Article Text

Abstract
Objective To prospectively evaluate 1-year clinical and radiological outcomes after operative and non-operative treatment of proximal hamstring tendon avulsions.
Methods Patients with an MRI-confirmed proximal hamstring tendon avulsion were included. Operative or non-operative treatment was selected by a shared decision-making process. The primary outcome was the Perth Hamstring Assessment Tool (PHAT) score. Secondary outcome scores were Proximal Hamstring Injury Questionnaire, EQ-5D-3L, Tegner Activity Scale, return to sports, hamstring flexibility, isometric hamstring strength and MRI findings including proximal continuity.
Results Twenty-six operative and 33 non-operative patients with a median age of 51 (IQR: 37–57) and 49 (IQR: 45–56) years were included. Median time between injury and initial visit was 12 (IQR 6–19) days for operative and 21 (IQR 12–48) days for non-operative patients (p=0.004). Baseline PHAT scores were significantly lower in the operative group (32±16 vs 45±17, p=0.003). There was no difference in mean PHAT score between groups at 1 year follow-up (80±19 vs 80±17, p=0.97). Mean PHAT score improved by 47 (95% CI 39 to 55, p<0.001) after operative and 34 (95% CI 27 to 41, p<0.001) after non-operative treatment. There were no relevant differences in secondary clinical outcome measures. Proximal continuity on MRI was present in 20 (95%, 1 recurrence) operative and 14 (52%, no recurrences) non-operative patients (p=0.008).
Conclusion In a shared decision-making model of care, both operative and non-operative treatment of proximal hamstring tendon avulsions resulted in comparable clinical outcome at 1-year follow-up. Operative patients had lower pretreatment PHAT scores but improved substantially to reach comparable PHAT scores as non-operative patients. We recommend using this shared decision model of care until evidence-based indications in favour of either treatment option are available from high-level clinical trials.
- tendon
- rupture
- tear
- hamstring tendons
Data availability statement
Data are available on reasonable request.
Statistics from Altmetric.com
Introduction
Proximal hamstring tendon avulsion injuries have a substantial burden, compromising sports participation and the more physical aspects of daily life.1–5 Systematic reviews report superior outcome after operative treatment in terms of satisfaction, patient-reported outcome measures, return to sports (RTS) and strength.2–4 Yet, they highlight the risk of bias as most studies are retrospective, and there is a lack of data on non-operative outcome. In a recent systematic review,2 less than 30 non-operative patients were included compared with more than 750 operative patients. As the comparison between treatments is limited, prospective data are needed, especially on outcomes following non-operative treatment.
In the absence of strong evidence, treatment decision-making for these severe injuries remains challenging. As little is known about non-operative outcomes, and operative treatment carries risks of complications, it is paramount to include patients’ preferences in the decision-making. Shared decision-making is a collaborative process in which patients and clinicians jointly establish treatment plans that integrate clinical evidence and patient preferences.6 It improves patient satisfaction and adherence through increased knowledge, lower decisional conflict and greater likelihood of receiving care aligned with patient values.7 8 In this pragmatic study, we employed a shared decision-making model.
Our objective was to prospectively evaluate 1-year clinical and radiological outcomes after operative and non-operative treatment of proximal hamstring tendon avulsions. Our hypothesis was that, in a shared decision-making model, operative treatment results in superior clinical and radiological outcomes.
Methods
Participants
Patients with a suspected proximal hamstring tendon injury between October 2016 and August 2019 were screened. Eligibility criteria are shown in box 1.
Eligibility criteria
Inclusion criteria
Age ≥18 years.
MRI-confirmed full-thickness injury of ≥1 proximal free hamstring tendon(s).
Exclusion criteria
Contraindication to MRI.
Previous full-thickness injury of ≥1 proximal free hamstring tendon(s) in the same leg.
Bony avulsion.
Unwilling to participate or unable to give written informed consent.
Concurrent disease/injury that renders the patient unable to follow the rehabilitation programme.
Shared decision making
Through a shared decision-making process with a surgeon (GMMJK/RWP) or sports medicine physician (JLT) and physiotherapist (CV), operative or non-operative treatment was chosen. All clinicians involved have more than 10 years of experience in muscle injury treatment. Key steps included choice talk, option talk and decision talk.6 Patients were informed about the diagnosis and the choice between operative or non-operative treatment. Using visual aids, patients were informed about anatomy, injury characteristics, advantages and disadvantages of operative and non-operative treatment and expected outcomes. For operative treatment, this included restoration of proximal continuity, improved functional/strength recovery, higher chance of resolution of radiating pain and pain during sitting, postoperative protection and risk of operative complications. For non-operative treatment, the ability to start physiotherapy immediately without risk of operative complications or need for postoperative protection were discussed, at the cost of uncertainty of proximal continuity restoration, and a possible greater chance of residual functional limitations/strength deficits.
To facilitate up-to-date shared decision-making, the information provided during the option talk was continuously updated based on annual quantitative interim analyses and emerging evidence. The latter included systematic reviews2 3 and worldwide surveys that evaluated current practice and preferences regarding the decision-making process.9 10 During the study period, decision-making was initially generally operative-minded and non-operative treatment was reserved for middle-aged patients with lower functional demand. Due to satisfactory outcome in this group, the provided information was updated and gradually more patients opted for non-operative treatment, but operative treatment was typically advised in 2-tendon avulsions with substantial retraction and persistent functional limitations/sciatic symptoms. Ultimately, patients without a strong preference for either treatment started physiotherapy and chose operative or non-operative treatment after evaluating progression of symptom resolution and functional recovery after approximately 2 weeks. Elite athletes always opted for operative treatment.
We refer to online supplemental appendix A for a modifiable shared decision-making aid for use in clinical practice.
Supplemental material
Operative treatment
Operative reattachment of the proximal hamstring tendons was performed per the current standard11 (online supplemental appendix B). By varying the degree of knee flexion during surgery following reattachment, tension on the repair was assessed. Based on this assessment, a cast was applied in the operating room. Cast immobilisation was continued for 2 weeks followed by a hinged knee brace that limited full knee extension but allowed knee flexion for 4 weeks. The brace was set at 30° knee flexion and gradually (10° per week) progressed towards full knee extension. A criteria-based rehabilitation programme (online supplemental appendix B) was initiated as soon as the knee brace was applied.
Supplemental material
Non-operative treatment
Non-operative patients were referred to a physiotherapist with extensive experience with these injuries (CV) and immediately started the rehabilitation programme (online supplemental appendix B) in phase II. Phase I served as a protective phase for operative patients only. Phase II focused on normalising gait and regaining control with functional movement without pain. Non-impact balance and proprioceptive exercises, gait training using an antigravity treadmill, and strengthening exercises of the hamstrings with addition of electrical stimulation as well as strengthening of hip rotators and trunk were initiated. Phase III was started when gait was normal and functional movements were carried out without pain or having to unload the injured leg. This phase focused on restoring pain-free control of work-specific and sport-specific movements. Hamstring strengthening was progressed to lengthened positions. Impact control and running exercises were started. Phase IV focused on preparing patients for return to work-specific and sport-specific activities. It was started when patients demonstrated dynamic neuromuscular control with multiplane activities at low-to-medium velocity without pain or swelling. During this phase, running, strengthening, and impact control exercises were progressed further. Drills were initiated to replicate work-specific or sport-specific demands. The goal of this final phase was to achieve dynamic neuromuscular control with multi-plane activities at high velocity and asymptomatic unrestricted participation in work-specific or sport-specific activities.
Data collection
Data collection was performed at the initial visit and at 2 months (questionnaires), 6 months (questionnaires and clinical tests) and 1 year (questionnaires, clinical tests and MRI) after start of treatment (date of surgery or physiotherapy referral). We chose not to use date of injury as baseline considering the potential delay between injury and diagnosis2 4 12 associated with this injury as well as potential treatment delay.
Questionnaires
Questionnaires included the Perth Hamstring Assessment Tool (PHAT),13 Proximal Hamstring Injury Questionnaire (PHIQ),14 EQ-5D-3L and Tegner Activity Scale (TAS).15 The PHAT (0–100, higher scores correspond with better outcome) consists of four questions on symptoms of pain/discomfort and level of activity specific for proximal hamstring tendon injury. It has high reproducibility (ICC: 0.84) and a minimal detectable change of 16.4 points.13 The PHIQ is a hamstring avulsion-specific questionnaire consisting of 11 questions on proximal hamstring tendon-specific symptoms, functional restrictions, subjective rate of recovery, and sports participation. No data on its psychometric properties are available. The PHAT and PHIQ were chosen as they specifically explore symptoms and functional limitations resulting from proximal hamstring tendon injury. The EQ-5D-3L and TAS were chosen to explore recovery more broadly in terms of quality of life, activities of daily living function and activity level. Details on the questionnaires are available in online supplemental appendix B.
Clinical tests
Tests to assess hamstring flexibility and strength were performed by one of five male physicians. Hamstring flexibility was measured in two positions: the passive straight leg raise (PSLR)16 and active knee extension test (AKET).17 Isometric knee flexor strength was assessed with a Hoggan MicroFET2 hand-held dynamometer (Hoggan Scientific, Salt Lake City, Utah, USA) in three positions: prone 0°/90° (°hip flexion/°knee flexion), prone 0°/15° and supine 90°/90°.17 18 Patients were verbally encouraged to perform a maximal voluntary contraction for 3 s while the tester held the dynamometer in place. We recorded the best of three efforts per position per leg in Newtons. If a patient reported onset of pain (pain score ≥3/10), that specific measurement was terminated. Previously reported inter-rater reliability for these testing positions was good (ICC 0.76–0.84).18 19 Detailed measurement methods are included in online supplemental appendix B.
MRI
The MRI protocol is included in online supplemental appendix B. MRIs were scored by an experienced musculoskeletal radiologist (FS). Assessment included proximal continuity, direct tendon retraction, fatty infiltration and assessment of the sciatic nerve.
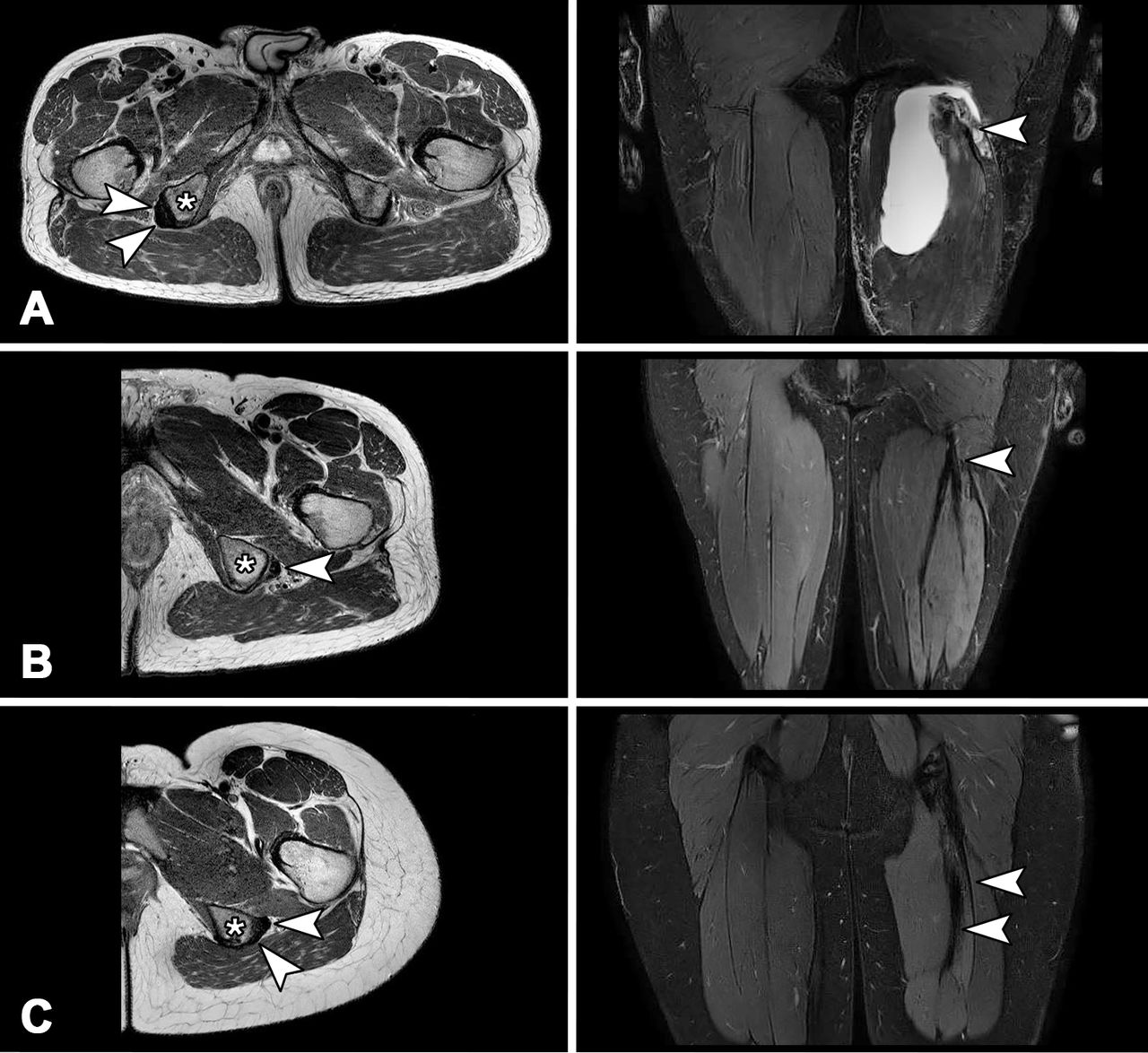
Continuity of the hamstring tendons with the ischial tuberosity was scored as either absent, continuity by means of separate tendons, or by a shared tendon (tendons are scarred together and attached to the ischial tuberosity with an organised, tendon-like structure) (figure 1). Direct retraction was defined as the shortest distance between mid-origin and most proximal margin of the tendon stump.20 Fatty infiltration per individual hamstring muscle was scored using a modified MRI version of the Goutallier classification21 (normal-to-mild: normal muscle or fatty streaks, moderate: fat ≤muscle and severe: fat >muscle). The sciatic nerve was evaluated for increased signal intensity, enlargement and contact with perinervous scar tissue.
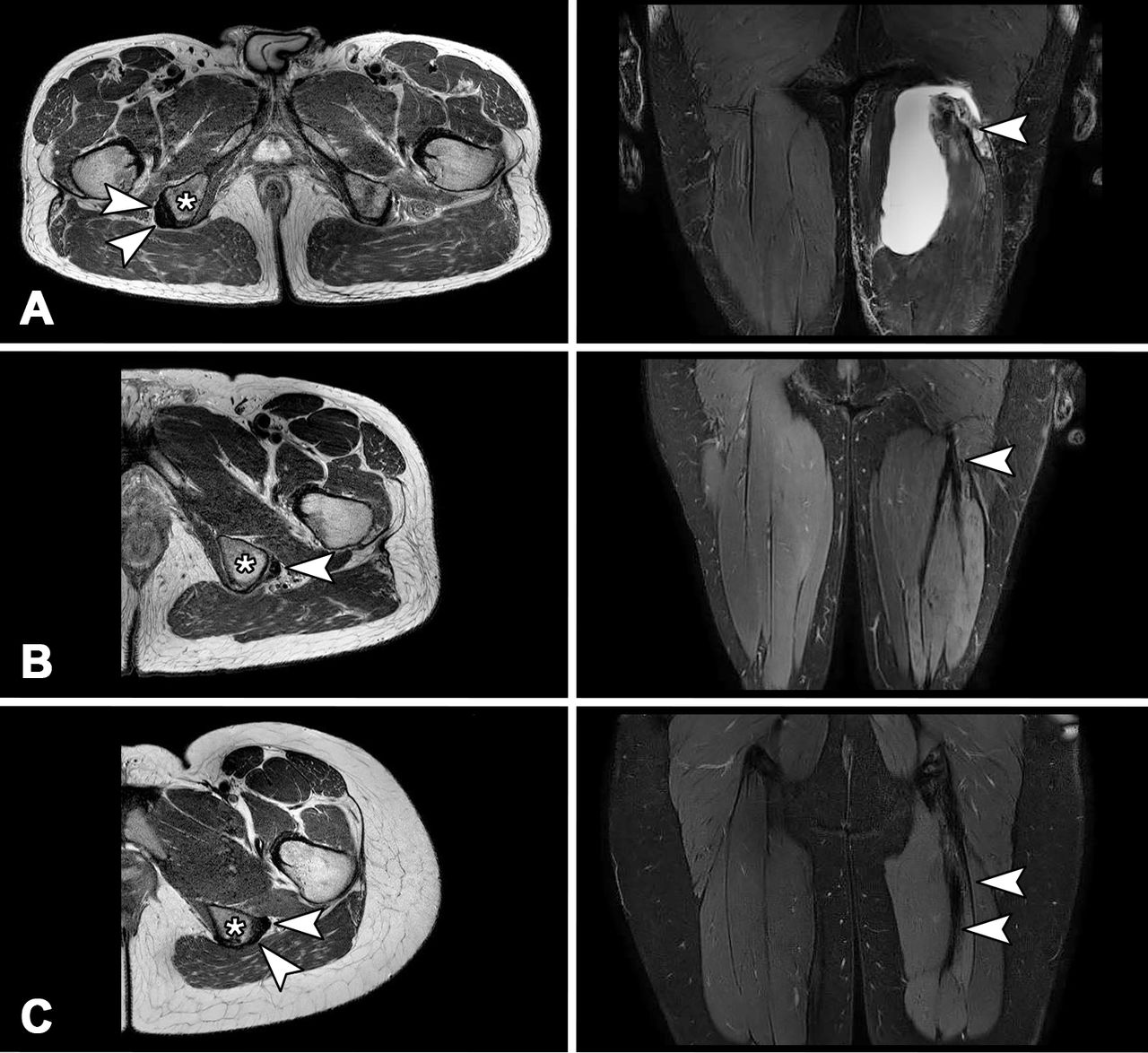
MRI assessment of proximal continuity following left-sided injuries. (A) No continuity. The axial image demonstrates both the conjoint (CT) and semimembranosus (SM) tendon (arrows) attached to the ischial tuberosity (asterisk) on the right but no tendons attaching on the left. The coronal image demonstrates discontinuity with the (hypo-intense) CT stump (arrow) in a haematoma indicating acute injury. (B) Continuity by a shared tendon at follow-up. The axial image shows a single attached neotendon (arrow) on the ischial tuberosity (asterisk). The coronal image demonstrates merging of both the CT and SM tendons (arrow) into a joint neotendon that courses proximally. (C) Continuity by separate tendons (arrows) on the ischial tuberosity (asterisk) at follow-up.
Primary outcome
The primary outcome was the PHAT score at 1 year after start of treatment.
Secondary outcomes
Secondary outcome measures included questionnaires (PHAT score and PHAT score change, PHIQ, EQ-5D-3L and TAS), rate of and time to RTS, and recurrence rate at 2 months, 6 months and 1 year after start of treatment. We additionally report clinical tests (hamstring flexibility and isometric strength) at 6 months and 1 year, and MRI findings at 1 year. RTS was recorded as: (1) return to the same sport at pre-injury level, (2) at a lower level, (3) in different sports or (4) no RTS. We also recorded time to RTS (in any sport at any level, in weeks from injury). Recurrence was defined as an MRI-confirmed full-thickness injury of ≥1 proximal free hamstring tendon(s) in the same leg within 1-year follow-up. Patients were instructed to contact the coordinating researcher in case of suspected adverse events.
Statistical analysis
Analysis was performed using SPSS (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, V.26.0. IBM). Descriptive data are presented as appropriate. Normality of data was assessed visually using histograms and normal Q-Q plots. Patients were analysed by intention to treat.
To test for the between-group differences in PHAT score at 1 year and PHAT score change in 1 year, a repeated measures general linear model was used. To test for between-group differences in secondary outcome measures at 1 year, we used χ2 tests and independent t-tests/Mann-Whitney U tests.
Post-hoc analysis
In a post hoc analysis for the primary outcome, adjustments were made for baseline variables (online supplemental Appendix B) that influenced the primary outcome with p<0.1. As between-group differences at baseline could potentially be attributed to timing of the initial visit, we repeated this sensitivity analysis with ‘time between injury and initial visit’ as covariate instead of ‘time between injury and start of treatment’, as well as the combination of both, to explore whether our choice of included time variable impacted outcome.
In case of missing data, data from the last observation were carried forward. Additional best-case/worst-case scenario analyses were performed in which highest and lowest values were entered for missing PHAT values.
Results
We included 59 patients (figure 2); 26 (44%) women and 33 (56%) men with a median age of 51 (IQR: 45–56). Twenty-six (44%) patients received operative and 33 (56%) patients received non-operative treatment. There were no cross-overs. Baseline data are presented in table 1. Operative patients presented significantly earlier after injury (median 12 vs 21 days, p=0.004) with significantly larger hamstring flexibility deficits (−34° and −28° compared with −12° and −11° for PSLR and AKET respectively, p<0.01), lower isometric strength (39%, 0% and 32% of contralateral strength compared with 64%, 32% and 50% in the prone 0/90, prone 0/15 and supine 90/90 positions p<0.01), and lower PHAT scores (32±16 vs 45±17, p=0.003). MRI demonstrated avulsion of both proximal tendons in 53 (90%) patients, isolated conjoint tendon avulsion in 2 (3%) and isolated semimembranosus tendon avulsion in 4 (7%). In the operative group, all injuries involved both tendons. In the non-operative group both tendons were affected in 27 (82%) patients, the conjoint tendon in 2 (6%) and the semimembranosus tendon in 4 (12%).

Flow chart of inclusion process.
Demographic data, clinical tests and MRI characteristics at initial visit
Median time between injury and start of treatment was 30 (IQR: 21–45) days in the operative group and 21 days (IQR: 12–48) in the non-operative group.
Clinical outcome
Primary outcome
PHAT scores in the operative and non-operative group at 1-year follow-up were 80±19 vs 80±17 (figure 3). There was no between-group difference in mean PHAT score at 1-year follow-up (p=0.97). There was no between-group difference in mean adjusted PHAT score at 1-year follow-up (p=0.23). The post hoc analyses with different time covariates did not change outcome. Best-case/worst-case scenario analyses also revealed similar outcomes (online supplemental appendix B).

{kind=link}
{kind=link}
{kind=link}
Mean (95% CI) unadjusted Perth Hamstring Assessment Tool (PHAT) score (0–100) (A) and adjusted score (B) for operative (solid line) and non-operative group (dashed line) at initial visit and at 2-month, 6-month and 12-month follow-up.
Secondary outcome
An overview of secondary clinical outcome measures is provided in table 2.
Clinical outcome at 2-month follow-up, 6-month follow-up and 1-year follow-up
The increase in mean PHAT score after 1 year in the operative group was 47 points (95% CI 39 to 55, p<0.001) and 34 points (95% CI 27 to 41, p<0.001) in the non-operative group (figure 3). The adjusted increase in mean PHAT score after 1 year in the operative group was 44 (95% CI 37 to 51, p<0.001) and 40 (95% CI 32 to 47, p<0.001) in the non-operative group. We adjusted for injured side, tendon retraction, perinervous scarring and days from injury to start of treatment.
In the operative group 6 (23%) patients did not return to sports at 1 year and 7 (27%) had returned to sports at preinjury level. In the non-operative group, 4 (12%) did not return to sports and 11 (33%) had returned to sports at pre-injury level. Time to RTS for the operative and non-operative group was median 25 (IQR: 20–33.5) and 24 (IQR:16–36) weeks. There were no statistically significant between-group differences in rate of and time to RTS. There was 1 (4%) recurrence in the operative group due to a water-skiing accident after 10 months.
Hamstring flexibility was near-symmetrical, without significant between-group differences. Isometric strength deficits were present in both groups. Operative patients had isometric hamstring strength (% of contralateral leg) of 73% (IQR 64–81.5), 66.5% (IQR 54–80) and 78% (IQR 64–93.5) in the prone 0/90, prone 0/15 and supine 90/90 positions. Non-operative patients had 91% (IQR 80–96), 60% (IQR 46–74.5) and 76.5% (IQR 68–89). Isometric strength in the prone 0/90 position was significantly higher in the non-operative group (p<0.001).
There were no significant between-group differences in TAS and EQ-5D-3L responses. The PHIQ revealed a significantly higher rate of stiffness (60% vs 28%, p=0.03) and lower rate of numbness and/or tingling in the injured leg (10% vs 40%, p=0.03) in the operative group compared with the non-operative group. There were no infections, deep vein thromboses, nor iatrogenic sciatic nerve injuries. At final follow-up, 96% of operative patients and 91% of non-operative patients stated that they would make the same treatment choice again (p=0.45).
Radiological outcome
Radiological outcomes are presented in table 3. MRI was available at 1 year for 21 (81%) operative and 27 (82%) non-operative patients. Proximal continuity was present in 20 (95%) operative and 14 (52%) non-operative patients (p<0.008). The only operative patient without proximal continuity at follow-up had sustained a reinjury due to a second water-skiing accident before the 1-year follow-up MRI. After excluding this reinjury, proximal continuity at follow-up was present in 100% of operative patients. In the non-operative group, restoration of continuity was significantly associated with tendon retraction in mm (OR 0.96, 95% CI 0.92 to 0.99, p=0.02).
Radiological outcome at 1-year follow-up
Discussion
Our prospective study of patients with proximal hamstring tendon avulsions showed that when a shared decision-making model of care was used, at 1-year follow-up: (1) clinical outcomes were comparable for operative and non-operative patients, (2) non-operative patients have better clinical outcome than previously assumed when treated using a phased rehabilitation programme and (3) proximal continuity of the hamstring complex was restored in approximately half of non-operative patients and nearly all operative patients.
Outcomes for operative and non-operative treatment groups
There is a lack of published data on non-operative outcomes. In this study, more than half of patients chose non-operative treatment after shared decision-making. This study contributes the largest group of non-operative patients to gain insight into non-operative outcomes, guide decision-making and help set patients’ expectations. While operative and non-operative treatment resulted in similar clinical outcome at 1-year follow-up, it should be noted that operative patients had lower baseline PHAT scores. It is conceivable that baseline PHAT scores in the operative group were lower because this group presented significantly earlier after injury, but could alternatively indicate worse injury and/or ‘collateral’ damage to adjacent tissues. It is unclear whether between-group differences in PHAT increase can be attributed to a treatment effect. Based on the adjusted analysis, differences in outcomes between operative and non-operative treatment may be more subtle than assumed to date.2 3 5 22 While this cannot be strongly stated because treatment was not randomly allocated, our findings indicate that further comparative studies are necessary and justified.
Aside from treatment effects, there are several potential confounders for outcome to consider as prognostic factors based on the adjusted analysis: we adjusted for injured side, tendon retraction, perinervous scarring, and days from injury to start of treatment. Tendon retraction and timing of surgery have previously been proposed as prognostic factors for clinical outcome.2 9 10 23 Accordingly, we noted that increased retraction and time from injury to start of treatment negatively impacted PHAT score improvement. Injuring the dominant leg potentially leads to more functional restrictions considering that a right-sided injury resulted in less improvement in PHAT score. Perinervous scarring on MRI also resulted in less PHAT improvement, potentially indicating that neurolysis may be required for symptom relief.
Return to sport and hamstring strength
Comparing the RTS of this study’s cohort with the existing literature reveals similar outcomes, despite our shorter follow-up. RTS is difficult to compare as it is defined variably across studies. In a recent systematic review with approximately 3 to 4 years follow-up, RTS and return to preinjury level were combined. The reported rates of RTS for operative and non-operative patients were 80% and 71%, which is in line with our findings. However, in our study a substantial proportion did so in other sports (8% in operative and 12% in non-operative patients) or at a lower level (39% and 36%). These findings indicate that return to preinjury sports at preinjury level is unrealistic within 1 year for a subset of patients. Persistent hamstring strength deficits, noted in both groups, have also been highlighted in previous smaller retrospective studies with longer follow-up.1 2 4 24 In these studies, however, operative treatment resulted in superior hamstring strength and RTS rates compared with non-operative treatment.2 24 It is possible that operative intervention is an ‘investment’ for superior long-term results, but this should be corroborated in larger prospective long-term analyses.
Continuity restoration and fatty infiltration on MRI
Radiological outcome after proximal hamstring tendon avulsion injury is sparsely reported and limited to postoperative patients. Available studies noted tendon healing after operative treatment in all cases with no-to-mild fatty infiltration of the hamstrings.25–27 We found tendon continuity in 52% of non-operative patients, mostly by a shared neotendon. While the distal semitendinosus tendon is known to ‘regenerate’ after being harvested for anterior cruciate ligament reconstruction in 60%–72%,28 this is a novel finding for the proximal hamstrings. We hypothesised that a ‘neotendon’ develops from longitudinal scar tissue in the lateral haematoma wall on resorption. Contrary to previous studies, we noted varying degrees of fatty infiltration in a substantial proportion of patients. Its clinical significance is unknown. Fatty infiltration in rotator cuff injury has been linked to decreased muscle function29 and appears irreversible after a certain stage,30 with potential implications for prognosis. It is conceivable that fatty infiltration is associated with hamstring strength deficits.
Strengths and limitations
Strengths include a prospective study design and a uniform rehabilitation protocol for both groups. Obvious limitations include the lack of random treatment allocation, lack of assessor blinding for clinical outcome, and the relatively small sample size. These limitations introduce risk of selection bias and assessor bias. The radiologist assessing radiological outcomes was blinded to clinical data, however, the presence of suture anchors on the follow-up MRI revealed which treatment the patient had undergone. As the shared decision-making process evolved over time, despite being beneficial for patient care, reproducibility is affected. Due to shared decision-making, psychosocial differences in addition to baseline differences in demographics and injury characteristics can be expected. Due to the duration of follow-up in this study, conclusions regarding long-term outcomes cannot be drawn.
Implications for clinical practice and future research
This study can serve to set patient expectations and underlines the clinical value of a shared decision-making model. Outcomes at 1-year follow-up were equally good in both groups with high patient satisfaction. More than 90% of patients stated that they would opt for the same treatment again. This indicates that the shared decision-making model succeeds in selecting the appropriate treatment for the individual patient in a predominantly middle-aged population. Our findings and conclusions cannot be generalised to elite athletes.
We recommend this approach until evidence-based indications for operative intervention are available. Regardless of treatment choice, patients should be informed that return to preinjury level of sports is unrealistic for the majority within the first year. Residual isometric strength deficits and fatty infiltration on MRI are expected. Proximal continuity of the hamstring complex was restored in approximately half of non-operative patients and nearly all operative patients.
As operative repair serves to restore continuity, it is worth investigating whether specific factors (eg, retraction, mechanical stimulus) can predict or influence spontaneous continuity restoration. By determining prognostic factors, indications for operative repair may be established. In particular, an in-depth analysis of the effect of tendon retraction on continuity restoration, collateral (nerve) damage and consequently functional outcome in a larger sample of non-operative patients would be beneficial to determine its role in decision-making and identify an evidence-based cut-off value. Large prospective analyses should determine whether there are long-term differences in outcomes between operative and non-operative treatment. Our findings indicate that clinical equipoise exists in the described study population, paving the way for randomised controlled trials.
Additionally, the decision-making process would benefit from future studies exploring which patient-specific and injury-specific factors predict the choice for operative or non-operative treatment.
Conclusion
In a shared decision-making model of care, both operative and non-operative patients with a proximal hamstring tendon avulsion have comparable clinical outcomes at 1 year follow-up. Operative patients started with lower pre-treatment PHAT scores, but improved substantially to reach equally high PHAT scores as non-operative patients. There were no clinically relevant between-group differences in secondary clinical outcome measures. Operative repair resulted in a significantly higher rate of proximal continuity. Proximal continuity of the hamstring complex was restored in approximately half of non-operative patients and nearly all operative patients. We recommend using this shared decision model of care until evidence-based indications in favour of either treatment option based on high-level clinical trials are available.
Summary box
What are the findings?
Clinical outcomes at 1-year follow-up after proximal hamstring tendon avulsion are comparable for operative and non-operative patients in a shared decision-making model.
Non-operative patients have better clinical outcome than previously assumed when treated using a phased rehabilitation programme.
Restoration of proximal continuity on MRI was observed in approximately half of patients without surgical intervention.
How might it impact on clinical practice in the future?
Reported outcomes can guide shared decision-making, clinical equipoise, and setting patients’ expectations.
A shared decision model of care can be used as both treatment options appear favourable, but future high-level clinical trials are necessary.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This observational prospective study was exempted from ethical review by the IRB as it followed our regular care protocols with exception of the questionnaires (METC, Amsterdam UMC, the Netherlands, #W17_231). All patients provided written informed consent.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AvanderMade
Contributors ADvdM (guarantor) was involved in study design, data collection, data analysis, data interpretation and drafting. RWP and CV were involved in data collection and drafting. FS was involved for his radiological expertise, assessment of MRIs and drafting. GR, MHM, JLT and GMMJK were involved in study design, data interpretation and drafting.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.