Article Text

Abstract
Importance Patellofemoral pain (PFP) is both chronic and prevalent; it has complex aetiology and many conservative treatment options.
Objective Develop a comprehensive contemporary guide to conservative management of PFP outlining key considerations for clinicians to follow.
Design Mixed methods.
Methods We synthesised the findings from six high-quality systematic reviews to September 2013 with the opinions of 17 experts obtained via semistructured interviews. Experts had at least 5 years clinical experience with PFP as a specialist focus, were actively involved in PFP research and contributed to specialist international meetings. The interviews covered clinical reasoning, perception of current evidence and research priorities.
Results Multimodal intervention including exercise to strengthen the gluteal and quadriceps musculature, manual therapy and taping possessed the strongest evidence. Evidence also supports use of foot orthoses and acupuncture. Interview transcript analysis identified 23 themes and 58 subthemes. Four key over-arching principles to ensure effective management included—(1) PFP is a multifactorial condition requiring an individually tailored multimodal approach. (2) Immediate pain relief should be a priority to gain patient trust. (3) Patient empowerment by emphasising active over passive interventions is important. (4) Good patient education and activity modification is essential. Future research priorities include identifying risk factors, testing effective prevention, developing education strategies, evaluating the influence of psychosocial factors on treatment outcomes and how to address them, evaluating the efficacy of movement pattern retraining and improving clinicians’ assessment skills to facilitate optimal individual prescription.
Conclusions and relevance Effective management of PFP requires consideration of a number of proven conservative interventions. An individually tailored multimodal intervention programme including gluteal and quadriceps strengthening, patellar taping and an emphasis on education and activity modification should be prescribed for patients with PFP. We provide a ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’ outlining key considerations.
- Lowever extremity
- Knee
- Sports physiotherapy
Statistics from Altmetric.com
Patellofemoral pain (PFP) has a high prevalence in general practice,1 orthopaedic2 ,3 and sports settings. Pain is exacerbated by tasks which increase patellofemoral joint (PFJ) loading including running, squatting and stair negotiation, with occupational and physical capacity often reduced.4 The condition affects a wide range of ages, often beginning in early adolescence.5 Between 71 and 91% of individuals report chronic ongoing pain up to 20 years following initial diagnosis.6–8 PFP may also increase the risk of developing patellofemoral osteoarthritis.9
Numerous biomechanical factors have been linked to PFP and these are discussed in more detail elsewhere.10 ,11 As a result, various conservative interventions have been proposed and evaluated, including education, exercise, taping, braces, foot orthoses, soft tissue manipulation and acupuncture.12 Barton et al13 published a review of systematic reviews in 2008, which covered literature until 2007. Since 2007 a number of high-quality reviews covering conservative interventions for PFP provide greater guidance for research and clinical practice. Thus, an updated review and summary of findings from high-quality systematic reviews is warranted.
Despite high-quality systematic reviews being a source of concise and accurate information to guide evidence-based practice, limitations in relying solely on their findings must also be considered. First, published reviews often omit emerging knowledge and early research findings due to stringent inclusion and exclusion criteria. Second, such reviews often inadequately address how best to apply findings clinically thus compromising external validity. In a preliminary study exploring experienced clinicians’ clinical reasoning, a perceived lack of clinical applicability of research and systematic review findings was a primary barrier inhibiting evidence translation to patient management.14 This is particularly important for clinicians who are confronted with assessing and treating markedly heterogeneous patient presentations and groups. To achieve optimal results, the clinician must additionally consider their own clinical experience and, ideally, synthesised expert guidance alongside published evidence.15 Methods are needed to garner and copresent such evidence in order to optimise evidence translation.16
This study combines findings from high-quality systematic reviews (ie, level 1 evidence) with clinical reasoning from clinicians considered as international experts in the management of PFP, similar to previously published and described methods.17 Our aim is to optimise patient outcomes, and provide a basis for reflection on practice and high-quality education through the development of a comprehensive ‘Best Practice Guide to Conservative Management of Patellofemoral Pain.’
Methods
Review of systematic reviews
Inclusion and exclusion criteria
Reviews published in any language and using an unbiased, documented and reproducible search were considered. Inclusion criteria of reviews required participants to be described as having retropatellar, peripatellar or PFP; anterior knee pain; patellar or patellofemoral dysfunction; or chondromalacia patellae. Each review was required to focus on PFP and primarily evaluate non-pharmacological interventions. Non-English papers were translated to English prior to evaluation. Non-peer reviewed publications were excluded.
Search strategy
MEDLINE, EMBASE, CINAHL and Current Contents were searched in September 2013 for systematic reviews published since May 2007 as an update from Barton et al.13 Limits were applied to limit the search to reviews. The following key terms were combined; (patellofemoral or patella or chondromalacia) and (pain or dysfunction or syndrome). Mesh headings were not used to narrow or broaden the search. In addition to the initial electronic search, reference list screening and citation tracking in Google Scholar was completed for each included review.
Review process
Titles and abstracts found during the initial electronic search were uploaded into Endnote Web (Thomson Reuters), and duplicates removed. Titles and abstracts were then screened for inclusion by two independent reviewers (CB and ST). To resolve disagreement about exclusion, a third reviewer was available. Where necessary, the full text was retrieved.
Quality assessment
A quality assessment scale specifically designed for PFP reviews13 was applied to each included review. Items within the scale were developed based on more generalised tools including the Oxman checklist18 and texts addressing quality expectations from systematic reviews.19 ,20 The scale is scored out of 26, containing 13 items (2 points per item) covering reporting of search methods (item 1); comprehensiveness of search strategy (items 2–5); reporting of inclusion criteria (items 6–7); avoidance of selection bias (item 8); use of quality assessment (item 9); methods used to synthesise findings (items 10–11); and appropriateness of conclusions (items 12–13). Further details of scale development, validity and reliability can be found in Barton et al.13 A score of equal to or greater than 20 was considered as high quality.13 Findings from high-quality systematic reviews were summarised to provide the basis for level 1 conservative management evidence definition.
Semistructured interviews
Participants
Prospective interview participants were identified from a list of attendees to the 2009 and 2011 ‘international patellofemoral pain retreats’ in Baltimore, USA;21 and Ghent, Belgium,22 respectively. Suggestion of additional participants was also sought during each interview. Each participant was required to have had at least 5 years clinical experience with PFP as a specialist focus, be actively involved in PFP research and be contributing to specialist international meetings. It was felt that experts with a good blend of clinical experience and research knowledge would be able to provide the best information on the perceptions of current evidence (published and unpublished), and its external applicability for the management for PFP. Seventeen international experts from the UK (5), USA (4), Canada (1), Belgium (1) and Australia (6) were included. There were 12 physiotherapists, 3 athletic trainers and 2 physical therapists. Further details related to participant characteristics are outlined in online supplementary file 1. Ethical approval was granted by Queen Mary Ethics of Research Committee (QMERC). Each participant provided informed consent.
Interview process
One interviewer (ST) completed and recorded all interviews, which lasted between 30 and 120 min, and were transcribed for further analysis. To limit bias during questioning as a result of clinical experience and beliefs, the interviewer had sound medical knowledge but minimal clinical experience in the musculoskeletal field. To further reduce bias, a second non-clinical medical researcher assisted in the creation of the topic guide (see box 1) and conservative management summary (see online supplementary figure 1) used to stimulate discussion between the researcher and interviewer. Content of the conservative management summary was based on systematic review findings and findings from a preliminary study exploring clinical reasoning for PFP management.14 Specifically, the summary was created to outline potential interventions, without highlighting their associated evidence base, and thus avoiding biasing interview participants. The topic guide included questions about the participant's background, how to access evidence informing PFP management, their perception about the available evidence and its external applicability, how current evidence influences their clinical reasoning and their thoughts on the conservative management summary shown (see online supplementary figure 1). Typically 50% of the interview was on the last section.
Topic guide used to facilitate semistructured interviews
Background and History
▸ Tell me about your current occupation?
▸ How long have you been working clinically?
▸ What types of patients do you see (or used to see if no longer working clinically)?
▸ How many cases of PFP do you see (or used to see if no longer working clinically) per week?
▸ Please tell me about your level of experience in teaching and research.
Examine how the evidence is accessed
▸ How do you access the evidence?
▸ Are you currently involved in research for PFP?
Explore perceptions of the evidence
▸ What are your perceptions of the evidence for PFP?
▸ What gaps do you feel exist in the evidence?
▸ What should the priorities be for research in this field?
▸ What barriers exist for the translation of evidence into clinical practice?
▸ What facilitators exist for the translation of evidence into clinical practice?
Management of PFP
▸ What do you feel is important when treating a patient?
▸ Do you perform any treatments that are not evidence based?
▸ Could you tell me about your clinical reasoning for those treatments that are not evidence based (if yes to previous question)?
Reflections on clinical pathway and perception of evidence and clinical reasoning for each modality
▸ What are your initial thoughts on the clinical pathway?
▸ Could you tell me about your perceptions of the evidence for each of the treatment modalities?
▸ Could you tell me about gaps in the evidence for each of the treatment modalities?
▸ Could you tell me about your clinical reasoning for each of the treatment modalities?

{kind=link}
Clinical summary of treatment modality options for patellofemoral pain management.
Data analysis
Qualitative data was evaluated using a ‘framework’ approach23 by an experienced physiotherapist with previous experience in conducting interviews and evaluating data related to qualitative research (CB). First, each transcript was read to gain familiarity, and then a thematic framework was formed by mapping the ideas and opinions stated by the interviewees and combining these to generate themes and subthemes, subsequently tabulated with each interviewee being coded to enable anonymous quote attribution. Additional interviews were performed until data saturation, whereby no new themes were being identified. A second experienced physiotherapist in the team also read through each interview transcript to reinforce the analysis (SL). Finally, the analysis was repeated by another experienced clinical academic (DM) with extensive clinical and qualitative research experience, in order to ensure the accuracy and validity of interpretation.
Triangulation was by means of respondent validation and performed by presenting each interviewee with the final themes, subthemes and accompanying findings, with a request for free comment. Any new comment was added to the Framework analysis.
Synthesis of level 1 evidence with expert opinion
For the purpose of synthesising level 1 evidence (high-quality systematic review findings) with expert opinion, the findings were tabulated with level 1 evidence findings designated as either ‘Findings supporting the intervention’ and ‘Other findings related to the intervention’ in two separate columns. A third column contained qualitative themes and subthemes associated with the review findings. Qualitative findings which did not have supporting review evidence were tabulated separately. These tools were used to facilitate discussion of each conservative management option and principle, and the development of the ‘Best Practice Guide to Management of Patellofemoral Pain.’ Identified themes and subthemes not underpinned by level 1 evidence were synthesised into the discussion where appropriate, and italicised in the ‘Best Practice Guide to Management of Patellofemoral Pain’ while findings with level 1 evidence were written in normal text (see table 1).
Results
Summary of systematic reviews
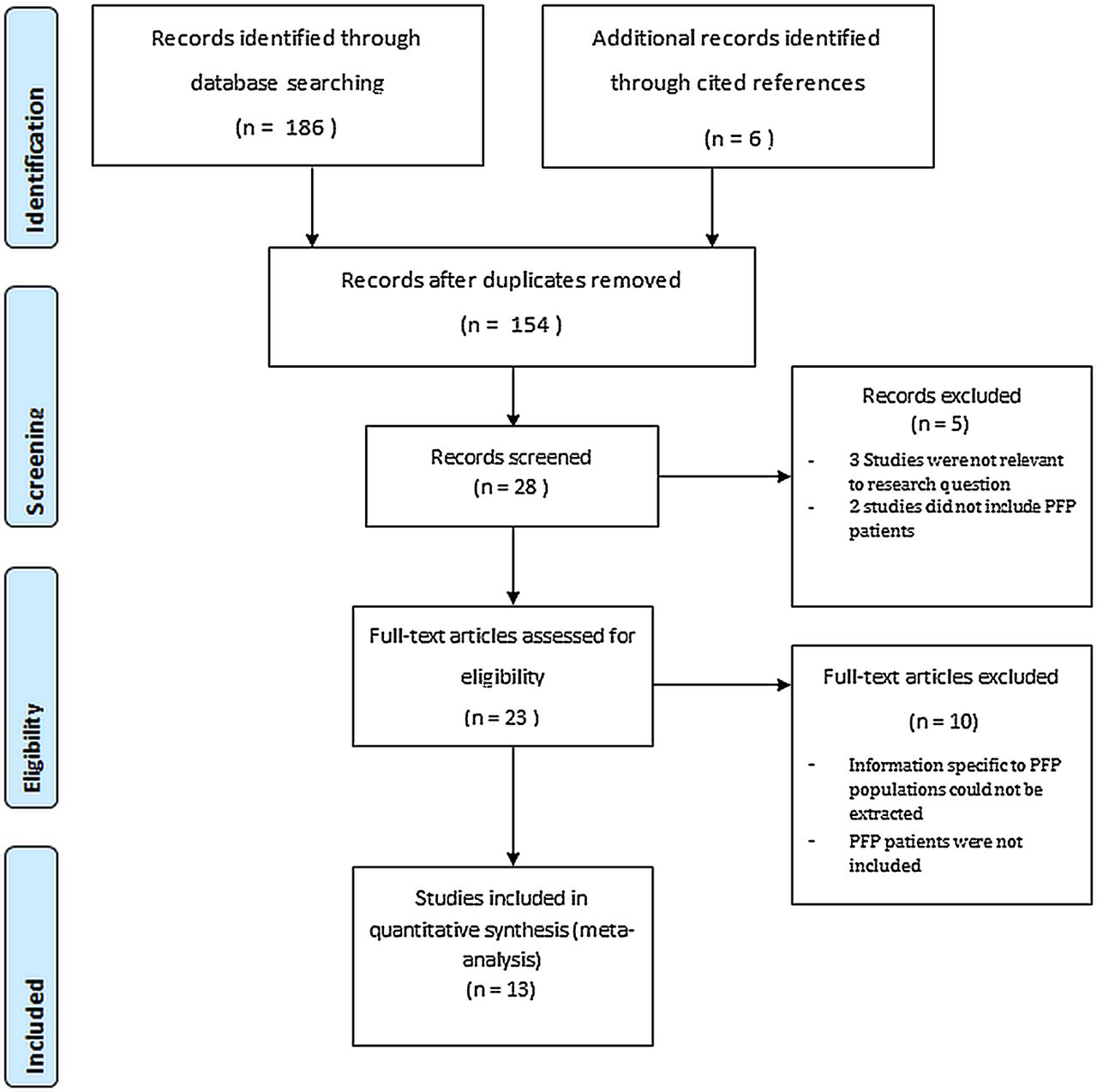
Figure 1 illustrates a flow chart of the search results. After the application of the inclusion and exclusion criterion, 13 contemporary reviews (ie, since 2007) were identified.24–36 Following quality assessment, six reviews30–35 were deemed high quality with scores ranging from 20 to 26 (see table 2). The average quality score was 16.3 (out of 26). Consistent limitations of lower quality reviews included absence of additional alternate searching, exclusion of non-English language studies, inadequate ranges of key words and an absence of two independent reviewers.
Quality assessment of included studies
Clinical reasoning qualitative data from international expert clinicians
Interview transcript analysis identified 7 sections with 23 themes and 58 subthemes. The seven sections were ‘Over-arching principles’ (see online supplementary file 2.1); ‘Exercise principles’ (see online supplementary file 2.2); ‘Exercise specifics’ (see online supplementary file 2.3); ‘Movement pattern and gait retraining’ (see online supplementary file 2.4); ‘Local interventions’ (see online supplementary file 2.5); ‘Acupuncture, dry needling and massage’ (see online supplementary file 2.6); and ‘Gaps in the evidence and future directions’ (see online supplementary file 2.7).
Synthesis of level 1 evidence with expert opinion
A summary of level 1 evidence (high-quality systematic review findings) and associated themes and subthemes from expert opinion is provided in table 3. Interventions covered in current high-quality systematic reviews include multimodal interventions, exercise, biofeedback, patellar taping, patellar bracing, foot orthoses and other adjunctive interventions including foot and ankle mobilisation, ultrasound and massage.
Summary of high-quality systematic review findings and associated expert opinion themes and subthemes
Identified themes and subthemes not also evaluated in included high-quality systematic reviews are summarised in table 4. These included a number of over-arching principles (see online supplementary file 2.1); exercise dose and principles to optimise outcomes (see online supplementary file 2.2); exercise to address the foot and ankle, core and lower limb flexibility (see online supplementary file 2.3); movement pattern and gait retraining (see online supplementary file 2.4); adjunctive interventions including foot and ankle mobilisation, ultrasound and massage (see online supplementary file 2.6); and gaps in the evidence and priorities for future research (see online supplementary file 2.7).
Themes and subthemes identified from interview transcripts unrelated to current level 1 evidence
The ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’
Multimodal interventions result in the strongest and most consistent evidence, particularly in the long term (1 year; see table 3).30 However, varying the multimodal programme components according to assessment findings for the individual patient emerged strongly from the interview data. Thus, treatment programmes should be individualised. A ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’ outlining key considerations for what may be included based on the synthesis of level 1 evidence with expert opinion can be found in table 1. The guide is divided into three sections including ‘Education,’ ‘Active Rehabilitation’ and ‘Passive Rehabilitation.’
Discussion
This mixed-methods study synthesises level 1 evidence from contemporary high-quality systematic reviews to guide management of PFP, formulation of clinical guidelines, reflection, educational initiatives and audit of treatment quality. Additionally, structured analysis of international experts’ reasoning was combined with the synthesised trial data to facilitate optimal evidence translation to clinical practice. The combination of methods yielded confirmation and illustration of findings, and important but under-researched topics that should facilitate clinical uptake as well as future innovation and evaluation. A comprehensive ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’ outlining key considerations for clinicians to follow is provided in table 1.
Multimodal interventions result in the strongest and most consistent evidence, particularly in the long term (1 year) (see 3.1 in table 3).30 Specifically, multimodal physiotherapy consisting of vasti and gluteal strengthening, stretching and PFJ mobilisation and taping has a moderate to large therapeutic effect in the short term (6–12 weeks), and small therapeutic effect in the long term (1 year).30 Framework analysis identified four key over-arching principles to ensure effective management, including—(1) PFP is a multifactorial condition requiring an individually tailored multimodal approach. (2) Immediate pain relief should be a priority to gain patient trust. (3) Patient empowerment by emphasising active over passive interventions is important. (4) Good patient education and activity modification is essential.
Active interventions
Exercise prescription principles
Compared to a control or placebo, current level 1 evidence indicates exercise prescription is clearly effective30 (see 3.2 in table 3), with both open (OKC) and closed kinetic chain (CKC) exercise providing large and clinically meaningful reductions in pain (see 3.1 in table 3 and supplementary file 2.2).37 However, it is unclear from high-quality systematic reviews whether OKC or CKC is more effective, or how important supervision is to ensuring successful outcomes.30 Findings from the qualitative component of this study provide greater guidance on these matters. Specifically, preference should be given to closed rather than open kinetic chain exercise in order to replicate function, although OKC exercise may be useful during early stage rehabilitation to strengthen specific musculature or target movements. Qualitative data suggested supervision be provided where possible to ensure correct technique and optimal movement patterns, particularly in the early stages. However, it must also be considered that high levels of supervision may not always be practical or financially viable, and as such, patients should be progressed to independence as soon as possible.
Exercise specifics
Quadriceps (particularly vastus medialis oblique—VMO) strengthening dominates current evidence-based exercise programmes (see 3.2 in table 3), and inclusion in rehabilitation was a strong feature of experts’ interviews (see 3.2–3.3 in table 3 and supplementary file 2.3). Despite evidence supporting a link between delayed activity of VMO and PFP,38 ,39 current level 1 evidence shows specific VMO electromyography (EMG) biofeedback may not improve rehabilitation outcomes (see 3.3 in table 3).30 Additionally, some experts highlighted the need to consider associated time and practical restraints of using EMG biofeedback in a clinical setting.
Passive interventions
Taping, bracing and orthoses
Level 1 evidence indicates medially directed patellar taping provides immediate pain reduction (see 3.4 in table 3),31 a feature that emerged strongly as desirable in early patient management to gain trust, facilitate active engagement and optimise outcomes (see table 4 and supplementary file 2.1). Inconsistent beliefs regarding the value of patellar taping in the longer term were consistent with varying conclusions drawn from high-quality systematic reviews evaluating taping in the longer term (see 3.4 in table 3). Specifically, one review35 reported no benefit, one review33 reported conflicting evidence and one review30 reported large positive effects for patellar taping outcomes. Important methodological considerations related to meta-analysis used in each review may explain these inconsistent conclusions.
Best Practice Guide to Conservative Management of Patellofemoral Pain
Callaghan and Selfe35 defined short term as 3 months or less, and chose to pool data from five studies with different time points (1 week to 3 months) and taping methods (ie, tailored and untailored), concluding patellar taping was not beneficial in the short term. In this instance it is possible that results from studies using untailored taping methods and longer term (eg, 3 months) follow-up may have washed out positive findings from studies evaluating tailored patellar taping and shorter, but clinically relevant, durations (eg, 1 week). Swart et al33 used a similar definition for short term (4–12 weeks), but chose not to pool data due to heterogeneity associated with time points and taping methods. Importantly, this led to a conclusion that findings were inconsistent. Finally, the review by Collins et al,12 separated time points so that 4 week and 12 week (ie, 3 month) data were considered separately, concluding large positive effects when taping is combined with exercise at 4 weeks. These contrasting findings highlight the need to consider the methods of meta-analysis and appropriateness of data pooling when interpreting results, and the need to evaluate the effect of varied taping methods (ie, tailored versus untailored) and time points in future research.
Level 1 evidence indicates patellar bracing, often designed to reduce lateral patellar tracking, is effective at providing immediate pain reduction (see 3.5 in table 3).31 This justifies experts recommendations for bracing in patients where taping is inappropriate, for example due to skin irritation. However, beyond the immediate term, the effectiveness of patellar bracing is reported to be inconsistent,33 possibly owing to the multifactorial nature of PFP and indicating the need for further research to identify those most likely to benefit.
Level 1 evidence indicates prefabricated foot orthoses do not improve outcomes at 12 or 52 weeks compared to placebo (flat inserts; see 3.6 in table 3).30 ,32 ,34 However, foot orthoses may improve outcomes over 6 weeks,32 ,34 although the clinical significance of reported pain reduction magnitude is debatable. Specifically, one review reported foot orthoses to yield a small positive effect on pain (SMD 0.59; 95% CI 0.15 to 1.04),30 while two others32 ,34 reported they do not provide greater pain reduction compared to placebo (flat inserts; see table 3, section 3.6). The discrepancy may be brought about by differences in CIs used when calculating standard mean differences, with the positive review30 using 95% CIs, and the other reviews32 ,34 using 99% CIs. Regardless, the lack of clinical meaningfulness of the pain reduction from foot orthoses prescription (MD 8.20 mm)32 ,34 pointed out by two of the reviews32 ,34 indicates foot orthoses as a stand-alone treatment are unlikely to constitute an adequate management plan. When used in conjunction with other interventions, there is conflicting evidence regarding the effects of combining foot orthoses with exercise compared to exercise alone in the short term (4–8 weeks),30 ,33 ,34 although this research must be treated cautiously as it is typically underpowered.30 ,34 Additionally, the addition of prefabricated foot orthoses to multimodal physiotherapy at 6, 12 or 52 weeks30 ,32 ,34 and the addition of foot orthoses to exercise at 52 weeks does not produce better outcomes.33
One important clinical consideration is that foot orthoses are not prescribed to all individuals presenting with PFP. Synthesis of expert clinical reasoning findings indicates that foot orthoses efficacy may be improved by targeting specific individuals based on measures of pronation. This belief is supported by case series studies which report that greater peak rear-foot eversion during walking40 and greater mid-foot mobility41 ,42 may be predictive of foot orthoses prescription success in individuals with PFP. Additionally, qualitative findings indicate that using the treatment direction test concept proposed by Vicenzino43 to identify those most likely to benefit may assist in more efficient tailoring of intervention in regard to foot orthoses prescription.
Adjunct interventions
Limited evidence from one systematic review30 indicates acupuncture may be effective in the management of PFP, but there are conflicting opinions among experts regarding its value in rehabilitation (see 3.7 in table 3 and supplementary file 2.6). Further research is needed in this area, particularly in individuals with PFP who possess muscle tightness, trigger points or more chronic pain. Limited evidence indicates ultrasound is not effective, with support from experts voicing that ultrasound should not be considered for individuals with PFP.
Expert opinion findings lacking supporting level 1 evidence
Overarching principles
Aiming for immediate pain relief was deemed important to gain patient trust and empower a patient to actively engage in treatment rather than rely on passive treatment of proven poor efficacy. Effective education including activity modification, managing patient expectations, and encouraging active management emerged clearly as the most important component of effective PFP management. However, patient education had no specific evaluation in level 1 research and is therefore a primary target for future research in order to develop and evaluate optimal educational resources. Additionally, qualitative evidence shows that clinicians need to be aware of, and address, potential psychosocial factors interacting with other aspects of patients’ presentation when managing PFP, again despite a lack of clear systematic review data.
Exercise prescription principles
Interviewed experts recommended the number of exercises prescribed be limited to approximately 3–4 in order to ensure compliance (see online supplementary file 2.2). Interestingly, this common recommendation is contrary to findings by a recent study investigating the dose–response effects of exercise for PFP.44 Specifically, high-dose rehabilitation involving seven exercises and taking approximately 60 min to complete was found to produce superior outcomes compared to low dose involving five exercises and taking approximately 20 min to complete.44 Establishing the optimal time needed per exercise session to enhance patient outcomes, while maintaining compliance should be a research priority. Other exercise principle recommendations included ensuring exercise specificity, avoiding irritability and encouraging frequent completion of exercises. Further research comparing different exercise approaches and principles is clearly needed in order to optimise outcomes for patients with PFP.
As previously stated the use of VMO EMG biofeedback is not supported by level 1 evidence30 and practicality in a clinical setting may be limited. However, the implementation of other more freely available biofeedback such as mirrors and video during exercise, to facilitate reversal of poor hip and knee mechanics was strongly advocated by experts and as such should be considered in clinical practice. Further research is needed to confirm its usefulness.
Exercise specifics
At the time of searching there was an absence of level 1 evidence (high-quality systematic reviews) to support the implementation of hip and gluteal exercises in PFP (table 3, section 3.2). However, there is growing evidence linking altered hip mechanics,45 ,46 and impaired gluteal strength and function to PFP.47 ,48 Interviewed experts also emphasised a perceived clinical efficacy for exercise prescription designed to reverse proximal movement and strength faults. Additionally, a number of studies have evaluated the efficacy of gluteal strengthening for PFP and reported favourable outcomes,49–51 although an updated systematic review to synthesise this research is needed. Regardless, current empirical study findings and strong advocacy from international clinical experts highlights the need to consider the inclusion of gluteal strengthening in the rehabilitation of individuals with PFP.
Moving more proximally, some experts also recommend the incorporation of core stability or trunk strengthening exercises into rehabilitation. Although lacking any validation through level 1 evidence or from clinical trials, recent studies have reported reduced lateral trunk strength52 and increased ipsilateral trunk lean during squatting53 and running,54 providing some justification for these recommendations. Qualitative data suggests the inclusion of distal strengthening may be important for some individuals with PFP, which may in some instances be more effective than foot orthoses. The paucity of research evaluating the efficacy of distal strengthening in PFP highlights an area requiring attention in future research.
Lower limb stretching in isolation currently lacks level 1 evidence, but some experts recommended consideration, particularly of the hamstrings and calf, in order to optimise knee and ankle biomechanics. Supporting justification for hamstring stretching, White et al55 reported an 8° reduction in hamstring flexibility in a group of individuals with PFP when compared to asymptomatic controls, with PFJ stress during squatting thought to increase in the presence of reduced hamstring flexibility.56 Additionally, Witvrouw et al57 reported reduced gastrocnemius flexibility may be a risk factor for PFP development. Inflexibility of the iliotibial band (ITB) has also been reported in individuals with PFP.58 Interestingly, stretching the ITB was not strongly advocated by experts interviewed, some stating it is not a modifiable factor or that stretching it is ineffective. Further research to evaluate the clinical effectiveness of stretching and how to determine those likely to benefit is needed.
Gait and movement pattern retraining
Although lacking level 1 evidence, movement pattern and gait retraining was advocated by experts interviewed in this study, with consideration of activities including walking, running, stair negotiation and sit to stand recommended (see online supplementary file 2.4). However, a lack of consensus among experts on the level of difficulty in implementing these strategies exists, primarily owing to the fact that the majority of research reporting favourable findings utilised gait laboratories to facilitate running retraining.59–61 Regardless, considering recent promising case series findings for gait retraining in runners with PFP,59–61 movement pattern retraining may be a valuable addition to the clinical management of PFP. Clearly further research to establish clinical approaches to facilitate movement pattern retraining, and evaluate their effectiveness is needed.
Adjunctive interventions
Massage and PFJ mobilisation in isolation lacks level 1 evidence, although they are frequently included in multimodal programmes evaluated in research and commonly applied in clinical practice (see online supplementary file 2.6). Inconsistent beliefs regarding the value of PFJ mobilisation in rehabilitation exists, but consensus was that mobilisation should only be considered in the presence of joint restriction, and never in a PFJ that was already hypermobile. Massage was advocated to reduce muscle and facial tightness, particularly of lateral structures, indicating research is needed to evaluate its value in the management of PFP. Distally, consideration to foot and ankle sagittal plane mobility is thought to be important. Specifically, mobilisation to address ankle and first ray dorsiflexion restriction in order to limit compensatory pronation and internal tibial rotation; and subtalar joint mobilisation to optimise shock absorption is recommended. Considering a lack of guidance on how best to determine the need for mobilisation and massage was provided, this should be addressed in future research.
Quality of available systematic reviews
Overall the quality of reviews has improved since the original review of systematic reviews related to the conservative management of PFP,13 with 46% (6/13) of reviews rated high quality and an average quality score of 16.3. This compares to 30% (3/10) of reviews rated high quality and an average quality score of 13.7 in the previous review.13 Importantly, four of the six high-quality reviews were not Cochrane reviews, compared to no high-quality non-Cochrane reviews being previously identified.13 Additionally, all reviews, except one29 used valid quality assessment scales to critique studies included. This equated to 86% (6/7) of lower quality reviews, much higher than the 43% (3/7) of lower quality reviews including valid quality assessment previously.13 Put together, these findings highlight improved methodological processes being undertaken by research groups completing systematic reviews evaluating conservative interventions for PFP.
Of the seven lower quality reviews, only two25 ,36 attempted any additional alternate searching, only one36 included non-English language studies, none were deemed to have used an adequate range of key words, and only three24 ,25 ,28 used two independent reviewers during application of their search strategy. Each of these methodological factors increases the risk of missing relevant studies,18 reduce the trustworthiness of findings,18 and hence should be addressed in future reviews.18 Of the lower quality reviews, only 43% (3/7) attempted or discussed limitations to meta-analysis,25–27 and 29% (2/7) used predetermined criteria for levels of evidence to base conclusions on.24 ,25 These methodological weaknesses mean the findings of these lower quality reviews are open to narrative bias,18 and should be addressed in future research.
Limitations
Although focusing on level 1 evidence (high-quality reviews) to summarise the current evidence base ensures only the highest possible quality of evidence is summarised, one inherent limitation is that published reviews often omit emerging knowledge and early research findings due to stringent inclusion and exclusion criteria. Additionally, there is often a lag between when the final search completed in the review and its publication. Therefore, some review findings included in this study may be considered outdated. To address this, contemporary research findings not synthesised in the results section were also included in the discussion of findings (eg, gluteal strengthening) and development of the ‘Best Practice Guide to Conservative Management of Patellofemoral Pain.’ Additionally, the interview component of this study included discussion of emerging evidence and clinical reasoning for the use of interventions lacking an evidence base.
Experts included in this study consisted of physiotherapists, physical therapists and athletic trainers, but did not include sports physicians, rheumatologists or surgeons. Therefore, those professions are not specifically represented as authors of the ‘Best Practice Guide to Conservative Management of Patellofemoral Pain.’ However, the guide is focused on conservative management which is commonly considered the first-line treatment approach for PFP.
It is likely that experts’ clinical reasoning is informed, and therefore could be described as biased, by systematic review findings given their professional interest. Moreover, given that many of the interviewed experts have been involved in the included systematic reviews, their clinical reasoning may have in turn biased focus, findings and conclusions reported. This is an inherent limitation of the evidence generation and synthesis process, and was not felt to be a barrier to high-quality clinical guidance of practice. The clinical summary (see online supplementary figure 1) used to guide discussion between the researcher and interviewee was based primarily on findings from included systematic reviews and may have therefore led to biased discussions regarding topics with current established evidence. To address this to some extent, the clinical summary used to stimulate discussion included interventions with emerging evidence—such as gait retraining—and did not outline the strength of evidence for any included intervention. Additionally, the topic guide (see box 1) included scope for discussion of clinical reasoning regarding interventions lacking evidence.
Initial evaluation and framework analysis was completed by an experienced physiotherapist, which could lead to biasing of findings. However, this individual did possess previous interview and analysis experience related to qualitative research. Additionally, data accuracy and interpretation was checked by an additional researcher with extensive qualitative research experience, and an additional experienced clinician. Validity of qualitative findings was further strengthened through triangulation of findings via respondent validation.
Gaps in evidence and future research directions
Based on a paucity of research or a discord between the evidence base and expert clinical reasoning, there is a clear lack of guidance regarding various exercise prescription principles, including the value of OKC and CKC; duration and frequency of exercise sessions; and level of supervision required at various stages of rehabilitation. Addressing these questions in future research should be a priority. The synthesis of current level 1 evidence with expert opinion for the management of PFP highlights a number of additional research priorities. These include empirical research to establish the value of core and distal strengthening, and the value of patellar taping in the longer term. Experts also highlighted a number of research priorities (see online supplementary file 2.7) including identifying modifiable risk factors so that better prevention programmes can be developed, and the source of pain to guide treatment. Further priorities were: development of tests to identify chronicity or osteoarthritis risks; optimised education; improved criteria to individually tailor interventions; long-term effectiveness of interventions; and the impact of psychosocial factors on PFP, including how to identify and address them. Specific interventions recommended as priorities for research included the effectiveness of proximal strengthening and gait retraining; and understanding how the foot, footwear and foot orthoses relate to pathology.
The ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’ has been based on a combination of contemporary level 1 evidence and the analysis of international experts’ clinical reasoning. However, despite its strengths, the guide should be considered preliminary. Further evaluation of its usefulness to guide clinical practice, and best methods of translation (eg, online tutorials, workshops, teaching at undergraduate level, etc.) is needed. Proof of efficacy should be definitively established by clinical trials. Finally, the methods used in this study have significant potential for replication in order to provide similar guides for the management of other conditions across the specialties.
Conclusion
Our mixed methods approach yielded qualitative data that complements robust systematic review data to help guide clinicians managing patients with PFP. A tailored multimodal intervention programme, complemented with patient education and activity modification is the key to effective PFP management. Active components should include quadriceps and gluteal exercise, with consideration to core and distal strengthening and movement pattern/gait retraining. Patellar taping can be applied to facilitate pain reduction in the early stages of rehabilitation. Stretching of the calf, hamstring and quadriceps should also be considered if indicated depending on individual assessment. Adjuncts may include foot orthoses, massage, and PFJ mobilisation. These principles are summarised in the ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’ which provides a foundation for discussion at the next International Patellofemoral Pain Research Retreat (Manchester, September 2015).
What is already known on this subject?
Patellofemoral Pain (PFP) is a highly prevalent multifactorial condition.
Numerous biomechanical and behavioural factors must be considered for effective management of PFP.
Systematic reviews that do not consider expert clinical reasoning or provide definitive guides to management when making recommendations are barriers to knowledge translation.
What this study adds?
This review of reviews uses only the best quality synthesised evidence, in combination with the world's experts’ views.
A clear ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’ based on the combination of the current evidence base and synthesised international expert opinion.
Effective and efficient management of PFP requires sound clinical reasoning to guide the provision of an individually tailored multimodal intervention programme including quadriceps and gluteal strengthening, patellar taping, and an emphasis on education and activity modification.
Acknowledgments
The authors would like to thank all the expert clinical academics who gave their precious time and expertise, and the senior musculoskeletal rehabilitation team at Bart’s Health NHS trust who fed back on the study findings. The authors would also like to thank Paulina Kloskowska, PhD candidate at the Centre for Sport and Exercise Medicine, Queen Mary University of London, for her German article translation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
- Data supplement 2 - Online supplementary file 1
- Data supplement 3 - Online supplementary file 2
- Data supplement 4 - Online supplementary file 3
Footnotes
Contributors DM, CJB and SM were involved in study concept and design. CJB, SL and ST participated in acquisition of data. CJB, SL and ST conducted analysis related to systematic review component. DM obtained funding and ethical clearance. All the authors took part in critical revision of manuscript for important intellectual content.
Funding Funding was received from The UK EPSRC (Engineering and Physical Sciences Research Council) and AXA-PPP healthcare via a Knowledge Transfer Account for some of DM's time. DM is part funded by the NIHR/HEE Senior Clinical Lecturer scheme. This article presents independent research part-funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None.
Ethics approval QMUL ERC.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Happy to share.