Article Text

Abstract
Objectives Evaluate the natural course of anterior cruciate ligament (ACL) healing on MRI within 5 years of acute ACL rupture and compare 2-year and 5-year outcomes based on healing status and treatment group.
Methods Secondary analysis of 120 Knee Anterior Cruciate Ligament Nonsurgical vs Surgical Treatment (KANON) trial participants randomised to rehabilitation and optional delayed ACL reconstruction (ACLR) or early ACLR and rehabilitation. ACL continuity on MRI (Anterior Cruciate Ligament OsteoArthritis Score 0–2) was considered evidence of ACL healing. Outcomes included Knee Injury and Osteoarthritis Outcome Score (KOOS), KOOS patient acceptable symptomatic state (PASS) and treatment failure criteria. Linear mixed models were used to estimate adjusted mean differences (95% CIs) in patient-reported sport and recreational function (KOOS-Sport/Rec) and quality of life (KOOS-QOL) at 2 and 5 years, between participants with MRI evidence of ACL healing and those who had (1) no evidence of ACL healing, (2) delayed ACLR or (3) early ACLR.
Results MRI evidence of ACL healing at 2-year follow-up was observed in 16 of 54 (30%, 95% CI 19 to 43%) participants randomised to optional delayed ACLR. Excluding participants who had delayed ACLR, 16 of 30 (53%, 36–70%) participants managed with rehabilitation-alone displayed MRI evidence of ACL healing. Two-year outcomes were better in the healed ACL group (n=16) compared with the non-healed (n=14) (mean difference (95% CI) KOOS-Sport/Rec: 25.1 (8.6–41.5); KOOS-QOL: 27.5 (13.2–41.8)), delayed ACLR (n=24) (KOOS-Sport/Rec: 24.9 (10.2–39.6); KOOS-QOL: 18.1 (5.4–30.8)) and early ACLR (n=62) (KOOS-Sport/Rec: 17.4 (4.1–30.7); KOOS-QOL: 11.4 (0.0–22.9)) groups. Five-year KOOS-QOL was better in the healed versus non-healed group (25.3 (9.4–41.2)). Of participants with MRI evidence of ACL healing, 63–94% met the PASS criteria for each KOOS subscale, compared with 29–61% in the non-healed or reconstructed groups.
Conclusions MRI appearance of ACL healing after ACL rupture occurred in one in three adults randomised to initial rehabilitation and one in two who did not cross-over to delayed ACLR and was associated with favourable outcomes. The potential for spontaneous healing of the ACL to facilitate better clinical outcomes may be greater than previously considered.
Trial registration number ISRCTN84752559.
- anterior cruciate ligament
- rehabilitation
- Magnetic Resonance Imaging
- osteoarthritis
- quality of life
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Many people with anterior cruciate ligament (ACL) injury experience poor long-term outcomes irrespective of management with ACL reconstruction or rehabilitation alone.
A common assumption is that a ruptured ACL cannot heal, therefore current treatments aim to restore functional stability to an ACL deficient knee.
The likelihood of ACL healing and the relationship between evidence of ACL healing on MRI and patient outcomes have not been previously studied.
WHAT THIS STUDY ADDS
Approximately half of all participants randomised to rehabilitation who did not cross over to delayed ACL reconstruction (ACLR) had evidence of ACL healing on MRI at 2-year and 5-year follow-up.
People with evidence of ACL healing on MRI at 2 years reported better Knee Injury and Osteoarthritis Outcome Score (KOOS) patient-reported sport and recreational function and KOOS-quality of life scores compared with the non-healed, delayed ACLR and early ACLR groups.
A high proportion of people (63% to 94%) with evidence of ACL healing on MRI reached the patient acceptable symptom state threshold for each KOOS subscale, and no one reached the criteria for treatment failure.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings suggest that about one-third of ruptured ACLs may display evidence of healing on MRI when patients are managed with rehabilitation only, and that ACL healing may be associated with favourable outcomes compared with early or delayed ACLR or a non-healed ACL rupture managed non-surgically.
Signs of ACL healing were visible on MRI as early as 3 months after injury, and most participants who crossed over to delayed ACLR did not have signs of healing on MRI. Further research is needed to determine whether the healing status of the ACL, after an initial period of rehabilitation, should inform further treatment decisions.
If high-quality research in other samples align with our findings, the objectives of mainstream ACL injury management may evolve to include facilitation of ACL healing.
Background
In North America, Europe and Australia, most anterior cruciate ligament (ACL) ruptures are treated with ACL reconstruction (ACLR) and the rate of ACLR is increasing.1–6 However, a native ACL has a complex structure and physiology, challenging to replicate by a surgical ACL graft. This includes proprioceptive fibres that assist in stabilising the knee7 and ACL bundles that work in synchrony to provide stability throughout all ranges of knee motion.8 An alternative treatment option to ACLR is management with exercise-based rehabilitation, which aims to provide functional stability to an ACL deficient knee. Secondary analyses of as-treated groups in randomised control trials (RCTs) have found similar patient-reported and structural outcomes after management with early ACLR versus non-surgical management with exercise-based rehabilitation.9–12 Many people with ACL injury experience poor long-term outcomes irrespective of management. Poor outcomes include episodes of giving way, sport and activity limitations, rupture of the ACL graft, subsequent meniscal injuries, persistent pain, early onset of knee osteoarthritis and impaired long-term quality of life (QOL).13–17
It is possible that spontaneous healing of a ruptured ACL can result in improved patient outcomes (such as less pain, better stability and function, reduced activity limitations, better QOL and a lower prevalence of osteoarthritis). However, the likelihood of ACL healing following non-surgical management is unclear, as is the relationship between ACL healing and patient outcomes. The Knee Anterior Cruciate Ligament Nonsurgical vs Surgical Treatment (KANON) trial is the first RCT to investigate outcomes following randomisation to early ACLR and rehabilitation, versus exercise-based rehabilitation with the option of a delayed ACLR in young adults.11 A range of measures were collected, including knee MRIs, radiographs, measures of passive knee laxity and patient-reported outcomes at baseline, 3 months, 6 months and 1, 2 and 5 years, providing an ideal opportunity to investigate the potential for ACL healing and the association between ACL healing and patient outcomes.
The aims of this exploratory study were to:
Report the proportion of patients with evidence of ACL healing on MRI in the first 5 years following acute ACL rupture managed with rehabilitation and optional delayed ACLR.
Describe 2-year and 5-year outcomes (Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales, Tegner Activity Scale (TAS), passive knee laxity and radiographic osteoarthritis) stratified by ACL healing and treatment status.
Investigate the relationship between ACL healing/treatment status, patient-reported sport and recreational function (KOOS-Sport/Rec) and knee-related QOL (KOOS-QOL) at 2 and 5 years following acute ACL injury.
Methods
Design
We performed a secondary analysis using data from the KANON trial (ISRCTN 84752559), involving 120 young active adults randomised to a strategy of early ACLR plus rehabilitation or rehabilitation with optional delayed ACLR. The study was approved by the ethics committee of Lund University (LU 535-01).
Participants
Patients aged 18–35 years with an acute ACL rupture within the previous 4 weeks, who presented to the orthopaedic departments at Skåne University and Helsingborg Hospitals, Sweden, were recruited into the KANON trial. A complete ACL rupture was confirmed by MRI for all but one participant.11 Despite the appearance of a partial ACL rupture on MRI, this participant had a positive pivot shift test conducted by two independent clinicians and was, thus, considered to have complete ACL rupture (this participant was randomised to exercise therapy plus optional delayed ACLR and had evidence of ACL healing on MRI at 2 and 5 years).11 Exclusion criteria included a less than moderate activity level (<5 on the TAS), professional athletes (10 on the TAS), total collateral ligament ruptures, a full thickness cartilage lesion or extensive meniscal fixation (fixation of meniscocapsular separations of ≥10 mm, requiring a change in the postoperative rehabilitation protocol).11 Sixty-two patients were randomised to early ACLR and 59 to rehabilitation with the option of delayed ACLR. Participants were randomly assigned to a management strategy by computer-generated random numbers in permuted blocks of 20, and the sequence was concealed using opaque sealed envelopes.11 Thirty (51%) patients randomised to initial rehabilitation had a delayed ACLR within 5 years. Patients who presented with symptomatic knee instability and a positive pivot shift test after undertaking rehabilitation had a discussion with the treating orthopaedic surgeon about ACLR as a treatment option.11 Other patients chose to undergo delayed ACLR for a variety of reasons.18 Only 1 out of 121 patients was lost to follow-up within 5 years. All trial methodologies including details on management strategies have been published.11 12
Exposure
Criteria for ACL healing
MRI was performed using a 1.5 T system (Gyroscan Intera, Philips, Best, The Netherlands) with a circular polarised surface coil using identical sequences for all participants and all time points (see online supplemental appendix 1 for details on the MRI protocol). We used the Anterior Cruciate Ligament OsteoArthritis Score (ACLOAS) MRI grading system to classify ACL healing.19 All available MRI scans were read by one musculoskeletal radiologist who is a coauthor (FWR) with 11 years of experience at the time of reading in standardised MRI assessment of knee trauma and osteoarthritis. The ACLOAS was designed to facilitate understanding of the natural history of ACL injury and subsequent osteoarthritis development.19 It contains specific criteria for grading the continuity of the ACL over time, whereby the native ACL is scored from 0 to 3 at a given time point19:
Supplemental material
0=Normal ligament with hypointense signal and regular thickness and continuity.
1=Thickened ligament and/or high intraligamentous signal with normal course and continuity.
2=Thinned or elongated but continuous ligament.
3=Absent ligament or complete discontinuity.
To address the first aim, the proportion of patients scoring a 0, 1, 2 or 3 on the above criteria at each follow-up time point will be reported. To address the second aim, a binary cut-off was applied, whereby a score of 0–2 was considered ‘evidence of ACL healing’ on MRI (ie, MRI evidence of continuity of the ACL), and a score of 3 was considered ‘non-healed’ on MRI (ie, MRI evidence of discontinuity of the ACL). Intraobserver reliability for grading the continuity of the ACL using the ACLOAS was 1.00 (baseline, all time points and longitudinal change) and interobserver reliability was 1.00, 0.84 and 0.59 (baseline, all time points and longitudinal change). Per cent agreement was 100% for intraobserver evaluation and 100%, 90.0% and 84.6% for inter-observer assessment (baseline, all time points and longitudinal change).20
Outcomes
KOOS subscales
The KOOS comprises five subscales: pain, symptoms, activities of daily living, sport and recreational function and QOL and was developed for use in people with knee injury or knee osteoarthritis.20 We have a priori chosen the KOOS-Sport/Rec and KOOS-QOL subscales as our primary outcomes. They are valid and reliable for use in people with ACL injury and have the highest content validity and the greatest room for improvement compared with other KOOS subscales.21 KOOS subscales (excluding the activities of daily living subscale which is of low relevance and results in a high ceiling effect in young and active ACL-injured individuals) at 2-year and 5-year follow-up were also reported descriptively.
To aid with interpretation of findings, we used KOOS thresholds corresponding to patient acceptable symptomatic state (PASS) and treatment failure that were calculated in a random sample of people in the Norwegian knee ligament register, 6–24 months following ACLR, based on responses to two questions22 (online supplemental appendix 1).
Osteoarthritis
One experienced musculoskeletal radiologist who is a coauthor (FWR) with 11 years of experience at the time of reading in standardised assessment of knee trauma and osteoarthritis, unaware of treatment allocation and clinical data, graded radiographs (frontal plane posteroanterior radiographs, sagittal plane radiographs of the tibiofemoral compartment and patella axial radiographs in weight bearing).12 Presence of ≥1 of the following criteria in ≥1 compartment (medial tibiofemoral, lateral tibiofemoral) was used to classify radiographic osteoarthritis of the tibiofemoral joint12:
Joint space narrowing grade ≥2.
Sum of the two marginal osteophyte grades from the same compartment=grade ≥2.
Grade 1 joint space narrowing plus grade 1 osteophytes in the same compartment.
For the patellofemoral joint, a similar definition was applied using only grading of osteophytes, as assessment of patellofemoral joint space narrowing was not performed.
Criteria were graded according to the Osteoarthritis Research International Atlas23 and approximates a grade 2 classification of osteoarthritis on the Kellgren and Lawrence Scale.24
Tegner Activity Scale
The TAS25 was used to assess the level of activity participation prior to injury and at 2-year and 5-year follow-up. Scores range from 0 (disability pension due to knee) to 10 (competition in elite sport).
Passive knee laxity
Passive knee laxity was assessed with the pivot-shift test at 2 and 5 years (combined tibiofemoral internal rotation and anterior tibial translation, whereby a grade 0 or 1 was classified as ‘normal’ or ‘nearly normal’,26 27 the Lachman’s test28 at 2 and 5 years (0 or 1 was classified as ‘normal’ or ‘nearly normal’ translation) and a KT-1000 (MEDmetric) arthrometer28 at 2 years (anterior tibial translation in millimetres, the mean of three tests performed at 134 newtons was calculated) by one of two experienced clinicians (performed ACLRs for ≥15 years and ≥40 ACLRs per year), who were not blinded to treatment assignment.11
Data analysis
Baseline characteristics and secondary outcomes were presented using descriptive statistics (means and SD or frequencies and percentages) and KOOS subscale trajectories depicted using line graphs. The number and proportion of people meeting KOOS subscale criteria for PASS22 29 and treatment failure22 29 at 2-year follow-up were reported, stratified by healing status and treatment group.
We estimated proportion with healed ACL on MRI for all participants randomised to rehabilitation plus optional delayed ACLR (participants who had delayed ACLR were assigned a non-healed status) and participants managed with rehabilitation alone (ie, those who had not crossed over to delayed ACLR at each time point) with Agresti-Coull CIs for proportions. Primary outcomes (KOOS-Sport/Rec and KOOS-QOL) were analysed using mixed linear regression models. The model fit was checked using diagnostic plots and the assumptions were judged as fulfilled. Models included the exposure (healing/treatment status: ACLOAS score 0–2 vs ACLOAS score 3, ACLOAS score 0–2 vs delayed ACLR, ACLOAS score 0–2 vs early ACLR), time points (1, 2, 5 years), their interaction and baseline KOOS subscale values as fixed effects. Individual was included as random effect. We then fitted similar models, but with adjustment for confounders (age, sex and smoking). In our primary analysis, the healing/treatment status was allowed to vary between time points. In a sensitivity analysis, we fitted the same models but with the healing/treatment status at 2 years as exposure. The model diagnostics for both KOOS-Sport/Rec and KOOS-QOL variables were satisfactory, despite small deviations from the assumption on normality of residuals and random effects. Due to the limited sample size within subgroups, 95% CIs informed our interpretation of findings rather than point estimates. Missing MRI data are described in online supplemental appendix 1.
Results
We included 120 participants from the KANON trial, 62 randomised to early-ACLR plus rehabilitation and 58 to rehabilitation with optional delayed ACLR (n=1 randomised to rehabilitation with optional delayed ACLR was excluded due to missing MRI data at all relevant follow-up time points). Four persons had missing healing status at 2 years, and four (different) persons at 5 years. Participant characteristics are reported in table 1.
Baseline characteristics stratified by management strategy at 2-year follow-up, and ACL healing status as visualised on MRI at 2 years after acute ACL injury
Aim 1: evidence of ACL healing on MRI
In participants randomised to rehabilitation plus optional delayed ACLR, 16 out of 54 (30%, 95% CI 19 to 43%) at 2-year follow-up displayed evidence of ACL healing on MRI. At that time point, 24 participants had crossed over to delayed ACLR and were all considered as non-healed in the above estimate. However, 3 of 15 participants who had delayed ACLR and frequent MRIs had evidence of ACL healing on MRI before crossing over to delayed ACLR (table 2). In participants (n=30) managed with rehabilitation alone at 2 years, 53% (95% CI 36 to 70%) had evidence of ACL healing on MRI at 2 years. At 5 years, 58% (95% CI 39 to 76%) of participants managed with rehabilitation alone (n=24) had evidence of ACL healing on MRI at 5-year follow-up (table 2).
The healing status of the ACL as visualised on MRI following acute ACL rupture managed with rehabilitation±delayed ACLR
Figure 1 depicts an example of ACL healing (normalisation) on MRI, over the 5-year period. Additional examples of ACL healing as visualised on MRI, and an example of non-healing, are provided in online supplemental appendix 2.
Supplemental material
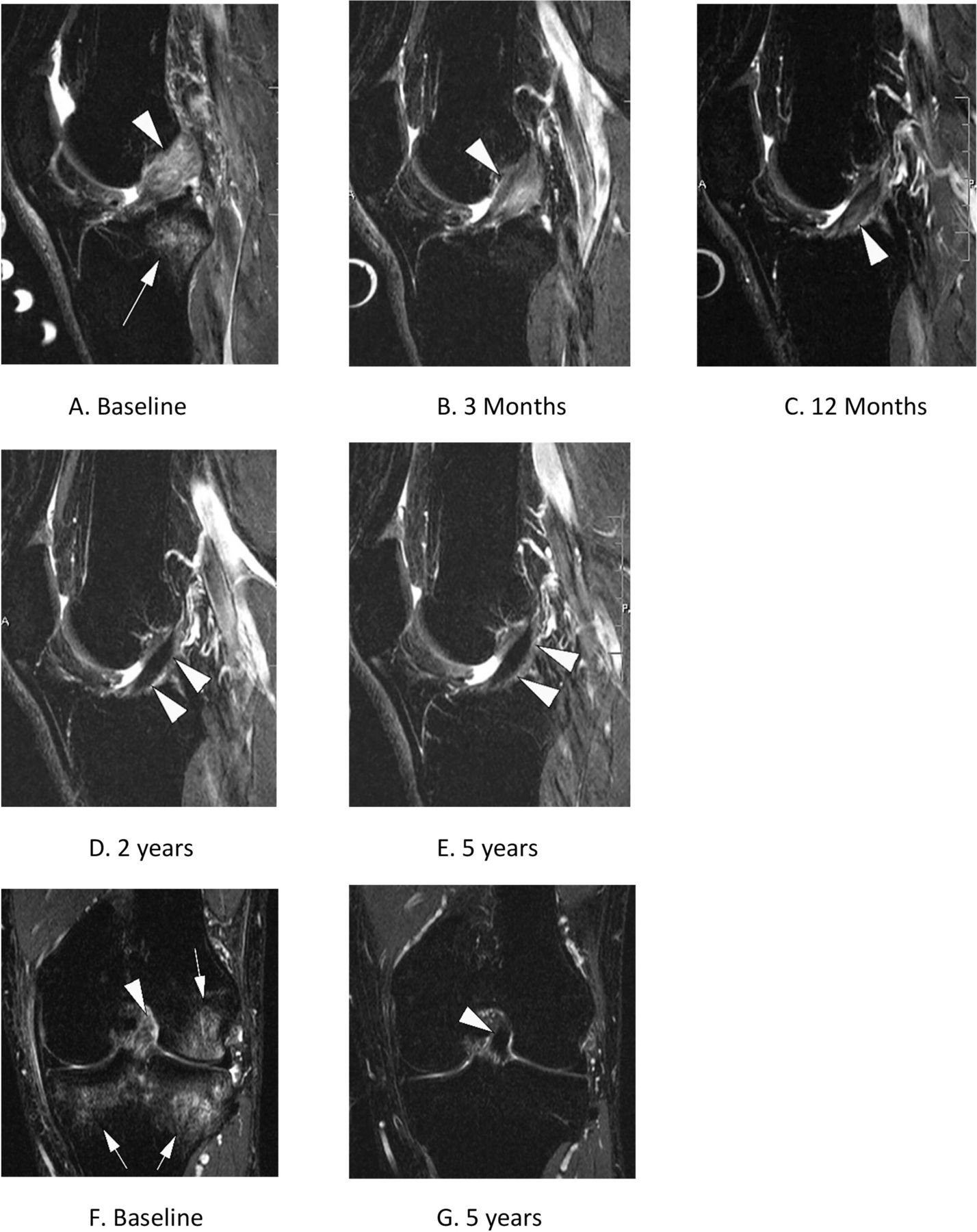
Evidence of ACL healing on MRI over 5 years in a KANON study participant (male, aged 31 years at the time of injury) randomised to rehabilitation and optional delayed ACLR. (A) Baseline sagittal short tau inversion recovery (STIR) MRI shows complete disruption of the ACL, which is depicted as a hyperintense thickened structure (arrowhead). In addition, image depicts a characteristic traumatic bone marrow lesion (also referred to as bone contusion) in the posterior lateral tibia (arrow). (B) 3-month follow-up MRI shows complete resolution of bone contusion. There is beginning scar formation with partial hypointensity in the course of the ACL. Scar is still markedly thickened. (C) At 1 year, there is near-complete normalisation of scar formation with a re-ligamentisation and regular course. There is some remaining intraligamentous hyperintensity (arrowhead). (D) 2 years after the injury there is complete normalisation of structure and signal indicating healing of the ligament. (E) At 5 years persistent normalisation with regular ACL course and signal intensity is depicted (arrowheads). (F) Corresponding coronal STIR MRI at baseline confirms the disrupted hyperintense ACL near the proximal femoral attachment (arrowhead). There are large bone contusions at the medial and lateral tibia and lateral femur (arrowheads). (G) At 5 years, normalisation with a now hypointense healed ACL is shown also in the coronal STIR image. There is compete resolution of bone contusions. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; KANON, Knee Anterior Cruciate Ligament Nonsurgical vs Surgical Treatment.
Only 4 out of 12 (33%) participants who had an MRI at 3 months and did not cross-over to delayed ACLR had a complete ACL rupture (ACLOAS grade 3) on 3-month MRI, compared with 13 of 14 (93%) who crossed over to delayed ACLR within 5 years. Individual patient trajectories depicting ACL healing status over time (as visualised on MRI at 3, 6, 12, 24 and 60 months follow-up) are presented in online supplemental appendix 3.
Supplemental material
Aim 2: 2-year and 5-year outcomes stratified by ACL healing and treatment status
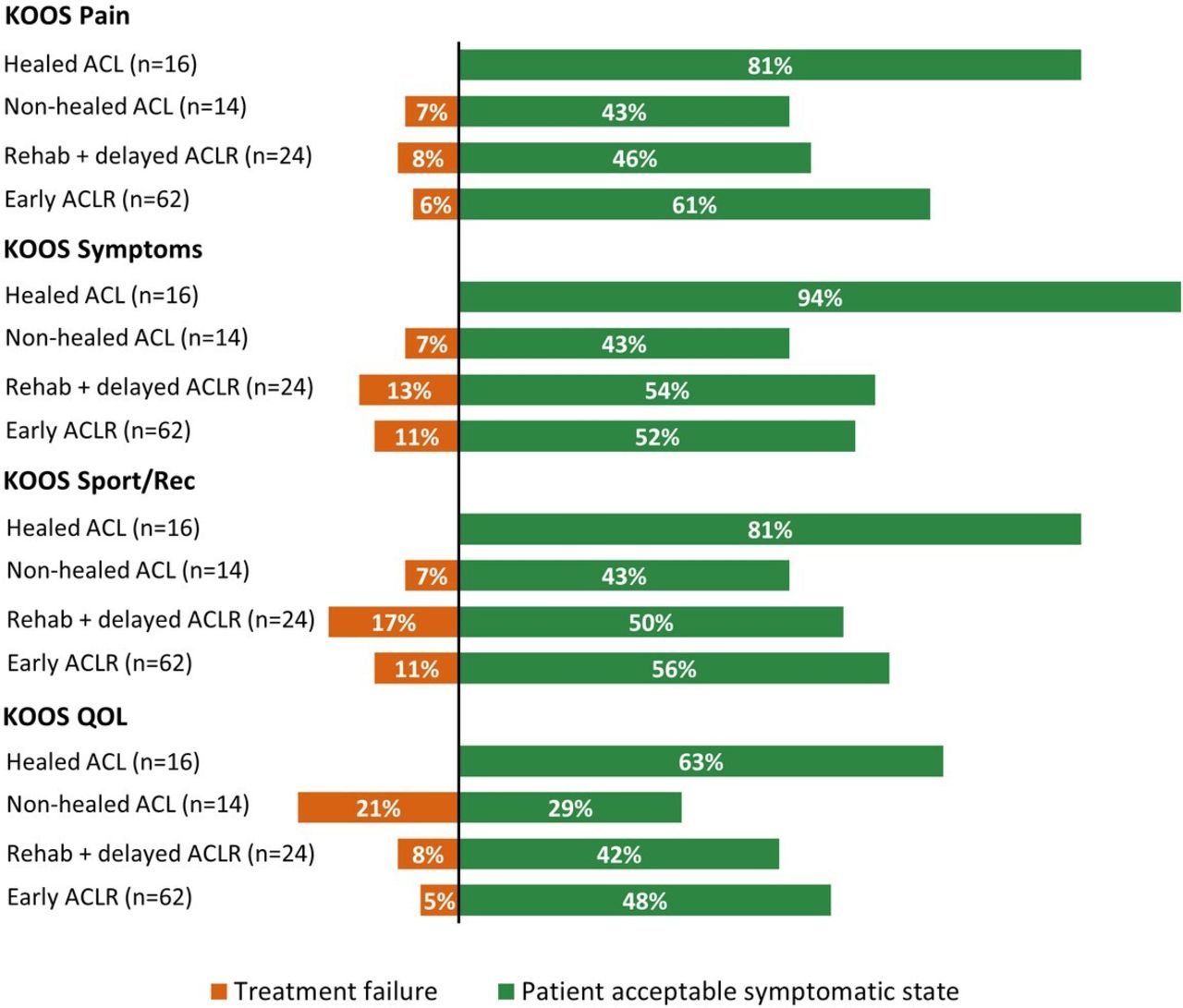
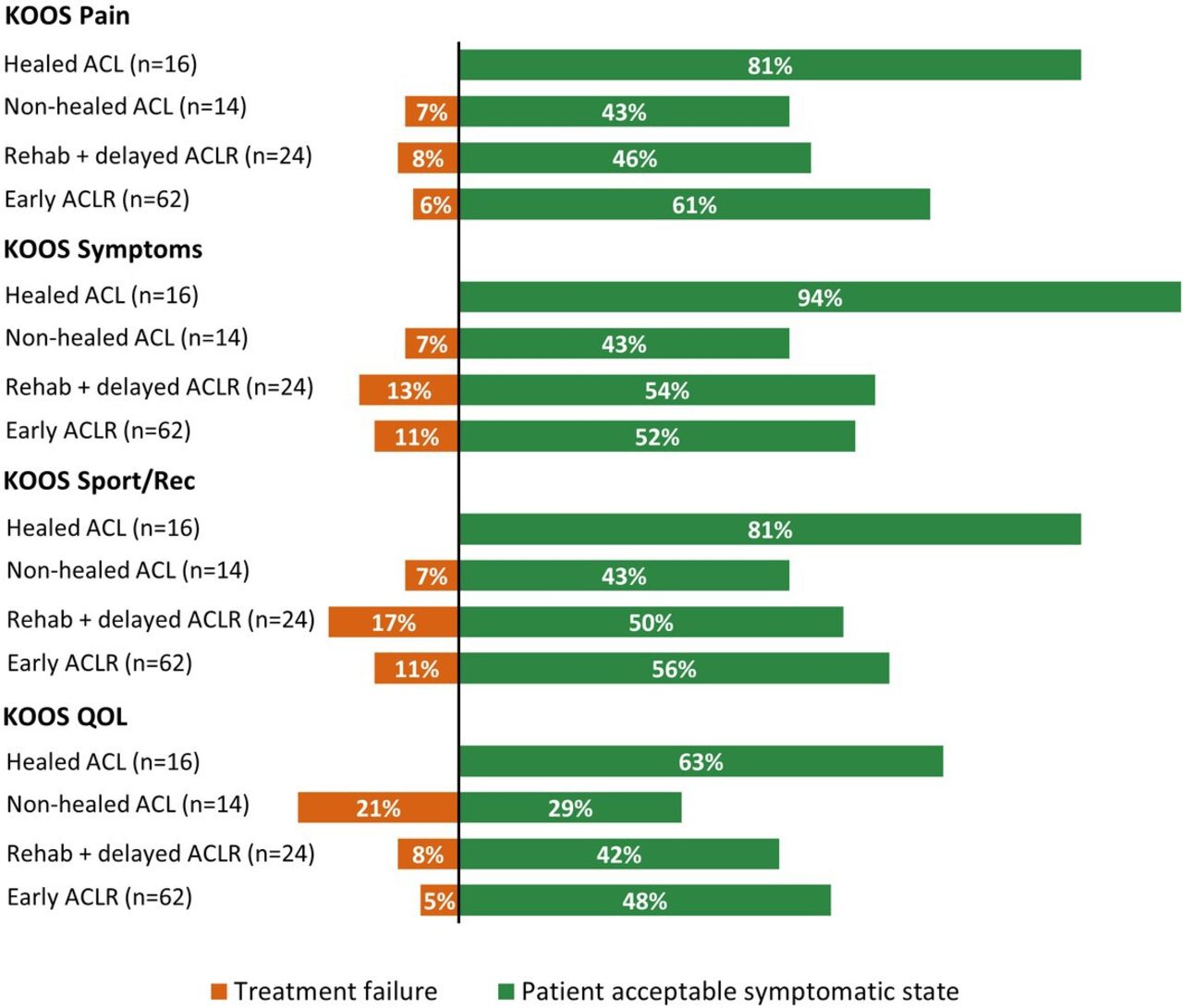
At 2-year follow-up, participants with evidence of ACL healing on MRI generally reported higher (‘better’) KOOS scores compared with the other groups (mean differences ranged from 10 to 22, table 3). At 5-year follow-up, KOOS scores were more similar to other groups (mean differences ranged from 1 to 16) (table 3). The trajectories of KOOS subscale scores over time, stratified by 2-year healing status and treatment group, are presented in figure 2. The proportion of participants with evidence of ACL healing meeting the PASS threshold within a given KOOS subscale at 2-year follow-up ranged from 63% (n=10) to 94% (n=15), and no individuals met the criteria for treatment failure (figure 3). In the other groups, 29%–61% of individuals met the PASS criteria within a KOOS subscale, and 5%–21% met the criteria for treatment failure (figure 3).

Mean KOOS subscale scores classified by treatment group and ACL healing status at 2 years. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; KOOS, Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life.
{kind=link}
{kind=link}
{kind=link}
The percentage of participants meeting criteria for patient acceptable symptom state and treatment failure for each KOOS subscale at 2-year follow-up. Percentages do not add up to 100%, the missing percentage is explained by participants who scored above the criteria for treatment failure and below the criteria for patient acceptable symptomatic state for a given KOOS subscale. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; KOOS, Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life.
2-year and 5-year outcomes stratified by ACL healing status as visualised on MRI and ACL management strategy
TAS scores were similar between groups at 2-year and 5-year follow-up (table 3). Fewer people in the healed and non-healed groups had ‘normal or nearly normal’ passive knee laxity at 2 and 5 years, compared with participants who had undergone ACLR (table 3). The proportion of participants with tibiofemoral and patellofemoral radiographic osteoarthritis in each group is reported in table 3.
Aim 3: the relationship between healing status, KOOS-Sport/Rec and KOOS-QOL scores
Mixed linear regression models are presented in online supplemental appendix 4 (crude models) and table 4 (adjusted models). Adjusted models suggest best outcomes in the healed group for both KOOS subscales at 2 years (table 4). The healed group reported better KOOS-QOL scores at 5 years, compared with the non-healed group. At 5-year follow-up, the other 95% CIs exclude the possibility that non-healed, delayed ACLR or early ACLR groups had clinically relevant, better KOOS-Sport/Rec or KOOS-QOL scores, compared with the healed ACL group. However, the 95% CIs do not rule out clinically relevant differences in favour of the healed ACL group (table 4).
Supplemental material
Adjusted mean differences in KOOS-Sport/Rec and KOOS-QOL between participants with evidence of ACL healing on MRI and the other three groups, per follow-up time
Discussion
Evidence of spontaneous healing of a ruptured ACL on MRI was observed in approximately half of young adults managed with rehabilitation alone who did not cross over to delayed ACLR. People with evidence of ACL healing reported better KOOS-Sport/Rec and KOOS-QOL scores at the 2-year follow-up, compared with the non-healed, delayed ACLR and early ACLR groups. At 5 years, there may be no meaningful difference in KOOS subscales between groups, although 95% CIs did not rule out that there may be clinically relevant differences in favour of the group with evidence of ACL healing on MRI. A high proportion (63–94%) of people with evidence of ACL healing on MRI reached the PASS threshold for each KOOS subscale, and no one reached the criteria for treatment failure.
ACL healing
The recommended treatment options for acute ACL injury do not consider the possibility for ACL healing.30 A key rationale for undergoing ACLR is that the ligament will not heal naturally, and management with rehabilitation alone likewise aims to provide (neuromuscular) stability to an ‘ACL-deficient’ knee joint. Our findings question the prevailing assumption that a ruptured ACL does not heal. We were unable to find prior studies reporting on ACL healing over multiple time points, including long-term follow-up. Aligning with our findings, a recent systematic review on spontaneous ACL healing in patients treated with different non-surgical approaches found restoration of continuity of the ACL on MRI in 31% of study participants, with MRIs assessed at 3–24 months postinjury.31
Some authors have suggested that proximal tears have a greater propensity for spontaneous healing, which could be explained by the difference in the vascularity of rupture locations.31 32 It is also possible that younger age, anterior fibre dislocation (ie, displacement of ACL fibres anterior to the tibial insertion leading potentially to impingement or extension deficit), remaining fibres in continuity not visualised on MRI and overlying synovial lining holding the ruptured ends in proximity33 may be associated with greater healing potential. The lack of a scaffold between the two ends of the injured ACL could be a key mechanism behind the failure to spontaneously heal. Murray and colleagues have shown that the use of a bridge enhanced ACL repair scaffolding may result in superior healing of the torn ACL, although the evidence is limited.34 Further research is needed to identify factors associated with ACL healing potential.
The relationship between ACL healing and patient outcomes
To gain new insight into the relationship between ACL healing on MRI and patient outcomes, we performed a number of exploratory analyses. Our findings suggest that participants with evidence of ACL healing on MRI had better 2-year outcomes (Sport/Rec and knee-related QOL) compared with people with a non-healed ACL or those who had early or delayed ACLR. Most participants (63%–94%) with evidence of ACL healing on MRI met the PASS criteria and none met the criteria for treatment failure at the 2-year follow-up. This was not the case for people without ACL healing or those who had undergone an early or delayed ACLR. Collectively, our findings support the hypothesis that people with spontaneous ACL healing on MRI experience favourable patient-reported outcomes.
Approximately 75% of participants with evidence of ACL healing on MRI at 2 years had normal passive knee laxity according to the pivot shift test, compared with 50% among people with no ACL healing and 90%–100% following early or delayed-ACLR. However, knee laxity assessed with the Lachman’s test found a lower proportion of participants with normal anteroposterior translation in the healed group. The evidence on ACL healing and knee laxity is mixed. For example, a small study of 31 patients with low activity levels managed with a knee brace found that 74% of patients had a clinically stable knee and MRI evidence of ACL healing at an average 16 months after injury.35 36 van Meer et al reported that 60% of 50 patients who received non-operative management for an ACL rupture showed some improvement in ACL fibre continuity on MRI at 2 years, while increased ACL fibre continuity was not associated with measures of knee laxity.37 The clinical relevance of assessing knee laxity is uncertain, considering that studies reporting more knee laxity in ACL-deficient patients found no differences in subjective knee instability, functional outcomes or physical activity levels between ACL-deficient and reconstructed groups.38 39
In our present study, all groups reported a mean TAS of 6 at 2 years and 5 at 5 years, which equates to participation in recreational sports. We note that a recent consensus statement recommended ACLR as the preferred treatment strategy for people wishing to return to competitive cutting/pivoting/jumping sports.40 This recommendation was made in the face of evidence showing that only 55% of people return to competitive sport after ACLR,14 as many as one in three young people who have an ACLR experience a second ACL injury,41 and that subsequent knee injury is most common in people who return to sport after ACLR.42
The low sample size of this study prevents us from drawing conclusions about any association between healing status and development of radiographic knee OA, even if the prevalence of radiographic OA in the healed group was low at 5 years.
Clinical implications
Of 13 participants with evidence of ACL healing on MRI at 1 year, only three underwent a delayed-ACLR before 5-year follow-up. Participants were not informed of their ACL healing status at any time point, so this should not have influenced their decision to have a delayed ACLR. Rather, we speculate that the better patient-reported outcomes among those with evidence of ACL healing influenced their decision not to have a delayed reconstruction, while conversely the worse outcomes for those without evidence of ACL healing influenced their decision in favour of surgical reconstruction. Since evidence of healing was apparent on MRI images as early as 3 months postinjury, further research should investigate whether the status of the ACL should inform treatment decisions following an initial period of rehabilitation. The possibility for the ACL to heal should feature in future discussions about ACL management options.
Future research directions
The lack of high-quality studies investigating ACL healing following ACL rupture is apparent. It is not known if a ruptured ACL with evidence of healing on MRI has comparable function to a non-injured ACL. Adequately powered longitudinal studies of non-surgically managed patients are needed to understand long-term outcomes, including rerupture rates, sports participation and performance, the prevalence of subsequent knee injury, surgery and osteoarthritis and the impact on long-term QOL. Interestingly, people in the healed ACL group underwent a mean 33 rehabilitation sessions, compared with 45, 76 and 63 sessions in the non-healed, delayed ACLR and early ACLR groups, respectively. Early ACLR is not cost-effective compared with rehabilitation and optional delayed ACLR for acute ACL rupture.43 Future research should investigate whether people with ACL healing on MRI have reduced healthcare costs and shorter work absenteeism, compared with people with a non-healed ACL and those undergoing early or delayed ACLR. Research is also needed to understand which patients’ characteristics (including acute MRI findings) predict subsequent ACL healing. Additionally, an ACLOAS grade 0–2 was considered to represent MRI evidence of ACL healing. This included ACLs with a thinned or elongated, but continuous appearance (grade 2). It is possible that participants with an ACL graded as ACLOAS grade 0 or grade 0–1 experienced better patient-reported outcomes and function than those with an ACLOAS grade 2. This would be a fruitful area for future research. Since different MRI classification criteria have been used,37 the implications of using different MRI criteria or more nuanced MRI features to classify ACL healing should be explored. Further research is needed to explore the potential for surgical and non-surgical strategies to facilitate healing of a ruptured ACL. The bridge-enhanced ACL repair may be an alternative to ACLR,44 and the impact of initial immobilisation in a brace followed by non-operative management with rehabilitation35 on the likelihood of ACL healing also requires further investigation.
Strengths and limitations
Strengths of this study include less potential for selection bias due to randomisation to early ACLR or rehabilitation plus optional delayed ACLR, and MRI data from a range of time points up to 5 years enabling a detailed exploration of ACL healing over time. A major limitation of this study is the small sample size after stratification based on treatment group and healing status. Because of this, we did not perform between-group statistical comparisons for most outcomes, and we took a cautious approach when interpreting the mixed linear regression models findings, focusing on all plausible values within the 95% CIs rather than the point estimates. It is possible that baseline injury-related variables (such as meniscal/chondral injury, ACL rupture location) could be related to ACL healing and patient-reported outcomes. However, research was lacking to inform which, if any, of these variables should be considered confounding factors. In the KANON trial, assessors were not blinded to treatment group allocation so the pivot-shift results may be biased. The KANON trial excluded professional athletes and individuals with low preinjury physical activity levels; therefore, our study findings are not generalisable to these subgroups.
Conclusion
In this group of young, non-professional sport participants, with an acute ACL rupture, approximately one in three patients who were randomised to optional delayed ACLR and every second patient managed with rehabilitation alone (who did not elect for delayed surgery) showed evidence of spontaneous healing of the ACL on MRI. Participants with evidence of ACL healing reported better sport/recreational function and knee-related QOL 2 years after injury, compared with the non-healed, delayed ACLR and early ACLR groups. These findings suggest that evidence of ACL healing may result in more favourable outcomes. The spontaneous healing potential of an acutely injured ACL is an important area of future research and should be discussed with patients when weighing up treatment options for ACL injury, acknowledging the evidence gaps in this area.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Lund University Ethics Committee (reference number LU-535). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RF and ME are joint senior authors.
Twitter @stephfilbay, @ewa_roos
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors All authors conceived and designed this analysis and participated in interpretation of findings. AT performed the statistical analysis. FWR analysed the MRI data. SRF drafted the first version of the manuscript. All authors contributed in revising the manuscript and gave their final approval of the submitted version. SF accepts full responsibility for the overall content and study conduct, AT is responsible for the statistical analysis.
Funding The KANON study received funding from the Swedish Research Council (RBF, LSL, EMR), Medical Faculty of Lund University (RBF, LSL, EMR), Region Skåne (LSL, RBF, EMR), Thelma Zoegas Fund (RBF), Stig & Ragna Gorthon Research Foundation (RBF), Swedish National Centre for Research in Sports (LSL, RBF), Crafoord Foundation (RBF), Tore Nilsson Research Fund (RBF) and Pfizer Global Research (LSL). SRF is funded by a National Health and Medical Research Council (NHMRC) Investigator Grant (number 1194428).
Competing interests EMR is deputy editor of Osteoarthritis and Cartilage, the developer of Knee injury and Osteoarthritis Outcome Score and co-founder of the Good Life with Osteoarthritis in Denmark (GLA:D) initiative to implement clinical guidelines in primary care; FWR is a shareholder of Boston Imaging Core Lab, and Consultant to Calibr and Grünenthal outside the submitted work.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.