Article Text

Objective
To establish match injury rates and patterns in elite female rugby union players in England.
Method We conducted a six-season (2011/2012–2013/2014 and 2017/2018–2019/2020) prospective cohort study of time-loss match injuries in elite-level female players in the English Premiership competition. A 24-hour time-loss definition was used.
Results Five-hundred and thirty-four time-loss injuries were recorded during 13 680 hours of match exposure. Injury incidence was 39 injuries per 1000 hours (95% CIs 36 to 42) with a mean severity of 48 days (95% CIs 42 to 54) and median severity of 20 days (IQR: 7–57). Concussion was the most common specific injury diagnosis (five concussions per 1000 hours, 95% CIs 4 to 6). The tackle event was associated with the greatest burden of injury (615 days absence per 1000 hours 95% CIs 340 to 1112), with ‘being tackled’ specifically causing the most injuries (28% of all injuries) and concussions (22% of all concussions).
Conclusions This is the first multiple-season study of match injuries in elite women’s rugby union players. Match injury incidence was similar to that previously reported within international women’s rugby union. Injury prevention strategies centred on the tackle would focus on high-burden injuries, which are associated with substantial player time-loss and financial costs to teams as well as the high-priority area of concussions.
- Injuries
- Rugby
- Women in sport
- Epidemiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Despite women accounting for a quarter of the global playing population, there is relatively little evidence available regarding the risk of injury in women’s rugby union match play.
Most injury prevention strategies are based on research on the men’s game; however, injury patterns have been shown to differ between men and women in various other sports.
For more targeted injury prevention, multiteam, longitudinal epidemiological studies on female rugby union players are needed.
WHAT THIS STUDY ADDS
Match injury incidence was lower than is reported in the literature for elite men’s competitions; however, mean and median severity of injury were higher.
Concussion was the most common injury diagnosis, with the incidence increasing over the study period.
The tackle event was associated with the greatest burden of injury, with ‘being tackled’ specifically causing the most injuries and concussions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Provides medical teams with expected injury rates and severities for professional female rugby-related injuries, to inform return to play strategies within clubs.
Highlights the tackle as a priority area to focus injury prevention efforts.
Supports the ongoing efforts to enhance the recognition, management and prevention of concussion in women’s rugby.
Introduction
Rugby union is a full contact invasion team sport that is characterised by frequent bouts of high-intensity activities such as running and sprinting along with contact events such as tackling, scrummaging, rucking and mauling.1 These physical demands, and, in particular, the regular exposure to collisions and physical contact, mean that the inherent risk of injury in elite men’s rugby union is considered substantial.2
Rugby Union is played by over 2.7 million women worldwide accounting for a quarter of the global playing population, with women competing under the same rules as their male counterparts both at community and elite levels.3 Despite the increasing popularity of the women’s game,3 4 relatively little evidence is available regarding the incidence, risk factors or severity of injuries sustained by female players during match play. Moreover, in the studies published to date, the variability in the adopted methodologies, particularly with regards to the injury definition, limits the ability to generalise and make cross-study comparisons. A search of current women’s 15-a-side rugby literature yields only seven injury surveillance papers examining the incidence of injuries in women’s rugby, with injury incidence rates varying from as low as 3.6 to 37.5 injuries per 1000 player-hours.5–12 Furthermore, because these studies focus on either single teams or single seasons, it is difficult to generalise regarding less frequent injuries because the numbers are small, and it is not possible to follow trends in injury patterns.
In rugby union, most injury prevention strategies are based on research on the men’s game; however, patterns of injuries have been reported to differ between men and women in sports such as football,13 handball14 and basketball.15 In addition, considering that gendered factors (ie, social and cultural expectations of what women should be and do) present in the training, competition and treatment environments may influence injury risk factors and contribute to the different injury patterns observed;16 stronger longitudinal injury epidemiological studies in female rugby are required for more focused injury prevention. The aim of this longitudinal study was to describe the incidence, severity and burden of match injuries in elite adult women’s rugby union. Secondary aims were to describe injuries in different positional groupings (forwards and backs) and to describe the type and location of, and game event responsible for, injuries.
Methods
Procedures
In each season, all clubs participating in the English Women’s Premiership (top level of adult female rugby in England) were invited to take part the study. Complete data, included in this analysis, were provided by 5/8 clubs in 2011–2012, 7/8 clubs in 2012–2013, 7/8 clubs in 2013–2014 and 10/10 clubs in 2017/2018, 2018/2019 and 2019/2020.
Definitions and data collection
From 2011/2012 to 2013/2014, data were collected using a paper-based format and then entered into a database by one of the research team. Based on limited resources in women’s rugby, it was not possible to continue surveillance from 2014/2015 to 2016/2017, but when the top league of the women’s game in England was relaunched in the 2017/2018 season, injury data capture was mandated by the competition governing body. Injury data from 2017/2018 to 2019/2020 were captured using an online clinical electronic medical record keeping system, ‘Rugby Squad’ (The Sports Office, UK). All injury data (nature of injury, location of injury, specific Orchard code diagnosis, game event associated with injury and days missed due to the injury) were captured by the teams’ medical personal responsible for diagnosis and treating the injuries. The study adopted the definitions and methodologies described in the consensus statement for reporting rugby injuries.17 A time-loss injury was defined according to the consensus statement as any injury that results in a player being unable to take a full part in future rugby training or match play for more than 24 hours from midnight at the end of the day the injury was sustained.17 Injury severity was defined as the number of days lost from match play or training.17 Match exposure was calculated as the number of matches played multiplied by the number of exposed players (15) and the match exposure time (80 mins). Data capture was managed by two researchers at the host institution, who validated all reported match injuries against match report cards completed by match officials, match exposure against fixture lists and implemented a quality control process to check for inconsistencies and duplicates in the data.
Data analysis
Player characteristics were calculated as mean±SD. Injury data were presented as count, proportion and incidence, with injury incidence calculated as the count of injuries per 1000 player hours and 95% CIs using the Poisson distribution. Incidence was compared using incidence rate ratios (IRR) and p values, with Holm-Bonferroni adjustments applied to p values to offset the increased risk of a type 1 error when conducting multiple comparisons. Significance was set at p≤0.05. Trends in injury types were assessed by comparing the incidence (±95 CIs) to the combined seasons’ mean±2 SD. Mean severity was calculated as the total sum of days absent divided by the total count of injuries. Median severity was calculated as the midpoint of the range of injury severities within the data set with IQR. Injury burden was calculated as the product of mean severity and incidence (days absent per 1000 player-match hours) and 95% CIs. If the 95% CIs between comparisons did not overlap, it was deemed that the injury burden comparisons were significantly different. Significant differences in values for injury incidence for grouped playing position (comparing backs vs forwards) and between the individual seasons observed were calculated using two-tailed Z test for comparison of rates18; significance was accepted at the 5% level (equal variances assumed), Stata V.16.0 was used for all statistical analysis.19
Results
Injury incidence
The mean±SD age of backs involved in the study across the six seasons was 25±2 years and forwards 26±2 years. Significant differences were observed between forwards and backs for height (backs 155±9 cm vs forwards 168±10 cm p<0.001) and weight (backs 68±2 kg vs forwards 77±2 kg p<0.001). In total, 13 680 hours (forward 7296; backs 6384) of match play and 534 injuries (forwards 335; backs 199) were recorded. This equates to an overall injury incidence of 39 injuries per 1000 hours (95% CIs 36 to 42), with forwards having a significantly higher injury incidence (46 injuries per 1000 hours, 95% CIs 41 to 51) than backs (31 injuries per 1000 hours, 95% CIs 27 to 36, IRR: 1.5 (1.2 to 1.8) p=0.001). There were no significant differences in injury incidence between seasons (table 1).
Number (n), incidence (injuries per 1000 hours), mean severity (days absence), burden (mean days absence per 1000 hours) and median severity (days absence) of match injuries per season
Injury severity and burden
A total of 25 649 days were lost from training or match play as a result of the match injuries sustained during the study period. Mean injury severity across the study period was 48 days (95% CIs 42 to 54) (table 1), with a significantly lower mean severity of injury in the 2012/2013 season than the 2017/2018 and 2018/2019 seasons. The mean injury burden across the study period was 1819 days absence per 1000 hours (95% CIs 1329 to 2489), with no significant difference in injury burden observed between seasons (table 1). There was no significant difference in the mean severity, median severity and burden of injury between forwards and backs.
Nature of injury
Across the study period, muscle and tendon and joint (non-bone) and ligament injuries were the first and second most common injury types, with both injury types having a significantly higher incidence of injury than all other parent injury types (p<0.05) (table 2). Joint (non-bone) and ligament injuries had a significantly higher burden of injury than all other parent injury types (875 days absence per 1000 hours, 95% CIs 497 to 1541) (table 2).
Number (n), incidence (injuries per 1000 hours), mean severity (days absence), burden (mean days absence per 1000 hours) and median severity (days absence) of match injuries by injury type
Location of injury
Across the study period, there was a significantly higher incidence of lower limb injuries than any other body region (figure 1), with injuries to the knee being both the most common (5.2 injuries per 1000 hours, 95% CIs 4 to 7) and highest mean severity (102 days, 95% CIs 72 to 131) lower limb injuries.

Incidence (injuries per 1000 hours) of match injuries by grouped body region. Error bars represent 95% CIs.
Considering lower limb injuries, joint and ligament injuries to the knee (3.1 injuries per 1000 hours, 95% CIs 2 to 4) and ankle (3.5 injuries per 1000 hours, 95% CIs 3 to 5) were the most common (online supplemental file 1). Medial collateral (MCL) (1.1 injuries per 1000 hours, 95% CIs 1 to 2) and anterior cruciate ligament (ACL) (0.4 injuries per 1000 hours, 95% CIs 0.2 to 1.0) injuries accounted for the highest incidence of knee injuries and lateral ankle ligament injuries accounted for the highest incidence of ankle injuries (1.2 injuries per 1000 hours, 95% CI: 1 to 2).
Supplemental material
The head/face was the body location with the highest incidence of injury (7.3 injuries per 1000 hours, 95% CIs: 6 to 9). Of the head/face injuries, 69% were concussions, which equates to a concussion incidence of 5.0 concussions per 1000 hours (95% CIs 4 to 6). Concussions most commonly occurred to players being Tackled (22%), followed by players Tackling (17%). The incidence of concussion increased from 2011/2012 to 2018/2019; however, there was no significant difference between seasons (figure 2).

Incidence of concussion per season of the surveillance period. Mean±2 SD. Error bars represent 95% CIs.
Injury event
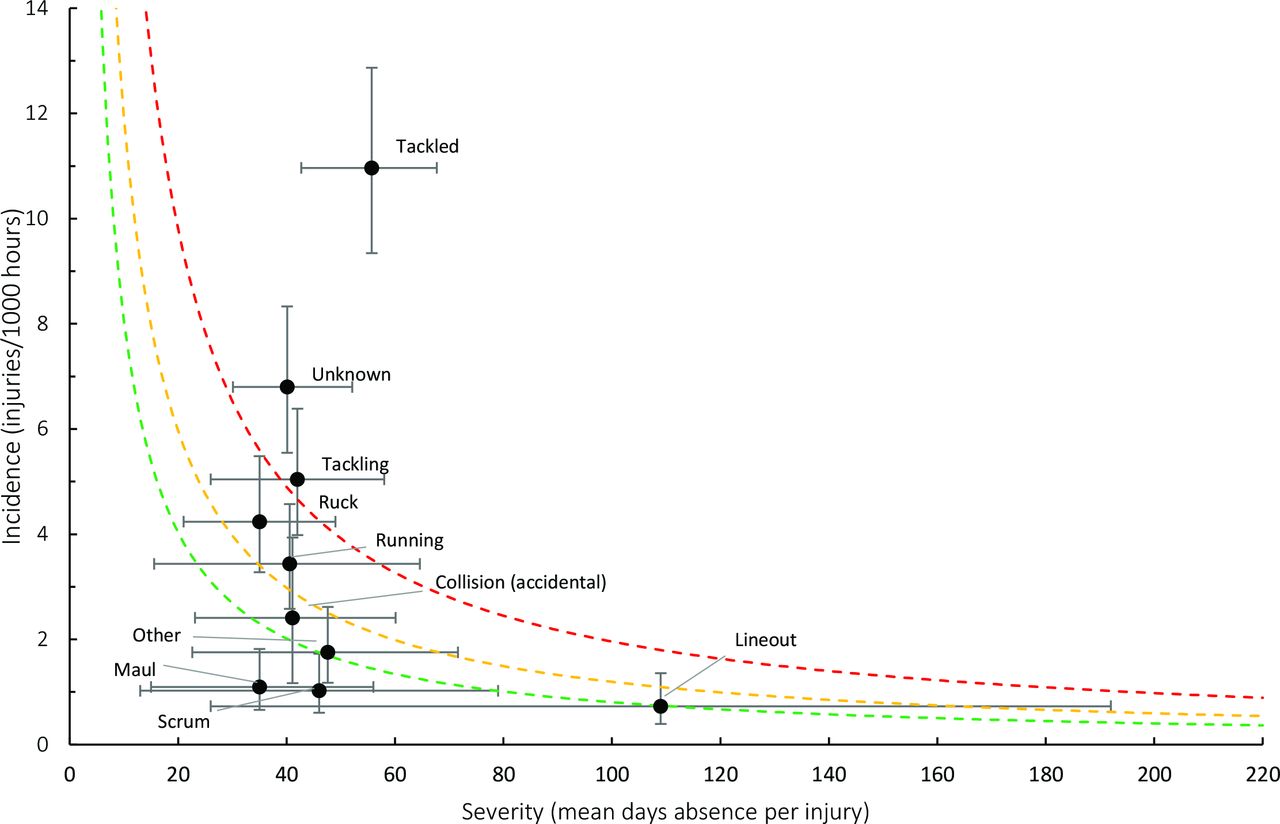
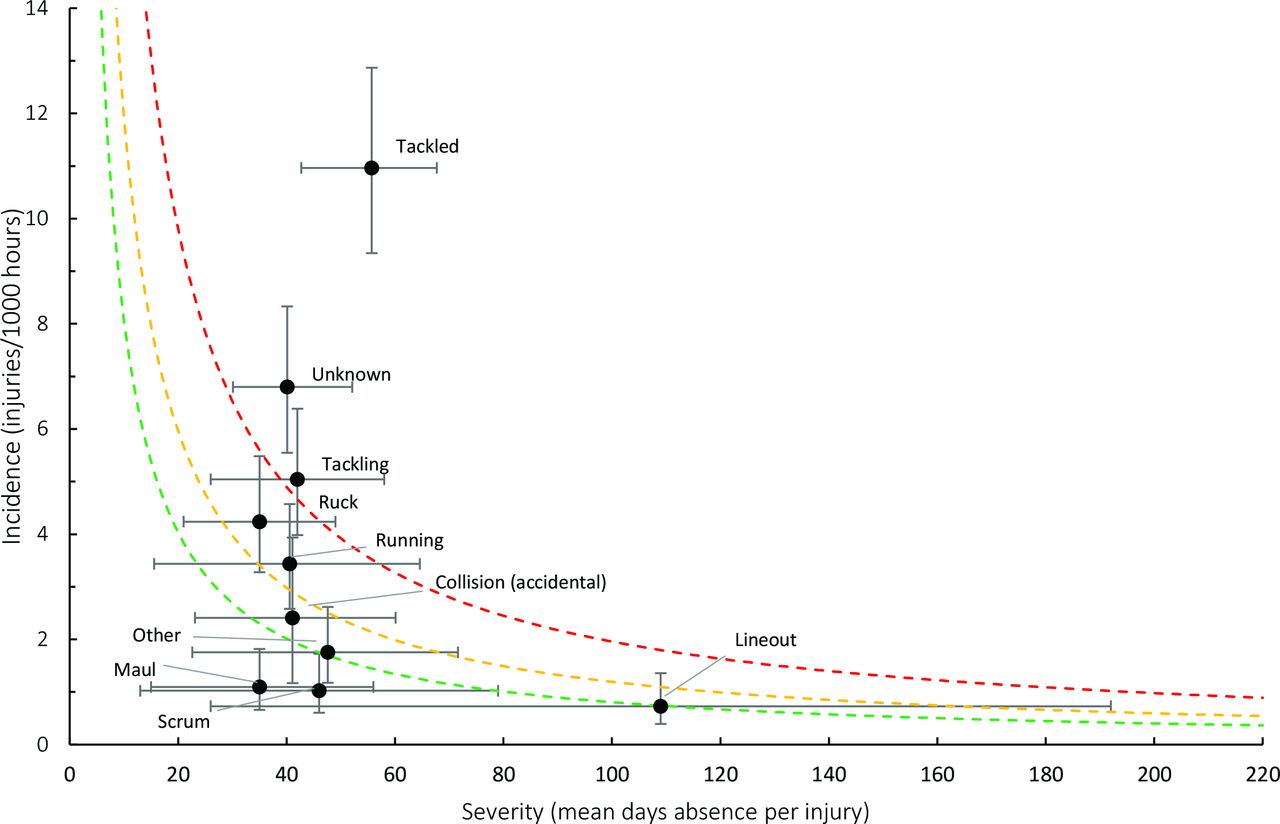
Injuries associated with the tackle accounted for 41% of all injuries, with the next most common injury activity being the ruck (11%). Of the tackle-related injuries, 68% were to the player being tackled (11.0 injuries per 1000 hours, 95% CIs 9 to 13) and 32% to the tackling player (5.0 injuries per 1000 hours, 95% CIs 4 to 6). The greatest burden of injury was to the player being tackled (615 days absence per 1000 hours, 95% CIs 340 to 1112) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Injury burden as a function of activity causing injury for the seasons 2011/12–2019/20. The y-axis represents incidence (number per 1000 hours) while the x-axis represents mean severity (days absence).21 Green line: values to the left and below represent the under the 25th burden percentile, these are low-risk injuries. Orange line: values to the left and below represent the under the 50th burden percentile, these are low-medium risk injuries. Red line: values to the left and below represent the under the 75th burden percentile, these are medium–high–risk injuries. Values to the right and above the red line are the most high-risk injuries.
Discussion
This is the first prospective longitudinal study of match injuries sustained by elite women’s rugby union players. The incidence of match injury was 39 injuries per 1000 hours (95% CIs 36 to 42) and mean severity was 48 days (95% CIs 42 to 54) absence per injury. Concussion was the most common specific injury diagnosis, with the incidence of concussion increasing over the surveillance period. The tackle event was associated with the greatest burden of injury, with ‘being tackled’ specifically causing the most injuries and concussions.
Incidence and severity
The incidence of match injuries was similar to the Women’s 2006 and 2010 World Cups (38 injuries per 1000 hours, 95% CIs 28 to 50 and 36 injuries per 1000 hours, 95% CIs 26 to 49, respectively)6 10 and in Irish amateur women’s rugby (36 injuries per 1000 hours).20 Given the limited amount of data available in elite women’s rugby, it is useful to make comparisons with men’s rugby, and the incidence of match injuries was lower than English elite men’s rugby (87 injuries per 1000 hours).21 The mean severity of injury (48 days, 95% CIs 42 to 54) was higher than reported in the English elite men’s competition (25 days, 95% CIs 22 to 28)21 and in a meta-analysis of elite men’s rugby (mean 26 days, 95% CIs 14 to 27).2 The median severity of 20 days was also higher than values reported in elite men’s rugby (range 5–12 days).21 22
One possible explanation for the lower injury incidence compared with the equivalent male playing population may be anatomic and physiological differences between sexes.23 24 It is also possible that female players may have lower levels of speed and power than male players, which may reduce the forces, and subsequent injury risk, encountered during a tackle event.23 25 Alternatively, although competing at the professional level, many of the women’s clubs operate most similarly to amateur men’s clubs, with medical staff typically only available during training and on match days.26 The relatively infrequent contact between medical staff and players may result in minor injuries being missed or undiagnosed and, thus, under-reporting of these minor injuries may, in part, contribute to the lower injury incidence observed. This relatively infrequent contact may also contribute to the higher injury severity observed as players have less access to treatment and rehabilitation.26 Players are also likely to have time constraints on rehabilitation activities as they balance these with normal day-to-day employment. In contrast, professional male players’ predominant employment is typically with their rugby club allowing them greater focus on rehabilitation, with increased contact with club medical staff. It is also worth mentioning that the gendered context of familial and domestic responsibilities, which are often greater for women than for men, and may create constraints on rehabilitation time.16
Lower limb injuries
Lower limb injuries are commonly reported in the literature on rugby injuries.2 The current study recorded a significantly higher incidence of lower limb injuries than any other body region, with injuries to the knee and ankle being the primary contributors to this. The knee was the most frequently injured lower limb location, with MCL injuries accounting for the greatest proportion (35%, n=15) of all knee injuries. This is perhaps unsurprising given that MCL injuries are frequently associated with cutting movements and direct valgus force to the lateral knee joint, which are both common events in rugby union.27 The incidence of ACL injuries observed in this study (0.4 per 1000 hours) is lower than those reported in Irish amateur Women’s rugby (0.8 per 1000 hours); however, the average severity of 288 days is within the range observed in professional men’s rugby.28 The short-term and medium-term outcomes for individuals following reconstructive ACL surgery or conservative management are mixed, with as many as 38% of both male and female athletes not returning to sport at their preinjury level 2–7 years postsurgery.29 The long-term health consequence of these injuries is also important, with as many as 87% of ACL injuries, resulting in post-traumatic osteoarthritis.30 ACL injuries may represent just a small proportion of the total number of injuries sustained, but from a player well-being and availability perspective, these are injuries for which effective injury prevention strategies are likely to offer a significant benefit.
Concussion
Concussion was the most common specific injury (ie, reflecting both location and type of injury) diagnosis across the study period, with an incidence of five concussions per 1000 hours (95% CIs 4 to 6), which is similar to Irish amateur women’s rugby (six concussions per 1000 hours, 95% CIs 5 to 7).20 The incidence of concussion increased over the study period, which reflects findings in other elite rugby settings21 31; however, it remained lower than the concussion incidence reported in elite men’s rugby in England (nine concussions per 1000 hours, 95% CIs 9 to 10).21 Female athletes have previously been reported to be more susceptible to sport-related concussions and experience worse outcomes when compared with male athletes,32 and so the context of evolving concussion identification over the study period may be important. It has been highlighted that structural and operational changes relating to the recognition of concussion implemented in the men’s game, such as in-game assessment of the head injury assessment protocol, real-time pitch-side video review for head injury events and the introduction of independent match day doctors, have contributed to the increase in reported concussion incidence.33 34 During the three-season data gap, protocols for improved postmatch identification of concussion were introduced in the elite women’s game in England, which may partly explain the increase in concussion incidence in the present study; however, the structural and operational changes described above for the men’s game were not introduced in the women’s game until after the period of this study. It will be interesting to see how this trend develops in future seasons as concussion recognition and management policies evolve in the women’s competition to be more reflective of those in the men’s competition.
While the incidence reported in this study was lower than in the equivalent men’s competition, the average severity of 39 days (95% CIs 28 to 50) is higher than the men’s reported 15 days (95% CIs 14 to 16).21 This is in line with evidence that female athletes experience worse outcomes,32 but data related to symptom profile and duration were not collected in this study, and days missed postconcussion provide only limited insight into the recovery of players. Nevertheless, female-specific head impact kinematics, physical and physiological characteristics and hormonal effects have been proposed as explanations for the prolonged concussion-related symptoms observed in women.32 35
The tackle
The tackle event, specifically being tackled, was associated with the greatest burden of injury, which is in accordance with the equivalent elite-level male competition.21 It is suggested that injury prevention strategies should target the areas of the game associated with the greatest injury burden as these incur substantial costs to teams both financially and due to time lost from participation.36 Studies conducted in elite male rugby have found poor contact technique to be a risk factor for injury, with more proficient tackling and ball-carrying technique found to reduce the risk of injury in the tackle event.37–39 Given that women’s rugby is less established than the men’s game, it is possible that tackle technique is less developed in some players due to their level of experience. Research has found that female rugby players experienced more injuries caused by whiplash mechanisms of contact with the ground during the tackle than their male counterparts.40 The findings in our study, which show that all injuries, including concussions, are most frequently caused by ‘being tackled’, provides support for additional research into the postulated whiplash processes from both a concussion and general injury prevention standpoint. While female-specific rugby research continues to develop, it is recommended that injury prevention strategies should incorporate skills training aimed at developing and improving tackle technique.41 42
In 2014, a global law change was introduced to the scrum engagement process, which requires the props to bind with the opposition before the players engage in an effort to reduce the forces on impact.43 The introduction of this law change occurred during the three-season gap in data collection of this study meaning that the first three seasons of data collection were under different scrum laws to the latter three seasons commencing in 2017/2018. Despite the change in scrum laws, no significant changes in injury rates in the scrum were observed. The 2017/2018 season also saw the women’s competition operating as a more professional league, having a clear set of competition minimum standards that include reference to governance and finance, player eligibility, registration requirements and player welfare, including minimum requirements for medical cover at matches and training.44 Although the league is classified as more professional for the 2017–2020 period than the 2011–2014, it would still be classified as semiprofessional in comparison to the professional male league. The increased professionalism of the competition has not resulted in any significant changes in overall injury rates.
Limitations
Although this manuscript aims to describe match injuries in the elite female rugby population, the authors acknowledge that training exposure and training injuries, which have not been addressed in this manuscript, will have had an impact on players and the match injury data presented. We acknowledge that changing from a paper-based to a web-based platform for data collection and transitioning from a three-digit Orchard code (OSICS-8) to a four-digit code (OSICS-10) may have had an effect on data recording. Consistency between seasons was supported by aligning with the consensus statement for injury surveillance in rugby union throughout the surveillance period.17
Conclusion
This is the first multiple-season study of match injuries in elite women’s rugby union players. The incidence of injury was similar to those previously reported for women’s international match play; however, lower than the elite men’s competition. Both the mean and median severity of injury were higher than those reported in elite men’s rugby. Concussion was the most common injury diagnosis, with the incidence of concussion increasing over the study period. The tackle event was associated with the greatest burden of injury, with ‘being tackled’ specifically causing the most injuries and concussions. Injury prevention strategies centred on the tackle would focus on high-burden injuries, which are associated with substantial financial and time-loss costs to teams as well as the high-priority area of concussions.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the University of Bath’s Research Ethics Approval Committee for Health. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to acknowledge the contribution made by the medical and conditioning staff and players.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @starling_linds, @drsimonkemp, @drkeithstokes
Contributors LTS and NG contributed equally as the primary authors of the manuscript and all other authors were involved in initial conception of the paper, interpretation of findings and provided significant feedback in refining the final manuscript. KS takes overall responsibility for the manuscript as guarantor.
Funding Funding for this study was provided by the Rugby Football Union through support of NG’s PhD and to support data collection in more recent years.
Competing interests SK and KS are employed by the Rugby Football Union.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.