Article Text

Abstract
Background A previous meta-analysis showed that maximal oxygen uptake increased by 3.51 mL/kg/min (95% CI 3.07 to 4.15) during a recreational football programme of 3–6 months in comparison with continuous moderate-intensity running, strength training or a passive control group. In addition, narrative reviews have demonstrated beneficial effects of recreational football on physical fitness and health status.
Objective The purpose of this systematic review and meta-analysis was to evaluate the magnitude of effects of recreational football on blood pressure, body composition, lipid profile and muscular fitness with reference to age, gender and health status.
Design Systematic review and meta-analysis.
Data sources MEDLINE, PubMed, SPORTDiscus, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Google Scholar were searched prior to 1 February 2017. In addition, Google Scholar alerts were set up in January 2012 to identify potential papers with the following key terms: recreational football, recreational soccer, street football and street soccer.
Eligibility criteria for selecting studies Randomised and matched controlled trials with participants allocated to a recreational football group or any other type of exercises or passive control group were included. Training programmes had to last at least 2 weeks to meet the inclusion criteria. The primary outcome measures were blood pressure, resting heart rate, body composition, muscular fitness, and blood lipids and glucose tolerance. A total of 31 papers met the inclusion criteria and were included.
Results The effect of recreational football on systolic blood pressure (SBP) versus no-exercise controls was most likely extremely largely beneficial (effect size (ES)=4.20 mm Hg; 95% CI 1.87 to 6.53). In addition, a most likely very large beneficial (ES=3.89 mm Hg; 95% CI 2.33 to 5.44) effect was observed for diastolic blood pressure (DBP), when compared with non-active groups. Furthermore, a most likely extremely large beneficial effect was shown for SBP and DBP in participants with mild hypertension (11 and 7 mm Hg decrease, respectively) and participants with prehypertension (10 and 7 mm Hg decrease, respectively). Meta-analysis of recreational football determined the impact on resting heart rate as most likely extremely largely beneficial (ES=6.03 beats/min; 95% CI 4.43 to 7.64) when compared with non-active groups. The observed recreational football effect on fat mass was most likely largely beneficial (ES=1.72 kg; 95% CI 0.86 to 2.58) and the effect on countermovement jump (CMJ) performance was most likely very largely beneficial (ES=2.27 cm; 95% CI 1.29 to 3.25) when compared with non-active groups. Possibly beneficial decreases were found in low-density lipoprotein levels (ES=0.21 mmol/L; 95% CI 0.06 to 0.36). Possibly largely beneficial effect was observed for DBP in comparison with continuous running training. Small harmful and unclear results were noted for SBP, fat and lean body mass, body mass index, as well as muscular fitness when compared with running and Zumba training.
Conclusion The present meta-analysis demonstrated multiple broad-spectrum benefits of recreational football on health-related physical fitness compared with no-exercise controls, including improvements in blood pressure, resting heart rate, fat mass, low-density lipoprotein cholesterol and CMJ performance. Additionally, recreational football is efficient and effective as Zumba and continuous running exercise regimens with highlighted social, motivational and competitive components.
- football
- health promotion
- physical fitness
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
It is now well established that physical fitness is a strong mortality predictor and that physical training is a cornerstone in the prevention and treatment of lifestyle diseases including hypertension, type 2 diabetes and osteoporosis.1–4 Conventional training approaches such as high-intensity interval training, endurance running and strength training are well known to be effective in improving cardiovascular, metabolic and musculoskeletal fitness, respectively.5–8 However, participation in multifaceted exercise training may be effective in simultaneously stimulating all three main fitness areas, thereby providing broad-spectrum fitness and health benefits.2–5 Over the last decade, there has been growing evidence that recreational football is precisely this type of multifaceted exercise training. Small-sided football training for untrained health adults across the lifespan as well as several patient groups have been shown to elicit average heart rates of 80%–85% of maximal heart rate (HRmax) during 60 min sessions, with 15%–50% of total training time in the highest aerobic training zone above 90% HRmax.6 In addition, small-sided football training comprises multiple strength training elements, with more than 100 high-intensity runs and hundreds of specific intense actions such as dribbles, shots, tackles, turns and jumps in 60 min training sessions.7 Many individual studies have reported recreational football to be an effective type of physical activity with positive effects on hypertension in middle-aged men8 and women,9 on cardiovascular and metabolic responses in patients with type 2 diabetes,10 on heart function,11 on physical capacity,12 on muscle mass in patients with prostate cancer11 and on bone mineral density and mass,13 with positive effects in various age categories and populations on cardiorespiratory fitness, muscular fitness, health profile and physical capacity,5 and three narrative reviews have confirmed the effects of recreational football training on cardiovascular, metabolic and musculoskeletal fitness regardless of age and health status.9 10 14 To date, only two systematic reviews and meta-analyses have evaluated the effects of recreational football, and these had a predominant focus on aerobic fitness. Milanović and colleagues6 meta-analysed 17 studies and reported that recreational football produces large improvements in maximal oxygen consumption (VO2max) compared with strength training and no-exercise controls, while a moderate effect size (ES) was observed in comparison with continuous endurance running. Likewise, Oja et al 15 showed significant positive effects on maximal oxygen consumption and resting heart rate (RHR) compared with a no-exercise control, with borderline significance for fat percentage. The effects of recreational football on broad-spectrum fitness and health benefits, however, have yet to be meta-analysed.
The purpose of this systematic review and meta-analysis was therefore to carry an up-to-date evaluation of the broad-spectrum health-related fitness effects of recreational football training in relation to age and health status, with a specific focus on the magnitude of effects on (1) blood pressure, (2) RHR, (3) body composition, (4) muscular fitness evaluated as jump performance, and (5) blood lipids and glucose tolerance.
Methods
Search strategy and study selection
The search and study selection strategy applied in this systematic review and meta-analysis was similar to that of a previous published paper by Milanović et al.6 All procedures relevant for papers’ identification were carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.16 Computerised literature searches were conducted on the following databases: MEDLINE, PubMed, SPORTDiscus, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Google Scholar. A structured search included papers published prior to 1 February 2017. In addition, Google Scholar alerts were set up in January 2012 to identify potential papers with the following key terms: recreational football, recreational soccer, street football and street soccer. A manual search was performed covering the areas of recreational football/soccer, recreational physical activity, recreational small-sided games and physical fitness using the following key terms and strings, either singly or in combination: (‘recreational small-sided games’ (All Fields) OR ‘recreational football’ (All Fields) OR ‘recreational soccer’ (All Fields) OR ‘street football’ (All Fields) or ‘street soccer’ (All Fields)) AND (‘effect’ (All Fields) OR ‘impact’ (All Fields) OR ‘influence’ (All Fields)) AND (‘physical fitness’ (Mesh) OR ‘health status’ (Mesh) OR ‘blood pressure’ (Mesh) OR ‘countermovement jump’ (Mesh) OR ‘CMJ’ (Mesh) OR ‘body composition’ (Mesh) OR ‘body mass index’ (Mesh) OR ‘lean body mass’ (Mesh) OR ‘body mass’ (Mesh) OR ‘resting heart rate’ (Mesh) OR ‘blood lipid’ (Mesh) OR ‘glucose tolerance’ (Mesh)) AND (‘randomised controlled trial’ (All fields) OR ‘randomized controlled trial’ (Publication Type)).
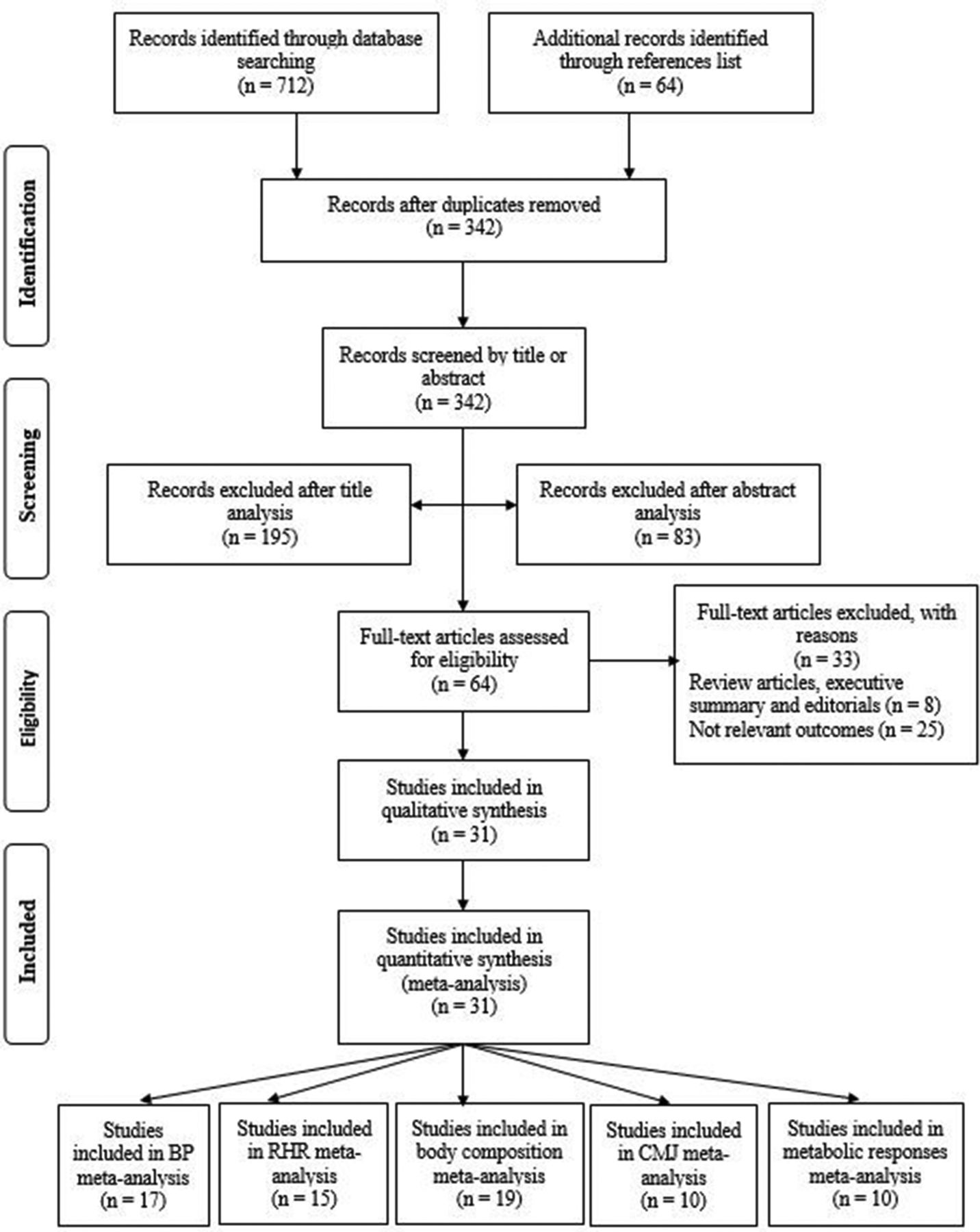
The study selection process is shown in figure 1. Two independent reviewers (ZM and NČ) performed the literature search, identification, screening, quality assessment and data extraction. First, the titles were initially screened by the reviewers during the electronic searches to assess suitability of papers, and all papers beyond the scope of this meta-analysis were excluded. Second, abstracts were assessed using predetermined inclusion and exclusion criteria. Third, the full texts of the remaining papers that met the inclusion criteria were retrieved for inclusion in the ongoing procedure and reviewed by the two reviewers to reach a final decision on inclusion in the meta-analysis. Finally, reference lists from retrieved manuscripts were also examined for any other potentially eligible papers. Any disagreements between the reviewers were resolved by consensus or arbitration by a third reviewer (GS). If full text of any paper was not available, the corresponding author was contacted by mail or ResearchGate. Inclusion and exclusion criteria were considered study characteristics and report characteristics (table 1).
Inclusion and exclusion criteria
Systematic review and characteristics of included studies selected for meta-analysis and relevant outcomes
Systematic review and overall observed effects for metabolic parameters
Type of study and participants
Randomised and matched controlled trials were included in meta-analysis without any restriction on age and health status of participants.
Type of interventions
Training programmes had to last at least 2 weeks, with participants allocated to a recreational football group and any other type of exercise or a passive control group. Studies with unbalanced diet in groups were excluded from analysis.
Type of outcome measure
The primary outcome measures for the meta-analysis were blood pressure, RHR, body composition, muscular fitness evaluated as jump performance, and blood lipids and glucose tolerance.

Flow chart diagram of the study selection; BP, blood pressure; CMJ, countermovement jump; RHR, resting heart rate.
Data extraction
The Cochrane Consumers and Communication Review Group’s standardised protocol for data extraction was used to extract (1) study characteristics including author(s), title and year of publication; (2) participant information such as sample size, age, health status and gender; (3) description of the training intervention, including types of exercise, intensity, duration and frequency; and (4) study outcomes, including the following physical fitness components: systolic and diastolic blood pressure, RHR, body mass, body mass index (BMI), lean body mass (LBM), fat mass, and metabolic responses including low-density and high-density lipoproteins (LDL and HDL), total cholesterol, triglycerides, fasting blood glucose and glucose tolerance, and muscular fitness (see supplementary file 1 and supplementary file 2). When needed, pre-BMI and post-BMI values were manually calculated. In most of the studies, mean and SD (also computed when dispersion was expressed as SEM) prevalues and postvalues were reported, while correlation was not reported. Accordingly, in these instances the correlation value was set at 0.5, as used previously by Bacon et al.17 Graph digitiser software (DigitizeIt, Braunschweig, Germany) was used to obtain data values in studies where only plots were published. Data extraction was undertaken by ZM, while NČ checked the extracted data for accuracy and completeness. Disagreements were resolved by consensus or by GS. The reviewers were not blinded to authors, institutions or manuscript journals. The summary of findings with appropriate quality of evidence table was created using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach.18 The methodological criteria were dependent on five primary domains (risk of bias, inconsistency, indirectness, precision and publication bias), as well as the overall quality of the evidence (high, moderate, low or very low).
Supplementary file 1
Supplementary file 2
Assessment of risk of bias
Risk of bias was evaluated according to the PRISMA recommendation.19 Physiotherapy Evidence Database(PEDro) scale was used to determine the quality of the studies and potential risk of bias. Two independent reviewers assessed the quality and risk of bias using checklists. Agreement between the two reviewers was assessed using k statistics for full-text screening and rating of relevance and risk of bias. In the event of disagreement about the risk of bias, the third reviewer checked the data and took the final decision on it. The k agreement rate between reviewers was k=0.94.
Statistical analysis
Difference in means and 95% CIs were calculated for the included studies. The I2 measure of inconsistency was used to examine between-study variability, with values greater than 50% considered indicative of high heterogeneity.20 This statistic, expressed as a percentage between 0 and 100, can be interpreted as the percentage of heterogeneity in the system or, basically, the amount of total variation accounted for by the between-studies variance.21 Publication bias was assessed by examining asymmetry of funnel plots using Egger’s test, and P<0.10 was considered a significant publication bias. Pooled estimates of the effect of recreational football on blood pressure, RHR, body composition, metabolic responses and muscular fitness using ES were obtained using random-effects models. ES values were classified as follows: <0.2 trivial, 0.2–0.6 small, 0.6–1.2 moderate, 1.2–2.0 large, and >2.0 very large and >4.0 extremely large.22 The precision of the pooled effect was reported as a 95% CI and as probabilities that the true value of the effect was trivial, beneficial or harmful in relation to threshold values for benefit and harm. The chance of the true effect being trivial, beneficial or harmful was then interpreted using the following scale: 25%–75%, possibly; 75%–95%, likely; 95%–99.5%, very likely; and >99.5%, most likely.17 These probabilities were then used to make a qualitative probabilistic inference about the overall effect.21 Five moderator variables with appropriate levels were selected for additional analysis of all outcomes: (1) type of control group (no-exercise, continuous running, strength training and Zumba groups); (2) gender (male and female); (3) age (18–45, 45–65 or >65 years); (4) length of training intervention (≤12 weeks and >12 weeks); and (5) training frequency (≤2 weeks and >2 weeks). In addition, the type of hypertension was used as a moderator for systolic blood pressure (SBP) and diastolic blood pressure (DBP) outcome where levels were normotensive, mild-hypertensive and hypertensive. All statistical analyses were conducted using Comprehensive Meta-analysis V.2 software (Biostat, Englewood, New Jersey, USA). P<0.05 was considered statistically significant.
Results
Study selection and characteristics
A total of 712 papers were identified across the databases in the initial search and an additional 64 papers were selected on the basis of their references. After duplications were removed, 342 papers remained. Based on a screening of the title and abstract, 278 articles were discarded (195 excluded after title analysis, 83 excluded after abstract analysis). The full text of the 64 remaining papers was assessed in more detail for eligibility. Each paper was carefully read and coded for study characteristics, participant information, description of the training intervention and study outcomes. Thirty-three papers did not meet the inclusion criteria, while 31 papers that met the inclusion criteria were included in the systematic review and meta-analysis. There were 17, 15, 19 and 10 papers included in the meta-analysis of blood pressure, RHR, body composition and muscular fitness, respectively (table 2). Additionally, 10 papers were included for metabolic response comparisons (table 3).
All eligible studies were controlled trials, published in English from the beginning of 2009 until February 2017. In order to perform meta-analysis from 31 papers that met the inclusion criteria, 17 studies5 8 9 23–36 featured data changes in blood pressure, 15 covered RHR,5 8 9 23–25 29–35 37 19 papers2 5 9–11 24–32 34–39 related to body composition, while 10 studies2 11 12 24 38–43 provided sufficient data for muscular fitness. Metabolic responses data extraction featured 10 studies for plasma LDL and HDL,5 9 10 24–26 30 31 35 45 8 studies for plasma triglycerides,9 10 24–26 30 35 45 9 for total cholesterol5 9 10 24–26 30 35 45 and fasting blood glucose,10 24–26 30 31 35 37 45 and 5 for glucose tolerance10 12 24 30 31 35 (figure 1).
Football training intervention
Recreational football training interventions were composed of a 10–15 min warm-up period followed by competitive game formats of 4 vs 4, 5 vs 5, 6 vs 6, 7 vs 7, and 9 vs 9 without specific tasks. Pitch dimensions ranged from 20×30 m to 45×65 m covered with grass and artificial grass surfaces or asphalt as well as indoor surfaces. Authors did not report the playing role of the goalkeeper or the specific rules used during matches. All subjects trained for between 10 and 72 weeks. The most common intervention periods were 12 weeks2 5 11 23 24 27 29 41 and 16 weeks.12 28 37 Total time in the high aerobic intensity zone (>90% HRmax) ranged from one-tenth to one-third of overall exercise time.
Study outcomes for blood pressure
The meta-analysed effects of recreational football on SBP and DBP were similar (table 4). The recreational football effect on SBP when compared with no-exercises controls was most likely extremely largely beneficial. A most likely extremely large beneficial (ES=3.89 mm Hg; 95% CI 2.33 to 5.44) effect on DBP was observed for recreational football compared with no-exercise groups. A most likely extremely large beneficial ES was observed in the group of participants with mild hypertension (decrease of 10.8 and 6.8 mm Hg for SBP and DBP in football group and 4 and 0 mm Hg in controls). In the prehypertensive group, the observed effects were most likely extremely largely beneficial (ES=5.52 mm Hg; 95% CI 3.51 to 7.54; decrease of 7.3 and 2.0 mm Hg for football group and controls) and likely extremely largely beneficial (ES=4.36 mm Hg; 95% CI 0.02 to 8.70; decrease of 9.5 and 4.7 mm Hg for football group and controls) for DBP and SBP. In the normotensive group, the observed effects were possibly largely beneficial for both SBP and DBP (ES=1.80 mm Hg; 95% CI −0.04 to 3.65 and ES=1.21 mm Hg; 95% CI −0.11 to 2.32).
Effect of recreational football on systolic and diastolic blood pressure with modifying effects for type of control group, gender, age, length of training intervention and training frequency
When the results were analysed separately for men and women, the meta-analysed effect of recreational football on SBP was possibly very largely beneficial and very likely extremely largely beneficial for men and women (ES=2.25 mm Hg; 95% CI 0.21 to 4.30 and ES=4.17 mm Hg; 95% CI 1.15 to 7.19, respectively). For the DBP results the evidence was stronger for an effect in men than in women, with most likely very large beneficial effects for men (ES=3.98 mm Hg; 95% CI 2.32 to 5.64) and likely very large beneficial effects for women (ES=2.28 mm Hg; 95% CI 0.82 to 3.75). When a comparison of recreational football effects was performed for the age groups, most likely extremely large beneficial and most likely very large beneficial effects were noted in the 45–65 age group for both SDP and DBP, as well as for the likely very large beneficial effects for DBP in the 18–45 age group. In the 18–45 and +65 groups, the effects were unclear for SBP, and in the +65 group the effects for DBP were unclear. Unclear (ES=0.67 mm Hg; 95% CI −1.90 to 3.24) and a likely very largely beneficial (ES=2.15 mm Hg; 95% CI 0.46 to 3.83) ES were seen for SBP and DBP for the duration time of up to 12 weeks of training. Most likely extremely large beneficial effects (ES=4.59 mm Hg; 95% CI 2.46 to 6.72) and most likely very large beneficial effects (ES=3.63 mm Hg; 95% CI 2.14 to 5.12) were observed for training periods lasting more than 12 weeks for SBP and DBP, respectively. When the results were moderated using training frequency, a likely large beneficial and most likely extremely large beneficial ES were retrieved for moderators (≤2 and >2 sessions per week) for DPB. Likely very large beneficial effects were observed for SBP for both moderators. A mean decrease of 5.3 mm Hg and 4.0 mm Hg for SBP and DBP was observed for football group and 3.5 and 0.7 mm Hg for controls, respectively.
The effects on SBP of football when compared with running and Zumba groups were possibly moderately harmful, while the effect on DBP was unclear when compared with a Zumba group. The effect of recreational football on DBP when compared with continuous running was possibly largely beneficial (ES=2.21 mm Hg; 95% CI −0.81 to 5.23).
Study outcomes for RHR
Meta-analysis of the effect of recreational football on RHR was determined as most likely extremely largely beneficial (ES=6.03 beats/min; 95% CI 4.43 to 7.64) when compared with a non-active control group (table 5). A small unclear effect was found in comparison with running (ES=0.57 beats/min; 95% CI −1.48, to 2.62). Most likely extremely large beneficial and very likely very large beneficial effects were observed for male and female gender moderators (ES=5.06 beats/min; 95% CI 2.48 to 7.64 and ES=2.95 beats/min; 95% CI 0.76 to 5.14). The effect on RHR in individuals 18–45 years old was beneficial (ES=3.19 beats/min; 95% CI 0.95 to 5.43, very likely very largely beneficial). When compared with the 45–65 and 65+ age groups, the observed effects were most likely extremely largely beneficial (ES=5.66 beats/min; 95% CI 2.14 to 9.18 and ES=6.00 beats/min; 95% CI 4.34 to 7.66). In cases where the results were compared by the training intervention duration moderators, the results were unclear and beneficial for up to 12 weeks (ES=1.99 beats/min; 95% CI −2.09 to 6.08) and longer than 12 weeks (ES=4.70 beats/min; 95% CI 2.76 to 6.65, most likely extremely largely beneficial). Most likely extremely large beneficial effects were observed when training frequency was ≤2, while very likely very large beneficial effects were reported in the case of two or more sessions per week. Most likely very large beneficial (ES=3.83 beats/min; 95% CI 2.16 to 5.51) effect of recreational football intervention was computed for the overall sample.
Effect of recreational football on resting heart rate and muscular fitness with modifying effects for type of control group, gender, age, length of training intervention and training frequency
Study outcomes for body composition
Trivial and small effects were observed for BMI compared with all other investigated training regimens (table 6). Similar results were observed for body mass where the meta-analysed effects were trivial to small regardless of the type of control moderators, with unlikely small beneficial and very unlikely small harmful effects for the no-exercise and running groups (table 6). ES values for LBM were trivial and small regardless of moderator variables (table 7). In addition, the meta-analysed effect of recreational football compared with Zumba and for participants 46–65 years old was unclear. With respect to the overall gender sample, the effect of football training was rated as very likely moderately beneficial (ES=1.10 kg/m2; 95% CI 0.54 to 1.66). Observed recreational football effect values with respect to fat mass were most likely largely beneficial (ES=1.72 kg; 95% CI 0.86 to2.58) when compared with no-exercise controls (table 7). The effects were possibly small harmful when compared with running (ES=−0.41 kg; 95% CI −1.24 to 0.42) and unclear when compared with Zumba (ES=0.35 kg; 95% CI −1.54 to2.24). With respect to gender, ES was very likely largely beneficial and possibly moderately beneficial for male and female moderators. Beneficial effects were observed in the groups of 18–45 years old and 45–65 years old (possibly moderately beneficial and most likely large beneficial). When subgroup analysis was performed, very likely large beneficial and likely moderately beneficial effects were observed for intervention duration of up to 12 weeks and over 12 weeks, while unlikely small harmful and most likely large beneficial ES was seen for up to two sessions per week and over two sessions per week.
Effect of recreational football on body mass index and body mass with modifying effects for type of control group, gender, age, length of training intervention and training frequency
Effect of recreational football on lean body mass and fat mass with modifying effects for type of control group, gender, age, length of training intervention and training frequency
Study outcomes for muscular fitness
Overall change induced by recreational football training on countermovement jump (CMJ) was classified as moderately likely beneficial (ES=1.08 cm; 95% CI 0.15 to 2.00). The meta-analysed effect on CMJ of recreational football compared with no-exercise controls was most likely very largely beneficial (ES=2.27 cm; 95% CI 1.29 to 3.25; table 5). The effect was unclear when compared with running (ES=0.28 cm; 95% CI −1.05 to 1.61) and possibly trivially harmful when compared with strength training (ES=−1.06 cm; 95% CI −3.40 to 1.28). In cases where the results were analysed separately for men and women, ES values were very likely largely beneficial and unclear. When compared between age groups, for 18–45 years old ES was unclear, for the group of 46–65 years old it was unlikely trivially harmful (ES=−0.01 cm; 95% CI −1.03 to 1.01), and for the 65+ group the result was very likely largely beneficial (ES=1.63 cm; 95% CI 0.48 to 2.78). For training intervention duration, the effects were classified as unclear (ES=0.09 cm; 95% CI −1.86 to 2.03) for the up to 12-week intervention period and most likely largely beneficial (ES=1.72 cm; 95% CI 0.77 to 2.66) for the over 12-week intervention period. With respect to the training frequency, the effects were likely largely beneficial (ES=1.56 cm; 95% CI 0.00 to 3.12) and likely moderately beneficial (ES=1.05 cm; 95% CI −0.15 to 2.25) for up to two sessions per week and over two sessions per week.
Study outcomes for metabolic responses
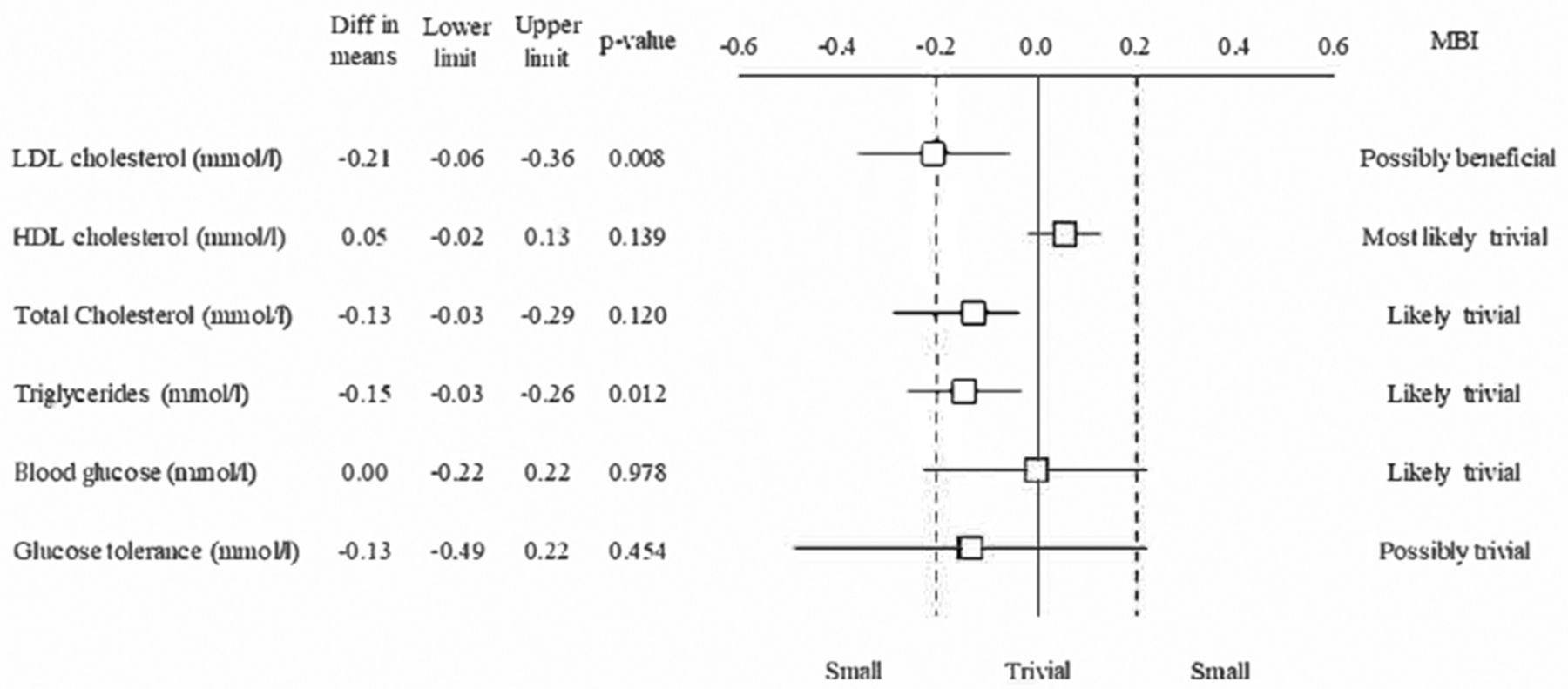
Effects of recreational football on metabolic responses were compared with no-exercise controls, but not compared by type of training intervention, sex, age, training frequency and duration moderators (figure 2). Overall effect was classified as possibly small beneficial (ES=0.21 mmol/L; 95% CI 0.06 to 0.36) for plasma LDL cholesterol (figure 2). Most likely trivial (ES=0.05 mmol/L; 95% CI −0.02 to 0.13) were observed for plasma HDL cholesterol. Likely trivial effects were observed for total plasma cholesterol (ES=0.13 mmol/L; 95% CI −0.03 to 0.29), plasma triglycerides (ES=0.15 mmol/L; 95% CI 0.03 to 0.26) and blood glucose (ES=0.00 mmol/L; 95% CI −0.22 to 0.22), while possibly trivial effects were seen for glucose tolerance (ES=−0.13 mmol/L; 95% CI −0.49 to 0.22) (figure 2).
{kind=link}
{kind=link}
Forest plot of the effect sizes and 95% CIs of the changes in overall metabolic parameters. HDL, high-density lipoprotein; LDL, low-density lipoprotein; MBI, magnitude-based inferences.
Publication bias
The Egger’s test was performed to provide statistical evidence of funnel plot asymmetry. The results indicated publication bias for blood pressure and CMJ analysis (P<0.10). Publication bias was not observed for the remaining variables (P>0.10).
GRADE recommendations for strength of evidence
Observed results strongly recommend to use recreational football to reduce BMI, body mass and LBM because overall quality of evidence is high without any publication bias or inconsistency among included studies (table 8). Moderate quality of evidence was determined for SBP and DBP without inconsistency. Results recommended recreational football because of its desirable effects on SBP and DBP. Additionally, certainty of metabolic parameters (total plasma cholesterol, LDL, triglycerides, fasting blood glucose and glucose tolerance) was high without risk of bias and inconsistency. In contrast, certainty of fat mass variable is low with serious inconsistency as well as strongly suspected publication bias.
GRADE quality of evidence of included studies and relevant outcomes
Discussion
The principal findings from the 31 papers that met the inclusion criteria were that recreational football has multiple positive effects on health-related physical fitness in comparison with no-exercise controls, including beneficial effects on systolic and diastolic blood pressure, RHR, fat mass, plasma LDL cholesterol and CMJ performance.
Previous meta-analyses have revealed that recreational football interventions lasting 3–4 months have a positive impact on maximal oxygen uptake compared with no-exercise controls in both men and women, with calculated average effects of 4.11 mL/kg/min15 and 3.51 mL/kg/min,6 respectively. One of the main findings of the present study is that, when compared with no-exercise controls, recreational football interventions demonstrate additional positive effects on cardiovascular fitness and health profile, including improvements in blood pressure. Indeed, the impact of 3–4 months of recreational football organised as 45–60 min two to three times per week was most likely beneficial for SBP and most likely beneficial for DBP compared with no-exercise controls. As expected, a greater blood pressure reduction was observed with 3–4 months of recreational football interventions for participants with hypertension than for individuals with normotension.45 The observed reduction in SBP and DBP was 11 and 7 mm Hg in subjects with mild hypertension and 10 and 7 mm Hg in individuals with prehypertension. These improvements are comparable with the acute effect of taking one standard dose of a blood pressure-lowering drug,46 and have important clinical importance as a blood pressure reduction of such a magnitude corresponds to a lowered risk of stroke by 20%–30% in individuals with hypertension.46
The positive effects were observed in both men and women, and for age groups of 18–45 years old and 45–60 years old. Specifically, the meta-analysis showed the effect of recreational football on SBP to be possibly very large and very likely extremely largely beneficial in men and women, and indicated that the effect on DBP was greater for men than for women. When recreational football effects were related to age, likely very large beneficial effects were observed for DBP in the 18–45 age group and most likely very largely beneficial for the 45–65 age group, whereas only the 45–65 age group had positive effects on SBP. It was interesting to note that a harmful effect was found for SBP and a large beneficial effect for DBP compared with continuous running. Aerobic training that lasts between 16 and 52 weeks can lower resting blood pressure (both SBP and DBP) by 1%–2%.35 47 Football training proved to be superior in lowering DBP directly induced through improved muscle capillarisation, decreased arterial stiffness and increased cardiac relaxation time.35 Recreational football effectively lowered SBP, but in comparison with Zumba exercise it had moderately negative effects. Physiological effects including cardiovascular response to Zumba activity are not fully elucidated and further research is needed.26 27
With regard to the impact of recreational football training on RHR, our findings provide further support for the previous scientific studies that found that heart rate decreases with 3–4 months of recreational football performed for 45–60 min two to three times per week (6 beats per minute).15 Hence, the present meta-analysis showed the effect of recreational football on RHR to be most likely extremely largely beneficial when compared with a non-active group, with positive very large effects in men as well as women. Positive effects were detected across all adult age ranges, including those aged 18–45 years old, 45–65 years old and over 65 years. No clear evidence was obtained when comparing the effects of recreational football on RHR with those of other sporting activities.
The present meta-analysis rates the effect of recreational football with respect to fat mass to be most likely largely beneficial compared with inactive controls, which is in accordance with the recent analysis by Oja et al.15 Thus, football training interventions lasting 12–16 weeks (2×60 min sessions/week) are likely to cause a decrease in total fat mass of 1–3 kg, which is clinically significant for overweight and obese adults.15 The present as well as other meta-analyses15 provide evidence that recreational football training is very likely beneficial for decreasing fat mass in both genders. Moreover, the 18–45 and 45–65 age groups were observed to respond to this type of physical training. The effects of football training are not as clear when compared with other exercise training protocols. For example, there are no clear effects when compared with Zumba dancing. Considering the limited number of studies reporting the effects of other sport disciplines, conclusions about the health benefits cannot yet be conclusively drawn. When evaluating the impact of recreational football on LBM, the effects were rated as trivial to small, when performed 2×60 min per week for 12–16 weeks, while the effect of football versus Zumba was unclear. In relation to gender, women display a greater effect than their male counterparts. In addition, participants in the 18–45 age group tend to respond better than older age groups (45–65 and 65+).
The effect of recreational football training on CMJ when compared with inactive controls was most likely very largely beneficial. The outcome of football training was unclear when compared with running and potentially lower when compared with strength training. Considering the limited existing data, no clear gender effect in women was detected with respect to the effects of recreational football training, while in men the effect was very likely largely beneficial. In individuals older than 65 years, somewhat greater ES were observed compared with the 18–45 age group. Finally, recreational football training interventions lasting longer than 12 weeks induced better responses in CMJ performance than interventions lasting less than 12 weeks.
Metabolic responses and their relationship to recreational football were displayed through changes in blood lipids, glucose concentration and glucose tolerance. It is strongly substantiated that exercise training lowers these metabolic risk factors for pathological conditions such as cardiac dysfunctions, sudden mortality and morbidity, arteriosclerosis and type II diabetes.3 24 35 In a narrative review by Bangsbo et al, 3 it was reported that changes provoked by recreational football were mainly non-significant, including reduced plasma LDL cholesterol level (4%–15%)5 29 33 and total plasma cholesterol (0.6%–8%),7 25 33 along with elevated HDL level (0%–9%).7 31 The present meta-analysis indicates similar outcomes with possibly small beneficial decrease in plasma LDL along with most likely and likely trivial in plasma HDL upregulation and triglycerides and total cholesterol decrement. The plasma LDL decrease was related mainly to increased weekly training frequency for the first 12 weeks, which could not be maintained for an additional 52 weeks when training frequency was reduced.24 35 The changes were generally caused by the responsive nature of LDL and HDL to aerobically induced energy expenditure.10 24 32 Additionally, the metabolic responses for fasting blood glucose and glucose tolerance (after 2 hours) were trivial. Although the precise effects of recreational football compared with other types of exercise were not meta-analysed due to insufficient data, it is evident that recreational football displays a greater effect on blood lipids compared with other aerobic exercise regimens,5 24 29 and that the magnitude of change is associated with sex, baseline obesity level and maximal oxidative capacity.32 Further scientific work should examine effectiveness of recreational football of different formats and in comparison with strength training on various health-related physical fitness components.
Despite the multitude benefits elucidated in the present systematic review and meta-analysis, there are some limitations. For example, it is plausible to suggest that studies reporting statistically significant or positive results are more likely to be published in scientific journals compared with results showing no treatment effects. In line with this statement, one of the limitations in this meta-analysis is the phenomenon of negative results publication bias. Additionally, the small number of included studies measuring metabolic parameters may be a limitation, since ES could not be calculated for moderator variables. Finally, the lack of duplicate data extraction could be considered as a limitation of this meta-analysis.
Conclusion
In conclusion, the present meta-analysis demonstrated multiple broad-spectrum positive physical health effects of recreational football training in comparison with no-exercise controls, including beneficial effects on blood pressure, RHR, fat mass, LDL cholesterol and CMJ performance. In addition, it was evident that the majority of these effects occurred independently of age and gender, and most of the effects, except improvements in CMJ, occurred after only 12 weeks of training. Recreational football proved to be similarly effective and beneficial when compared with other exercise regimens on health-related physical fitness components. Thus, recreational football is a worthwhile alternative to Zumba dancing and continuous running providing similar decreases in body weight and fat mass.
What is already known?
Recreational football is an intense versatile activity with marked positive effects on aerobic fitness.
This exercise modality is suitable for both genders regardless of age, fitness level and skills.
Recreational football is a highly motivating activity compared with conventional exercise programmes.
What are the findings?
Recreational football displays positive effects on health-related physical fitness in comparison with no-exercise controls, including beneficial effects on cardiovascular, metabolic and musculoskeletal health.
Recreational football induces a broad-spectrum positive impact on health-related physical fitness in healthy people regardless of gender and fitness level.
Recreational football can be applied as an effective broad-spectrum non-pharmacological treatment of lifestyle diseases, such as hypertension and metabolic syndrome.
References
Footnotes
Contributors ZM, SP and NČ selected the studies and extracted the data. ZM and GS analysed the data. ZM, NČ and PK were responsible for conception and design, and drafting and revising the manuscript. ZM, PK and MM wrote the paper, and all authors commented on the paper and approved the final version.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.