Article Text

Statistics from Altmetric.com
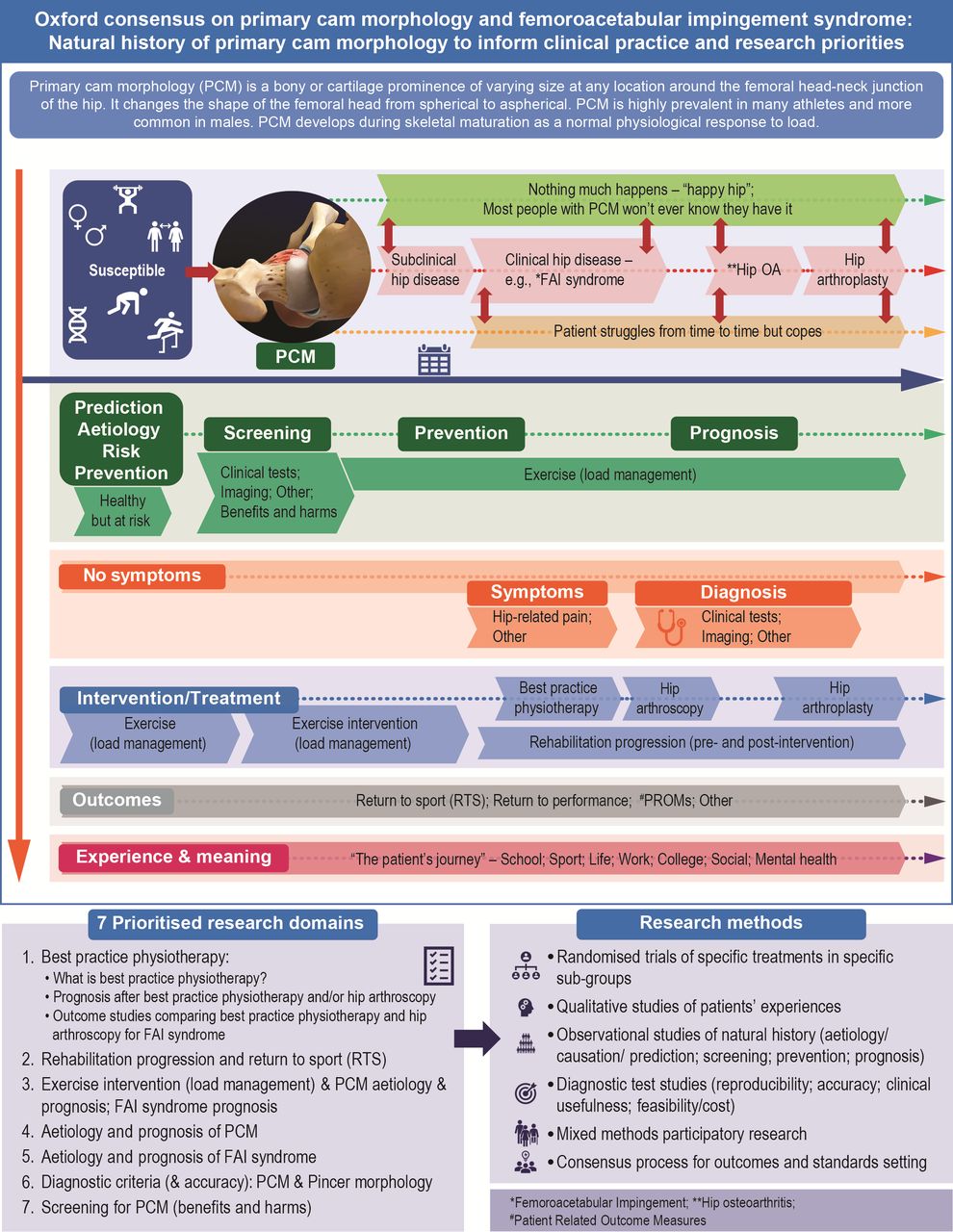
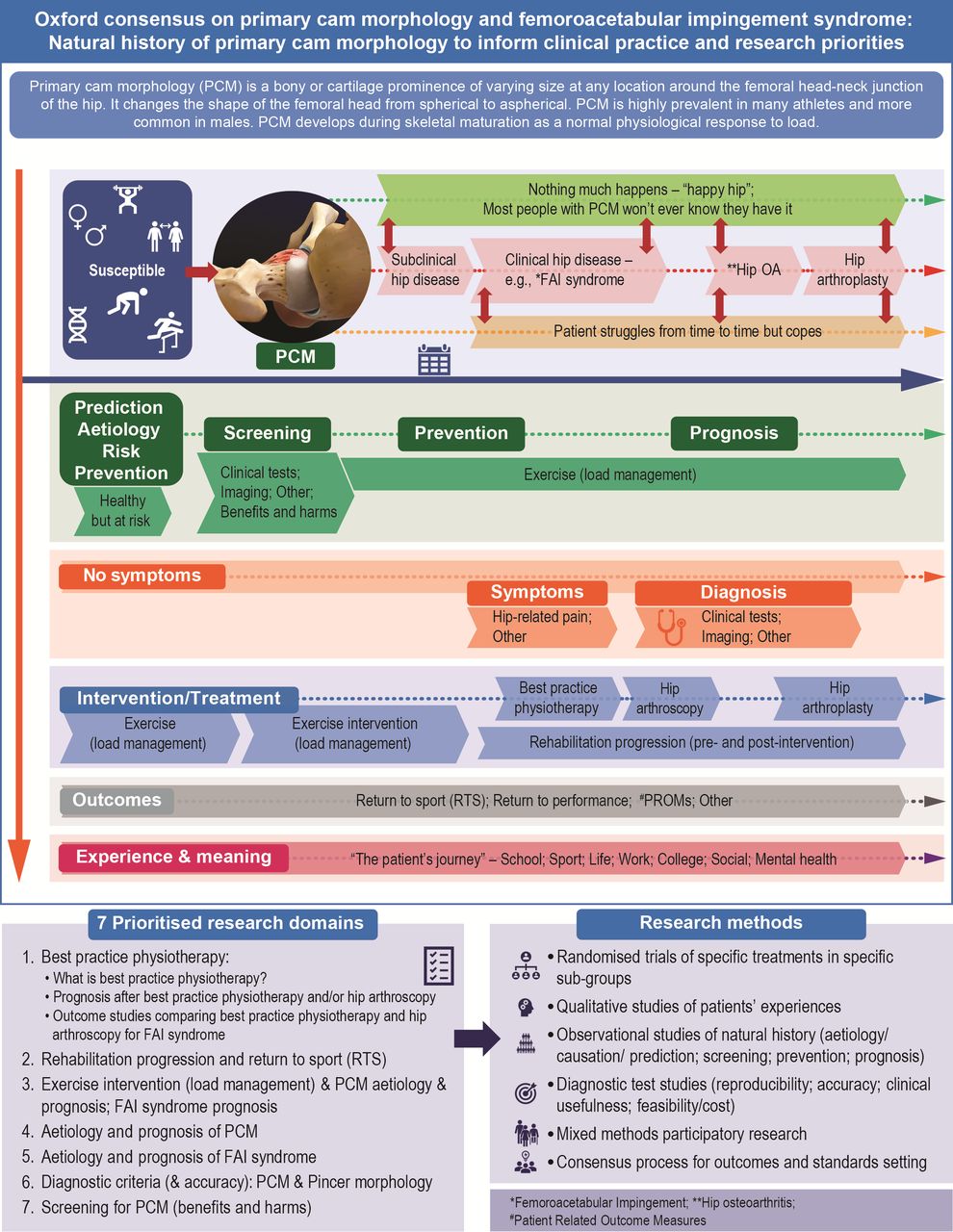
This infographic illustrates the natural history of primary cam morphology (PCM) to inform the Oxford Consensus Study’s seven prioritised research domains on conditions affecting the young person’s hip.1 2 We share 16 key messages for athletes, patients, clinicians and researchers:
Among other possible risk factors (including genetics), playing a high-load sport like football (soccer) or ice hockey while growing (during adolescence) is the key risk factor for developing PCM.3 4
Many young athletes have asymptomatic PCM. However, at present, no one knows how many; clinicians and researchers have ‘measured’ PCM in different ways (often using alpha angles on imaging).5
PCM seems more common in males. Research on PCM in females is sparse; no studies have yet investigated how PCM develops in female athletes.5
Clinicians and researchers cannot predict who will develop PCM. Therefore, coaches cannot, with confidence, manipulate training to reduce a young athlete’s risk of developing PCM.
Most athletes who have PCM thrive; they compete with ‘happy hips’ and never develop symptoms.
Some athletes with PCM develop symptoms like hip-related pain. This is called ‘femoroacetabular impingement (FAI) syndrome.’6 A few athletes with FAI syndrome might develop hip osteoarthritis (OA) in the future.7
Clinicians and researchers cannot yet predict the ‘at risk’ athletes with PCM who might develop hip disease such as FAI syndrome or hip OA. However, size matters; large alpha angles are associated with a greater risk of developing hip OA.8
The word ‘syndrome’ has a negative connotation to many patients. Most athletes with FAI syndrome do well when treated with a combination of education and progressive exercise rehabilitation.
Clinicians, researchers and patient partners should prioritise research to determine what ‘best practice physiotherapy’ is by comparing different treatment options.9
Other clinicians besides physiotherapists can lead exercise rehabilitation. When referring to non-surgical treatment for hip-related pain, the term ‘clinician-led progressive exercise rehabilitation’ is better than ‘physiotherapy’.9
Some patients with FAI syndrome might need surgery—it is a small proportion but clinicians and researchers cannot yet predict who.
Surgery can be hip arthroscopy to remove the bony prominence and/or repair damaged tissue like the hip’s cartilage. On occasion older athletes with advanced hip OA might need their hips replaced (hip arthroplasty).
Return to sport (RTS) after treatment for hip-related pain is important, especially to career athletes. However, clinician-scientists cannot yet, with confidence, advise on the best time to RTS. Following hip surgery, some athletes return to compete at their previous sporting levels; others have compromised performance.
Should clinicians and/or researchers screen young athletes for PCM? Probably not, but we do not know for sure. Some asymptomatic athletes with PCM might benefit from early intervention like adapting training load or targeted muscle strength training.
In addition to the cost and possible X-ray exposure, screening can also cause psychological harm. This happens when athletes are labelled with, and might worry about, a ‘condition’ (PCM) that will never bother them.
Some athletes (and their parents) worry that knowledge about PCM might negatively influence coaching decisions and their sporting careers.
{kind=link}
Ethics statements
Patient consent for publication
Ethics approval
The University of Oxford’s Medical Sciences Interdivisional Research Ethics Committee (MS IDREC) provided ethics approval for the study - R73576/RE001. Participants gave informed consent to participate in the study before taking part.
Footnotes
Twitter @DrPaulDijkstra, @Seaniemc89, @clare_ardern, @JoanneLKemp, @AndreaBMosler, @blazey85, @TO_dpr, @azizfar, @aserner, @rwilly2003, @oke_jason, @KarimKhan_IMHA, @trishgreenhalgh
Correction notice This article has been corrected since it published Online First. The title has been updated.
Collaborators Young Athlete’s Hip Research (YAHiR) Collaborative: Rintje Agricola; Thor Einar Andersen; Olufemi Ayeni; Ian Beasley; Mario Bizzini; Marco Cardinale; Tafadzwa Chiokwindo; Richard de Villiers (deseased); Lars Engebretsen; Tom Entwisle; Emin Ergen; Scott Fernquest; Celeste Geertsema; Mo Gimpel; Fares Haddad; David Hanff; Joshua Heerey; Per HolmichFranco Milko Impellizzeri; Julie Sandell Jacobsen; Christa Janse van Rensburg; Ara Kassarjian; Vikas Khanduja; Stephanie Kliethermes; Cara Lewis; Travis Maak; Susan Mayes; Inger Mechlenburg; Nonhlanhla Mkumbuzi; Sofie Nelis; Antony Palmer; Theodora Papadopoulou; Marc Philippon; Lauren Pierpoint; Lindsey Plass; Noel Pollock; Michael Reiman; Nia Roberts; Nikki Rommers; Nisrine Sawaya; Toni-Jane Snoxell; Jomar Souza; Louise Strickland; Tina Taseska; Kristian Thorborg; Jane Thornton; Hans Tol; Larissa Trease; Pim van Klij; Pieter Volcke; Adam Weir; Fiona Wilson; Mara Yamauchi.
Contributors HPD proposed the idea of a Delphi consensus study on the topic, planned and coordinated the study as part of his DPhil Evidence-Based Health Care studies. TG, MC, JLO, KMK and SG-J supervise the lead author’s DPhil studies and provided oversight to the study with other members of the Delphi Study Steering Committee (SMA, CLA, JLK, ABM, AP, PB, AS). All steering committee members contributed to, revised and refined the list of Delphi statements. AP co-led the patient and public involvement group with HPD and, with DR and RWW, facilitated an authentic patient’s voice throughout. AF, with oversight by JLO, contributed to the statistical analysis of the study. Although EM and VM contributed to all stages of the Delphi study, their focus was the imaging and research priorities domains. CLA and KMK co-chaired with HPD the Interactive Group Process while ABM, AP, JLK, SG-J, DR, SMA, EM, PB, RWW, AS and MC acted as group leads for the 6 small multistakeholder groups. HPD wrote the first draft of the Infographic manuscript. HPD created the Infographic; IS applied his graphic design skills to inform the final version Infographic. All listed authors contributed to reviewing, editing and revising the Infographic manuscript, and have read and agreed to the submitted version of the Infographic manuscript. The Young Athlete’s Hip Research (YAHiR) Collaborative listed as 'collaborators' were all Delphi panel members and contributed to the online Interactive Group Process and the ENHR ranking exercise.
Funding The lead author received a Kellogg College, Oxford Research Support Grant to the value of £1000.
Competing interests SMA, PB, DR, AF, AS, EM, VM, RWW, IS, JLO, SG-J, MC and TG declare they have no competing interests.HPD is an associate editor for BJSM; CLA is Editor-in-Chief of Journal of Orthopaedic and Sports Physical Therapy (JOSPT); JLK is an editor of BJSM; ABM is a BJSM deputy editor; AP is an editor at BMJ; KMK was Editor-in-Chief of BJSM from 2008 to 2020 but holds no position with BJSM or BMJ Group at present (June 2022). Collaborator group: JT and NM are BJSM editors; KT and FW are BJSM deputy editors; LE is BJSM IPHP editor; JoT, CJvR, SK, and AW are BJSM associate editors.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The Oxford consensus steering committee (HPD, SMA, CLA, JLK, ABM, AP, PB, AS, JO, KMK, SGJ, MK, TG), 5 women and 8 men, were English-speaking (as a first- or second language) white academics (11 with PhDs); 4 were physicians, 6 allied healthcare practitioners, and 3 health researchers. AP represented the Young Athlete’s Hip Research (YAHiR) Collaborative’s Patient and Public Involvement Group. One resided in the Global South. Interpreting ‘diversity’ as more than representation of certain demographic groups, the steering committee ensured a diverse and informed Delphi panel, representing six multi-profession stakeholder groups, including previously minoritised groups relevant to this research field (eg, women, athletes, patients and the community, participants from the Global South). This study’s online Delphi method, with a specific focus on anonymity and access to adequate topic-specific resources, supported a more equitable and inclusive process. First, the study’s online Delphi method was more equitable (as opposed to an in-person meeting) as traditionally underrepresented groups had similar opportunities to participate—levelling the playing field (they didn’t need to travel and could share their opinion in a ‘safe space’). Second, the study’s online Delphi method was more inclusive (referring to a positive and supportive experience) as our efforts included online meetings to share and discuss study resources and topic-specific information, and giving patient and public involvement partners leading roles in all aspects of the study (including steering committee membership, active involvement in study design, leading roles in online discussions, and co-authorship of study reports, including peer reviewed papers). Finally, in addition to the steering committee members, the main authors included a biostatistician (AF), two radiologists (EMcN, VM), and two additional members of the YAHiR Collaborative’s Patient and Public Involvement Group (DR and RW). The 18 main authors include six women (including the senior author, TG).