Article Text

Statistics from Altmetric.com
Nearly one in five of the world’s population lives with a disability.1 While physical activity, including sports participation, is important for all, people with disabilities are at inherent risk for low engagement with a consequential increased risk for chronic disease related to a sedentary lifestyle. These include cardiometabolic disease and mental health conditions.2 Persons with a disability are 16%–62% less likely to meet physical activity guidelines.3
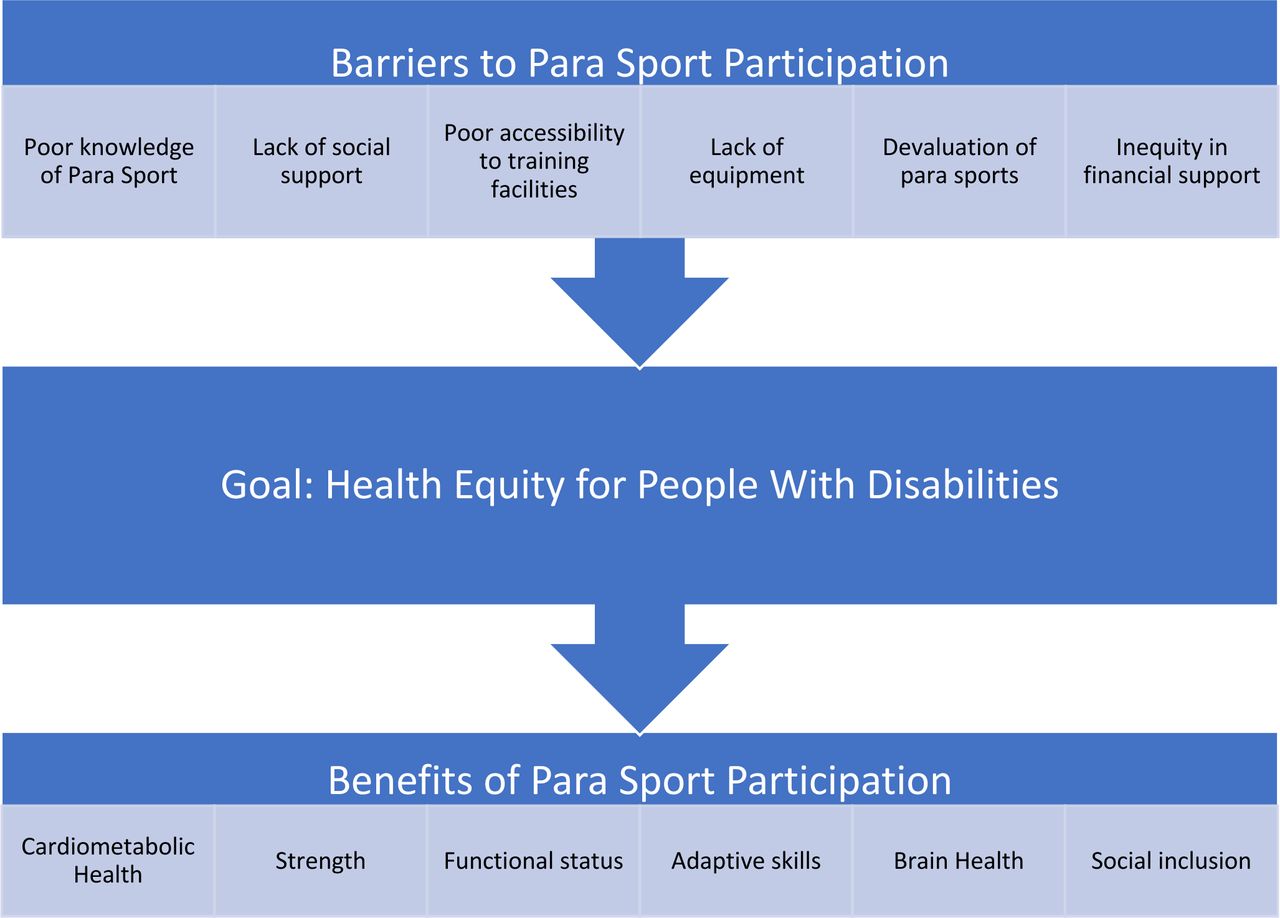
Barriers to sports participation include poor knowledge of para sport (eg, which sports are available, how to find opportunities or train), lack of social support, poor accessibility to training facilities, lack of equipment and the devaluation of para sport across society4 (figure 1). An additional concern is the inequity in financial support for para sport, especially in low-resourced environments. Even in high-income countries, para sport is often underfunded in comparison to elite sport for athletes with no disability, and data have shown that Paralympic athletes do not have the same opportunities as Olympic athletes.5 This inequity begins early in life given that children with a disability are often excluded from physical education sessions or marginalised within the school sports system.6 This editorial aims to promote health equity through para sport by highlighting such health disparities for the Sports and Exercise Medicine (SEM) community.

{kind=link}
Key summary points.
Health benefits of para sport
Physical activity and sports participation lead to several benefits in the general population, including improvements in physical and mental health, the development of social skills, and positively impacting health economics through disease prevention and treatment. Likewise, exercise and sports participation provide many health benefits to people with disabilities.
Cardiometabolic Health
Evidence supports that aerobic exercise improves waist circumference, insulin sensitivity and bladder function in persons with a spinal cord injury (SCI).3 7 Among stroke survivors, aerobic exercise reduces blood pressure and cholesterol concentrations.3 Studies specific to other para athlete groups have shown improvement in cardiovascular parameters such as peak oxygen uptake, cardiac output and respiratory function.8 However, a few studies have assessed the longitudinal effect of exercise on chronic disease prevention for individuals with a disability, and current exercise recommendations are based on those for the general population with the expectation that both populations will experience similar health benefits from physical activity and sports.
Strength
Data support that many para athletes participating in wheelchair sports have higher upper body strength values compared with both able-bodied and disabled non-athletes.9 In addition, strength training can reduce pain, optimise lean muscle mass and improve lipid profiles in persons with SCI.7 In individuals with cerebral palsy and Parkinson’s disease, strength training can improve muscular strength through both neurological and structural adaptations.3 10
Functional status and adaptive skills
Individuals with disabilities, such as limb deficiency, visual impairment and intellectual impairment, benefit greatly from both aerobic and anaerobic exercise as it has the potential to improve functional measures such as coordination, balance and mobility.3 8 In persons with an intellectual disability, sports participation allows the individual to learn and practise adaptive skills such as following routines and rules, personal care and communication.
Brain health and social inclusion
Participation in para sport also has positive effects on brain health and social inclusion, with evidence supporting a sense of increased confidence, independence, acceptance and quality of life. Sport can assist people to adapt to their disability.4 A study including elite para athletes showed that as many as 97% of athletes were employed5—a rate much higher than that in the general population of people with disabilities. Concerning brain health, physical activity may improve cognition and reduce the rates of depressive symptoms in individuals with neurological injuries such as stroke or multiple sclerosis.3
Taken together, the health benefits of para sport have the potential to improve all health-related domains (body function and structure, activity, participation, personal factors and environmental factors) as described by The International Classification of Functioning, Disability and Health. Despite these benefits, ongoing barriers for inclusion of all athletes in sport still lead to reduced rates of para sport participation. Given the global prevalence of disability, this should be considered a critical public health concern with significant social equity implication.
Solutions to promote health through para sport
Full health equity can only be achieved when individuals have the opportunity to attain their optimal health potential and are not held to a disadvantage based on predetermined circumstances such as a disability. It is critical that the SEM community works actively towards achieving health equity through physical activity and sports; such a mission is in line with the United Nations Sustainable Development Goal to ensure healthy lives and promote well-being for all, including people with disabilities. To achieve this, more opportunities for people with disabilities are needed within healthcare, the education sector and sports organisations. Some potential solutions to promote health through para sport include:
Prioritise research that focuses on athletes with disabilities, as studies on the health benefits of physical activity and sports participation in this population have been marginalised,3 with many of the existing exercise recommendations based on consensus rather than actual evidence.
Educate healthcare professionals, physical education teachers, sports administrators and coaches about para sport, including how to train individuals with a disability and the associated health benefits.
Inform policy-makers and advocates about the health benefits of para sport as well as ongoing barriers to participation that might be addressed through legislative solutions (eg, required inclusion of students with disabilities in school-based sports).
Ensure that para athletes have the same financial support as athletes with no disability, providing equitable opportunities to participate in both recreational and competitive sport.
Improving health equity for people with disabilities through physical activity and sport has the potential to enhance health among the 15% of people living with disabilities. This should be an urgent global health priority. The time to act is now!
This article is part of a series commissioned by the BJSM for the World Innovation Summit for Health (WISH) 2022. The BJSM peer reviewed, edited and made the decision to publish. The lead author(s) received a small honorarium for this work. The series, including open access fees and honoraria, is funded by WISH, which is an initiative of the Qatar Foundation.
Ethics statements
Patient consent for publication
Acknowledgments
This article is part of a series commissioned by the BJSM for the World Innovation Summit for Health (WISH) 2022. The BJSM peer reviewed, edited and made the decision to publish. The series, including open access fees, is funded by WISH, which is an initiative of the Qatar Foundation.
Footnotes
Twitter @KristinaFagher, @wderman, @CABlauwet
Correction notice This article has been corrected since it published Online First. The acknowledgements statement has been added.
Contributors CB contributed to the idea of the article. All authors then contributed with expertise and writing.
Funding KF has a post-doc position (D2021-0018) funded by the Swedish Research Council of Sports Sciences.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.