Article Text

Abstract
Background Evidence on the role of very low or very high volumes of leisure time physical activity (PA) on the risk of all-cause and cause-specific mortality is limited. We aimed to examine the associations of different levels of leisure time PA with the risk of all-cause, cardiovascular disease (CVD) and cancer-specific mortality.
Methods Data were from 12 waves of the National Health Interview Surveys (1997–2008) linked to the National Death Index records through 31 December 2011. A total of 88 140 eligible participants aged 40–85 years were included.
Results Compared with inactive individuals, those performing 10–59 min/week of PA had 18% lower risk of all-cause mortality (hazard ratio (HR): 0.82, 95% confidence interval (CI): 0.72–0.95). Those who reported 1–2 times (150–299 min/week) the recommended level of leisure time PA had 31% (HR: 0.69, 95%CI: 0.63–0.75) reduced risk of all-cause mortality. Importantly, the continued benefits were observed among those performing leisure time PA 10 or more times (≥1500 min/week) the recommended minimum level (HR: 0.54, 95% CI: 0.45–0.64). For 10–59, 150–299 and ≥1500 min/week of PA, the corresponding HRs (95% CIs) for CVD-specific mortality were 0.88 (0.67–1.17), 0.63 (0.52–0.78) and 0.67 (0.45–0.99), respectively: for cancer-specific mortality were 0.86 (0.66–1.11), 0.76 (0.64–0.89) and 0.53 (0.39–0.73), respectively. In addition, there was a larger reduction in all-cause and cause-specific mortality for vigorous vs. moderate intensity PA.
Conclusions We found that beneficial association between leisure time PA and mortality starts from a low dose. Doing more vigorous exercise could lead to additional health benefits.
- physical activity
- cardiology
- death
- cohort study
Statistics from Altmetric.com
Introduction
It is well established that physical activity (PA) is associated with a reduced risk of cardiovascular disease (CVD), cancer, type 2 diabetes mellitus and mortality.1–3 In 2008, the United States (US) and World Health Organization (WHO) guidelines on PA recommended a minimum of 150 min/week of moderate-intensity aerobic PA (eg, brisk walking) or 75 min/week of vigorous-intensity aerobic PA (eg, running) or an equivalent combination of both.4 5 However, less than half of US adults have met this recommendation in 2015.6
Several studies have confirmed that a low dose of exercise is beneficial for reducing the risk of mortality.7–10 A recent meta-analysis demonstrated that a low dose of moderate-to-vigorous leisure time PA in older adults, which was less than the recommended minimum by the PA guidelines,4 5 was associated with a 22% lower risk in mortality.8 Another study that included data from six cohorts of 6 61 137 middle-aged and older adults reported similar findings.9 In addition, a study conducted in Taiwan demonstrated that moderate exercise of around 15 min/day (or 90 min/week) reduced the risk of all-cause and CVD-specific mortality by 14% and 19%, respectively.7 Using primarily college-educated and non-Hispanic white adults, the Aerobic Center Longitudinal Study reported a reduced risk of all-cause and CVD mortality among participants who reported running at least 5–10 min/day compared with inactive participants.10
It is unclear, however, whether there is a potential harm resulting from excessive PA, defined as a greater number of hours of PA more than the recommended. Several studies evaluated this association but results were inconsistent. A common finding is a U- or a J-shaped association between PA levels and mortality risk,11–14 while others reported a protective effect with very high levels of PA.9 For instance, the Million Women Study11 and the Copenhagen City Heart Study14 reported increased risk of mortality or CVD events for strenuous PA, while the harmonised pooled analysis of six cohort studies found it progressively increasing, although at a modest rate, health benefits with PA up to 10 times the minimum recommended amounts by the PA guidelines.9
In the current study, using a nationally representative sample of US adults, we aimed to assess the association between levels of leisure time PA and risks of mortality from all causes, CVD and cancer. In addition, we investigated the risk of mortality associated with very low or very high levels of leisure time PA.
Methods
Study population
We used the data from 3 66 376 study participants aged 18–85 years who participated in 13 cross-sectional waves of the National Health Interview Surveys (NHIS) during 1997–2009. The NHIS is an ongoing national cross-sectional survey administered by the National Center for Health Statistics of the Centers for Disease Control and Prevention (CDC) to monitor the health of the civilian noninstitutionalized US population.15 It uses a stratified, multistage sampling design to collect information on health and lifestyle behaviours from sample participants representative of the general US population using personal household interviews. Major revisions to the survey questionnaires of the NHIS took place in 1982 and 1997, thus we used the data starting from 1997 through 2009 to ensure consistency in participants’ responses.
Data on the baseline of the NHIS were linked to mortality data in 2011. Among the 3 66 376 participants, 2 78 236 were excluded because of <3 years of follow-up duration (n=27 384 in 2009), aged <40 years (n=1 34 777), the presence of chronic disease (n=1 08 343), missing information on study exposure, i.e., PA (n=3240), missing information on covariates (n=4360) or the presence of pregnancy (n=132), resulting in a final analytical sample of 88 140 US adults aged 40–85 years.
Study outcome
The study outcome was mortality during the follow-up period. Using the International Classification of Diseases – 10th Revision (ICD-10) codes, the mortality-specific outcomes included CVD-specific mortality (codes I00–I09, I11, I13, and I20–I51, I60–I69) and cancer-specific mortality (codes C00–C97). Eligible study participants were linked to the National Death Index (NDI) records through 31 December 2011 to determine their mortality status,16 similar to previous studies.17 18 Previous studies have identified that the NDI records matching algorithm yielded a good agreement (98.5%), with 96.1% of decedents being correctly classified as deceased and 99.4% of non-decedents being correctly classified as alive.19 20
Study exposure
The primary study exposure was leisure time PA defined by frequency and duration of PA for the study participants. All study participants were asked two sets of questions that assessed the frequency and duration of leisure time PA. Frequency was assessed as PA for at least 10 min and categorised into: vigorous PA (eg, running, faster cycling and competitive sports, etc.) and light or moderate PA (eg, brisk walking, dancing and gardening, etc.). Using a combination of frequency (times/week) and duration of PA (minutes/time), we defined leisure time PA as measured in minutes/week units. We used minutes/week instead of metabolic equivalent value (MET) for easier translation of our findings. PA guidelines defined 1 min of vigorous-intensity activity as equivalent to 2 min of moderate-intensity activity,4 5 therefore we calculated the total PA level (minutes/week) for each study participant by converting vigorous-intensity PA into the equivalent moderate-intensity PA. The main study exposure, total leisure time PA, has been categorised into eight groups: 0, 10–59, 60–149, 150–299, 300–449, 450–799, 800–1499 and ≥1500 minutes/week, similar to earlier studies.9
We carried out a sensitivity analysis where we defined 1 min of vigorous-intensity activity as equivalent to 1 min of moderate-intensity activity, and the overall results were found to be similar (data not shown). In addition, two types of PA intensity (light-to-moderate or vigorous intensity) were categorised into the following groups: 0, 10–59, 60–149, 150–299, 300–599 and ≥600 minutes/week, and their associations with the risk of all-cause, CVD- and cancer-specific mortality were estimated.
Covariates
The study covariates included study participants’ demographic characteristics and lifestyle behaviours. Demographic variables included sex, age, race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic and other), education level (<high school, high school and >high school) and marital status (married, divorced/separated/widowed, never married). Lifestyle behaviours included body mass index (categorised into underweight, normal weight, overweight and obese), smoking status (never, former and current smokers), and drinking status (lifetime abstainer, former drinker, current light to moderate drinker and current heavy drinker).21
Statistical analysis
Participants’ baseline characteristics according to eight leisure time PA categories (0, 10–59, 60–149, 150–299, 300–449, 450–799, 800–1499 and ≥1500 min/week)9 were presented using proportions for categorical variables. A multivariable Cox proportional hazards regression model was used to estimate the risk of all-cause and cause-specific mortality with level of total leisure time PA, adjusting for potential confounding factors including demographic factors and lifestyle behaviours. We used the Schoenfeld residual plots to examine the proportional hazards assumption and we noted no violations. To estimate the potential differences in confounding effects, we used three models for covariates adjustments. Model 1 included sex, age and race/ethnicity; Model 2 included variables in Model 1 plus education and marital status; and Model 3 included variables in Model 2 plus lifestyle variables. Hazards ratios (HRs) and 95% confidence intervals (CIs) were reported. To evaluate the dose-response relationship of total PA (as a continuous variable) with mortality risk, Cox models with penalised splines22 were used with R version 3.3.3. The output includes a graphic representation of the fitted splines and standard error bars, with log HR for mortality on the y-axis and total PA on the x-axis. In addition, the associations of the study outcomes with two PA intensity categories (light-to-moderate and vigorous PA) were also evaluated. Additionally, the association of leisure time PA with the risk of all-cause mortality was also assessed by survey year. The heterogeneity of the study participants’ responses between survey cycles was tested by Cochran’s Q test in meta-analysis. Stratified analyses were conducted to assess whether the association of PA with all-cause mortality differed according to demographic and lifestyle variables. All data management and analyses were performed using SAS version 9.3 (SAS Institute Inc) and R-version 3.3.3. Two-sided P<0.05 was considered significant for statistical inferences.
Results
Overall, the study cohort included a total of 88 140 US adults aged 40–85 years at baseline. Table 1 presents the descriptive characteristics of the study participants in the total study cohort and also between the eight categories of the study exposure (categories of PA levels).
Baseline characteristics according to total leisure time physical activity level, NHIS, 1997–2008
During a median follow-up of 9.0 years, there were 7855 all-cause deaths, 1 695 CVD-specific deaths and 2269 cancer-specific deaths. As shown in table 2, when adjusted for all study covariates, participants performing 10–59 min/week of leisure time PA had 18% lower risk of all-cause mortality (HR=0.82, 95% CI=0.72–0.95) than physically inactive ones. Similar estimates were found among those who reported 60–149 min/week of leisure time PA (HR=0.78, 95% CI=0.72–0.86). Those who reported 1–2 times (150–299 min/week) or 2–3 times (300–449 min/week) the recommended level of leisure time PA had 31% (HR=0.69, 95% CI=0.63–0.75) and 33% (HR=0.67, 95% CI=0.61–0.74) lower risk of all-cause mortality, respectively. Similar benefits were found for PA levels at 3–5 times (450–799 min/week: HR=0.58, 95% CI=0.52–0.66), at 5–10 times (800–1499 min/week: HR=0.63, 95% CI=0.56–0.72), and at 10 or more times (≥1500 min/week) the recommended minimum by the PA guidelines (HR=0.54, 95% CI=0.45–0.64).
Association between total leisure time physical activity level and risk of all-cause and cause-specific mortality
Similar protective effects on CVD-specific and cancer-specific mortality were also observed across different leisure time PA categories (table 2). The HRs and 95% CIs for CVD-specific mortality for 10–59, 60–149, 150–299, 300–449, 450–799, 800–1499 and ≥1500 minutes/week leisure time PA were 0.88 (0.67–1.17), 0.76 (0.63–0.92), 0.63 (0.52–0.78), 0.64 (0.49–0.82), 0.64 (0.49–0.83), 0.74 (0.57–0.97) and 0.67 (0.45–0.99), respectively. The corresponding HRs and 95% CIs for cancer-specific mortality were 0.86 (0.66–1.11), 0.84 (0.72–0.98), 0.76 (0.64–0.89), 0.85 (0.71–0.99), 0.71 (0.59–0.86), 0.65 (0.51–0.83) and 0.53 (0.39–0.73), respectively.
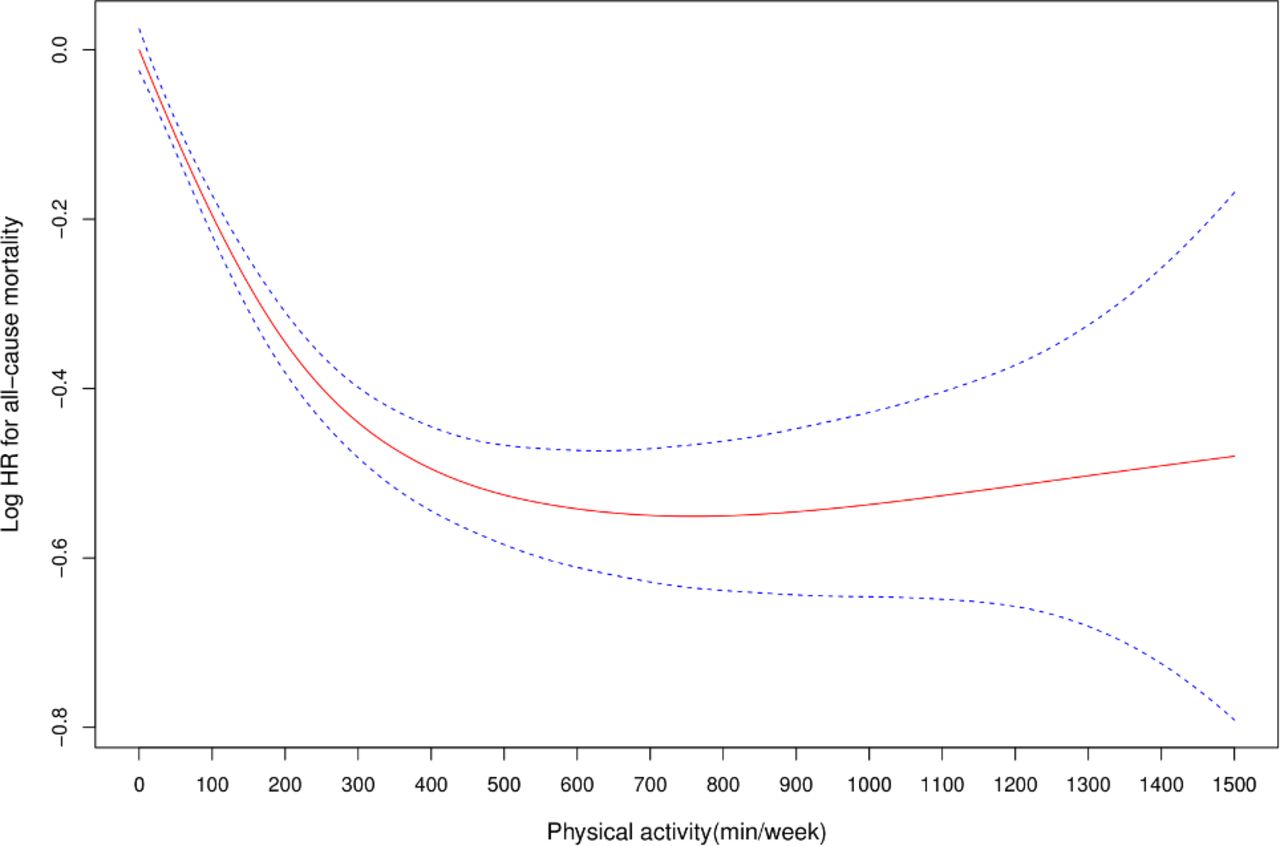
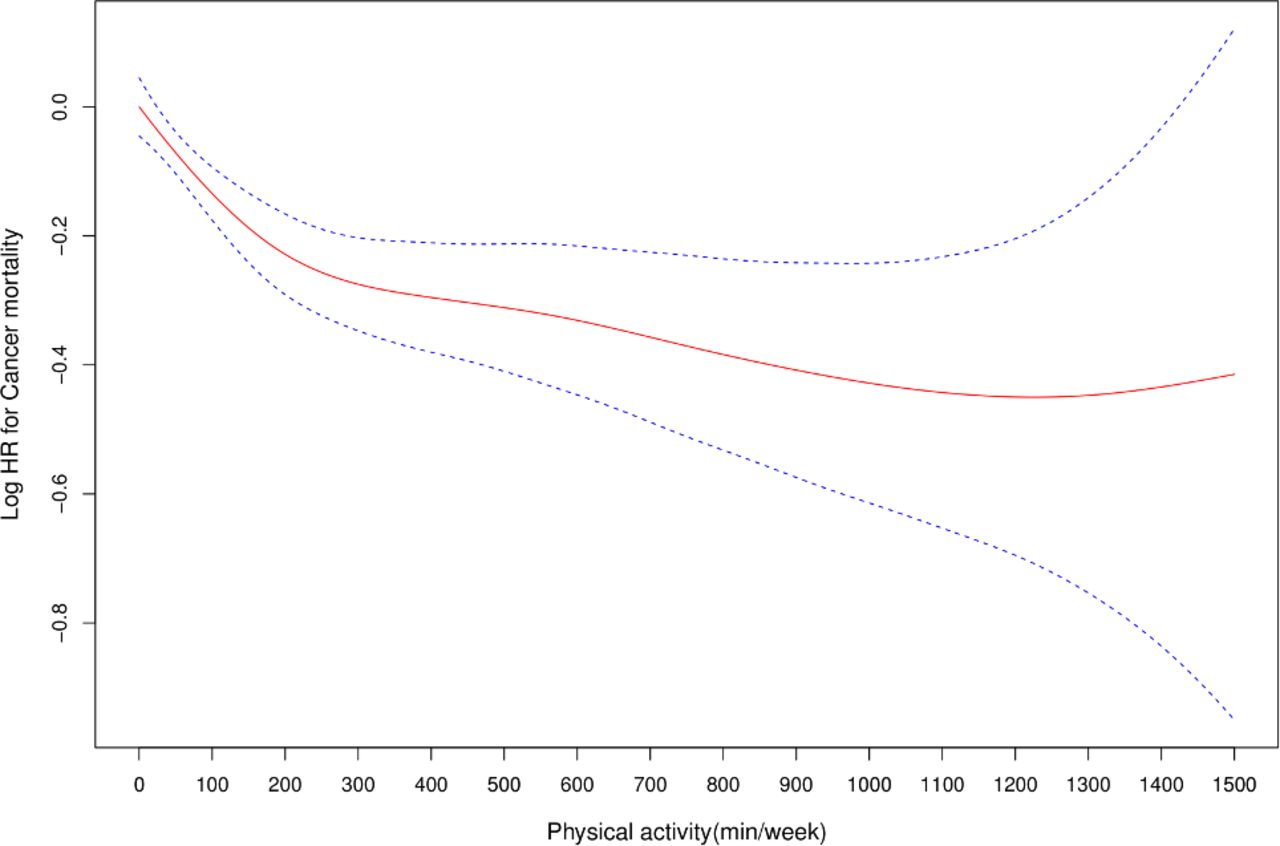
The Cox models with penalised splines showed that there was a curvilinear relationship between total leisure time PA (as a continuous variable) and risk of all-cause mortality (P for nonlinearity <0.001, figure 1), CVD-specific mortality (P for nonlinearity <0.001, figure 2) and cancer-specific mortality (P for nonlinearity <0.001, figure 3). Compared with physical inactivity, the protective effect of PA on all-cause mortality started at a low dose and became stronger with an increasing dose up to the level of more than 10 times of the recommended PA. In addition, the dose-response association of leisure time PA with cancer-specific mortality was more apparent compared with the association with CVD-specific mortality, especially at high PA levels (figures 2 and 3).

Dose-response association between total leisure time physical activity (as a continuous variable, min/week) and risk of all-cause mortality.
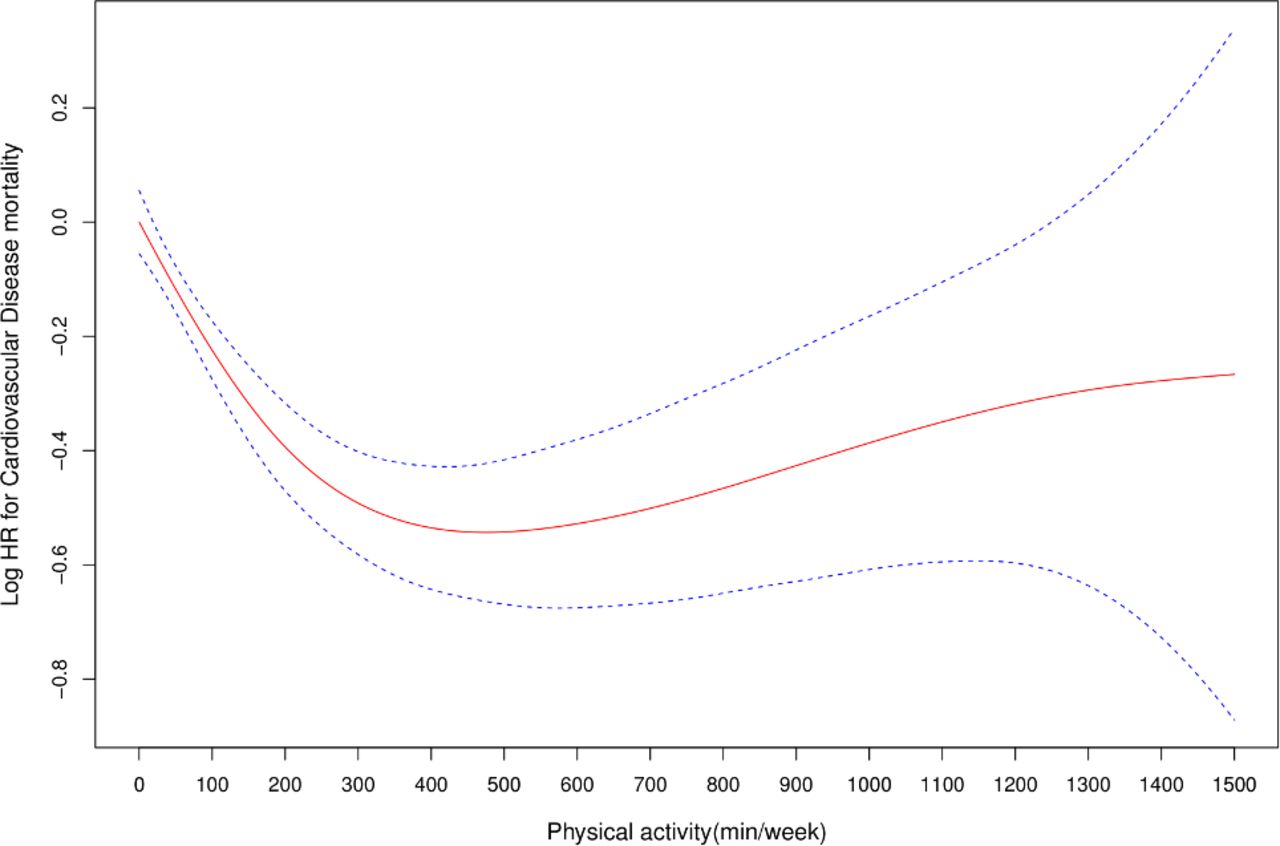
Dose-response association between total leisure time physical activity (as a continuous variable, min/week) and risk of CVD- specific mortality.

{kind=link}
{kind=link}
{kind=link}
Dose-response association between total leisure time physical activity (as a continuous variable, min/week) and risk of cancer-specific mortality.
We examined the association between leisure time PA and the risk of all-cause mortality stratified by survey year and found results similar with those of the pooled data. In addition, we found no statistically significant difference in heterogeneity in the associations across the survey years, which allowed us to combine all data in this study (online supplementary table S1).
Supplementary file 1
Table 3 presents the association of leisure time PA with all-cause and cause-specific mortality risks in the two PA intensity categories. Low levels (10–59 min/week) of either light-to-moderate or vigorous intensity PA were associated with reduced risk of all-cause mortality. In addition, higher levels (≥600 min/week) of both PA intensities were found to be associated with a lower risk of all-cause and cancer-specific mortality, respectively.
Association between leisure time physical activity level and the risk of all-cause and cause-specific mortality by intensity of activity
In stratified analyses, we found the same direction of associations regardless of demographic factors and lifestyle variables, although variations in estimates were noticed (online supplementary table S2). The associations were more significant in the older group than in the middle-aged group, in women than in men, and in never or ever smokers than in current smokers.
Discussion
Using a nationally representative sample of US adults, our study suggested that individuals with 10–59 min/week of light-to-moderate PA had significant health benefits compared with physically inactive adults. Individuals with high levels of PA could achieve further health benefits. Importantly, very high levels of PA (10 or more times than the recommended minimum by the PA guidelines) continued to have health benefits against mortality risk.
Currently, about 51% US adults fail to meet the recommendation for PA.6 Very low levels of PA, such as about 5–10 min/day may be easy to achieve by most adults; thus, it is important to determine whether PA at such a level is beneficial. To date, only two large studies have been conducted to determine the precise minimum level of leisure time PA that is beneficial.7 10 Both studies suggested 5–10 min/day (30–59 min/week) running10 or 15 min/day (90 min/week) moderate-intensity exercise7 to reduce the risk of all-cause and cause-specific mortality. Similar to these two studies, our study findings suggest that leisure time PA for 10–59 min/week may have a beneficial effect on all-cause mortality.
There have been contradictory findings on the association between very high leisure time PA levels and mortality risk.9 11 14 Several studies reported harmful effects with very high leisure time PA levels,11 14 while others,9 including ours, suggested beneficial effect. Two mini reviews by Eijsvogels et al23 24 stated that the disappearance of health benefits of PA at a high dose in the two previous studies11 14 might be subjected to methodological limitations. In the Million Women Study, individuals who performed daily strenuous PA had an increased risk of cerebrovascular disease and venous thromboembolism when compared with inactive study participants. However, the baseline characteristics of two subgroups were not comparable and this finding might be misleading.11 In the Copenhagen Study, the mortality rate was higher in high intensity joggers (>3 times/week for >4 hours at a fast pace) than non-joggers. However, the sample of high-intensity joggers was very small (n=36).14 Our study using a nationally representative sample of US adults had sufficient sample size for the very high PA category (141 deaths occurred in 2500 participants), thereby supporting the beneficial effect of very high levels of PA on mortality risk. Our findings, however, were based on samples from a general healthy population, and may not be generalisable to high-risk patients.25 In addition, we also found participants who performed more than 1500 minutes/week leisure time PA were more likely to be young white men with higher education level. Indeed, this highest level of leisure time PA is difficult to achieve for a working adult.
We also found significantly lower risk of all-cause and cause-specific mortality among individuals who do vigorous PA compared with those who only do light/moderate PA, and these results were consistent with previous studies.7–10 Because of the higher exertion involved, participation in vigorous-intensity activity is more time-efficient than moderate-intensity activity.7 Thus, vigorous-intensity PA may be an attractive option for able-bodied individuals with limited time.
Our finding on the protective effects of leisure time PA on cause-specific mortality is consistent with previous studies.10 26–28 It is well established that PA improves fitness and physical function.29 A systematic review of intervention studies indicated that physical exercises such as running and playing football improved metabolic fitness, muscular performance and cardiac function, and were beneficial for weight loss,30 which may help explain why PA decreased the risk of CVD mortality. The protective effects of PA on cancer mortality have also been widely established in previous studies.26 28 The protective effects of PA against cancer risk may be mediated by reductions in body weight, circulating sex hormones and inflammation, and improved immune functions.31 Thus, our study findings emphasise the importance of PA in the prevention of CVD and cancer deaths.
There have been several publications on associations between accelerometer measured PA and the risk of mortality.32–35 Data from the 2003–2006 National Health and Nutrition Examination Survey reported that both self-reported and accelerometer-assessed moderate-to-vigorous PA were associated with the risk of all-cause and CVD-specific mortality.32 Other studies also demonstrated that all intensities of objectively measured PA were beneficially associated with all-cause and cause-specific mortality.33–35 The study exposure measurement in our study is subjective, however findings were similar to those from studies with PA objectively measured.
The 2018 Physical Activity Guidelines for Americans has become available recently.36 The guidelines concludes that PA reduces the risk of morbidity and mortality, and there are various ways to achieve the benefits of PA. It also states that bouts, or episodes, of moderate-to-vigorous PA of any duration may have health benefits; further, higher intensity, longer duration and/or higher frequency will bring about greater health benefits. Overall, our study findings concur with the recommendations of the 2018 Guidelines.
Study strength and limitations
Our study has numerable strengths. First, we utilised data from samples representative of the general US middle- and old-age population with a relatively large sample size. Second, we addressed the possibility of reverse causation by excluding participants from all analyses who were followed within the first 3 years and who reported diagnosis with at least one chronic disease condition. Third, we conducted several sensitivity analyses to investigate the association in different sub-populations. Our study also has several limitations. First, information on study exposure and most covariates was obtained through participants’ self-reported responses, which might be subject to recall bias. Second, data on participants’ PA were not available during the follow-up period. Repeated evaluations of PA, rather than a one-time evaluation, could likely improve the robustness of PA effect sizes. Third, although we adjusted for many confounders at baseline, several unmeasured confounders such as dietary intakes or disabilities have not been captured. Future epidemiological studies will benefit from collecting information on these unmeasured variables and test for the possible roles of confounding, interaction, mediation in the causal pathway between PA and mortality. Fourth, data on occupational, transport or other domains of PA were unavailable in the current study. Further studies should examine the impacts of other PA patterns on mortality risk. In addition, we had no data on sedentary behaviours which may modify the association between PA and mortality risk.37
Conclusions
Assuming causality of the associations we observed, both low and high levels of PA have beneficial effects on all-cause and cause-specific mortality risk. Importantly, vigorous PA has added benefits for reducing mortality compared with moderate PA. Promoting PA of any intensity and amount is an important approach to reducing mortality risk in the general population.
What are the findings?
Our cohort study suggested that a low dose of light to moderate-intensity physical activity was associated with lower risk of mortality: individuals doing more exercise could achieve additional health benefits. Of note, there was still benefit rather than excess risk associated with very high levels of leisure time physical activity.
How might it impact on clinical practice in the future?
Since the benefits of physical activity start at a low dose with additional benefits associated with high doses, clinicians should encourage patients to increase physical activity regardless of baseline levels.
Acknowledgments
We thank the National Center for Health Statistics of the Centers for Disease Control and Prevention for sharing the NHIS data. We thank Dr. Steven Moore for sharing the code for calculating covariate-adjusted survival curves that was adapted for this analysis.
References
Supplementary materials
Press release
Footnotes
Contributors BX and MZ designed the study, performed data analyses and had full access to all the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis. MZ drafted the manuscript. SPV, LMS and SL made critical revision of the manuscript for important intellectual content. All authors approved the final submitted version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.