidence map (figure 4) by each outcome (ie, muscle strength, pain, physical function, self-reported function).

Risk of bias (RoB) summary. (A) Individual systematic review RoB scores. (B) Breakdown of the RoB across the four domains and overall RoB score. * indicates that an RCT was not included in our data synthesis because the systematic reviews that assessed it were excluded from our data synthesis due to high RoB. RCT, randomised controlled trial.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Evidence map for ACL rehabilitation interventions. Only the four most consistent outcomes reported across systematic reviews presented for clarity. CKC, closed kinetic chain; CPM, continuous passive motion; NM, neuromuscular; NMES, neuromuscular electrical stimulation; OKC, open kinetic chain.
Neuromuscular electrical stimulation
Four reviews (total of 16 RCTs) evaluated the effect of NMES following ACLR.31 32 42 43 Moderate-certainty evidence from the most recent review indicates a large effect size for the addition of NMES (two to six sessions per week) to standard rehabilitation to improve quadriceps strength in the first 4–12 weeks postoperatively.31 There was very low to low-certainty evidence from two reviews indicating that the addition of NMES in the first 2 postoperative months resulted in greater self-reported and physical function immediately following the period of NMES application (and one review that was inconclusive). The number of NMES treatment sessions and electrical parameters varied widely in the original RCTs with no consistent dose-dependent effect.
Open kinetic chain exercises
Three reviews (total of 11 RCTs) compared open versus closed kinetic chain exercises during ACLR rehabilitation and found no significant difference in measures of knee laxity, muscle strength, self-reported function and physical function between the two approaches at any follow-up time (ranging between 4 weeks and 19 months) irrespective of graft type.28 29 43 Moderate-certainty evidence from the most recent review indicates no difference in knee laxity and quadriceps strength in the short term, self-reported function in the long term and rate of adverse events (eg, graft rupture) within the first 2 years.29 Conclusions were similar when comparing an early (<4 weeks postoperative, with knee flexion range limited to 45°–90°) versus delayed (12 weeks postoperative) start of open kinetic chain exercises, with most other outcomes associated with very low to low-certainty evidence.
Structured in-person rehabilitation
Two reviews (total of seven RCTs) evaluated structured in-person rehabilitation (ie, regular supervised rehabilitation plus home exercises) versus structured home-based rehabilitation (ie, regular unsupervised home-based exercises with occasional supervised sessions) following ACL tear and reconstruction. Both reviews concluded that structured in-person rehabilitation (range of 14–36 physiotherapy visits over 2–9 months) was generally not superior to structured home-based rehabilitation (range of 3–17 physiotherapy visits over 2–9 months) for range of motion, quadriceps and hamstring muscle strength, knee laxity and functional (self-reported and physical) outcomes both in the short-term and long-term (ie, up to 2 years) post-injury/surgery.40 43 The certainty of evidence for all outcomes from the most recent and highest quality review was low to moderate.40
Knee bracing
Moderate-certainty evidence from one review (seven RCTs) indicates that postoperative knee bracing following ACLR provides no benefit for knee laxity and physical function.37 There was also low-certainty evidence for bracing having no effect on self-reported function and pain.
Preoperative rehabilitation
There was low-certainty evidence from one review (three RCTs) that preoperative rehabilitation consisting of 3–6 weeks of muscle strengthening and neuromuscular (ie, function and stability) control exercises improves self-reported and physical function (eg, hop performance) 3 months post-ACLR, with no effect on return to sport outcomes and inconsistent evidence for effect on quadriceps strength.36
Cryotherapy
Low-certainty evidence from two reviews (total of 11 RCTs) indicates that cryotherapy (via cold compression devices) during the first 1–2 days post-ACLR can reduce postoperative pain and analgesic use up to approximately 1 week post-surgery (compared with no cryotherapy).26 42 The only included meta-analysis suggested a 14% (95% CI 12% to 17%) reduction in pain 48 hours postoperatively with the application of cryotherapy.26 Low to very low-certainty evidence showed cryotherapy had no effect on range of motion or quality of life. Although cryotherapy did not increase the risk of adverse events, there is no evidence for its effect on outcomes beyond 1 week.
Psychological interventions
Low-certainty evidence from one review (four RCTs) showed improvement in psychological and knee laxity outcomes with the addition of psychological interventions consisting of guided imagery, relaxation, coping modelling and visual imagery 6–12 weeks following ACLR.35 There was no consistent effect on self-reported function, health-related quality of life, pain or quadriceps strength.
Whole body vibration
Two reviews (total of 10 RCTs) assessed the effectiveness of whole body vibration following ACLR either following a single session or multiple sessions (up to 30) over 10 weeks in addition to standard rehabilitation.33 34 Very low to low-certainty evidence indicated a positive effect of whole body vibration (as an add-on to strength training) applied over multiple sessions on quadriceps and hamstring strength, balance and physical function but no effect of single sessions (compared with no/local vibration) on quadriceps strength or rate of force development.
Supplement use
Very low-certainty evidence from one review (10 RCTs) suggests that protein-based supplements taken between 6 and 18 months postoperatively may help to promote quadriceps size and strength following ACLR.38 Very low to low-certainty evidence of no effect was observed for creatine, vitamin and hormone-based supplements on quadriceps strength and self-reported function.
Blood flow restriction training
Very low-certainty evidence from one review (four RCTs) indicates blood flow restriction (inflatable cuff or tourniquet) during low-intensity resistance training in the first 2–16 weeks post-ACLR (ranging from two times per day to two times per week) results in greater improvements in quadriceps size and lean muscle mass compared with low-intensity resistance training alone.39
Neuromuscular control exercises
Two reviews (total of 12 RCTs) evaluated the effects of different neuromuscular control interventions (eg, balance, perturbation training, backward walking, plyometrics) compared with standard resistance-based rehabilitation (ie, mostly open kinetic chain exercises).41 43 Very low to low-certainty evidence indicates that two to three neuromuscular control training sessions per week over 1–9 months following ACL tear or reconstruction are more effective than standard rehabilitation to improve quadriceps/hamstring strength and self-reported function but provide no benefit for knee proprioception.
Continuous passive motion
Very low-certainty evidence from one review (two RCTs) indicates that CPM during the first week post-ACLR is no more effective at improving range of motion and pain than active range of motion exercises.42 Low-certainty evidence also shows that CPM was less effective at improving joint position sense than continuous active motion.
Discussion
This overview and critical appraisal of the best-available evidence for ACL or meniscal injury rehabilitation demonstrated a disappointingly low level of evidence for the effectiveness of rehabilitation interventions to improve symptomatic and functional outcomes in young adults with ACL injury with or without associated injuries. There was no systematic review evidence available to inform isolated meniscal injury rehabilitation. From 22 systematic reviews of ACL injury rehabilitation, the certainty of evidence for most rehabilitation interventions was low to very low. The strongest level of evidence (moderate certainty) was found for: (1) NMES to improve quadriceps strength; (2) open versus closed kinetic chain exercises to be similarly effective for quadriceps strength, self-reported function and knee laxity; (3) structured home-based rehabilitation to be similarly effective to structured in-person rehabilitation for quadriceps and hamstring strength, self-reported function and knee laxity; and (4) a lack of effectiveness of postoperative knee bracing on physical function and knee laxity.
Our review provides an up-to-date overview of the best-available evidence for clinicians rehabilitating ACL-injured patients and highlights a lack of evidence for isolated traumatic meniscal injury rehabilitation. Although the overwhelming evidence was drawn from studies of individuals following surgical management (ACLR), the findings are likely also applicable to those choosing a non-operative approach following ACL injury given the similarity in impairments and outcomes between the two management strategies (although the timing and focus of interventions may differ without the need for post-surgical restrictions and graft site morbidity in a non-operative approach).3 Our review overcomes limitations of previous overviews of systematic reviews evaluating ACL injuries only, that were limited in scope (ie, a 2012 overview included only five systematic reviews),18 lacked critical appraisal (ie, a 2016 overview performed no quality assessment)16 and included lower levels of evidence (ie, cohort studies included in a 2016 overview).17 Importantly, the current study is the first to assess level of evidence using GRADE as recommended by Cochrane.
All interventions evaluated in the current review were evaluated in at least one recent (ie, since 2018) systematic review. The only exceptions were: (1) cryotherapy, where the most recent systematic review (published in 2019)25 was excluded from data synthesis due to high risk of bias (although conclusions were the same as the 2014 review included in data synthesis26); and (2) CPM, which was reported in a 2017 systematic review of multiple interventions.42 With the large and rapidly expanding number of studies published on ACL injuries, and the 142 original RCTs underpinning the evidence for rehabilitation in this review, such a low level of evidence was surprising. The low to very low-certainty evidence observed for most interventions was assigned using an adaptation of the GRADE criteria specifically designed for overviews of systematic reviews and was driven by the small number of participants in the original trials (ie, most RCTs n<50, only four with n>100), large heterogeneity in interventions and outcomes evaluated, and high risk of bias (online supplemental appendix 5). Despite the low-certainty evidence for most interventions, the findings of this best-evidence synthesis could help guide clinical rehabilitation programmes following ACL injury by arming clinicians with the best-available evidence to optimise patient outcomes.
The lack of systematic reviews evaluating isolated meniscal injury rehabilitation in young adults highlights a clear need to synthesise and critically appraise existing RCT evidence and conduct new RCTs to improve outcomes for young adults (eg, <30 years of age) following isolated meniscal injury.47 48 Systematic reviews of rehabilitation for meniscal pathology have mostly focused on older adults (ie, mostly >40 years of age) with degenerative meniscal lesions and were thus excluded from the current overview. Findings from reviews of older adults indicate that an exercise therapy approach (either primarily in person or home based) is an effective rehabilitation strategy, but given degenerative meniscal lesions are part of the OA disease process, the goals and expectations (and therefore content) of rehabilitation are likely different to younger adults with traumatic injuries.49 50 In contrast, traumatic meniscal injuries are often associated with similar impairments to ACL injuries, yet the extent to which the findings of this review apply to isolated meniscal injuries is unknown.
For young adults undergoing ACLR, a goal-based exercise therapy programme progressing through different phases of recovery over 9–12 months is considered the gold standard of rehabilitation.12 Such an approach is advocated in clinical practice guidelines17 even without full evaluation in clinical trials. One-third of the 12 different interventions evaluated in this overview were exercise related (ie, open kinetic chain, preoperative rehabilitation, supervised rehabilitation, neuromuscular control exercises)—most other interventions were adjuncts to supplement exercise therapy. Clinicians need to consider the cost–benefit of adjuncts involving additional modalities (eg, neuromuscular electrical stimulation, blood flow restriction, whole body vibration) given the mixed level of evidence.
Despite the perceived value of exercise therapy following ACL injury and reconstruction, there is little certainty regarding its effectiveness and no clarity concerning specific therapeutic dosage and delivery. This stems from most trials after ACL injury not individualising interventions (ie, same programme for all patients) and failing to adequately document exercise frequency, intensity, volume and progression.51 Such a problem is not unique to the ACL field—it similarly affects implementation of rehabilitation for other musculoskeletal conditions.52 With the development of a specific template to describe exercise interventions to a minimum standard—Consensus on exercise Reporting Template53 —future clinical trials should use such a template to structure intervention reports to increase clinical uptake of exercise programmes and enable research replication. Expecting one optimal dosage and delivery regimen is unrealistic, but with a body of evidence that adequately documents critical components of exercise dosage and delivery, clinicians will be able to make a more informed decision when prescribing exercise. Interestingly, results of the current overview indicate moderate-certainty evidence that less regular physiotherapy visits (ie, 3–17 over 2–9 months) are not inferior to regular physiotherapy visits (ie, 14–36 over 2–9 months). It is important to note that, although the structured home-based rehabilitation approach (ie, less regular physiotherapy visits) is often termed ‘home based’ in the literature,43 it is not purely home based and can include many (ie, up to 17) supervised sessions to educate, motivate and progress patients. There is no evidence that a completely unstructured home-based rehabilitation programme with no supervised visits is equivalent to occasional/regular supervision.
Research implications: where to next?
Promisingly, the findings of this overview support some existing recommendations in ACL clinical practice guidelines (eg, use of preoperative rehabilitation, cryotherapy, NMES, while discouraging CPM and knee bracing).12 Yet, our findings also highlight that clinical practice guidelines do not always reflect best-available evidence. Contrary to popular beliefs perpetrated in recent clinical practice guidelines (ie, that open kinetic chain exercises should be delayed for at least 4 weeks post-ACLR),17 early introduction of open kinetic chain exercises was not associated with any adverse outcomes (moderate-level evidence) indicating they might be safely introduced to perform isolated quadriceps strengthening. What was most alarming was the paucity of high-quality (or even moderate-quality) evidence from which ACL rehabilitation guidelines are based. This overview highlighted a need for high-quality clinical trials with sufficient sample sizes to improve the overall body of evidence, since most evidence is too weak to confidently guide clinical practice guidelines. Most of the original 142 RCTs included in the systematic reviews included fewer than 30 participants. Furthermore, only three types of interventions (whole body vibration, supplement use, blood flow restriction training) had RCTs published since 2015. Such restricted samples of participants, together with our inability to perform a single meta-analysis, are an inditement on the quality and variability of the current evidence.
Given that a return to competitive sport without reinjury and a satisfactory quality of life are key determinants of rehabilitation success for patients,54 55 it was surprising that so few systematic reviews included return to sport (n=3), prevention of reinjury (n=0) and quality of life outcomes (n=1). There is a clear and alarming gap in our understanding of how to optimise these important outcomes for patients following ACL injury. Similarly, no included systematic review could provide evidence for the effect of interventions beyond the initial rehabilitation period of 6–12 months and no education or behaviour change interventions aimed at improving exercise adherence and ability to self-manage longer term were included. Persistent symptoms and functional impairments are common, and may increase the risk of early post-traumatic OA following ACL injury.56 57 Clinical trials evaluating the effect of rehabilitation interventions beyond the first postoperative year, particularly for those with or at high risk of (early) post-traumatic OA, are required.58 The fact that most evidence was based on findings in men (56%–95% male participants in each systematic review) highlights the importance of considering how women respond to ACL rehabilitation interventions. This is pertinent given that women have a higher risk of primary ACL injury59 and generally have poorer outcomes following ACL injury than their male counterparts.60 Finally, the absence of systematic review evidence to inform rehabilitation for isolated meniscal injuries indicates an important area of future work.
Limitations
A potential limitation of our review was that we restricted our inclusion to reviews published in English. It is unlikely this substantively influenced our findings as 20 of the 22 included systematic reviews had an unrestricted search by language. A lack of meta-analyses and subgroup data available in the included systematic reviews prevented our planned meta-analysis of meta-analyses and subgroup analyses, respectively. This limited our ability to compare effect sizes across different interventions, which was mentioned in our protocol. There may have been some RCTs evaluating relevant interventions that were published since the included systematic reviews that were not captured in our review. However, most of the specific interventions we evaluated were reported in recent systematic reviews (ie, most published since 2019/2020), thereby limiting the number of existing RCTs not captured by the systematic reviews we included. Finally, the race and geographical diversity of participants included in the systematic reviews is not known.
Conclusions
This systematic review of systematic reviews found that current recommendations for ACL injury rehabilitation are mostly based on low to very low-certainty evidence stemming largely from a low number of participants included in the original RCTs. Moderate evidence was found for: (1) NMES to improve quadriceps strength; (2) open versus closed kinetic chain exercises to be similarly effective for quadriceps strength, self-reported function and knee laxity; (3) structured home-based rehabilitation to be similarly effective to structured in-person rehabilitation for quadriceps and hamstring strength, self-reported function and knee laxity; and (4) a lack of effectiveness of postoperative knee bracing on physical function and knee laxity. No systematic review evidence was available to inform meniscal injury rehabilitation. High-quality randomised trials with a focus on exercise-based interventions and longer-term outcomes are needed to improve the overall body of evidence and guide future clinical practice guidelines for knee injury rehabilitation.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank physiotherapist, Mick Hughes, and ACL-injured athlete, Rachel Hibbert, for providing consumer input into this overview.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @agculvenor, @m_girdwood, @Knee_Howells, @melhabphysio, @jwhittak_physio, @ewa_roos
Contributors AGC, JLW, EMR and KMC designed the systematic review and were involved in priority theme setting. AGC, BP and MH completed all searches and study selection (including inclusion and exclusion of abstracts). AGC and MG completed all data extraction and risk of bias assessment. AGC and CBJ planned the analyses, and all authors interpreted the data. MG prepared all figures. AGC wrote the initial draft. All authors critically revised the manuscript for important intellectual content and approved the final version of the manuscript.
Funding This review is part of the OPTIKNEE consensus (https://bit.ly/OPTIKNEE) which has received funding from the Canadian Institutes of Health Research (OPTIKNEE principal investigator JLW #161821). Initial priority theme setting was supported by a La Trobe University Research Focus Area Collaboration Grant (OPTIKNEE principal investigator AGC). AGC is a recipient of a National Health and Medical Research Council (NHMRC) of Australia Investigator Grant (GNT2008523). MG is a recipient of a NHMRC of Australia PhD Scholarship (GNT1190882). The funders had no role in any part of the study or in any decision about publication
Competing interests AGC, BP and JLW are Associate Editors of BJSM. KMC is a senior advisor of BJSM. All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.