Article Text

Abstract
Objective To determine whether reported therapeutic interventions for arthrogenic muscle inhibition (AMI) in patients with ACL injuries, following ACL reconstruction, or in laboratory studies of AMI, are effective in improving quadriceps activation failure when compared with standard therapy in control groups.
Design A scoping review of the efficacy of interventions was conducted in accordance with the methodological framework of Arksey and O’Malley and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Search terms included ‘arthrogenic muscle inhibition’, ‘quadriceps activation following knee injuries’, ‘anterior cruciate’ or ‘knee’ combined with ‘quadriceps activation’, ‘quadriceps inhibition’, ‘corticomotor’, ‘arthrogenic’, ‘brain activation’ and ‘neuroplasticity’. Articles were evaluated for risk of bias using the PEDro (Physiotherapy Evidence Database) criteria. The overall quality of evidence for each intervention was assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE).
Data sources PubMed, EMBASE and Cumulative Index to Nursing and Allied Health Literature databases.
Eligibility criteria for selecting studies Isolated case reports and articles reporting outcomes in patients with chronic disease or major trauma were excluded. All other original research articles were included.
Results 780 potential articles were identified. 20 met the inclusion criteria. These studies provided a moderate quality of evidence to support the efficacy of cryotherapy and physical exercises in the management of AMI. There was low-quality evidence for efficacy of neuromuscular electrical stimulation and transcutaneous electrical nerve stimulation, and very low-quality evidence for efficacy of ultrasound and vibration.
Conclusions This scoping review demonstrated moderate-quality evidence for the efficacy of cryotherapy and physical exercises in improving quadriceps activation failure after ACL injury and reconstruction. These therapeutic modalities are therefore recommended in the management of AMI.
- knee acl
- quadriceps
- hamstring
- neuromuscular
- rehabilitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Quadriceps weakness is a frequently observed barrier to effective rehabilitation following ACL injury and reconstruction.1 2 It may lead to a wide range of important consequences, including extension deficit,3 gait abnormality,4 quadriceps atrophy,1 5 6 poor function,6 dynamic instability,7 persistent knee pain and early osteoarthritis.1 8
Quadriceps activation failure after ACL reconstruction (ACLR) is not simply an isolated local phenomenon related to atrophy. Many authors describe its synchronous occurrence in both reconstructed and contralateral limbs.9 This has been attributed to arthrogenic muscle inhibition (AMI), a process in which quadriceps activation failure is caused by neural inhibition. Mechanisms for this inhibition include alteration in muscle resting motor thresholds, changes in the discharge of articular sensory receptors, altered spinal reflex excitability (affecting the group I non-reciprocal (Ib) inhibitory pathway, the flexion reflex and the gamma loop)10 and abnormal cortical activity (intracortical inhibition and a requirement for greater frontal cortex theta power in basic movement and joint position sense tasks).11 12
Recently, several clinical studies have suggested specific treatment modalities for AMI.13–34 Most of the therapeutic interventions for AMI aim to alter motor excitability using disinhibitory mechanisms.35 These improve voluntary quadriceps activation by targeting either joint mechanoreceptors, the peripheral nervous system around the joint (mainly group III and IV afferent nerves) or the central nervous system directly.10 35 The aim of this scoping review was to determine the strength of evidence supporting the use of common therapeutic interventions for AMI in patients with ACL injuries, following ACLR, or in laboratory studies of AMI.
Methods
We conducted a scoping review as this approach is superior to a systematic review in addressing an exploratory research question.36 37 We followed the five-stage methodological framework of Arksey and O’Malley36 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 checklist (see figure 1). The study protocol was registered with PROSPERO (International prospective register of systematic reviews) database (trial registration number: CRD42017067499).
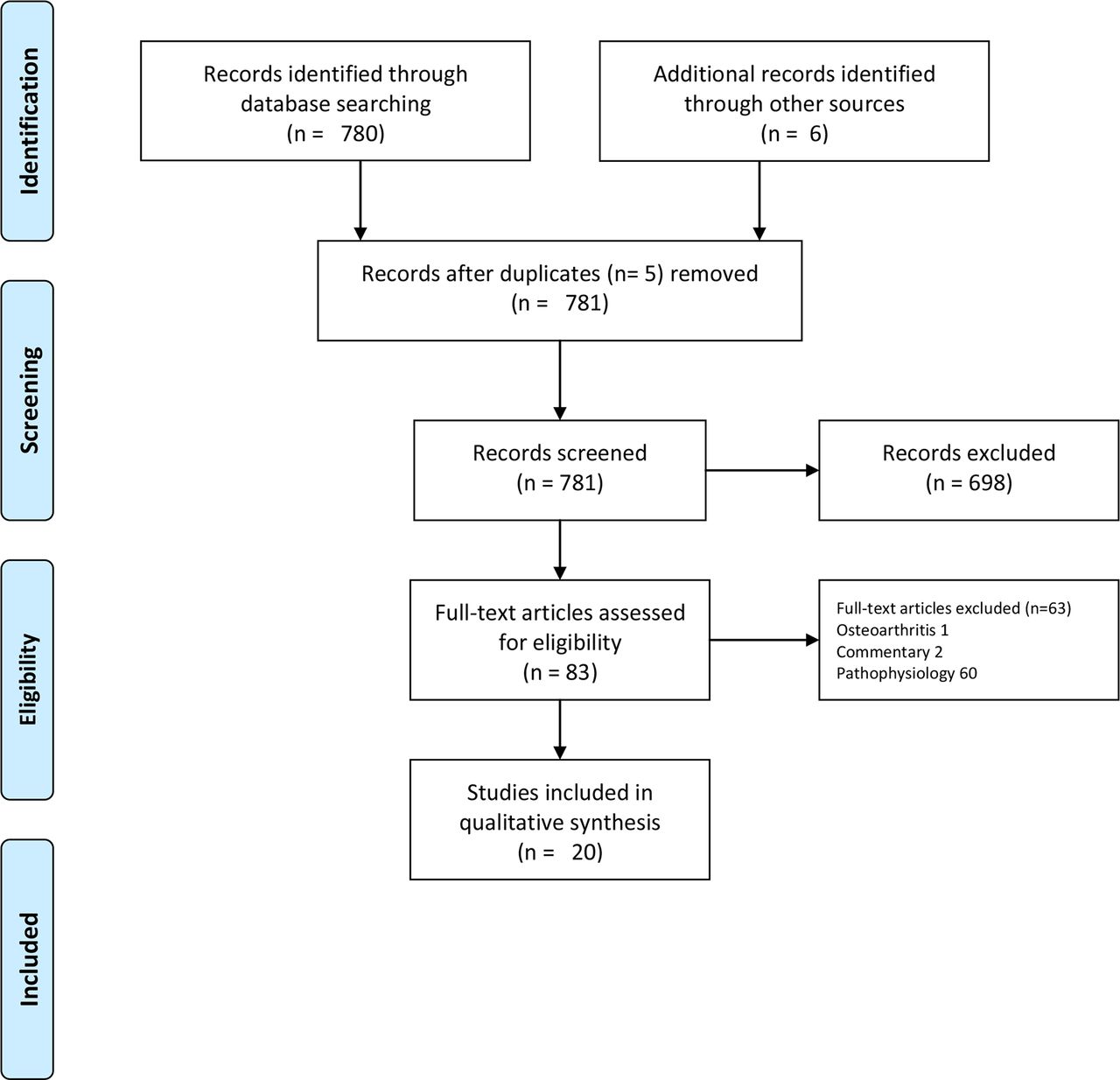
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Stage 1: identifying the research question
Our research question was ‘What is the strength of evidence supporting the use of common therapeutic interventions for AMI in patients with ACL injuries, following ACL reconstruction, or in laboratory studies of AMI?’
Stage 2: identifying relevant studies
The literature search used subject mapping and keywords and is presented in online supplementary appendix 1. The search strategy was applied to the PubMed, EMBASE and Cumulative Index to Nursing and Allied Health Literature databases by two authors independently on 12 March 2017. The same authors also independently performed all aspects of the study selection.
Supplementary file 1
Stage 3: study selection
We included primary research studies that evaluated the efficacy of therapeutic interventions for AMI. The main focus of the review was on AMI in patients following ACL injury or reconstruction. Due to the fact that treatment of AMI is an emerging concept with a small evidence base, it was deemed appropriate to use a scoping review methodology and include studies that intended to evaluate the efficacy of therapeutic interventions for the same pathological processes in selected, relevant, alternative settings. Therefore, studies including young patients with artificially induced knee effusions and other relevant acute knee pathologies (restricted to other knee ligament injuries, meniscal pathology and patellofemoral instability) were also included. Only studies published in the English language were included.38 39
We excluded isolated case reports and articles which included patients with chronic conditions (eg, osteoarthritis) or major trauma (fracture, multiligament injury, neurovascular injury). Any disagreement between reviewers regarding study eligibility were resolved through discussion.
Each article was reviewed for relevance, and the references of the included articles were examined to identify further eligible studies.
Stage 4: charting the data
Data extraction and risk of bias assessment were performed independently by two investigators. A template was used for data extraction that included study design, participants, inclusion/exclusion criteria, intervention investigated, comparators, outcome measures (quadriceps activation/strength including central activation ratio (CAR), peak torque, maximal voluntary isometric contraction (MVIC), H-reflex amplitude, knee flexion angle symmetry and muscle fibre conduction velocity), main findings, conclusion and level of evidence.
Stage 5: collating, summarising and reporting the results
Due to heterogeneity among studies with respect to the populations, interventions and outcomes studied, it was not possible to pool data. Instead, we collated efficacy data with respect to the outcome measures defined in stage 4 and synthesised a narrative summary of the evidence for each intervention.
To determine the strength of evidence, the following steps were undertaken. All included articles were individually evaluated for risk of bias using the Physiotherapy Evidence Database (PEDro) criteria.40 41 The level of evidence for individual studies was assessed according to the Oxford Centre for Evidence-based Medicine.42 The overall quality of evidence for each therapeutic intervention was assessed using the GRADE working group grades of evidence.43 Details of how the GRADE guidelines were applied are included in online supplementary appendix 2. Effect sizes were calculated using the methodology of Thalheimer and Cook.44
Supplementary file 2
Results
The search strategy yielded 780 articles. The references of these articles were then reviewed and a further six eligible studies were included. Five studies were removed as they were duplicates. After application of eligibility criteria, a total of 20 relevant articles were identified. The date of publication of the included studies ranged from 1990 to 2017.
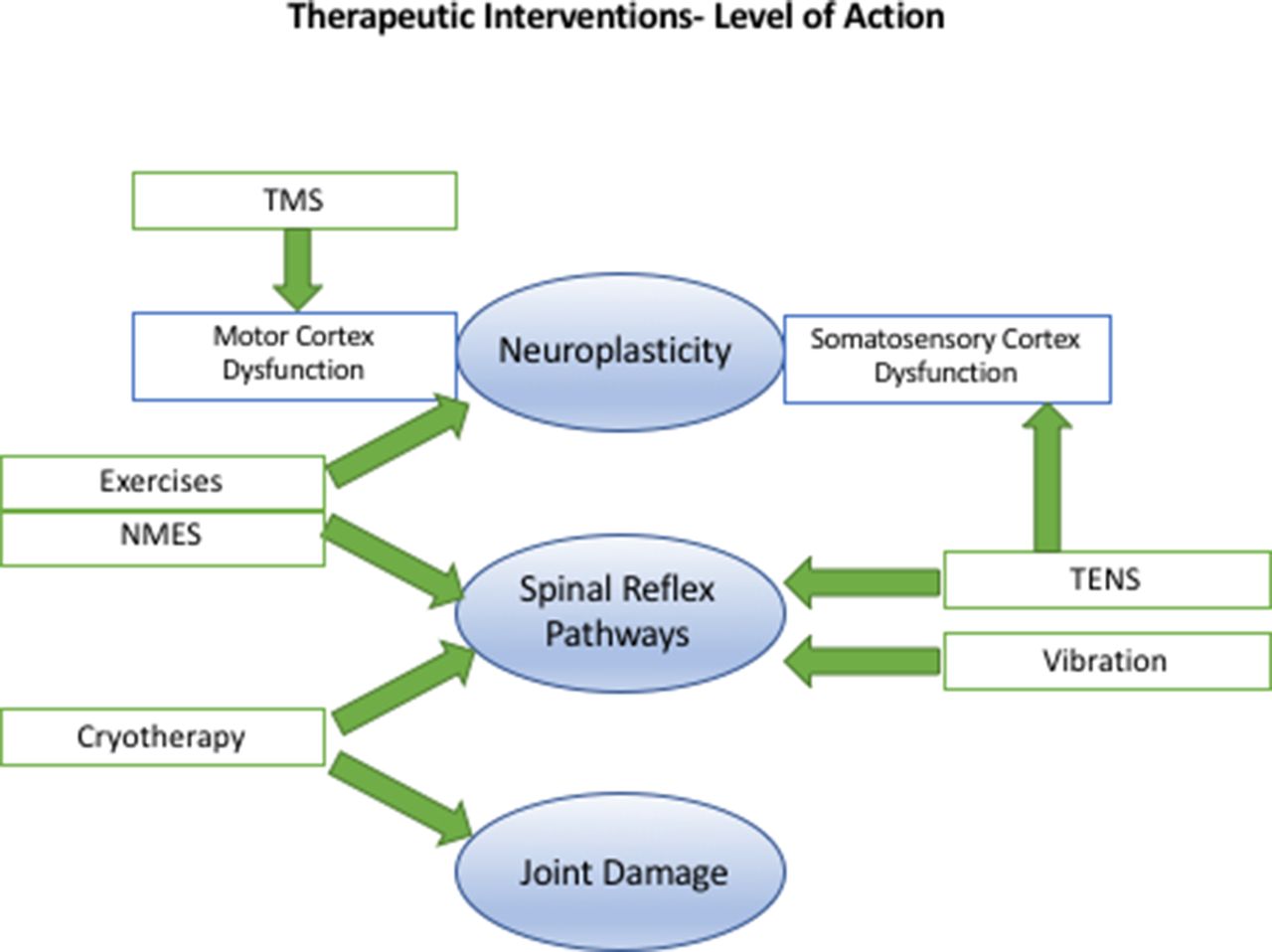
Table 1 summarises the study characteristics, level of evidence of the included studies, outcomes, effect sizes and the GRADE recommendation for each intervention. Table 2 demonstrates how the PEDro scores were calculated for each study. Table 3 demonstrates how the GRADE recommendations for each intervention were determined. The mechanism and level of action of the therapeutic interventions studied are summarised in figure 2.
Summary of included studies
GRADE table

{kind=link}
{kind=link}
Therapeutic interventions for arthrogenic muscle inhibition and their level of action. NMES, neuromuscular electrical stimulation; TENS, transcutaneous electrical nerve stimulation; TMS, transcranial magnetic stimulation.
Cryotherapy
Four studies evaluated the efficacy of cryotherapy in AMI. This included three randomised controlled trials (RCTs). All studies showed that cryotherapy improved the features of AMI; effect sizes were very large. Specifically, three of the studies demonstrated that cryotherapy was associated with significant improvement in quadriceps strength (measured by maximal voluntary isometric contraction).14–16 Additionally, Hopkins et al 13 demonstrated a significant improvement in quadriceps motor neuron pool recruitment (measured by the H-reflex). Note that two of these studies did not specifically evaluate patients following ACLR—they were laboratory studies of patients with artificially created knee effusions.13 14
Using the GRADE approach, there was moderate-quality evidence for the efficacy of cryotherapy in the treatment of AMI.
Exercise
Four studies evaluating the efficacy of exercise therapy in patients with AMI after ACLR were identified. These included the cryotherapy-based studies from Hart et al and Kuenze et al,15 16 which also made an adjunctive use of exercise. All of the included studies demonstrated that exercise therapy was associated with a significant improvement in quadriceps activation (MVIC and CAR).15–17 26
Three of the exercise programmes consisted of traditional open chain exercises with resistance, and progressive closed chain strengthening exercises of quadriceps and hamstring muscles.15–17 Resistance exercises included quadriceps sets, straight leg raises with hip abduction/adduction and progression to free-standing quarter squats, wall squats, hamstring curls, hip flexion/extension and leg press. Flexibility was attained using hamstring, quadriceps and calf stretching exercises. The fourth study examined the effect of a hamstring fatigue exercise protocol on patients with AMI following ACLR, in a case–control study.26 Hamstring fatigue was induced by participants performing squats to a height of approximately 0.45 m from the ground at the rate of one squat every 2 s. The quadriceps CAR of the ACLR group was significantly higher when evaluated after hamstring fatigue exercises (mean 96.0%, SD 7.6%) versus prefatigue (mean 81.2%, SD 15.8%; p=0.01).
GRADE assessment revealed moderate-quality evidence for the efficacy of exercise in the treatment of AMI.
Neuromuscular electrical stimulation
Two studies evaluated the same cohort of non-randomised patients who were allocated to four different rehabilitation groups.17 18 The authors reported that the group with combined neuromuscular electrical stimulation (NMES) and eccentric exercise demonstrated restored biomechanical limb symmetry that most closely resembled a control group of healthy individuals.18 However, there was no advantage with respect to quadriceps strength and activation.17 Furthermore, eccentric exercise alone recovered quadriceps strength (MVIC) better than individuals who only received NMES therapy, or the standard care following ACLR.17
Patterned electrical neuromuscular stimulation is a form of NMES which is proposed to mimic muscle-firing patterns of healthy individuals. A randomised trial failed to demonstrate any difference in knee extension torque or quadriceps activation, compared with a sham treatment.27
GRADE assessment revealed low-quality evidence for the efficacy of NMES in the treatment of AMI.
Transcutaneous electrical nerve stimulation
In the only randomised clinical study of transcutaneous electrical nerve stimulation (TENS) in patients with ACL rupture, there was no difference in isometric strength and quadriceps CAR among three groups (exercise only, exercise and TENS device, and 20 min of cryotherapy immediately prior to each daily exercise session).21 While all groups demonstrated a significant improvement in quadriceps strength, and effect sizes suggested potential clinical benefit to patients with AMI, the disinhibitory modalities were no better than exercise alone.
Three randomised trials, however, have shown some effect of TENS in improving AMI in the laboratory setting.13 19 20 Two trials showed a significant improvement compared with controls in the quadriceps muscle strength (MVIC),19 20 and the third showed it effectively disinhibited the quadriceps motor neuron pool (measured by H-reflex).13 Although TENS disinhibited the quadriceps motor neuron pool during the treatment, its beneficial effects were lost 30 min after cessation of treatment. In contrast, the beneficial effects of cryotherapy continued up to the final measurement of the H-reflex at 60 min post-treatment.
GRADE assessment revealed low-quality evidence for the efficacy of TENS in the treatment of AMI.
Vibration
Pamukoff et al 22 evaluated the role of vibration therapy. The authors randomised ACL reconstructed patients to three groups (whole body vibration (WBV), local muscle vibration (LMV) and control). There was a statistically significant increase in CAR (+4.9%) following WBV and LMV (+2.7%). There was also a reduction in quadriceps active motor threshold following WBV (−3.1%) and LMV (−2.9%), suggesting that the interventions increase corticomotor excitability. In a laboratory study, Blackburn et al 23 also identified that quadriceps CAR improved in WBV (11.4%) and LMV (7.3%) groups, but not in controls. However, we contend that these small changes are of limited clinical significance, particularly given that the mean time since ACLR was over 50 months and the patients did not have proof of AMI. Furthermore, these studies only evaluated the immediate effects of WBV and LMV.
GRADE assessment revealed very low-quality evidence for the efficacy of vibration in the treatment of AMI.
Ultrasound
An RCT evaluated patients with an intra-articular knee injury (22 of 30 were ACL injuries) and quadriceps CAR<90%.24 Non-thermal ultrasound (active) or sham treatment was applied to the knee for a duration of 17 min. The investigators observed increased quadriceps motor neuron pool excitability after ultrasound application compared with the sham group (14%–19% increase in the H-reflex amplitude, p=0.015).
GRADE assessment revealed very low-quality evidence for the efficacy of ultrasound in the treatment of AMI.
Transcranial magnetic stimulation
Only one trial was identified: an RCT (n=20) evaluated transcranial magnetic stimulation (TMS) in patients who had a partial meniscectomy and ongoing quadriceps weakness (CAR<85%).28 No significant difference in CAR or MVIC was seen compared with the control group that had no treatment. This systematic review did not identify any evidence supporting the use of TMS in the treatment of AMI.
Taping and bracing
Two RCTs assessed the effects of taping on quadriceps muscle performance.29 30 One assessed patients following ACLR,30 and the other assessed patients with a history of knee pathology and quadriceps CAR<90%.29 Neither study demonstrated a benefit over placebo for any outcome measure. A trial of 14 patients following ACLR randomised patients to receive either a knee brace, neoprene sleeve or no brace.31 No differences were observed between brace and no-brace conditions after aerobic exercise.
The available evidence does not support taping or bracing in AMI.
Other
A small case series of nine patients with anterior knee pain evaluated active release technique protocols.32 The active release technique is a system of soft tissue manipulation, purported to relieve tissue tension via the removal of fibrosis and adhesions. There was no effect in reducing quadriceps inhibition or increasing quadriceps strength. Another study found application of local anaesthetic cream had no effect in improving the sensorimotor function of the knee in subjects with ACL injury.33 An RCT of 12 patients with a history of knee-joint pathology and quadriceps CAR of <90% evaluated superficial heat application and found no effect on quadriceps function.34
The available evidence does not support these treatments in AMI.
Discussion
AMI is responsible for a considerable morbidity after ACLR.1 3 5–8 The main findings of this systematic review are that there is moderate-quality evidence to support the efficacy of cryotherapy and physical exercise therapy (open and closed chain resistance training, with hamstring fatigue exercises) in patients with AMI after ACL injury or reconstruction.
It is important to understand the pathophysiology of AMI to appropriately target therapeutic interventions. Several studies report an association between hamstring overactivity and dyskinesia with quadriceps weakness in AMI.45–47 This has been attributed to the flexion reflex spinal pathway, which produces a pattern of flexor facilitation and extensor inhibition. It is reported that greater hamstring coactivation is associated with significantly worse knee function.48 It is therefore unsurprising that hamstring fatigue exercises in patients with AMI following ACLR have been reported to be associated with a significant increase in quadriceps strength.26 In addition, all of the studies included in this review that evaluated physical therapy exercises (including open chain exercises with resistance, progressive closed chain quadriceps and hamstring strengthening exercises) in patients following ACLR, or artificially created knee effusion, demonstrated significantly improved quadriceps function (MVIC or CAR), which may indicate restoration of more optimal quadriceps neuromuscular function.14
All of the included studies on cryotherapy also demonstrated significantly improved quadriceps strength,13–16 and one study demonstrated reversed decline in motor recruitment (measured by H-reflex),13 in patients with AMI. Cryotherapy may reduce the discharge of sensory receptors and slow articular nerve conduction, thus decreasing transmission of the afferent impulses that contribute to deleterious spinal reflexive excitability.14
In this review, TENS13 19–21 and NMES17 18 27 had a low level quality of evidence to support their efficacy.19 TENS demonstrated large effect sizes in laboratory trials of artificial knee effusions. Although the single clinical trial on ACLR patients demonstrated no advantage over cryotherapy or exercise therapy alone, treatment with TENS demonstrated effect sizes that suggest potential benefits to patients with AMI.21 However, all patients in the TENS group also underwent exercise therapy, and therefore the role of TENS could not be evaluated in isolation. The three clinical trials identified in this study showed small to negligible effect sizes.17 18 27 The clinical results for both NMES and TENS preclude recommendation of these modalities in the management of AMI.
In this scoping review ultrasound therapy24 and vibration22 23 demonstrated very low-quality evidence for efficacy. Although two clinical studies (one vibration and one ultrasound) in ACLR patients demonstrated small statistically significant improvements (in CAR and H-reflex, respectively), these were of questionable clinical importance. Currently these modalities cannot be recommended in the management of AMI.
Other therapies including TMS,28 taping,29 30 bracing,31 application of heat34 and soft tissue release strategies32 were of no clinical benefit in the management of AMI.
Limitations
We note that some of the included trials were laboratory studies, and these cannot necessarily be extrapolated to the clinical scenario of AMI that occurs after ACL injury. The study methodology has attempted to account for this when awarding the GRADE level of evidence, with a decrease in the score by one level for studies that did not directly assess ACL-injured or reconstructed knees. Another limitation was that the studies were heterogeneous in design and limited by small patient numbers. The quality assessment of the trials using the PEDro scale ranged from 3 to 9 out of a maximum of 10. Lower quality studies were not excluded due to the relatively small number of clinical trials identified. Only English-language articles were included.
Conclusion
This scoping review demonstrated moderate-quality evidence for the efficacy of cryotherapy and physical exercises in improving quadriceps activation failure after ACL injury and reconstruction. These therapeutic modalities are therefore recommended in the management of AMI.
What is already known?
Lack of knee joint extension and impaired contraction of the quadriceps femoris muscle following ACL reconstruction is known as arthrogenic muscle inhibition (AMI).
AMI is associated with gait abnormality, long-term quadriceps atrophy, poor function, dynamic instability, persistent knee pain and early osteoarthritis.
What are the new findings?
Cryotherapy and physical exercises should form the mainstays of management of AMI.
Exercise should include traditional quadriceps and hamstring muscles open chain exercises with resistance, progressive closed chain strengthening exercises, as well as hamstring fatiguing exercises.
There is low-level evidence to support neuromuscular electrical stimulation and transcutaneous electrical nerve stimulation.
There is very low evidence to support ultrasound therapy and vibration.
Taping, bracing, application of heat and soft tissue release strategies demonstrated minimal or no benefit in the management of AMI.
Acknowledgments
None
References
Footnotes
Contributors All authors have given final approval of the submitted manuscript and their agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have made substantial contributions to the design of the work and manuscript writing. Conceptualisation of the work was by MT, BS-C and AS. The acquisition, analysis and interpretation of data were performed by WB, AS and AB. All authors were involved in drafting the work or revising it critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BS-C, AS and MT are all paid consultants for Arthrex. BS-C also receives royalties and research support from Arthrex.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.