Article Text

Abstract
Purpose To determine associations between thermal responses, medical events, performance, heat acclimation and health status during a World Athletics Championships in hot-humid conditions.
Methods From 305 marathon and race-walk starters, 83 completed a preparticipation questionnaire on health and acclimation. Core (Tcore; ingestible pill) and skin (Tskin; thermal camera) temperatures were measured in-competition in 56 and 107 athletes, respectively. 70 in-race medical events were analysed retrospectively. Performance (% personal best) and did not finish (DNF) were extracted from official results.
Results Peak Tcore during competition reached 39.6°C±0.6°C (maximum 41.1°C). Tskin decreased from 32.2°C±1.3°C to 31.0°C±1.4°C during the races (p<0.001). Tcore was not related to DNF (25% of starters) or medical events (p≥0.150), whereas Tskin, Tskin rate of decrease and Tcore-to-Tskin gradient were (p≤0.029). A third of the athletes reported symptoms in the 10 days preceding the event, mainly insomnia, diarrhoea and stomach pain, with diarrhoea (9% of athletes) increasing the risk of in-race medical events (71% vs 17%, p<0.001). Athletes (63%) who performed 5–30 days heat acclimation before the competition: ranked better (18±13 vs 28±13, p=0.009), displayed a lower peak Tcore (39.4°C±0.4°C vs 39.8°C±0.7°C, p=0.044) and larger in-race decrease in Tskin (−1.4°C±1.0°C vs −0.9°C±1.2°C, p=0.060), than non-acclimated athletes. Although not significant, they also showed lower DNF (19% vs 30%, p=0.273) and medical events (19% vs 32%, p=0.179).
Conclusion Tskin, Tskin rate of decrease and Tcore-to-Tskin gradient were important indicators of heat tolerance. While heat-acclimated athletes ranked better, recent diarrhoea represented a significant risk factor for DNF and in-race medical events.
- exercise
- hot temperature
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The globalisation of sport (eg, mega-events such as the Olympics or FIFA world cups for the first time in South-America, Asia, Africa or Middle-East) alongside global warming and congested competition calendars increasingly expose athletes to hot conditions. While an air-conditioned stadium was used during the recent 2019 athletics World Championships (WC), this is evidently not possible for endurance road-race events. Unfortunately, despite some retrospective analyses,1 2 there is a paucity of data on how hot ambient conditions affect the physiological responses, health and performance of elite athletes during competition.
In-competition studies report core temperatures ≥40.0°C (a threshold commonly used to determine the severity of exertional heat illness (EHI))3 in asymptomatic endurance athletes,4 with some elite athletes reaching as high as 41.5°C.5 While most athletes remain asymptomatic when competing in the heat,6 severe EHI (ie, exertional heat stroke (EHS)) is one of the two main causes of death in athletes.7 8 EHI risk is increased in athletes with a previous EHI and/or a recent episode of illness (predominately gastrointestinal),6 9 while heat acclimation is the most important countermeasure to protect athlete health and performance in hot ambient conditions.10 11 Despite this, only 15% of athletes acclimated in 2015, before the Beijing athletics WC.12 The following year, educational materials were developed by the International Cycling Union and 38% of cyclists acclimated in 2016, before the cycling WC in Doha.13 World Athletics further developed similar educational material in 2019, ahead of the Doha WC (online supplemental appendix 1). However, the subsequent proportion of athletes who acclimated for this event remained to be determined; and the relationship between acclimation, previous EHI, recent illness and thermal responses, remain largely unclear, particularly within elite male and female athletes. Such data would help tailor preventive measures with greater validity to elite competition, given current measures are currently based predominately on non-elite athlete data.
Supplemental material
The current study aimed to initially determine athletes’ thermal responses during the male and female road-races of the 2019 Doha WC, alongside ascertaining their preparation strategies and health-status before the event (eg, acclimation strategy, recent illness, etc). The overall objective was to establish any differences and/or association between these factors and the risk of did not finish (DNF) or suffering an in-race medical event.
Methods
Design
This cross-sectional study included: (i) a pre-race questionnaire; (ii) an in-race monitoring of core (Tcore) and/or skin (Tskin) temperatures and (iii) a retrospective analysis of the medical events and performance. Athletes were free to participate in any measures of this cross-sectional study irrespective of completing other measures.
The study was conducted during the road-races of the Doha WC (27 September–6 October 2019), held in hot and humid environmental conditions (table 1). The marathons, 20 km (20KRW) and 50 km (50KRW) race-walks were completed on 7 km, 1 km and 2 km loop laps, respectively. All road-races were held during the night with starting times between 23:30 and midnight (table 1).
Races and athletes characteristics
Participants
All athletes competing in the marathons, 20KRW and 50KRW (n=305) could participate. They were informed of the project through their national federations, coaches or support staff. Tskin (n=107 athletes) and Tcore (n=56 athletes) were measured, with 83 athletes completing the prerace questionnaire. The 80 athletes visiting the medical facilities were classified as per the International Institute of Race Medicine classification (by their attending physician and the WC chief medical officer) and 10 of them were not included for final analyses (8 presented for injury plus 2 were discharged without symptoms); leaving 70 athletes with in-race medical events (ie, related to illness) to be analysed. The sample sizes for the different comparisons are presented in table 2.
Number of participants for the different measures
Measures
Core temperature
Tcore (precision 0.1°C; sampled every 30 s) was continuously recorded using e-Celsius ingestible capsules (BodyCap, Caen, France). Athletes ingested the capsule 4–6 hours prior to their event, encouraging transit through the stomach into the gastrointestinal tract while minimising pill-loss through defaecation.5 Peak Tcore (consistently observed at the end of race) alongside Tskin during the last lap, were used to calculate the Tcore-to-Tskin gradient at the end of the event. For DNF, the end of their event was determined as the point of race abandonment.
Nude skin temperature
Tskin (average of the frontal, lateral and posterior nude areas) was recorded during the first and last lap of the races via thermal cameras (FLIR A6750sc and FLIR T1030sc).14 Details are provided in online supplemental appendix 2.
Supplemental material
Performance
Ranking and finishing times were extracted from official race results, with the latter expressed as a percentage of the athlete personal best at the time of the WC (PB; obtained from World Athletics’ official starting list).
Questionnaire
Participants completed a preparticipation questionnaire (available in 12 different languages; online supplemental appendix 2) similar to the questionnaire developed and used before the 2015 athletic WC12 and the 2016 cycling WC.13 The questionnaire surveyed: (i) demographic data such as sex; (ii) EHI history; (iii) recent illness during the 10 days preceding the event and (iv) heat-acclimation strategy.
Environmental conditions
Measured every 30 min using a heat stress metre (Kestrel 4400, Boothwyn, Pennsylvania, USA) mounted on a tripod ~1.5 m above the floor, ~4 m from the course (near the start/finish line).
Statistical analyses
Data were analysed in Wizard (V.1.9.41, Evan Miller). The thermal responses (eg, Tcore, Tskin or Tcore-to-Tskin gradient) were analysed through two-tailed t-tests when comparing two categories (eg, sex, or yes/no for previous history of EHI, recent illness or acclimation) and analysis of variance when comparing multiple categories (eg, event). The categorical variables (eg, number of medical events vs sex or yes/no for previous history of EHI, recent illness or acclimation) were compared using χ2 tests. Sidak adjustments were applied for multiple comparisons. Two-tailed alpha was set at ≤0.05. Data are presented as mean±SD.
Results
From 305 starters, 219 athletes finished their race (72%), 75 DNF (25%) and 11 were disqualified (during race-walks). No differences in age, height or body mass were observed between finishers and DNF (all p≥0.337, table 1). Finishers completed their event 12%±7% slower than their PB (table 1).
Thermal responses
Peak Tcore was 39.6°C±0.6°C (independent of event, p=0.499).15 The Tcore of the DNF athletes (p=0.150), or of athletes with a medical event (p=0.576), were not different from other athletes (figure 1). Conversely, DNF finished their race with a higher Tskin than finishers Tskin during their final lap (32.0°C±1.4°C vs 30.6°C±1.2°C, p<0.001, figure 1). The absolute Tskin decrease during the entire race (−0.1°C±1.1°C vs −1.5°C±0.9°C, p<0.001) and the rate of Tskin decrease per kilometre (0.00°C/km±0.07°C/km vs −0.05°C/km±0.04°C/km, p<0.001) were lower in DNF than in finishers. Similarly, athletes with a medical event had a lower Tskin rate of decrease per kilometre than others (−0.03°C/km±0.05°C/km vs −0.06°C/km±0.06°C/km, p=0.011).
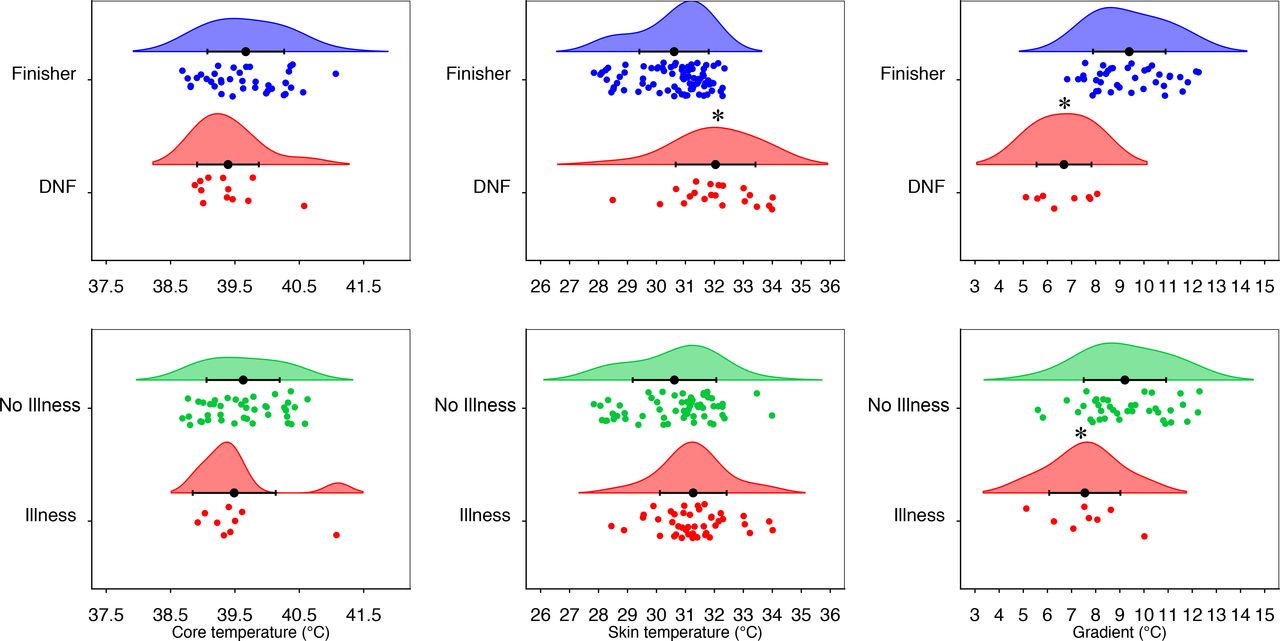
Rain clouds30 of the core temperature, skin temperature and core to skin temperature gradient at the end of the races. Mean±SD and individual values for the did not finish (DNF)/finishers (top panels), and for the athletes being/not being admitted to the medical facility for an in-race illness (bottom panels); *p<0.05.
While potentially affected by early withdrawal, the Tcore-to-Tskin gradient was lower in DNF athletes than in finishers (6.7°C±1.2°C vs 9.4°C±1.5°C, p<0.001; figure 1). Athletes with a medical event had a lower Tcore-to-Tskin gradient than others (7.6°C±1.5°C vs 9.0°C±1.7°C, p=0.029).
Medical events
Fifty-seven per cent (n=43) in DNF vs 17% (n=37) in finishers (p<0.001) visited the medical facility including: 20 exercise-associated collapse; 16 exercise-associated muscle cramps; 16 heat-exhaustion; 12 gastrointestinal disturbances; 1 heat-exhaustion with exercise-associated collapse and 1 heat-exhaustion combined with gastrointestinal disturbances. No EHS was diagnosed in the medical tent. One athlete was transferred to a hospital emergency ward (possible panic attack) and was discharged some hours later.
Average systolic/diastolic blood pressures were 115±13/69±13 mm Hg at admission, with an extreme value of 73/40 mm Hg in a female marathoner diagnosed with hypotensive collapse and dehydration (discharged after intravenous fluid replacement and leg elevation). Most athletes were conscious (100%) and alert (94%), but required assistance (wheelchair (n=33), stretcher (n=12), buggy (n=7), ambulance (n=3); while 17 walked-in).
Previous EHI
Of the survey responders, 61% had previously experienced a variety of EHI symptoms while training/competing in the heat (eg, cramping, headache, nausea) and 17% of all responders declared to have been previously diagnosed with EHI. Cramping was the most common symptom previously experienced (26.5%) as well as the most common complaint at the medical facility during the WC (9%, n=27).
The DNF subsample was not associated with a history of EHI symptoms (p=0.459) or EHI diagnosis (p=0.860). The peak Tcore was also similar between athletes with a history of EHI and others (39.6°C±0.6°C vs 39.6°C±0.6°C, p=0.968). However, in-race medical events were higher in athletes with a previous history of EHI symptoms (16/51 or 31% vs 4/32 or 13%, p=0.050).
Recent illness
Of the responders, 33% declared symptoms of illness during the 10 days preceding their event (independent of event; p=0.116) (figure 2). Overall, this was not associated with DNF (p=0.688) or in-race medical events (p=0.385). The most common symptom was insomnia (figure 2). Only three athletes reporting insomnia had their Tcore monitored (peak Tcore 39.5°C, 40.3°C and 40.7°C).

Recent illness (in the 10 days preceding the World Championships). *P<0.05.
The second most commonly reported symptom, diarrhoea (9% of all athletes) was more prevalent in the athletes suffering an in-race medical event than in others athletes (5/17 or 29% vs 2/60 or 3%, p<0.001). Concerningly, 71% (ie, 5/7) of athletes reporting a diarrhoea episode in the 10 days preceding the competition suffered an in-race medical event vs 17% (ie, 12/70) of the athletes not reporting recent diarrhoea (p<0.001, figure 2). Moreover, although not statistically significant (p=0.167), 43% of the athletes with recent diarrhoea DNF (ie, 3/7) vs only 20% (ie, 13/65) of the other athletes. The final Tcore (39.8°C±0.8°C vs 39.6°C±0.6°C, p=0.549) and Tskin (31.1°C±1.8°C vs 30.8°C±1.4°C, p=0.734) were not statistically different between athletes with and without recent diarrhoea.
Heat acclimation
Most athletes (80%, independently of event, p=0.596) had some form of heat exposure before the current WC. The proportion of athletes with a dedicated 5–30 days heat preparation period was 63%, depending on event (p=0.049), with a lower prevalence in marathon than 50KRW (48% vs 82%, p=0.028; 20KRW 63%, figure 3). Within the athletes training in the heat, the methods also differed between events (p=0.049) with 83% of marathon runners relying on natural outdoor heat only, whereas 33% of the 50KRW and 55% of the 20KRW trained in a hot room (figure 3). Similarly, the proportion of athletes incorporating passive heat exposure during their taper was lower in marathoners (21%) than in race-walkers (55%) (p=0.010).

{kind=link}
{kind=link}
{kind=link}
Proportion of athletes who acclimated for 5–30 days ahead of the World Championships (top left), main methods for acclimation (bottom left) and effects on other variables (right panel). DNF, did not finish; HA, heat acclimation; Live, athletes declaring to live in a hot country; Medical, admittance to the medical facility for in-race illness; temp, temperature; 20KRW, 20 km race-walk; 50KRW, 50 km race-walk.
Athletes who acclimated had a non-significantly lower Tcore at the start (−0.2°C, p=0.095) and a significantly lower peak Tcore (−0.4°C, p=0.044) compared with athletes who did not acclimate (figure 3). Athletes who acclimated had a non-significantly higher Tskin during the first lap (+0.7°C, p=0.060) that was compensated by a larger decrease during the race (−1.4°C±1.0°C vs −0.9°C±1.2°C, p=0.060) and no differences in final Tskin (p=0.646). Athletes who acclimated ranked better during their race (18±13 vs 28±13, p=0.009), but the relative performance was not different (112.6%±5.1% PB vs 113.3%±7.3% PB, p=0.643). Lastly, although not statistically significant (p≥0.179), 30% (n=9/30) and 32% (n=10/31) of the athletes who did not acclimate were respectively DNF or in-race medical event, versus only 19% (n=9/47 and n=10/52) of the athletes who acclimated (figure 3).
Sex
There were no differences between sexes regarding whether athletes had some form of heat exposure (78% vs 81%, p=0.731), a 5–30 days acclimation period (56% vs 68%, p=0.242), a recent illness (38% vs 29%, p=0.426), a previous history of EHI (12% vs 21%, p=0.307) or DNF (p=0.355). Women had faster relative performance than men in the 20KRW (p<0.001) and 50KRW (p=0.006), but a slower relative performance on the marathon (p<0.001, likely related to the difference in environmental conditions, table 1).
The proportion of women with an in-race medical event was higher than men (32% vs 17%, p<0.001). This difference was however likely due to the different environmental conditions during the women and men marathons (table 1) as there was no effect of sex on the prevalence of in-race medical event during race-walks (p=0.597), where environmental conditions were similar.
The peak Tcore was not different between women and men (39.5°C±0.6°C vs 39.6°C±0.6°C, p=0.544). The final Tskin was higher in women than men (31.5°C±0.8°C vs 30.4°C±1.6°C, p<0.001). Whereas this may be largely related to large differences during the marathons (31.5°C±1.2°C vs 29.0°C±1.1°C, p<0.001), the final Tskin of the women was also marginally higher than the men during the race walk (31.5°C±0.4°C vs 31.0°C±1.4°C, p=0.145). The Tcore-to-Tskin gradient was significantly lower in women than men (7.8°C±0.9°C vs 9.3°C±1.9°C, p=0.005), but only during the marathon.
Discussion
The current project aimed to determine the athletes’ thermal responses and preparedness for a WC held in hot-humid conditions. First, athletes commonly reach Tcore above 40.0°C with the maximum Tcore observed during the 20KRW (41.1°C); confirming that the highest Tcore are not always reached during the longest events.5
Second, there were 70 medical encounters related to in-race illness. An increase in environmental heat stress has been reported to increase the number of heat-related illness cases in international marathon and race-walk events.2 Given that up to 13 athletes required a wheelchair during a single event (women’s marathon, table 1), the current study suggests that event organisers should consider a 1:5 wheelchairs to starters ratio for WC road-races in hot and humid conditions.
Third, numerous athletes (26.5%) reported to have previously experienced cramping when exercising in the heat. This proportion is similar to that reported in elite long-distance athletes (25.5%)12 and cyclists (26%).13 Cramping was also the most frequently observed complaint at the medical facility (9%). While most muscle cramps are attributed to premature muscle fatigue,16 the current observation support that exercising in the heat may still promote cramping in some athletes.17
Fourth, there was no consistent effect of sex on relative performance, refuting the common belief that women are at a greater disadvantage than men when competing in the heat. Indeed, most differences arise from anthropometric differences and sex per se does not significantly affect thermal responses, except during intense exercise in dry heat allowing full sweat evaporation.18–20 Thus, in the humid conditions of the current WC, where sweat rates exceeded the maximal evaporation rate possible, the effect of sex on performance was likely trivial.21 Moreover, a retrospective analysis of 7 international athletic championships revealed 132 cases of heat illnesses, but did not observe sex differences.2 No effects of sex were also observed for heat-related illness in elite cycling13 and beach volleyball.6 Yet, this latter study reported that 60% of the heat-related medical time-outs were among women,6 and the current study also showed a higher proportion of women than men suffered a medical event (although due to the higher ambient temperatures during the women’s). Also, Tcore >41°C were only observed in female athletes both during the 2016 cycling WC5 and the current athletic WC. Overall, there may be an effect of sex on the sensitivity to heat in elite athletes, but it appears marginal as compared with the large effects of exercise heat stress per se.
Fifth, despite an elevated 41% DNF during the women’s marathon, a Spearman’s rank correlation showed that the overall DNF proportion did not differ from previous WC (p=0.206, based on public data since 1983) (online supplemental appendix 3). However, as compared with the standing World record at the time of each WC (ie, to account for the evolution of performance across three decades), completion time was relatively slower at the 2019 WC than previous WC (p<0.001, online supplemental appendix 3). Therefore, the main performance consequence of heat in elite athletes was a reduction in speed (ie, a lower absolute intensity), likely due to the attempted maintenance of the same relative intensity (eg, heart rate).22
Supplemental material
Sixth, the fact that 63% of athletes heat-acclimated for 5–30 days indicates increased awareness of, as well as increased number of athletes adopting heat acclimation. Indeed, only 15% and 38% of the athletes undertook heat acclimation prior to the 2015 athletic WC12 and 2016 cycling WC,13 respectively. This increase likely reflects the efficacy of educational material produced by the International Cycling Union (UCI) ahead of the 2016 cycling WC and then by the International Association of Athletics Federations (IAAF) ahead of the 2019 athletic WC (online supplemental appendix 1). While marathoners were less inclined to have a dedicated heat acclimation block, this could be partially explained by the fact that more marathoners than race-walkers declared living in hot countries, and thus may have considered it not necessary to perform specific acclimation (figure 3).
Seventh, a third of the athletes declared symptoms of illness during the 10 days preceding their event. This is a worrying increase compared with the 13% of athletes reporting symptoms during the 4 weeks preceding the 2015 athletics’ WC,23 or the 22% of cyclists reporting symptoms during the 10 days preceding the 2016 cycling WC (ie, same questionnaire as the current study).13
Risk factors and countermeasures
The leading objective of the current project was to determine the associations between the above responses and the risk of DNF or medical event. For example, it has been shown that 19% of amateur runners experienced illness symptoms in the 8–12 days preceding a long distance endurance event, increasing their risk of DNF ~twofold.24 In the current study, there was no overall relationship between DNF or in-race illness and a recent symptom (the most common symptom being insomnia possibly due to the races being held close to midnight). However, the second most common symptom, diarrhoea, was a major risk factor for in-race medical events (figure 2). This confirms a recent retrospective analysis of beach volleyball WC and world-tour events suggesting that a recent episode of diarrhoea increased the severity of heat-related medical time-out.6 Considering the changes in gut microbiota and gastrointestinal symptoms affecting thermoregulation when exercising in the heat,25 it is likely that starting a race in a hot and humid environment with less than optimal gastrointestinal health/function may impose increased thermoregulatory challenges. The deleterious effect of diarrhoea on the capacity to exercise in the heat is likely multifactorial (including hydration and electrolyte level) as final Tcore (39.8°C±0.8°C vs 39.6°C±0.6°C, p=0.549) and Tskin (31.1°C±1.8°C vs 30.8°C±1.4°C, p=0.734) were not statistically different between athletes with and without recent diarrhoea. The current data also confirm that EHI history is a risk factor for experiencing a medical event when competing in the heat,9 but to a lower extent than a recent diarrhoea.
Heat acclimation is the most important preventative countermeasure to protect athlete health and performance in hot ambient conditions.10 11 In line with laboratory data showing that heat acclimation lowers Tcore for a given exercise load (and sometimes at rest),26 the current data show a non-significant lower Tcore at the start and a significantly lower peak Tcore in competition (figure 3). Importantly, athletes who acclimated had a better finishing position (figure 3), although it may reflect a general tendency for the best athletes to better prepare rather than a different relative performance. It is also noteworthy that >30% of non-acclimated athletes DNF and/or suffered an in-race medical event, versus only 19% of the acclimated athletes (figure 3).
In the effort of determining the associations between the various physiological and pathophysiological responses to competing in the heat, a new technology was also deployed (online supplemental appendix 2) to provide the first in-race Tskin measures ever obtained.14 Although it is important to reaffirm that Tcore is the clinical criterion to diagnose EHS and associated risk of organ damage, the current data showed that higher Tskin and a reduced Tcore-to-Tskin gradient are important indicators of the athlete’s ability to cope with heat stress, finish the race and/or potentially require medical attention (figure 1). This confirms for the first time, during outdoor elite competition, that the Tcore-to-Tskin gradient is a central component of exercise capacity in the heat.27 Indeed, a lower gradient requires a higher skin blood flow to maintain a given level of heat dissipation.28 Importantly, the current WC road-races were contested at night and further studies remain necessary with different thermal loads.
Limitations
The current data represent a snapshot of the 2019 WC, held late in the season, during a pre-Olympic year and at night. Variations in events, period or time may lead to slightly different observations. Given the ‘real-world’ observations performed, not all athletes provided all information and they were free to follow their usual routines without any restrictions imposed by the research team. Therefore, values such as skin temperature may have been affected by the different cooling strategies of the athletes. Future studies should obtain nuanced detail behind DNF and medical events. The results from previous WC are presented only for context and complete retrospective analyses of the relationships between weather, health and/or performance are available elsewhere.2 29
Conclusion
The present study is the first to determine the association between athletes’ thermal responses, preparation, health status, medical events and performance during a ‘real-world’ elite sporting event held in a hot-humid environment. Heat acclimation is increasingly practised and demonstrates various ‘real-world’ benefits for elite athletes competing in the heat. However, the prevalence of precompetition illnesses is concerning and a recent diarrhoea episode was markedly associated with an in-race medical event. Our results also challenge some current beliefs and practices such as considering Tcore ‘only’. Tskin and Tcore-to-Tskin gradient are shown here to be important indicators of the athlete’s ability to cope with heat stress.
Summary box
What is already known on this topic?
Athletes commonly reach core temperatures >40.0°C when competing in the heat.
The risk factors for developing exertional heat stroke are unclear but acclimation may be an important countermeasure to protect health and performance.
What are the findings?
Skin temperature, its rate of decrease and the core-to-skin temperature gradient (but not core temperature per se, 39.6±0.6°C) were related to did not finish (DNF) or an in-race medical event.
Nine per cent of surveyed athletes had diarrhoea in the 10 days preceding the World Athletics Championships, increasing their likelihood of DNF (from 20% to 43%) and an in-race medical event (from 17% to 71%).
Sixty-three per cent of athletes had a dedicated heat acclimation of 5–30 days.
They were better ranked, less likely to DNF or have an in-race medical event, alongside having lower thermal strain than the other athletes.
How might it impact on clinical practice in the future?
Real-time measuring technologies under development should integrate skin temperature monitoring.
Health status during the 10 days preceding a competition in the heat should be closely monitored, with a particular attention to diarrhoea.
Educational materials on heat acclimation should be promoted to assist athlete preparation for hot weather events.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Anti-Doping Lab Qatar Institutional Review Board (E2019000302) and conformed to the current Declaration of Helsinki guidelines. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the World Athletics Health and Science Department for their endorsement, financial and operational support. The authors thank the local organising committee for their operational support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ephysiol, @Ihsan_mo, @paolo_emilio, @DrJuanMAlonso, @Marco_Cardinale, @NicolvanDyk, @chris_esh, @goipergormance, @Louidoc, @DrNathanT
Contributors SR designed the study and is responsible for the overall content as guarantor. All authors contributed to data collection and/or analyses. All authors revised the manuscript and approved the final version.
Funding This study was supported by World Athletics (formerly International Association of Athletics Federations).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.