Article Text

Abstract
Objective To describe the criteria used to clear athletes to return to sport (RTS) following primary ACL reconstruction.
Design Scoping review.
Data sources MEDLINE, Embase, CINAHL and SPORTDiscus electronic databases were searched using keywords related to ACL and RTS.
Eligibility criteria Prospective or retrospective studies reporting at least one RTS criterion for athletes who had primary ACL reconstruction with an autograft.
Results In total, 209 studies fulfilled the inclusion criteria. RTS criteria were categorised into six domains: time, strength, hop testing, clinical examination, patient-report and performance-based criteria. From the 209 included studies, time was used in 178 studies (85%), and in 88 studies (42%) was the sole RTS criterion. Strength tests were reported in 86 studies (41%). Sixteen different hop tests were used in 31 studies (15%). Clinical examination was used in 54 studies (26%), patient report in 26 studies (12%) and performance-based criteria in 41 studies (20%).
Summary Time and impairment-based measures dominated RTS criteria, despite sport being a complex physical and biopsychosocial activity with demands across all aspects of function. Time was included as a criterion in 85% of studies, and over 80% of studies allowed RTS before 9 months. Whether RTS tests are valid—do they predict successful RTS?—is largely unknown.
- acl
- testing
Statistics from Altmetric.com
Introduction
When should an athlete return to sport (RTS) after an ACL reconstruction?1 2 Evidence-based guidelines2–4 advocate for a test battery to evaluate quality and quantity of movement with a limb symmetry index (LSI) of at least 90%. However, limb symmetry does not indicate the athlete has reached the preinjury level of function, the preinjury function may be insufficient for safe sports participation and performance, and qualitative asymmetries can exist despite quantitative symmetry.5 6 Inconsistent and contradictory recommendations, which can arise when using a time-based as opposed to a criterion-based protocol, challenge practitioners and athletes when they are working together to plan RTS. It is unclear whether RTS testing practices reflect recommendations for a multifactorial, multidisciplinary approach to RTS decision making.7–9 The first step in establishing guidance on RTS testing is to understand how such testing is approached in the published literature.
A previous review10 describing the criteria used to determine unrestricted participation in sport was limited in at least four ways: (1) only one electronic database (MEDLINE) was searched; (2) only studies published between April 2001 and April 2011 were eligible for inclusion; (3) the population of interest was not clearly defined; and (4) the International Classification of Functioning, Disability and Health (ICF) criteria were not addressed.11 The ICF framework reflects an athlete-centred approach to understanding the current state of RTS testing.
The primary aim of this scoping review was to describe the criteria used in published research to clear athletes to RTS following primary ACL reconstruction. The secondary aim was to summarise the historical trends of RTS criteria and the current status of RTS testing.
Methods
A scoping review design and methodology was used due to the exploratory nature of the research question. Scoping reviews are recommended when the aim is to collate and comprehensively summarise the literature on topics of a substantial and varied nature.12 13 Due to the descriptive and exploratory nature of scoping reviews, study quality and risk of bias assessments are not appropriate and do not influence scoping review outcomes.12 13
Identification and selection of studies
We conducted librarian-assisted computer searches of the MEDLINE, CINAHL, Embase and SPORTDiscus electronic databases for studies on discharge criteria for RTS following primary ACL reconstruction. The search was performed on 12 September 2017 with no date limit. The goal was to maximise the sensitivity of our search strategy,14 15 increasing the likelihood that all appropriate studies were identified. The search was limited to humans and English language, peer-reviewed publications. The search strategies for MEDLINE, CINAHL, Embase and SPORTDiscus are listed in online appendix I. The reference lists of relevant systematic reviews identified during the title and abstract screen were also hand searched to identify any potentially eligible articles that may have been missed in the electronic database search.16
Supplemental material
Inclusion in this review was based on:
Study design: prospective or retrospective intervention or observational studies with a population greater than 10 athletes (to avoid small case series and case reports that may not best represent RTS after ACL reconstruction) published in English language. Systematic reviews, conference abstracts, case studies, narrative reviews and non peer-reviewed studies were excluded.
Participants: athletes (as defined by each study) of any age or competition level who had undergone primary ACL reconstruction with an autograft. At least 80% of participants had to be an athlete for the study to be included for review. We set a minimum of 80% athletes to maximise the chance that participants desired to RTS. We defined non-athletes as those who did not participate in sport. If studies did not define the population of interest as athletes but stated that patients returned to sport, we assumed they were athletes. Athletes with concomitant surgical procedures (eg, meniscus resection or repair, collateral ligament repair, posterior cruciate ligament reconstruction or repair) performed in combination with ACLR were included provided the ACL reconstruction was the primary procedure (80% of surgical procedures performed in the study).
Intervention: at least 80% of athletes in the study underwent ACL reconstruction with an autograft. Studies where allografts, ACL repair or other graft sources were used in a primary surgical procedure, and studies where ACL reconstruction was not the primary procedure performed were excluded.
Outcomes: any criterion used for clearance to RTS.
Time: all postsurgical time frames reporting RTS criteria were included. There were no limits to year of study publication.
All references were downloaded to the Rayyan reference management platform (rayyan.qcri.org), and duplicates were removed prior to screening. Two authors independently screened titles, abstracts and reviewed articles in full text. During title and abstract screening, if at least one reviewer concluded that a study met the selection criteria or if it was unclear whether the study should be included or excluded, the study was included. Discrepancies between reviewers after full-text screening were resolved via consensus or discussion with a third reviewer for final inclusion.
Data extraction
We extracted the criteria used for clearance to RTS and general demographic and surgical data (table 1). Data elements were extracted to a custom Excel spreadsheet by one reviewer and verified by a second independent reviewer. Disagreements were resolved via consensus or discussion with a third reviewer. For the majority of studies, RTS criteria were not the main focus of the study. Therefore, RTS criteria were most commonly reported in the methods section. In studies where RTS criteria were the main focus of the study, criteria were reported in the results section.
Variables extracted for this scoping review
Data management
Demographic data were summarised as frequencies, or arithmetic mean and SD or median and IQR, as appropriate (Microsoft Excel, Microsoft Corporation, Santa Rosa, California). After data extraction, we used consensus to identify six main RTS criteria categories based on consensus of the logical grouping of criteria: time, strength, hop testing, patient-report, clinical examination and performance-based criteria (table 2). We further classified these categories (and associated RTS criteria)—reflecting the ICF17—as impairment, activity, participation, contextual and time criteria (table 2). RTS criteria were summarised as frequencies and presented in summary tables. To summarise time trends in RTS criteria, criteria were binned by year of study publication 1986 to 2017 and presented as a relative proportion of the total criteria reported in each year.
Return to sport criteria categorisation and associated International Classification of Functioning, Disability and Health (ICF)17 framework classification
Results
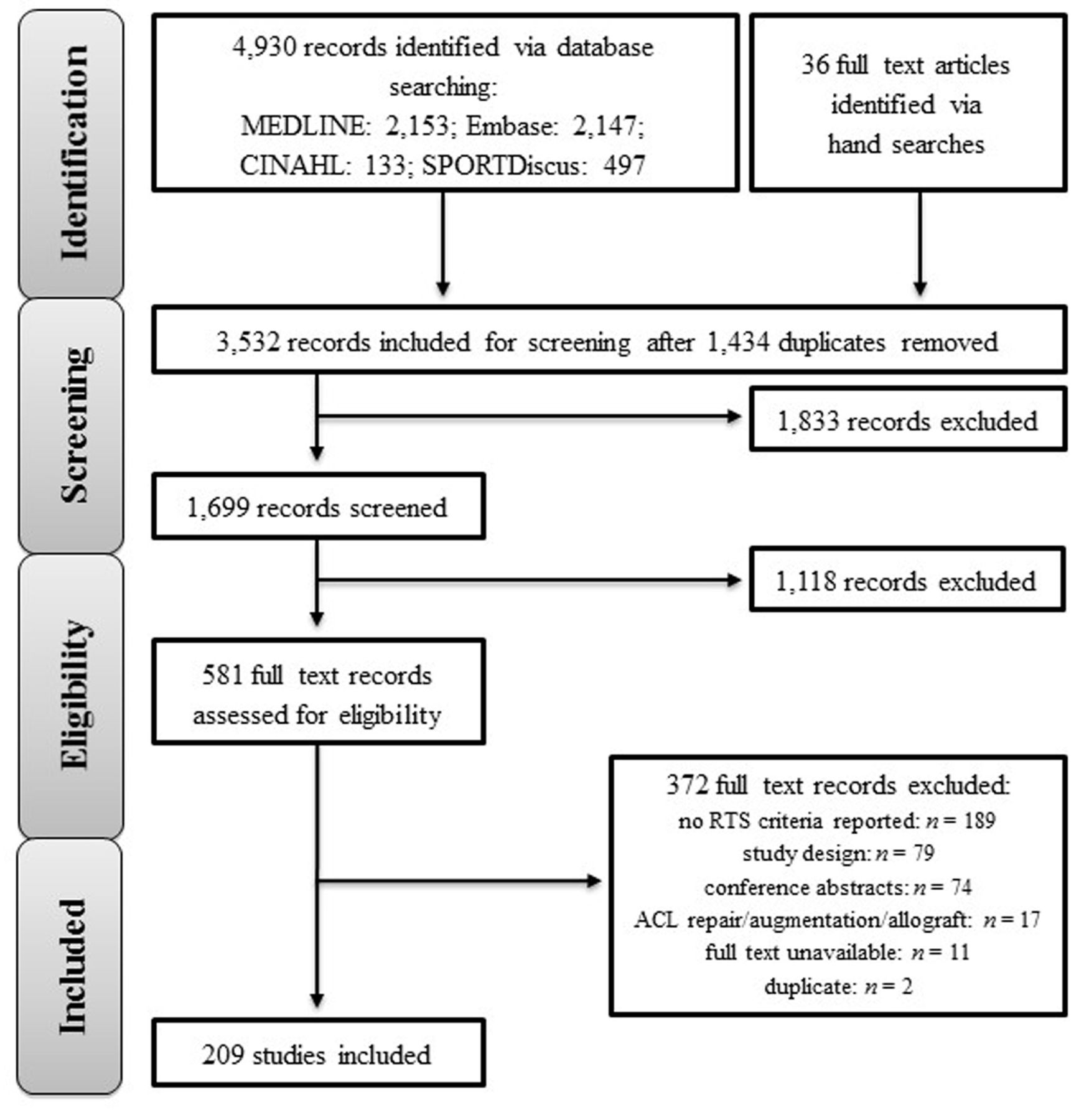
The electronic database search yielded 4930 records. We included 209 for qualitative review after title, abstract and full-text review (figure 1). Studies that were excluded after full-text review are reported in online appendix II.
Supplemental material

Study search flow diagram. RTS, return to sport.
Participants
This scoping review summarises the results of RTS testing of over 22 000 participants with primary ACL reconstruction. Approximately two-thirds of participants were men, and the mean time to RTS was 7.6 months (table 3).
Demographic characteristics of included studies
RTS criteria after ACL reconstruction
The previous review of RTS criteria11 included 159 studies reporting RTS criteria, and due to minor differences in selection criteria, 113 were eligible for inclusion in our scoping review. There were 96 articles published since the 2011 review11 that were eligible for inclusion in our scoping review.
Time
Time to RTS was reported as a criterion in 178 of the 209 included studies (85%) (table 4). Time was the sole criterion used to clear athletes to RTS in 88 studies (42%). Thirty-one studies (15%) did not use time as a RTS criterion. Eighteen studies (8%) reported a time frame for RTS clearance; seven studies18–24 (3%) reported a range (eg, RTS at 6–12 months) and 11 studies24–34 (5%) reported different RTS times based on type of sport (eg, non-contact at 4 months and contact at 6 months).
Time as a RTS criterion
Supplemental material
Strength tests (impairment measures)
Of the 209 included studies, 86 (41%) included strength as a RTS criterion (table 5). Two studies35 36 (1%) used isokinetic and isometric testing measures. Forty per cent of the 50 studies that used isokinetic strength as part of RTS criteria required a LSI of at least 85% for clearance to RTS.
Strength as a RTS criterion
Hop tests (activity measures)
From the 209 included studies, 30 (14%) reported using at least one hop test as a RTS criterion (table 6). Of these 30 studies, 22 (73%) required a LSI of at least 85% for clearance to RTS.
Hop performance as a RTS criterion
Patient-report (contextual factors)
Patient-report criteria were used in 26 (12%) of the 209 studies and included the subcategories patient-reported outcome measures (PROMs), subjective statements and reports of pain (table 7). Six studies37–42 (3%) used one outcome measure, and two studies43 44 (1%) used two measures. One study45 reported pain and subjective reports as RTS criteria and one study40 used PROMs and subjective statements as RTS criteria.
Additional measures used as criteria for clearance to return to sport
Clinical examination (impairment measures)
Fifty-four studies (26%) reported completing a clinical examination as part of RTS testing (table 7). Tests of ligament stability, range of motion, effusion and thigh circumference were included as part of different clinical examinations.
Thigh circumference
Thigh circumference was reported in three studies (1%) with defined criteria of ≤1 cm46 ,47 or ≤2 cm.48
Ligamentous stability
Twenty-five studies (6%) used at least one laxity test (table 7). Two studies48 49 defined a criterion of <3 mm side-to-side difference for clearance to RTS.
Range of motion (ROM)
Thirty studies (14%) used knee ROM as a RTS criterion (table 7). Nine studies48 50–57 required full range of flexion and extension, and four studies31 32 58 59 required only full extension. ‘Full ROM’ was not consistently defined. One study52 examined active and passive range of motion, and two studies57 60 examined passive range of motion only.
Performance-based criteria (impairment, activity and participation measures)
From the 209 included studies, 41 (20%) used performance-based criteria (tests of agility, proprioception, aerobic endurance, quality of motion, reported completion of a specific programme and non-specific performance-based criteria) to clear athletes to RTS (table 7). The 28 studies (13%) requiring completion of a specific programme as part of RTS criteria did not provide specific details regarding what the programme entailed.
Time trends in RTS criteria
Time was the sole criterion used to clear athletes to RTS in studies published between 1986 and 1989 (figure 2). Since 1990, time has represented approximately 50% of the total RTS criteria reported in published research (figure 2). Measures of impairments (ie, strength and clinical examination) represented approximately 30% of the total RTS criteria reported in published research (figure 2). Measures of performance-based criteria represented approximately 10% of the total RTS criteria reported in published research (figure 2).

Relative proportion of return to sport criteria reported in a given year.
Discussion
This review provides a compendium of tests that might be a helpful starting point for the practitioner and athlete planning RTS. The 209 included studies reported criteria that covered each of the ICF domains, although time and impairment measures were the most frequently reported criteria (figure 3). Measures of participation were rarely reported (figure 3). For the researcher, the results of our scoping review highlight the limited assessment of the participation and contextual elements of the ICF (figure 3). These parameters are relevant for at least two reasons: (1) participation is what athletes typically care most about, and (2) the call for RTS testing to focus on replicating the key physical, physiological and psychological demands of the athlete’s sport.9

Return to sport criteria mapped to the ICF domains. The relative size of the footballs represents how frequently different classifications of RTS criteria are reported in published studies.
Finding a balance between respecting biology and increasing load
Time was the most frequently reported criterion for RTS—85% of the studies included in our scoping review reported time as a RTS criterion. In two out of every five studies in our scoping review, athletes were cleared to RTS solely on the basis of time since ACL reconstruction. In over 90% of studies that used time as a RTS criterion, athletes were cleared to RTS within nine postoperative months.
Current guidelines for rehabilitation and RTS following ACL reconstruction include time among other criteria.3 The days of rehabilitation and RTS progressions solely governed by time (eg, at 3 months the athlete starts running, at 5 months the athlete starts training and at 6 months the athlete starts unrestricted sport) should be long behind us.62 However, tempering aggressive rehabilitation and RTS progression40 63 to account for biology—healing of the ACL graft and recovery of neuromuscular function—is important because of the link between time since surgery and knee reinjury risk.64 Criterion-based rehabilitation and RTS progressions should be evaluated with appropriate tests of impairments, activities, participation and contextual factors and combined with a minimum 9-month time criterion.3 64
Greater focus on the athlete and the sport
The dominance of measures of impairment (in comparison with measures of activity, participation and contextual factors) might reflect that impairment-based measures (eg, static knee laxity and strength) often require limited (or relatively easily accessible) equipment and space. They may also be easier to standardise than other types of tests. In contrast, assessing movement quality or other performance-based tests may require more complex equipment (eg, high definition video set-up), large amounts of space (eg, a football pitch) and can be more difficult to standardise.65 However, there is a problem: if we only test impairments, we lack information about the athlete’s capacity to cope with all of the physical and mental demands of playing sport. Measures of impairments are also poorly related to participation.66 The validity and responsiveness of higher level assessments, such as performance-based measures, also has limitations and requires further clarification.65
Over 75% of studies examining strength and/or hop testing used an LSI cut-off to determine pass or fail. Recently, there has been a call for caution when interpreting LSI,5 6 67 68 especially in the absence of an accurate baseline measure. Presurgical strength measurements of the uninvolved limb have been advocated5 as a basis for a more accurate LSI due to deterioration in the strength of the uninvolved limb following surgery.69 Biomechanical injury risk factors may also be present, despite limb symmetry.6 70 Therefore, the relevance and applicability of LSI to RTS testing requires further clarification. The practitioner working in the team environment may have the luxury of access to preinjury or presurgery screening data, which can help overcome the need to rely on LSI. For the practitioner without access to a trustworthy baseline evaluation of the uninjured limb, LSI remains an acceptable measure, provided you are cognisant of its limitations.68
Helping practitioners contribute effectively to shared RTS decisions
Contributing effectively to shared RTS decisions relies on the practitioner’s knowledge of the health of the athlete’s injured tissue or body part, the stress that the injured tissue or body part needs to be able to withstand and the context of sports participation.7–9 Tests of body structure (ie, impairments, including effusion and quadriceps strength) can provide information about tissue health. Tests of activities that resemble the basic demands of sports performance (eg, hopping and agility) can provide information about the capacity of the injured tissue or body part to withstand stress. Tests of participation (eg, pitch-based programme) provide more relevant, sport-specific information regarding tissue stress.
Understanding the demands of the sport is also a key source of information regarding how much stress is exerted on the body during sport.7 8 Understanding the demands of the athlete’s sport is vital, and an area that coaches—who are the experts in the technical and tactical demands of the sport—might help with.
Understanding the context of sports participation (including the importance of the match and coach pressure) provides information to guide the practitioner and athlete when deciding on their shared risk tolerance. There is always some risk associated with returning to and participating in sport. Effective RTS planning involves managing risk—balancing the sometimes competing tensions of performance and reinjury prevention.71 Tests of psychological readiness to return to sport, reinjury anxiety or performance anxiety might provide insight into the context of sports participation from the athlete’s perspective. Only one study included in our scoping review used a validated measure to assess psychological readiness.43 Given that psychological factors can influence RTS,72 these might be important factors to assess with respect to RTS.
Is research guiding practice in RTS?
How do the RTS tests reported in research stack up against the sort of information that practitioners and athletes need to help them make high-quality RTS decisions?7–9 In our scoping review, impairment-based tests of body structure were the most frequently reported group of tests (half of all studies). Twenty-six per cent of studies used activity-based tests (hop tests were the most common). Ten per cent of studies assessed personal or contextual factors including confidence and self-reported knee function. Fewer than 5% of studies used participation-based tests. These results suggest that often researchers may not be providing athletes and practitioners with sufficient information to make an informed RTS decision in practice.73
How researchers can help practitioners
Validity (how sure we are that the test is measuring what it is supposed to be measuring) is an important aspect to consider when measuring outcomes, both in research and in practice. Take movement quality as an example—validity governs the extent to which we can be sure that our observation of knee position in the frontal plane (ie, the knee varus/valgus position) is an accurate measure of neuromuscular function.
The RTS predictive validity (ie, does the result on the test predict the outcome) of many RTS tests is unknown. There is preliminary evidence of RTS predictive validity for psychological readiness to return to sport, low fear of reinjury, symmetrical hop performance and ‘normal’ knee function.74 75 This means that for most RTS tests, we do not know whether passing the test means the athlete will RTS. Therefore, establishing the RTS predictive validity of RTS tests should be a priority for future research.
Research is especially needed to underpin the development of accurate, sport-specific, practically relevant and cost-effective tests of participation for athletes after ACL injury. Capitalising on new technologies such as augmented or virtual reality might also be a worthwhile avenue for future research as a way of realistically replicating some of the context of sports participation without excessive space or personnel requirements.
How practitioners can help athletes
The multifactorial nature of RTS suggests that a group of tests measuring athlete-centred constructs, rather than a single test in isolation, can provide an important basis for practitioners and athletes when planning RTS. Clearly, one test will not provide enough information and, for this reason, should not be the sole deciding factor in an RTS risk assessment.7 The 2016 consensus on RTS9 outlines five recommendations to guide the choice of RTS tests:
Use a group of tests (test battery).
Choose open tasks (less controlled) over closed tasks (more controlled) where possible.
Include tests with reactive decision-making elements.
Assess psychological readiness to return to sport.
Monitor internal and external workload.
Our scoping review indicates that published research on RTS often does not mirror the 2016 consensus statement. One explanation is that 95% of the studies in our scoping review were published prior to the most recent consensus on RTS, which outlines these recommendations. Therefore, in future research, we may begin to see a shift in the RTS criteria reported. Appropriate RTS tests of impairments, activities, participation and contextual factors, combined with a minimum 9-month time criterion,3 64 are worthy of further investigation. In at least one recent study, a movement quality test (Landing Error Scoring System) was used as part of a RTS test battery along with the International Knee Documentation Committee subjective knee form and the ACL-Return to Sport after Injury scale.42
All of the studies included in our scoping review were focused on the RTS element of the RTS continuum (figure 4).9 However, for many athletes, return to performance—the third element of the RTS continuum—is their primary focus. The RTS continuum illustrates that there are at least two key transitions for athletes following injury: return to playing their sport and return to performing at the desired level in their sport. Research on athlete performance following ACL reconstruction is limited and has focused on match statistics.76 However, match statistics may not provide adequate information on load, physiological capacity or psychological aspects of performance.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The three elements of the RTS continuum.
Limitations
There are limitations to our scoping review, with implications for athletes, practitioners and researchers:
We reported tests that have been used in published research. Other innovative and potentially useful tests may be used in practice but not reflected here.77
It is unclear whether passing RTS tests predicts whether an athlete will return to sport participation or the previous level of sport participation after ACL reconstruction.
It was beyond the scope of this review to assess the predictive validity of RTS tests for safe RTS following ACL reconstruction. For many of these tests, we cannot draw conclusions regarding whether the RTS tests were associated with a reduced risk of new knee injury on resuming participation in sport.
To be included in our review, studies had to be published in English and peer reviewed, representing a possible publication bias, as well as the possibility that these limitations may have excluded other relevant tests and data. We excluded studies where participants received an allograft for their ACL reconstruction to avoid graft type as a confounding variable and studies of participants with revision surgery. Therefore, the results of our scoping review may not be generalisable to athletes with allograft or revision ACL reconstruction. We accepted the definition of ‘athlete’ as it was used in an individual study. Therefore, it is possible that different studies defined athlete in different ways, and different RTS tests may be used in different athlete populations. We did not extract data in duplicate. However, a second person independently verified the extracted data. In most studies, it was unclear how the RTS tests were conducted (ie, which practitioner(s) administered the tests and made judgements about clearance to RTS). It is possible that practitioners with different education and training backgrounds might prioritise different RTS criteria and contribute different information to the shared RTS decision-making process.
Conclusion
Eighty-five per cent of studies used time as a RTS criterion after ACL reconstruction. Measures of participation and contextual factors were uncommonly reported as RTS criteria after ACL reconstruction. Strength (41% of studies), physical performance-based criteria (20% of studies) and patient-report criteria (12% of studies) were infrequently used as RTS criteria.
What is already known
In the decade leading up to 2011, few objective functional criteria were used to clear athletes to return to sport (RTS) after ACL reconstruction.
Sport has physical and psychological demands that must be considered when planning RTS.
What are the new findings
Time continues to be the primary criterion used to clear athletes to RTS after ACL reconstruction.
Strength (41% of studies), physical performance-based criteria (20% of studies) and patient-report criteria (12% of studies) were infrequently used as RTS after ACL reconstruction.
Despite the initiation of the International Classification of Functioning, Disability and Health model in 2002 with the goals of assessment at the individual, social and policy level, RTS testing after ACL reconstruction was primarily limited to assessment of time and impairments.
Acknowledgments
The authors would like to thank Leila Ledbetter, MLIS, for assisting with the literature search for this study.
References
Footnotes
Contributors CRB contributed to initial search, data extraction, initial drafting, review and editing of the manuscript. SP contributed to initial search, data extraction, initial drafting, review and editing of the manuscript. CLA contributed to initial drafting, review and editing of manuscript. JRM contributed to initial search, data extraction and review of manuscript. CDG and JS contributed to data extraction and review of manuscript. MPR contributed the idea of the manuscript, initial search, review of data, initial drafting, review and editing of the manuscript. All authors approved of final version of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data available upon request.