Article Text

Statistics from Altmetric.com
Do I really need this test, treatment or procedure? What are the downsides? What happens if I do nothing? And are there simpler, safer options?
These four questions, promoted by Choosing Wisely Canada, featured prominently at the two 2018 conferences, Too Much Medicine in Helsinki, Finland (figure 1), and the sixth annual Preventing Overdiagnosis conference in Copenhagen, Denmark. Over 600 of the world’s leading researchers and thinkers in preventing overdiagnosis came together for two weeks in August 2018 to highlight the problems caused by medical excess and to identify evidence-informed practices to wind back the harms of too much medicine.

You can review highlights from the Too Much Medicine symposium on Twitter @TooMuchMed.
This education review aims to bring the sport and exercise medicine reader up to date on this topic. An expanded version with additional references and resources is provided in the online supplementary file.
Supplemental material
Too many people are being overdiagnosed, leading to overtreatment and wasted resources that could be better spent preventing or treating genuine illness. While debates about its definition continue, narrowly defined, overdiagnosis refers to deviations, abnormalities, risk factors and pathologies that would never cause symptoms or early death. It relates to problems of overmedicalisation and disease mongering, resulting in what one keynote speaker described as a ‘tsunami of overtreatment’.
As a review in BMJ discovered1 (figure 2), many factors drive overdiagnosis and cause harm, including cultural beliefs that ‘more is better’, financial incentives, expanding disease definitions and lowering treatment thresholds. While clinicians have been, and will forever be, challenged to balance Hippocratic notions of beneficence and non-maleficence, the scales are heavily tipped by the underlying influence of industry—such as Big Pharma, divisions of the media more interested in promotion than journalism, and medical journals serving professional rather than public interest. Attempting to summarise discussions at these recent conferences, we saw three specific problems: (1) Vested interests have too often replaced the best interests of patients. (2) Clinicians are being misinformed by flawed guidelines. (3) A lack of systemic transparency (regarding funding, impact and outcomes) is restricting clinicians in providing the best quality care for patients. Pollution, whether intentional or not, occurs at multiple points in the flow of healthcare information.
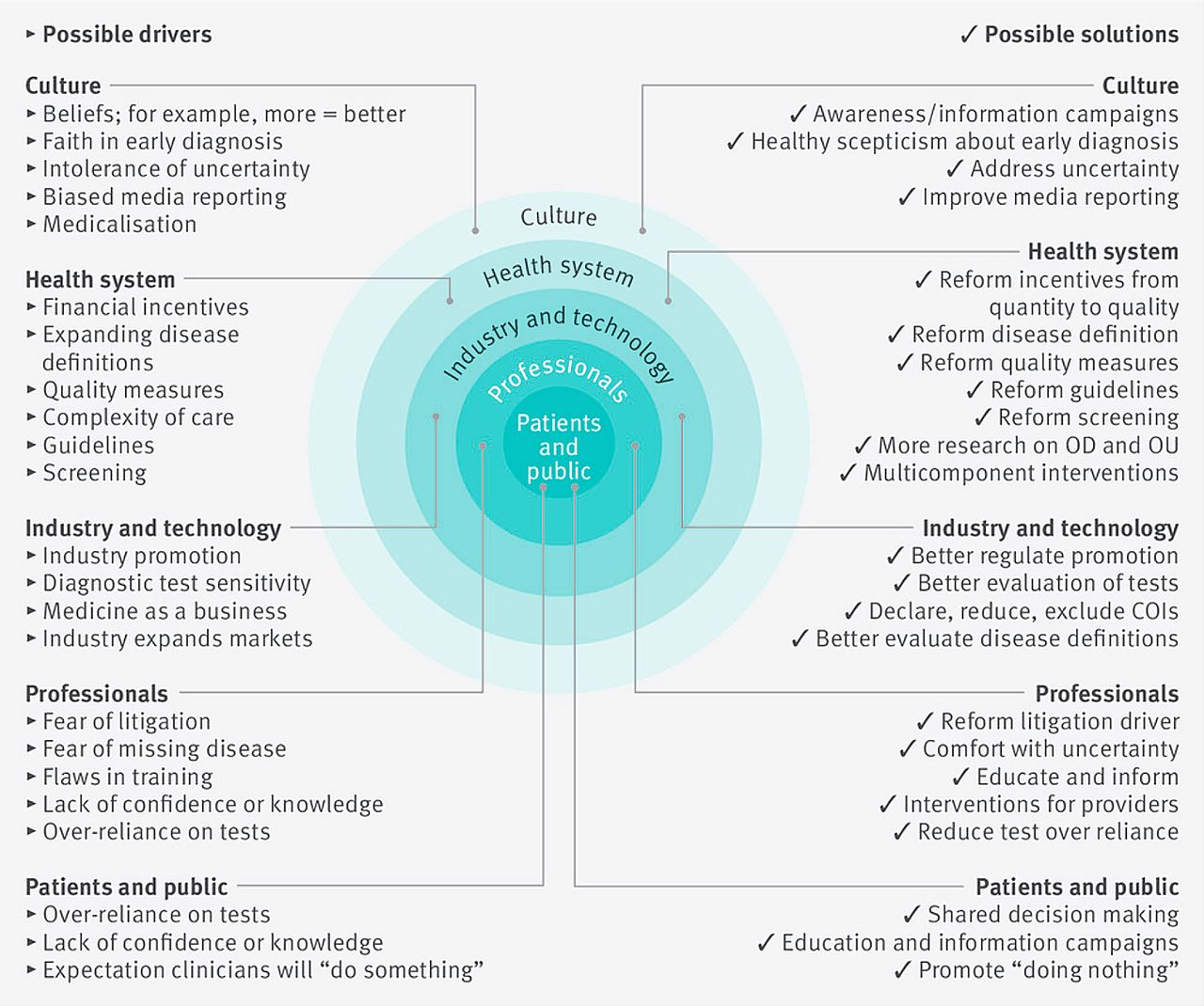
Mapping the drivers of overdiagnosis to possible solutions. COI, conflict of interest; OD, overdiagnosis; OU, overuse. (first published in BMJ) (adapted from Pathirana et al.1)
Here we introduce three themes from the conferences.
You’re sick, you just don’t know it yet
‘What is disease’ may seem like an elementary question, perhaps taught on day one of medical school, yet defining disease and its absence proves to be a circular, slippery slope (figure 3). The WHO definition of health as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’2 ignores that our perceptions of health and disease are context-dependent and change over time. At what point in their lives has anyone been ‘completely’ healthy?

Disease implies the converse of ‘complete’ health (whatever that means!).
Disease can refer to ‘a combination of signs and symptoms, phenomena associated with a disorder of function or structure or illness associated with a specific cause’.3 There are, however, no universally accepted criteria for defining disease, and so how do we differentiate ‘real’ diseases from human behaviours or experiences that happen to be ‘abnormal’ or unpleasant? We don’t.
Consider low back pain (LBP)—the number one cause of disability worldwide, which accounts for 83 million years lived with disability each year.4 Is LBP a disease? Or is it in fact a symptom? LBP can flag serious pathology, such as malignancy or infection, but for most individuals it is a benign problem without specific aetiology. Many individuals who consult their doctor or physiotherapist will experience no clinical benefit from receiving a diagnostic label. And if ‘labelled’, they may be more likely to adopt the sick role and suffer costly invasive treatments (eg, spinal implants) that have questionable value (figure 4).

What is driving the rising prevalence of chronic low back pain?
Medicalising ordinary life may be better described as disease mongering—that is, widening the boundaries of treatable illness to expand markets to sell medication and provide medical procedures/services. In what one speaker described as ‘the corporate construction of disease’, Big Pharma sponsors disease definitions (eg, Allergan and dry eyes; GSK and heartburn; GSK and restless leg syndrome) and promotes them to both prescribers and patients (figure 5). By magnifying all aspects of an ordinary ailment, upgrading mild symptoms to severe, and marketing risk as disease, disease mongering can augment population-wide fear and infect the healthy with lasting perceptions of ill-health.

Disease branding helps establish a condition as legitimate and serious.
Expanded disease definitions and lowered diagnostic thresholds means that it will soon be possible for everyone to be sick and require pharmacological intervention. If changes to recent guidelines highlighted at the conferences are any indication, it will not be long before prehypertension and prediabetes are preceded by preprehypertension and preprediabetes, and every one of us is categorised into a class of disease severity. According to the new American College of Cardiology/American Heart Association hypertension guidelines,5 one in every two American adults will soon be classified as having high blood pressure. All-encompassing diagnostic criteria enable healthy people to be labelled with lifelong disease, encouraging the treatment of the ‘worried well’ and the overutilisation of finite medical resources.
If you’re not sick, you just haven’t had enough tests
Thanks to rapid technological advances, we are increasingly able to find cancers, abnormal anatomy and risk factors for disease such as elevated blood pressure or cholesterol. Screening helps reveal low-risk abnormalities earlier, long before they cause symptoms or require treatment (if at all). While the overdiagnosis of breast, prostate and thyroid cancers through screening are common examples, there are similar concerns with musculoskeletal imaging (figure 6).
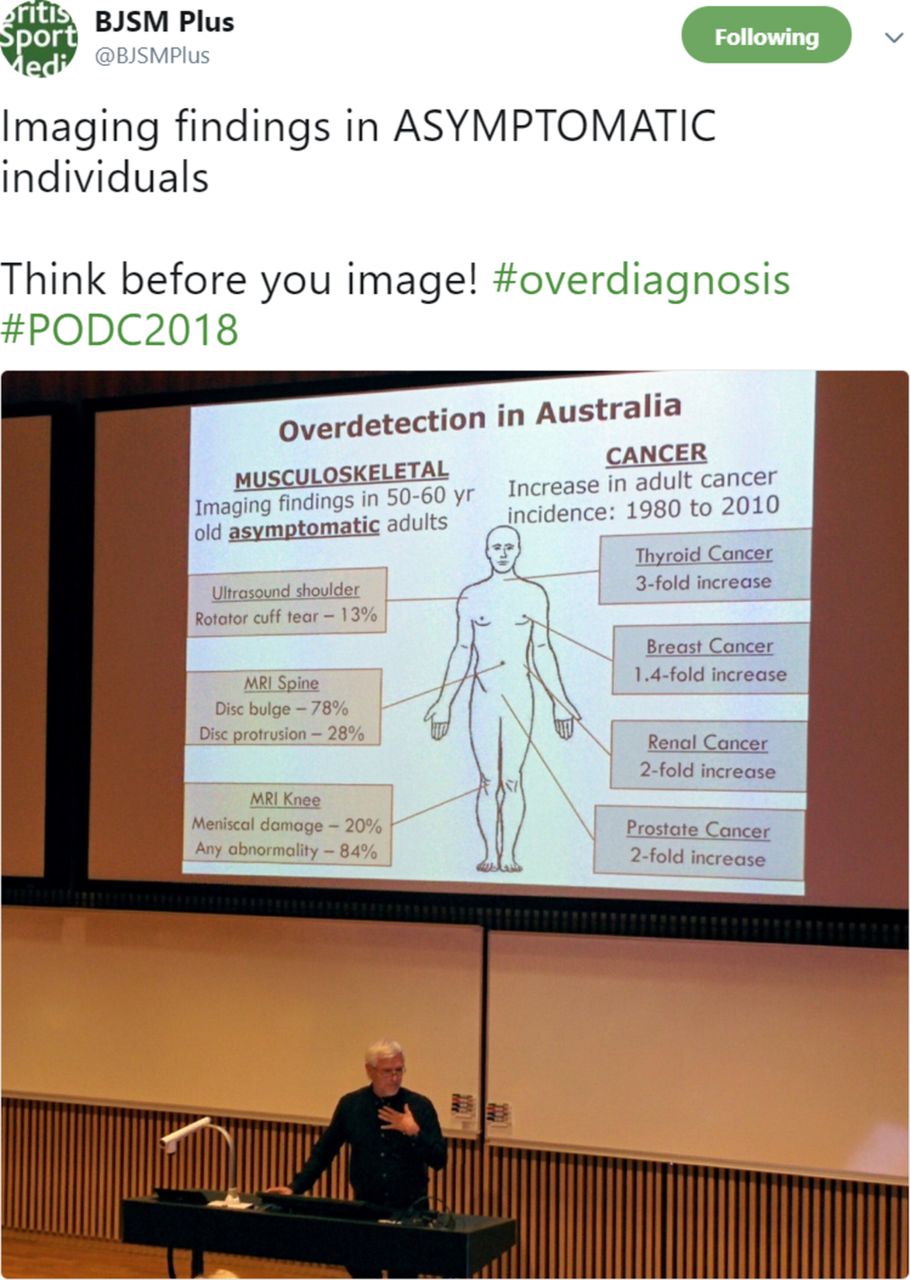
Prof Paul Glasziou, a former Director of the Centre for Evidence-Based Medicine in Oxford, currently at Bond University in Australia, explaining the consequences of screening programmes and unnecessary imaging during his keynote at Preventing Overdiagnosis 2018.
Imaging asymptomatic knees, shoulders and backs without indications of serious underlying pathology can lead to costly incidental findings, or ‘incidentalomas’ (a neologism combining the term ‘incidental’ [benign] and common tissue pathology suffix ‘oma’). While few coincidental diagnoses may be beneficial, many findings lead to unnecessary anxiety and a cascade of clinical follow-up (figure 7). The more we test, the more we will find.

The Ottawa Ankle Rules can help clinicians determine whether a patient with foot or ankle pain should undergo X-rays to diagnose a possible fracture and reduce costly, unnecessary imaging. MSK, musculoskeletal.
A pill for every ill
Physicians are armed with a prescription pad, so they tend to prescribe medication. Surgeons are equipped with a scalpel, so they operate. Give us a hammer and everything looks like a nail. We all start medical school with a goal to help people, and so when the potential opportunity arises, we use the tools we have to intervene. ‘I can or I must fix it’ is a learnt response from years of studying abnormal pathology and pharmacological mechanisms of action. The real question is: Why are we not taught that doing nothing is sometimes the best approach? And whatever happened to watchful waiting or conservative management?
Big Pharma promises a pill for every ill, and medical device companies provide a tool for every procedure. We note that for federal government approval (e.g. Food and Drug Administration), devices have a lower bar to reach than do medications. Magic bullets and quick fixes are much easier to sell than physical activity, nutrition, mindfulness and other unattractive lifestyle interventions—all lumped together in the last 30 seconds of a 15-minute consultation while the patient is getting up to walk out the door.
The topic of many presentations at the conferences, Choosing Wisely is a campaign that aims to engage doctors and patients in decisions about potentially unnecessary medical tests, treatments and procedures (figure 8). It started in the USA in 2012 and has since expanded internationally. The initiative encourages medical specialty societies (sport and exercise medicine included) to identify five tests and procedures that could potentially be avoided to reduce the harms of too much medicine.

Do you really need that MRI or knee scope?.
Orthopaedic surgery received some heavy criticism at the conferences and many speakers were quick to highlight the unnecessary procedures that continue to be performed on trusting patients. It has already been over 15 years since we found out that for patients with osteoarthritis of the knee, arthroscopic lavage or debridement are no better than placebo.6 More recently, Professor Teppo Järvinen (@shamteppo), the Chair of this year’s Too Much Medicine symposium, and his research team also demonstrated the lack of efficacy of common surgical procedures for degenerative meniscal tears7 and shoulder impingement.8 As more than 600 conference attendees found out, a surgical fix does not always fix the problem.
An uphill battle
Professor Allen Frances, an American psychiatrist known for chairing the task force that produced the fourth revision of the Diagnostic and Statistical Manual, framed the uphill battle against too much medicine as a ‘David vs Goliath story’. The forces that benefit from maintaining and increasing overdiagnosis have seemingly endless resources to promote it, and the relative few supporting evidence-based best practice have pocket money in comparison. And while overdiagnosis may be the most important story in health today, it struggles to find its way onto the front pages. We need to amplify and disseminate the conferences’ important messages beyond the echo chamber of academic circles. We need to work out how to fire the slingshots, because ‘the goliath is very big and we are awfully small’.
Several major medical journals have dedicated special editions solely to articles discussing the harms of too much medicine, such as the BMJ’s Too Much Medicine campaign and JAMA’s Internal medicine’s Less is More series. There are books, podcasts and even annual conferences (figure 9), yet efforts to reduce overdiagnosis are still hindered by clinicians’ and patients’ lack of awareness of the problem.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Save the date: The seventh international Preventing Overdiagnosis conference #PODC2019 will be in Sydney, 5–7 December 2019.
We must all play our part to prevent overdiagnosis. Global action is needed from all stakeholders. Clinicians can start by:
Embracing a healthy dose of scepticism and taking a more questioning approach to healthcare.
Adopting more thoughtful management approaches and referral practices that empower patients to engage in shared decision making based on the best available evidence.
Advocating for more transparent healthcare systems (funding, impact and outcomes) and models that do not promote fee-for-service.
Because when it comes to medicine, sometimes less is more.
Acknowledgments
The authors thank Dr Ray Moynihan for comments on a draft of this manuscript.
Footnotes
Twitter Follow Daniel Friedman at @ddfriedman
Contributors DJF was responsible for conception and initial draft of the manuscript. KMK was involved in drafting and critical revision of the manuscript, as well as final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KMK is the Editor in Chief of BJSM and was at arm’s length (and blinded) from the review process in BJSM.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.