Article Text

Abstract
Objectives At present, there is no cure for osteoarthritis (OA), but severe hip joint degeneration can require total hip arthroplasty (THA). The literature on OA after elite sport is limited. We hypothesise that elite athletic activity increases the risk of receiving a THA later in life.
Methods We linked a cohort of former Norwegian world-class athletes (1402 females and 1902 males, active 1936–2006) to the Norwegian Arthroplasty Register (THA performed 1987–2020). We used standardised incidence ratio (SIR), one-minus Kaplan-Meier and relative Cox regression (relative HR, RHR), with 95% CIs, and funnel plots at age 75, to assess THA risk for different sport disciplines, joint impact categories of sport disciplines and sex. The risk of THA for the corresponding general Norwegian population was used as reference.
Results We found an overall increased risk for THA for the former elite athletes (SIR 2.11, 95% CI 1.82 to 2.40) at age 75 years, compared with the general population. THA risk at age 75 years was 11.6% for female athletes and 8.3% for male athletes. SIR was 1.90 (95% CI 1.49 to 2.31) for female and 2.28 (95% CI 1.87 to 2.70) for male athletes. Among males, high joint impact sport disciplines were associated with increased risk compared with low-impact sport disciplines (RHR 1.81, 95% CI 1.06 to 3.08, p=0.029).
Conclusion Having been an elite athlete was associated with a doubling of THA risk compared with the general population for both sexes. High joint impact sport disciplines were associated with subsequent THA for male athletes.
- athletes
- sport
- hip
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The long-term effects of elite athletic activity on hip health are unclear.
WHAT THIS STUDY ADDS
This study found a doubled risk of total hip arthroplasty (THA) among former elite athletes compared with the general population for both sexes. Approximately 1 in 9 former elite female athletes and 1 in 12 former elite male athletes had received a THA by age 75.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Lifestyle, activity and rehabilitation strategies to reduce the development and progression of hip OA in former elite athlete should be considered.
Introduction
Globally, hip and knee osteoarthritis (OA) is the 11th highest contributor to disability.1 Joint replacement surgery may be the final result of severe, symptomatic and long-term OA. The indications for total hip arthroplasty (THA) surgery vary, but typically include pain, loss of function, radiological changes and failed conservative therapy (mainly exercise and pharmacological treatment).2 In the Norwegian Arthroplasty Register (NAR), the reason for surgery is reported as idiopathic OA in 74.1% and trauma sequelae (secondary OA) in 7.7% of cases.3 With an increasing prevalence of OA,4 knowledge on potential modifiable risk factors for OA development is vital. High age and female sex are known unmodifiable risk factors for hip OA.5 Established modifiable risk factors include increased body mass index (BMI) at a young age,6–8 injury9 and occupation.10 11 Further hip joint specific risk factors include acetabular dysplasia12–14 and the bony morphological variants of cam morphology,14 15 the latter with higher incidence among athletes than among the general population.16–19
Physical activity, including elite athletic activity, has been regarded as a potential modifiable risk factor,5 though study findings are inconclusive. Biomechanical modelling suggests that moderate mechanical loading is necessary for cartilage homeostasis,20 21 supported by clinical studies showing cartilage thinning in spinal cord-injured individuals.22 In vitro studies on explant models indicate that cyclic, intermittent cartilage loading stimulates chondrocyte metabolism.21 Another hypothesis is that muscle weakness plays a role in the pathogenesis of OA,23 and evidence shows that exercise therapy is beneficial in the early management.24–27 Surprisingly, leisure time physical activity, defined as the amount of leisure time being physically active, including commuting to and from work, may increase the risk of receiving arthroplasty.28 Heavy manual work has also been associated with increased prevalence of OA29–32 and an increased risk of early THA revision.33 Preliminary evidence also suggests that tactical personnel (firefighters, military service and veteran parachutists) have a greater incidence and prevalence of OA.34
Participation in certain sport disciplines, or categories of sport disciplines, have been associated with a higher prevalence of hip and knee OA.35 36 A study of former National Football League players found that OA prevalence depended on field position.37 A 2017 systematic review investigated the risk of hip OA in male elite athletes and found a fivefold increase in risk for handball players36; but also identified a paucity of data on female athletes. Another systematic review, from 2016, concluded that elite sport participation increased the risk for OA, but that the evidence was weak.38 Study design limits the conclusions that can be drawn from these reviews with many case–control or cross-sectional studies included.39–46 Evidence from a small number of longitudinal studies show an increased risk of OA with increasing levels of activity.47–49
Clifford and Mallon created a joint impact classification based on a literature review and their clinical experience, and it has since been applied to compare OA risk across sports.36 39 50 Some data suggest that high joint impact sport disciplines increase the risk of developing hip OA, apart from long-distance running.36 One study, on male athletes only, found an increased risk of receiving an arthroplasty after high joint impact sports participation (soccer, handball, hockey).39
Robsahm et al 51 established a cohort of 3428 former Norwegian world-class athletes to study their risk for cancer compared with the Norwegian population and between sport disciplines. This large cohort provides an ideal opportunity to clarify the relationship between hip health and participation in a variety of elite sport disciplines. We linked this cohort of former athletes with a national register of all patients receiving THA. We aimed to investigate the influence of elite athletic activity on THA risk later in life. Our hypothesis is that elite athletic activity increases the risk of receiving a THA later in life.
Methods
Participant data linkage
The included cohort of former Norwegian world-class athletes51 consisted of athletes from 51 different sport disciplines, who had represented Norway in international championships or been ranked top three in domestic championships from 1936 through 2006. In 2006, the athletes received an invitation letter with a questionnaire, including a request for consent to participate in the cohort. Of the 3427 athletes, 3386 consented to participating in further studies on lifestyle disease.
The NAR was established in September 1987 and contains data on all THAs in Norway, with a 98% completeness of reporting.52 On 31 October 2020 by applying the unique 11-digit identity number of Norwegian citizens, we linked the elite athletes to the NAR for information on THA. On the same date, we also obtained data on death and emigration through from the National Population Register of Norway.
Data preparation
The main independent variable of interest related to the risk of receiving a THA in our study was sport discipline. In addition, the joint impact classification (table 1), was applied to categorise sport disciplines in subgroups.50 We considered sport disciplines not included in the classification as ‘unclassified’. Age, sex and adolescent BMI (weight and height at age 20 was obtained from the questionnaire) was adjusted for in the analyses.
Sport disciplines represented in the cohort of Norwegian world-class athletes and their category of joint impact after the classification of Clifford and Mallon50
The cohort of former Norwegian world-class athletes established by Robsahm was used to identify elite athletes in the NAR. From the questionnaire, age of first national or international competition, age of retirement from athletic carrier and anthropometric measures were obtained. The hips of the athletes were followed in NAR until age of receiving a primary THA, age of death emigration, or age at 31 October 2020 (end of follow-up), whichever occurred first. For athletes who retired from active sport before 1 September 1987, we used their age on 1 September 1987 as age at start of follow-up. Death, emigration and end of follow-up were considered censored observations. If the first registered THA was a revision surgery (removing or replacing a previous THA), the follow-up was censored at the age of the revision. The follow-up period, and hence age, for the athletes started at establishment of the NAR (1 September 1987); data on athletes retired before this date were analysed as left-truncated. The athletes may experience bilateral THAs; hence, hip was considered as the unit of observation, resulting in two records per athlete.53 Median age of follow-up was calculated according to Schemper and Smith.54
Statistical analysis
Descriptive statistics of demographic data are presented as mean values with SD for continuous variables, and as frequencies with percentages for categorical variables.
We applied time-to-event analysis to analyse the total effect of sport discipline on receiving a primary THA.
Standardised incidence ratios (SIRs) were calculated according to Andersen and Vaeth.55 Population rates for THA were calculated for sex, and in 1-year intervals for age and calendar year, using the entire NAR and population tables from Statistics Norway. We calculated SIR with 95% CIs separately for males and females through 10 000 bootstrap replicates. To account for bilaterality, the bootstrap replicates were calculated over 2000 individuals/athletes (and not per hip).
The total risk of receiving THA was calculated as one minus Kaplan-Meier probabilities. One minus the expected survival curves for receiving THA in the Norwegian general population (with the same composition of sex, age and calendar year as the athlete cohort) were calculated using the rates for receiving a THA based on the number of THAs per individual in the entire Norwegian population according to Lie et al.56
Due to small sample sizes for the individual sport disciplines, we calculated funnel plots for the risk of receiving THA at 60, 65, 70, 75 and 80 years of age for the athletes. Only figures at 75 years are presented, since the median age for receiving a THA is 74 years.57 The funnel plots were based on 5000 bootstrap replicates of the calculated one minus survival for all included sport disciplines. The funnel plots are presented with 95% CIs and 99% CIs in addition to one minus the expected survival at the given age. Sport disciplines with less than five observations at 75 years were omitted.
To adjust for potential confounders, in the total effect for receiving a THA, we applied Cox regression models, with robust variance estimates to account for bilateral THAs. Furthermore, relative Cox regression comprising the population rates for THA as an offset, was carried out.58 The RHR (adjusted relative HR) mimics (‘is close to’) the ratio of the calculated SIRs of the categories of the variables included in the model. Due to a strong assumption in the relative Cox model, the RHRs will not equal the fraction of the SIRs at 75 years of age. Due to increased exercise levels among elite athletes the last decades,51 we analysed the relative Cox regressions separately for retirement from elite athletic activity before (and after) 1975.
The statistical package ‘R’ (R Foundation for Statistical Computing, Vienna, Austria) was used to calculate SIRs, observed and expected survival probabilities, Funnel plots, functional form for continuous variables in the relative Cox regressions, and Schoenfeld residuals for the relative Cox regressions. The statistical package Stata V.17 (StataCorp) was applied for the relative Cox regressions. P values less than 0.05 were considered statistically significant.
Patient and public involvement
The former hurdler Harald Gjengedal (deceased April 2021) was involved as a patient representative in our study, and contributed especially in initial discussions.
Equity, diversity and inclusion
Both male and female authors contribute to the present article. A sizeable proportion of female athletes are included in the study.
Results
Descriptive statistics
Of the 3386 athletes, 82 athletes deceased before the start of NAR in 1987 and were therefore excluded from the analyses. Thus, 3304 athletes were included in the analyses (figure 1).

Flow chart showing participants from the original cohort of Norwegian world-class athletes and participants included in the data set of this study.
The final dataset contained 51 different sport disciplines (table 1). There were 1394 former elite athletes (651 females) from 12 high joint impact, 403 (159 females) from 8 intermediate joint impact, 744 (239 females) from 12 low joint impact and 763 (353 females) from 19 unclassified sport disciplines. Wrestling, boxing, ski jumping, Nordic combined and archery had no female representation.
For females and males, respectively, the inclusion age (age at questionnaire) was 42.3 (SD=14.8) and 51.0 (SD=17.5), the mean career length was 10.7 (SD=5.7) and 13.3 (SD=5.9) years, and the mean age at retirement was 26.7 (SD=6.1) and 29.9 (SD=6.0) years (table 2). A total of 257 THA operations were reported. There were 31 revision THAs, of which 26 were excluded and 5 censored at revision. Thus, we included 226 primary THAs in the analyses; of these, 45 athletes had bilateral THA (90 hips) and 136 were unilateral. During follow-up, 484 athletes had died and 24 emigrated (low impact: 171; intermediate: 74; high impact 120; unclassified 144). The total follow-up time was 187 322 person-years. Median follow-up age was 53.7 (IQR: 44.7–65.0).
Descriptive statistics (numbers (N), mean with SD or percentage (%) and median with IQR) for demographic data of the study sample
Risk analysis
The overall risk for female athlete to receive a THA before age 75 years was 11.6% (95% CI 8.7% to 14.3%), while it was calculated to be 7.0% in the general population. For male athletes, the risk was 8.3% (95% CI 6.8% to 9.8%), while it was 3.9% in the general population.
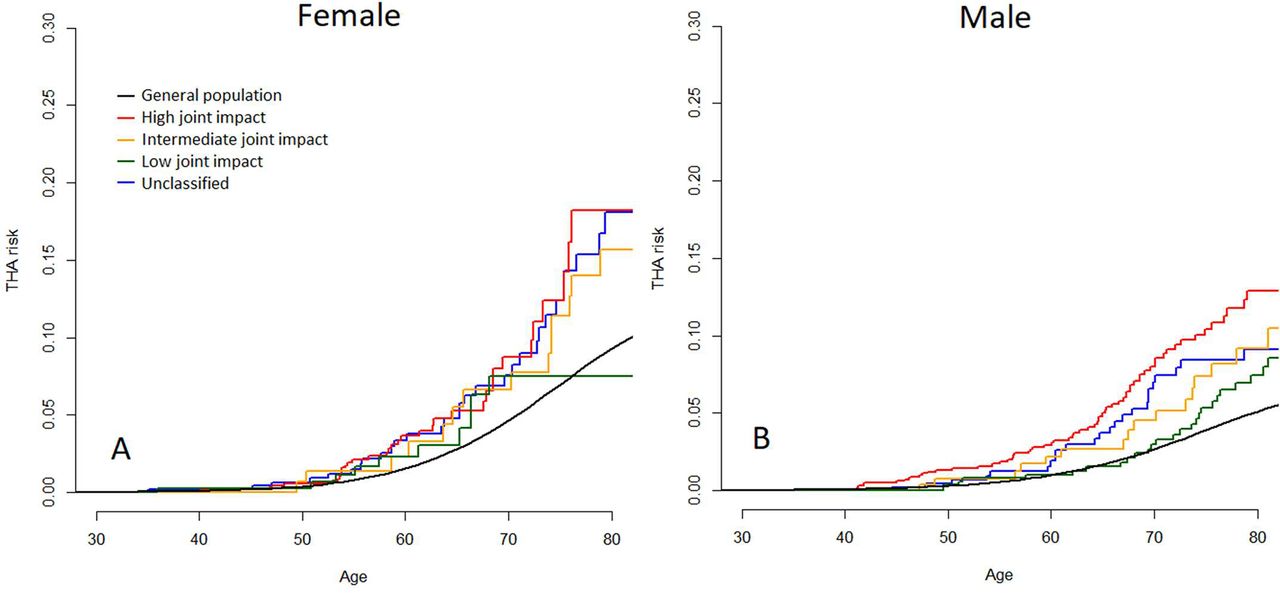
The SIR for receiving a THA before age 75 years was 2.11 (95% CI 1.82 to 2.40) for former elite athletes in comparison to the general population. For female athletes SIR was 1.90 (95% CI 1.49 to 2.31), while it was 2.28 (95% CI 1.87 to 2.70) for male athletes. The increased risk of receiving THA for both sexes, compared with the general population, is illustrated with the calculated one minus survival curves in figure 2.

One minus Kaplan-Meier curves showing the probability of THA at different ages for female athletes and male athletes. The athletes are categorised by high, intermediate, low or unclassified joint impact sport participation, and compared with the Norwegian general population. THA, total hip arthroplasty.
In unadjusted Cox regression, we found that female athletes had an increased risk of THA compared with male athletes (HR 1.47; 95% CI 1.07 to 2.02). However, the relative Cox regression adjusted for the THA risk in the general population showed no increase for females (RHR 0.87, 95% CI 0.64 to 1.19).
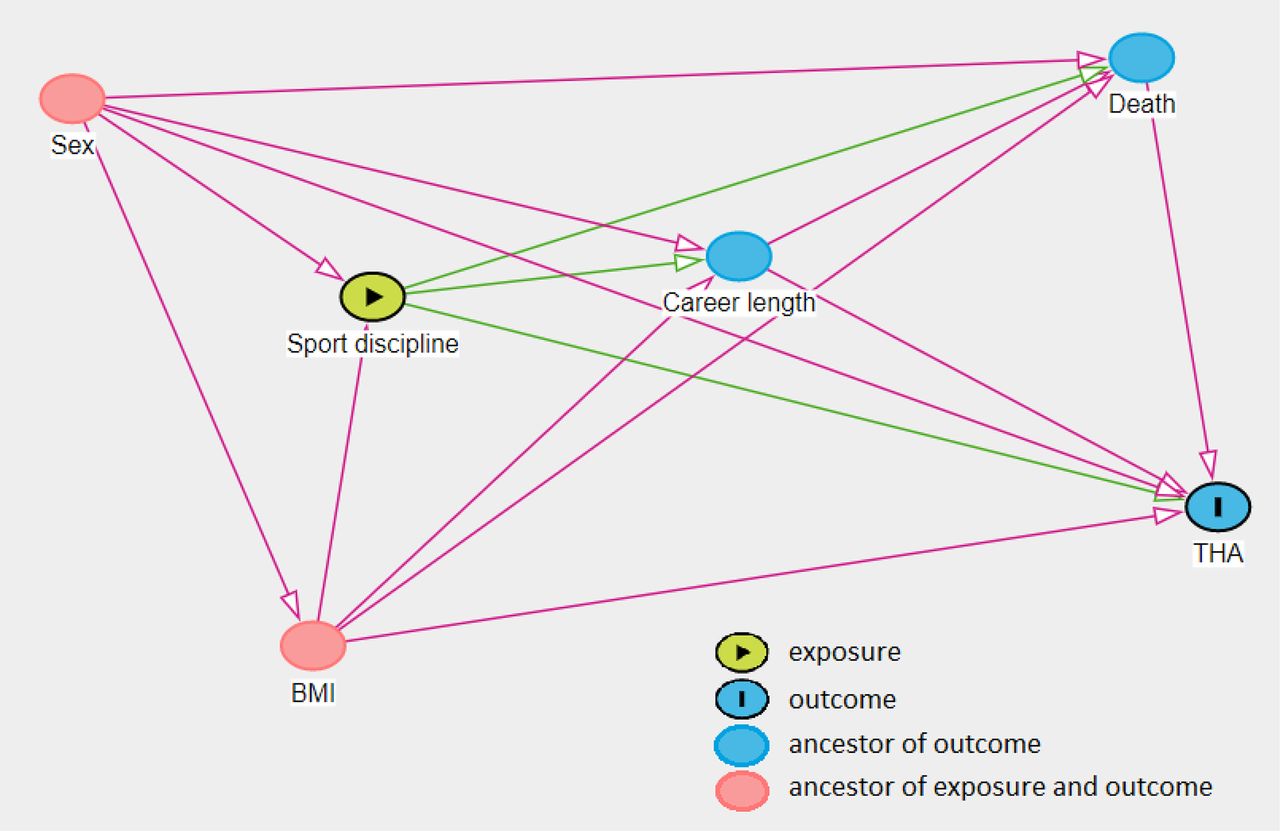
Using directed acyclic graphs (DAGs, figure 3), sex and BMI at 20 years of age were identified as potential confounders for the total effect of sport discipline on the risk for receiving a THA.

Direct acyclic graph (DAG), showing the minimal sufficient adjustment sets containing BMI and sex for estimating the total effect of sport discipline on total hip arthroplasty (THA). BMI, body mass index.
For females, we found no significant differences between the sport impact categories (table 3, figure 2A). For males, sport disciplines defined as high impact had a significantly higher risk for THA than the low impact category (table 3, figure 2B). This finding was only present for male athletes active after 1975 (RHR 2.34, 95% CI 1.23 to 4.46, p=0.010).
Standardised incidence ratio (SIR) and relative HR (RHR) (adjusted for BMI and sport classification) of THA in female and male former athletes
Unadjusted analysis of career length showed no association with THA risk for females (RHR 1.01 95% CI (0.98 to 1.04), p=0.618) and males (RHR 1.01 95% CI (0.98 to 1.04), p=0.428). For females, we found that those with a BMI >25 kg/m2 at age 20 years had a 6.8 times increased risk compared with those with a BMI <20 kg/m2 (p=0.001), while a BMI of 20–25 kg/m2 had a 2.6 times increased risk (p=0.002) (table 3). When stratified by sex, the relative Cox regression and the standard Cox regression gave similar results (not presented). The unadjusted analyses gave practically the same results as the adjusted analysis.
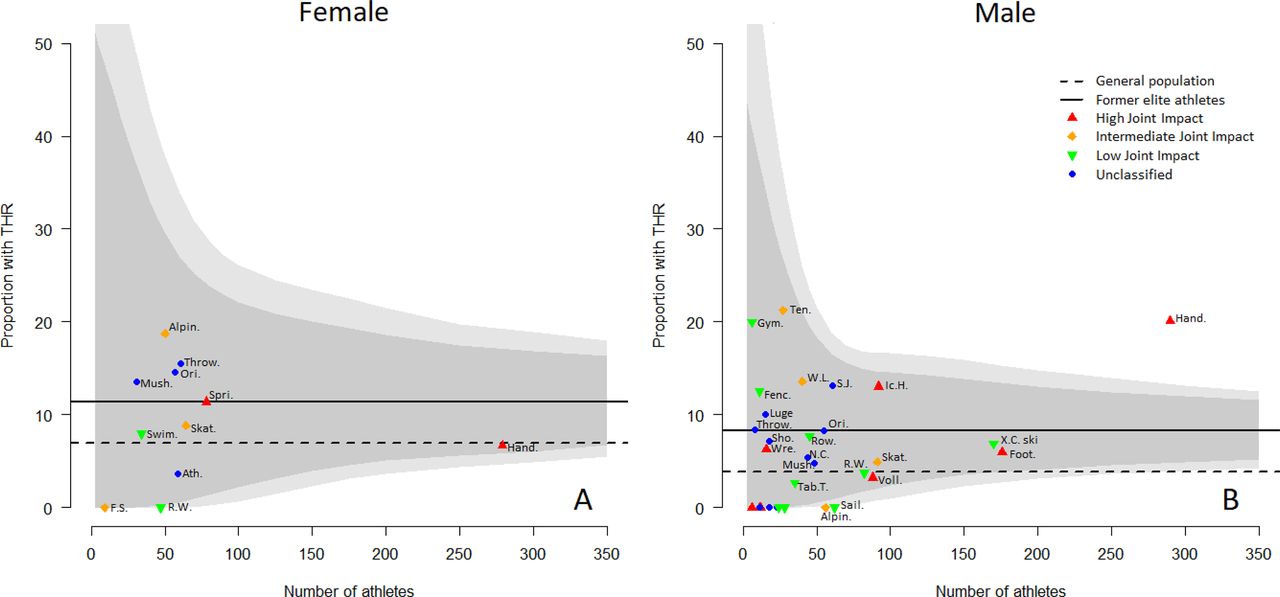
The funnel plot displaying the different sport disciplines show a zero risk of THA at age 75 years among female racewalkers (figure 4A). For males, a zero risk at 75 years was seen in sailing and alpine skiing. The proportion of male handball athletes receiving THA (20.1%) was five times higher than in the general population, and outside the 99% confidence limits for the average risk for male athletes at 75 years of age (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plots showing proportion of 75 year-old former female and male athletes with THAs in the cohort of Norwegian world-class athletes. The funnels show the 95% and 99% confidence level. The solid horizontal line is the average of the cohort. The dotted horizontal line is the average for the corresponding general population. Sport disciplines: Alpin., alpine ski; Ath., Athletics (high jump, long jump, pole vault, triple jump); Fenc., fencing; Foot., football (US soccer); F.S., figure skating; Gym., gymnastics; Hand., handball; Ic.H., ice hockey; Mush., mushing; N.C., Nordic combined; Ori., orienteering; R.W., race walking; Row., rowing; S.J., ski jumping; Sail., sailing; Sho., shooting; Skat., skating; Swim., swimming; Tab.T., table tennis; Ten., tennis; Throw., discus throw, hammer throw, javelin throw, shot put, weight throw; Voll., volleyball, indoor and beach; W.L., weight lifting; Wre.,wrestling; X.C. ski, cross-country and biathlon.
When comparing female handball players to female athletes in other sport disciplines with more than 30 athletes, no differences in THA risk were found. For males, football, X.C. skiing (cross-country and biathlon), alpine skiing, skating, mushing, and the merged group of sports with less than 40 athletes all had a significantly lower risk of receiving a THA compared with handball (online supplemental tables 1 and 2).
Supplemental material
Using a test of the slope for scaled Schoenfeld residuals, we found that for females the proportionality assumption in the relative Cox model was accepted (smallest p=0.199). For males, we found deviations for the proportionality assumption for impact and BMI (p<0.05), but not for career length.
Discussion
Key findings and interpretation
At present, this is the most extensive study on this topic so far, due to a high number of participants, female representation, a longitudinal design and the large number of sport disciplines represented. Overall, having been an elite athlete was associated with a doubled risk of THA when compared with the general population, both for female and male athletes. Female athletes had the highest absolute risk, but males had the highest relative risk (risk increase) when compared with the respective female and male general population. Approximately 1 in 9 former elite female athletes and 1 in 12 former elite male athletes received THA, compared with approximately 1 in 16 females and 1 in 26 males of the general population. As elite athletes represent the highest healthy segment of a population,59 their elevated risk of THA may be thought as remarkable.
The population risk of THA at 75 years of age in our study was lower than the female 16.0% and male 8.3% lifetime risk calculated by Ackerman et al.60 This is not unexpected, since Ackerman et al calculated the risk based on the average life expectancy (83.8 years) for the Norwegian population and risk of hip OA and subsequent THA increases with high age.3 9
We found that the different joint impact categories had similar or higher risk of THA compared with the general population. For male athletes, low joint impact sport disciplines had the lowest risk of THA (RHR=1), while high joint impact sport disciplines had the highest risk (RHR=1.81). This finding is in line with previously reported studies on male athletes.39–49 Two sport disciplines from opposing joint impact categories (cross-country skiing and football) show similar THA risk. This may indicate a suboptimal categorisation of one or both sport disciplines, with regard to THA risk. It should be noted that a classification like the joint impact classification is fraught with uncertainty. Cross-country skiing technique may represent low impact, but training volumes can be much higher than football. Joint impact could be classified based on ground reaction force, the demand for ranges of motion, training volume/intensity, the risk of acute injuries and other factors. Not knowing how to weigh each of these factors, it seems inherently difficult to classify sport disciplines according to hip joint ‘load’. Based on the overall longitudinal risk displayed in the survival curves in this study, however, the joint impact classification did give a rough association of THA risk for elite male athletes. This fits with findings of increased prevalence of cam morphology in high impact sports of previous studies.61 For female athletes, the joint impact categories had similar risks of THA. We had fewer female athletes included and they were younger than the male athletes, and the results of subanalyses (ie, joint impact categories) could give different results with a longer follow-up. This study has filled a desperately needed gap in representation of female athletes in studies of hip OA risk, as previous studies lack results for female athletes.
For female athletes, the risk of THA increased with increasing BMI as reported at age 20, which was not found in men. This contrasts with previous findings that THA risk is associated with high BMI at a young age for both sexes,8 however, the BMI in our data set is quite homogenous with tight CIs and within normal range compared with these previous studies. While most sport disciplines included limited athlete numbers to determine the exact THA risk, a few sport disciplines with larger samples show that THA risk differed between sports. We found that former elite male handball athletes had a higher risk than athletes from other sports, in line with results from some other studies.36 39 40 Football is the most studied sport on this topic36 and groin injuries are prevalent in this sport discipline.62–64 We found the risk of THA among former elite male football athletes to be increased compared with the general population, in line with most previous studies.41 65 Former elite male cross-country skiers showed greater risk of hip OA than the general population, in line with another longitudinal study.48 For former elite female athletes, handball had similar risk as the general population, considerably lower than for their male counterparts. We do not have a clear explanation of this difference, but the aforementioned low number of older female athletes, especially in the high joint impact category, may explain this finding. Most other sport disciplines have too few participants for an exact risk estimate. However, it is noteworthy that certain sport disciplines (race walking for females, alpine skiing and sailing for males) showed lower or no THA risk in our study. If some sport disciplines lower the THA risk, this could be valuable (eg, when searching for hip protective factors). Longitudinal studies with larger sample sizes are needed for this risk assessment.
Strengths, limitations and impact on clinical practice
Several sport disciplines in this study have not been investigated previously. Limitations of the study are the low number of participants in some sport disciplines, shorter follow-up of female athletes, and the lack of and THA’s before 1987. The width of the CIs, for example, in figure 4, shows the uncertainty and low statistical power of our estimates in sports with few athletes. History of injury and occupation are two unmeasured potential confounders. Recall and response bias may have influenced the original data collection. The RHR estimates are subject to built-in selection bias and should be interpreted with care. The relatively low number of THAs prevents a sensible subanalysis on different causes of receiving the THA.66 Furthermore, the mechanisms leading to THA for elite athletes can be multiple and complex, rendering the surgeon-reported cause of THA of minor interest in this study. We have used hip as the unit and adjusted for clustering of hips within individual in the analyses. We consider this to strengthen the analyses, since athletes in sport disciplines with a high risk may have bilateral THAs, which both will be included in the analyses. Still, it is important to take multiple observations per individual into account in the analyses.53 We found deviations for the proportionality for impact and BMI for males, thus care should be taken in the interpretation of these regression coefficients.
Our findings are primarily generalisable to elite athletes of northern European origin, as the cohort of former Norwegian world-class athletes includes athletes with participation in international competitions or finishing top three in national competitions. However, all athletes of approximately the same training and competition history (eg, serious youth athletes, athletes on high national levels) may be thought to have a similar risk, even if they did not reach the medal podium. The results are less generalisable to leisure time exercisers.
We recommend that elite athletes are targeted for hip OA prevention efforts. For males, this is more important for athletes from the high joint impact sport disciplines than the low joint impact sport disciplines. Further studies are needed to determine the accurate risk of sport disciplines other than male handball, football and cross-country skiing, and to determine why former elite male handball athletes have such a high risk. With the expected increase of OA in the coming decades,4 further studies to answer these questions should be feasible.
Conclusion
Former elite athletes have a doubled THR risk compared with the general population for both sexes. Approximately 1 in 9 former elite female athletes and 1 in 12 former elite male athletes had undergone THA. The joint impact classification is associated to THA risk in former elite male athletes, but its association to THA risk for former elite female athletes is unclear.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Norwegian Regional Ethics Committees approved this study, Reference number ID(s): 2009/2455 REK-sør-øst C; 297112018/1782/REK-vest; 25646. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @larsengebretsen
Contributors DHN is the overall content guarantor. DHN, OF, GK, TER, MBJ, LE, LN, RB and SAL contributed to study conceptualisation, interpretation of results, and write-up and revision of the manuscript. DHN, GK and SAL performed the statistical analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.