Article Text

Abstract
Objective The placement of automated external defibrillators (AEDs) at collegiate sporting venues is a growing trend. The purpose of this study was to investigate the prevalence, location and past utilisation of AEDs at National Collegiate Athletic Association (NCAA) Division II and III universities.
Design Cross-sectional survey.
Setting NCAA Division II and III universities.
Participants Questionnaires were mailed to the head athletic trainer at NCAA Division II and III (N=711) colleges and universities in the fall of 2003. Findings were compared to previously published results at Division I institutions.
Main outcome measure Prevalence, location and past utilisation of AEDs.
Results Completed surveys were returned by 254 NCAA Division II and III institutions for a 35.7% response rate (254/711). 205 (81%) institutions had at least one AED in the university athletic setting, with a median of 2 AEDs per institution (range 1–9). Athletic training rooms (75%) were the most likely location to place an AED. Twelve cases of AED use for sudden cardiac arrest were reported with 67% (8/12) occurring in older non-students, 16% (2/12) in intercollegiate athletes and 16% (2/12) in students (non-intercollegiate athletes). The AED deployed a shock in eight cases. 8 of 12 (66%) victims were immediately resuscitated, but only 4 survived to hospital discharge (overall survival 33%). None of the intercollegiate athletes or students survived.
Conclusions Most NCAA Division II and III institutions that responded to the survey have implemented AEDs in their athletic programs, although they have a lower prevalence of AEDs than previously reported at Division I universities. Although no benefit was demonstrated in a small number of intercollegiate athletes, AEDs were successfully used in older individuals on campus with cardiac arrest.
Statistics from Altmetric.com
The presence of automated external defibrillators (AEDs) has grown significantly in the collegiate athletic setting since the late 1990s.1 2 The success of public access defibrillation programs combined with an increased awareness of sudden cardiac arrest (SCA) in the athletic population and the desire to prevent a catastrophic sudden cardiac death (SCD) has led to a greater emphasis on emergency preparedness and the prompt availability of AEDs.3
SCA is the leading cause of death in young athletes,4 but identification of athletes with underlying cardiovascular disease is difficult as many of these athletes are asymptomatic and do not have abnormal findings on a physical exam. Four of five athletes who suffer a SCD have no premonitory symptoms before their SCA.5 Thus, cardiac arrest is often the sentinel presentation of their cardiovascular disease, emphasising the need for appropriate emergency planning and secondary prevention of SCD.
In the treatment of SCA, prompt recognition of SCA combined with early cardiopulmonary resuscitation (CPR) and early defibrillation are critical. The time from cardiac arrest to defibrillation is the strongest determinate of survival, with survival rates declining approximately 7–10% with each minute defibrillation is delayed.6 A target goal of <3–5 min from the time of collapse to the first shock in response to a cardiac arrest has been recommended by the American Heart Association and an Inter-Association Task Force.3 7 Emergency preparedness for SCA requires a comprehensive and coordinated response plan, reviewed and practiced by targeted responders at least annually and has the potential to benefit student-athletes and other persons at athletic events such as spectators, coaches and other individuals on campus.3 8
The presence and utilisation of AEDs at National Collegiate Athletic Association (NCAA) Division I institutions has been previously reported.1 2 The purpose of this study was to investigate AED prevalence and past utilisation at NCAA Division II and III institutions.
Methods
Study design
The study was a retrospective survey with questionnaires mailed to the head athletic trainers at NCAA Division II and III (N=711) colleges and universities in the fall of 2003. The study design was similar to a previous study of NCAA Division I institutions completed by the authors2 and used a similar questionnaire with minor modifications to gather more specific information about each AED use. A single follow-up letter or email request was sent over a 2-month period if a response was not received within 4 weeks of the initial mailing. Head athletic trainers were surveyed as a likely individual to have knowledge of AEDs and past utilisation within the college athletic setting.
The outcome measures analysed included: (1) prevalence and location of AEDs at Division II and III universities, (2) past AED utilisation and (3) obstacles to implementing AEDs. AED prevalence and location were also compared to our findings at NCAA Division I universities.2
The institutional review board of the University of Pennsylvania approved the study.
Statistical analysis
Collected data were analysed by descriptive statistics using SPSS V.11.0 (SPSS, Chicago, Illinois, USA). Division II and III universities were subdivided based on their NCAA classification to measure and identify factors on university or athletic resources affecting AED usage. The immediate resuscitation rate and deployment of a shock were measured in the event of an SCA event and use of an AED. Demographic information was calculated based on the age range of the SCA victim and subsequently divided into groups based on their activity on campus: older non-student (such as spectators, coaches, officials or other attendees on campus), intercollegiate athlete or student non-intercollegiate athlete.
Results
Completed surveys were returned by 254 NCAA Division II and III institutions for a response rate of 35.7% (254/711); 96/254 (37.8%) of Division II institutions and 158/254 (62.2%) of Division III institutions returned surveys. The head athletic trainer completing the survey was employed at the school for an average of 8 years (range of 1–43). The cost of each AED ranged from US$0 (ie, donated) to US$5000 with an average cost of US$2270 per AED.
Location and prevalence
Two hundred and five (81%) institutions of 254 respondents had an at least one AED in the university athletic setting (74/96 (77%) of Division II institutions; 128/158 (81%) of Division III institutions), with a median of 2 AEDs per institution (range 1–9). Institutions had AEDs for an average of 3.18 years (range of 1–7 years; 1998–2004). Schools were more likely to acquire their AED in recent years, with the greatest number of schools (50) acquiring their AED in 2003. Athletic training rooms were the most likely location to store an AED, with 75.6% of schools having at least one AED (range 1–4) located in their athletic training room. Locations for AEDs on other parts of campus are described in table 1.
Location of AEDs at NCAA Division II and III institutions
AED use and outcomes
Twelve AED uses to treat SCA were reported by 12 institutions (4.7% of all respondents). The details and outcomes of these cases are summarised in table 2. Athletic trainers provided the AED used in 5 of 12 (42%) cases, and campus police responded with the AED in 4 of 12 (33%) cases. The setting of the SCA was primarily at a recreation/fitness facility (5) or an intercollegiate athletic practice or competition (3); two events also occurred on campus and one event occurred each at an intramural competition and a swimming facility.
Details and outcomes of SCA cases
Eleven of 12 cases involved a witnessed collapse. In 7 of 11 cases with a witnessed collapse, it was reported that the SCA victim did not have a pulse or spontaneous respirations for any amount of time after collapse. CPR was initiated before the application of the AED in 11/12 cases. The average time from collapse to initiation of CPR was 80 s (range ≤30 s to 3–4 min), with CPR initiated in <30 s in five of the cases. The average time from full cardiopulmonary arrest to application of the AED was 3.27 min (range <30 s to 10 min) in the 11 cases that reported this information.
The AED deployed a shock in 10 cases. Four SCA victims received multiple shocks; three cases reported two shocks and one case had four shocks (average=1.75 shocks per case).
The SCA victims included three spectators (25%), two intercollegiate athletes (16.6%), two student non-intercollegiate athletes (16.6%), two attendees on campus (16.6%), one retired faculty (8.3%), one campus staff member (8.3%) and one senior athlete (8.3%). The age range of SCA victims was 20–80 years of age (mean=50). Students or student-athletes represented 33% (4/12) of SCA cases, and older non-students represented 67% (8/12) of SCA cases.
Eight of 12 (66%) victims were immediately resuscitated with return of spontaneous circulation at the site of the SCA, but only four survived to hospital discharge (overall survival 33%). None of the four students (two intercollegiate athletes and two non-intercollegiate athletes) survived to hospital discharge. Of the older victims, four of eight (50%) survived to hospital discharge.
Arrival of an ambulance took between 2 and 20 min after initial activation of the emergency medical services (EMS) system (mean=7.9 min; 10 incidents reported). For the four cases of SCA that occurred during exercise, one occurred at rest after practice, two during moderate intensity exercise and one during heavy exercise. The cause, profile and outcome of SCA events are described in table 2.
Obstacles to implementing AEDs
Forty-six of 49 schools without AEDs provided information about their obstacles to acquiring and implementing AEDs. Eleven institutions responded that AEDs were purchased but not yet installed on campus, 22 were currently debating the need for AEDs, 7 had not addressed the need for AEDs and 6 addressed the issue and chose not to purchase AEDs. Twelve institutions stated that money and resources were the primary obstacle to implementing an AED, and one cited medical-legal concerns. Five respondents without AEDs wished they had an AED for a past situation when one was not available. These situations included one elderly fan collapsed during a match; one spectator died of a heart attack during a game; one fan had a heart attack and survived; one athlete suffered syncope and was later diagnosed with hypertrophic cardiomyopathy and one athlete suffered an arrhythmia during exercise.
Comparison to Division I
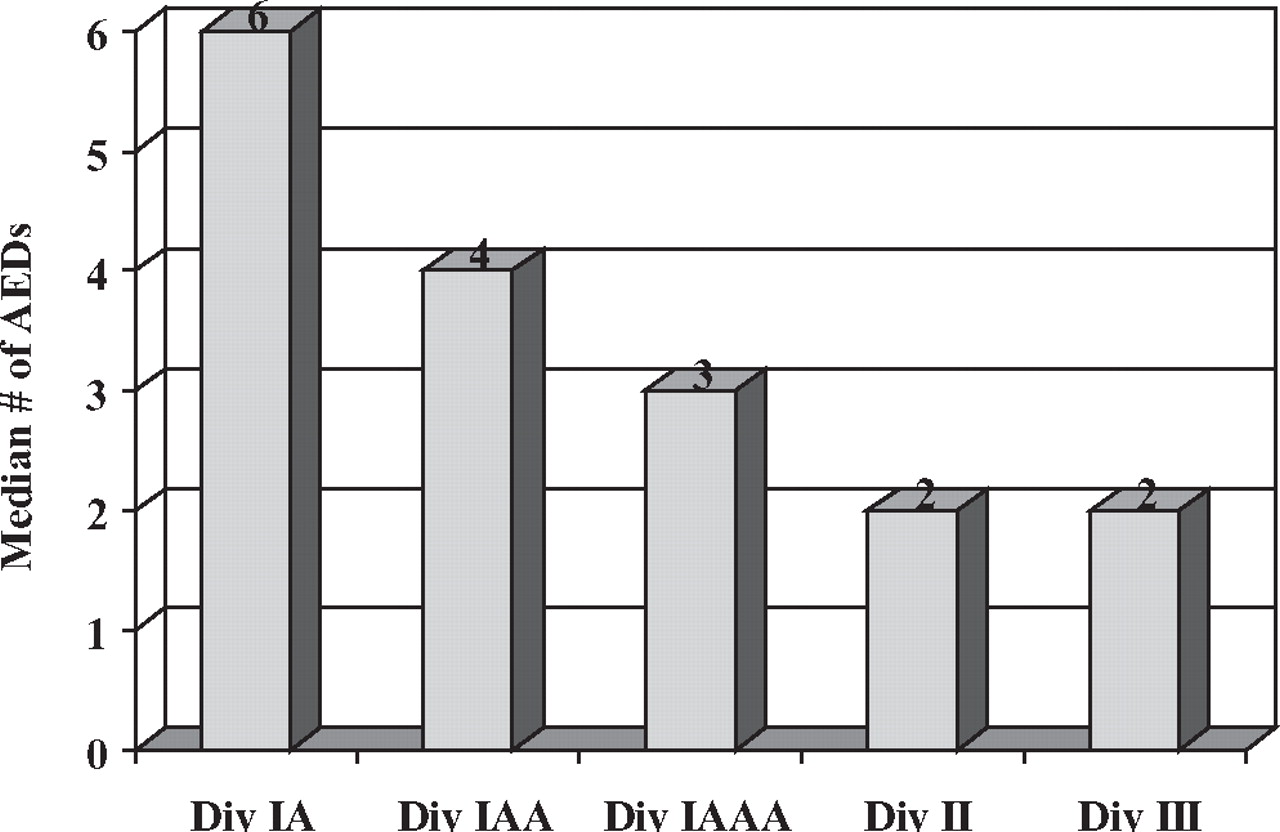
This study followed a similar survey by the authors on the prevalence, location and utilisation of AEDs at Division I athletic programs conducted in the same year (2003).2 Ninety per cent of Division I institutions had at least one AED at selected athletic venues, compared to 77% of Division II and 81% of Division III institutions (fig 1). Division I universities had twice the median number of AEDs per institution compared to Division II and III including when adjusted for the number of intercollegiate athletes (fig 2 and 3). The athletic training room was the most common location to place an AED in all Divisions.

Prevalence of automated external defibrillators at National Collegiate Athletic Association Division I, II and III institutions.
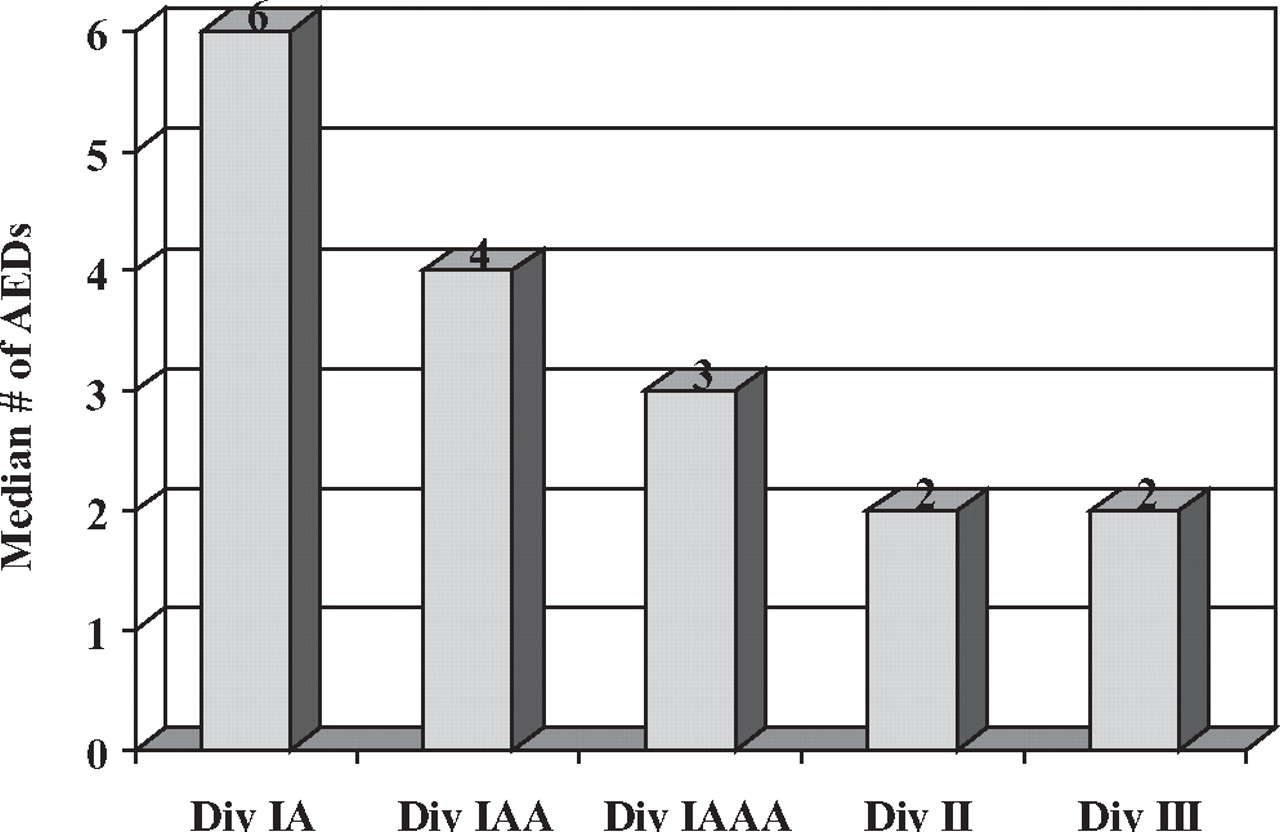
Median automated external defibrillators per institution.

{kind=link}
{kind=link}
{kind=link}
Automated external defibrillators per 100 student-athletes.
Discussion
The single greatest factor affecting survival after SCA is the time interval from arrest to defibrillation.9 Survival rates from out-of-hospital cardiac arrest using the traditional EMS system in the USA are <5%.10,–,12 The placement of AEDs in public locations where cardiac arrest commonly occurs, such as airports, casinos, shopping malls and other highly trafficked areas, has proven to be an effective strategy to improve survival from SCA.13,–,17 Jorgenson et al18 found the rate of AED use was 11.6% per year in public places such as malls, residential buildings and recreational facilities and that lay responders could successfully use AEDs in an emergency situation without harm or injury to patients, bystanders or the operators. Recent advances in technology have further simplified operation of an AED, improved effectiveness and accuracy and reduced cost.
Lay rescuer and public access defibrillation programs are designed to shorten the time interval from SCA to shock delivery. These programs train lay rescuers and first responders in CPR and AED use and place AEDs in high-risk public locations for SCA. Studies of rapid defibrillation using AEDs with non-traditional first responders and trained or untrained laypersons have demonstrated survival rates from 41% to 74% if bystander CPR is provided and defibrillation occurs within 3–5 min of collapse.2 14,–,17 19,–,23 Key elements to the success of these programs include training of motivated responders in CPR and AED use, a structured and practiced response and short response times.
In the collegiate athletic setting, AEDs provide a means of early defibrillation for young athletes and for other individuals on campus who may experience an unexpected cardiac arrest. At Division I universities, Drezner et al found that older non-students such as spectators, coaches and officials accounted for 77% of SCA cases at collegiate sporting venues and that treatment with an AED provided a survival benefit with a 54% overall immediate resuscitation rate.2 Coris et al also demonstrated that four of five AED uses on a Division I campus were used for treatment of SCA in spectators and athletic department staff rather than intercollegiate athletes, and the survival rate to hospital discharge was 61%.24
This is the first study to investigate AED utilisation at NCAA Division II and III athletic programs. This study was a retrospective survey and limited by a low response rate, the potential for recall bias and the potential under-reporting of SCA cases if unknown to the athletic trainers completing the questionnaire. The prevalence of AEDs found in this study also may have been influenced by responder bias, with those universities having AEDs being more likely to respond to the survey.
Similar to Division I,2 24 this study demonstrated a 50% survival rate for older non-students who suffer SCA at Division II and III institutions if treated promptly with an AED. AED use for SCA also was more likely in an older non-student than in a student or student-athlete. None of the four intercollegiate athletes or students with SCA survived. This finding is similar to initial reports of AED utilisation in the college athletic setting that did not identify a survival benefit in a small number of intercollegiate athletes with SCA.2 24 25 Drezner et al26 also reported a poor overall survival rate of only 11% for exercise-related SCA in the youth from 2000 to 2006 in the USA.26 The reasons for the lower survival rate in athletes is only speculative but could be due to delayed rescuer recognition of SCA or a higher prevalence of cardiomyopathy that may become more resistant to defibrillation.
More recently, preliminary findings from the National Registry for AED Use in Sports demonstrate improved survival for student-athletes with SCA in the high school athletic setting.27 Upon review of 1710 nationwide high schools with on-site AED programs, 36 (2%) schools reported a case of AED utilisation within a 1-year period from July 2006 to June 2007. Twenty-two of the cases were in older non-students and 14 cases were in high school student-athletes. The overall survival rate to hospital discharge was 64% for both student-athletes and older non-students with SCA.27 These findings strongly support the value of on-site AED programs for the treatment of SCA in young athletes.
A critical component to emergency planning for SCA in athletics is to individualise response plans to account for the geography of the area covered, location and distances between athletic venues, the likely first responders to an emergency and the number of AEDs available for distribution. Most Division II and III athletic programs responding to this study had only 1–2 AEDs. Placement of the AED in a central location accessible to many potential responders, such as the athletic training room, may provide the best strategy to achieve early defibrillation at multiple locations. In this study, the AED was brought to the scene of SCA by responding emergency personnel in 6 of 12 cases (campus police in four cases and emergency medical technicians or firefighters in two cases). Division II and III universities had a higher reliance on the EMS system to achieve early defibrillation than did Division I universities.2 This is probably related to the presence of more AEDs distributed at a wider number of athletic facilities in Division I programs, a finding that could reflect disparities in financial resources.
All potential first responders to SCA—coaches, administrators, athletic trainers and campus security personnel—must know the locations of an AED on campus. In this study, the most common setting for AED use was exercising at a recreational facility (5 of 12 cases). A communication system also needs to be developed to activate both the EMS system and the local response team so the AED can be brought to the site of SCA as quickly as possible. Integration of the AED program with the local EMS system also has been shown to increase survival from SCA.21 28
What is already known on this topic
▶ The placement of automated external defibrillators (AEDs) in public locations shortens the time to defibrillation in the treatment of sudden cardiac arrest and is an effective strategy to improve survival.
▶ In the collegiate athletic setting, AEDs provide a means of early defibrillation for student-athletes and for other individuals on campus who may experience an unexpected cardiac arrest.
What this study adds
▶ AED use for sudden cardiac arrest (SCA) at collegiate athletic venues is more likely in an older non-student than in a student or student-athlete.
▶ Prompt utilisation of an AED provides a high survival rate for older non-students who suffer SCA at National Collegiate Athletic Association Division II and III universities.
In conclusion, most NCAA Division II and III institutions that responded to this survey have implemented AEDs in their athletic programs, although they have a lower prevalence of AEDs than previously reported at Division I institutions. AED programs should be part of a comprehensive emergency plan for SCA that includes an effective communication system, training of potential first responders in CPR and AED use, acquisition of appropriate emergency equipment and routine practice and review of the response plan. Early defibrillation and decreasing response times are critical to improving survival rates for SCA in the athletic setting.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the University of Pennsylvania.
-
Provenance and peer review Not commissioned; externally peer reviewed.