Article Text

Abstract
Objective To assess whether physically active yoga is superior to waitlist control, treatment as usual and attention control in alleviating depressive symptoms in people with a diagnosed mental disorder recognised by the Diagnostic and Statistical Manual of Mental Disorders (DSM).
Design Systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Data sources Data were obtained from online databases (MEDLINE, EMBASE, PsychINFO, CENTRAL, EMCARE, PEDro). The search and collection of eligible studies was conducted up to 14 May 2019 (PROSPERO registration No CRD42018090441).
Eligibility criteria for selecting studies We included randomised controlled trials with a yoga intervention comprising ≥50% physical activity in adults with a recognised diagnosed mental disorder according to DSM-3, 4 or 5.
Results 19 studies were included in the review (1080 participants) and 13 studies were included in the meta-analysis (632 participants). Disorders of depression, post-traumatic stress, schizophrenia, anxiety, alcohol dependence and bipolar were included. Yoga showed greater reductions in depressive symptoms than waitlist, treatment as usual and attention control (standardised mean difference=0.41; 95% CI −0.65 to −0.17; p<0.001). Greater reductions in depressive symptoms were associated with higher frequency of yoga sessions per week (β=−0.44, p<0.01).
- exercise
- psychiatry
- review
- depression
Statistics from Altmetric.com
Introduction
Globally, mental disorders are responsible for 32.4% of disability adjusted life years (a year of 'healthy' life lost), placing mental disorders at a distant first in the global burden of disease in terms of years lived with disability.1 Depressive disorders, such as major depressive disorder, are the leading cause of disability worldwide, affecting more than 340 million people.2 They are predicted to be the second largest contributor to the global burden of disease by the year 2020.3 Depressive disorders are highly comorbid with other mental disorders, such as anxiety disorders4 and psychotic disorders.5 Physical comorbidities are also present in 65% of people with depressive disorders,6 commonly including obesity, type 2 diabetes, metabolic syndrome and cardiovascular disease.7 This is driven in part by modifiable lifestyle related risk factors, such as low levels of physical activity and high levels of sedentary behaviour.8 Physical inactivity is associated with higher levels of depressive symptoms in the general population9 and in those with major depressive disorder.10 There is a clear need for interventions which are efficacious in improving both physical activity and depressive symptoms11 12 and multicomponent lifestyle interventions incorporating a combination of physical activity, exercise and diet.13 14 Treatment guidelines for mental disorders from leading international organisations now recommend the integration of physical activity based interventions as part of routine psychiatric care.11 15–17 Despite these recommendations, translation of evidence into clinical practice and routine implementation of exercise interventions as part of standard care is limited.18
One form of exercise that is increasing in popularity in western culture, particularly among psychiatric patients,19 is yoga. Yoga is a multicomponent mind–body practice comprising physical postures, movement, breathing control and techniques, relaxation, mindfulness and meditation.20 Mindfulness, meditation and exercise are all effective in reducing depressive symptoms.21 22 Yoga practice often includes a combination of each and therefore may have additional benefits beyond a single component (eg, mindfulness, meditation or exercise alone). Furthermore, yoga has demonstrated efficacy in improving exercise adherence and may provide an alternative engagement strategy for people who do not want to engage in conventional forms of exercise.23
People living with mental disorders commonly experience depressive symptoms—for example, 25% of people diagnosed with schizophrenia and 81% of people diagnosed with generalised anxiety disorder also have depression.24 25 Several systematic reviews and meta-analyses have assessed a range of yoga interventions, using various styles of yoga, and have shown improvements in mental health across various mental disorders26 27 (see table 1). However, no previous review has investigated the transdiagnostic benefits of yoga. Earlier reviews that focused on yoga for people with depression reported positive effects but all conclude that findings must be interpreted with caution due to the heterogeneity of the yoga interventions and poor methodological reporting.28–30 This review differs from previous reviews as it includes a range of mental disorder diagnoses and considers the transdiagnostic potential for yoga across all mental disorder groups, thus allowing for a more comprehensive assessment of the potential benefits for depressive symptoms across the range of mental disorders.
Summary of previous literature reviews on yoga and mental disorders
Hence the primary aim of this review was to determine the effects of physically active yoga on depressive symptoms compared with control in people with any type of mental disorder. Additionally, the review examines the physical health outcomes of yoga interventions for people with mental disorders. We also sought to identify the key components of yoga based interventions that are associated with better outcomes.
Methods
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines31 and was prospectively registered with the PROSPERO database (ID: CRD42018090441).
Data sources and searches
The following sources were searched from database inception to 14 May 2019: MEDLINE (Ovid), EMBASE (Ovid), PsychINFO (Ovid), the Cochrane Central Register of Controlled Trials (CENTRAL), EMCARE (Ovid) and the Physiotherapy Evidence Database (PEDro). MeSH headings used were ‘mental disorders’ or ‘mental disease’ AND ‘yoga’, with all branches entered as keywords (Supplementary Table 1). Manual searches were conducted using the reference lists from recovered articles and relevant systematic reviews and meta-analyses.
Study selection/inclusion criteria
Participants
Studies of adults aged 18 years or older with a current Diagnostic and Statistical Manual of Mental Disorders (DSM)-3, 4 or 532 diagnosis of any mental disorder, including depressive disorders, anxiety disorders, affective disorders, trauma and stress related disorders, psychotic disorders, panic disorders and alcohol and substance use disorders were included. Participants with other clinical health conditions in addition to a mental disorder were not excluded.
Interventions
Yoga interventions were defined as a structured, formal and premeditated form of physical activity involving the integration of specific body movements (asana) with breathing (pranayama) and/or mindfulness (including meditation),27 29 where the movement component (physical activity) made up more than 50% of the total intervention.
Control conditions
Treatment as usual, waitlist or attention controls were included. Trials that compared one type of physical activity with another (eg, yoga vs aerobic exercise) without an adequate control group were excluded.33
Outcome measures
The primary outcome measure was change in depressive symptoms across all mental disorders (mean±SD), measured on validated scales, scored from baseline to post-intervention. Secondary outcomes of interest were exercise capacity (eg, measures of cardiorespiratory fitness and strength), biomarkers (eg, cortisol), quality of life, cognition, sleep, anthropometry (eg, body mass index, waist circumference), remission rates, attendance, dropout rates and adverse events.
Study design
Only randomised controlled trials (RCTs) were eligible.
Exclusion criteria
In the case of multiple publications from the same study, outcome measures were collated to create a ‘complete study’. Trials were not excluded because of nationality or clinical setting (inpatient, outpatient, community setting or mixed). Studies not available in English were excluded.
Data extraction
After removal of duplicates, two researchers (JB and OL) independently screened titles and abstracts using Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). Both authors applied eligibility criteria, and a final list of included articles was developed through consensus. A third reviewer (SR) was available for mediation throughout this process.
Data were extracted from the included articles using a predetermined data extraction form by two authors (JB and DG) and cross-checked for accuracy by a third author (OL). The data extracted included participant and trial characteristics (diagnosis, type of yoga, control condition, programme length, session duration, frequency, intensity, supervision) and yoga effects on mental disorder severity, as per disorder specific scales. Information regarding the yoga interventions was extracted for meta-regression analyses. The type of yoga was determined by the authors’ specifications in the protocol. A simple ‘yes’, ‘no’ or ‘not specified’ was used to determine whether the following aspects of yoga were reported in the intervention: specific yoga postures, consistent sequencing of postures, yogic philosophy, meditation, mindfulness ('attention to breath' met this criterion), breathing techniques ('pranayama' or other controlled breathing exercises met this criterion) and/or encouragement of home practice.
Study quality
Study quality was reported using the PEDro checklist34 and scores as reported on the PEDro database. Two authors cross-checked 35% of the included studies against PEDro scoring for quality assurance. A study was deemed to be of high quality with a score of 6–10, of fair quality with a score of 4–5 and of low quality with a score <4. The PEDro scores for articles included in this review are presented in table 2.
Physiotherapy Evidence Database table for included reviews
Data analysis
Random effects meta-analysis was conducted with Comprehensive Meta-Analysis software (CMA, V.3) in the following steps. Firstly, changes in mental disorder symptoms were calculated using pre- and post-means (SD) of depressive symptom severity scores of the yoga and control groups, calculating the standardised mean difference (SMD) and 95% CI as the effect size. Secondly, subgroup analyses of yoga modality (eg, vinyasa, chair, kripalu), diagnoses, intervention supervision (yes vs home practice) and intensity, as specified by the authors (eg, gentle hatha) were conducted. In the final step, exploratory meta-regression analyses investigating the moderating role of trial duration, number of sessions per week, trial quality, session length and number of components of yoga used in the intervention on the effect size were conducted. In the absence of sufficient data to conduct meta-analyses, a narrative synthesis of results was conducted. Statistical heterogeneity was assessed using the I2 statistic. An I2 value >75% was considered to indicate considerable heterogeneity, I2 50–75% was considered to indicate substantial heterogeneity and I2 <40% was considered to indicate limited heterogeneity.35 Publication bias was assessed with Egger36 and Begg and Mazumdar,37 and corrected using Duval and Tweedie trim and fill analysis.38
Results
Search results and flow of trials through the review
A total of 3880 records (excluding duplicates) were identified, and the titles and abstracts were screened. Full text versions were retrieved for 80 articles, of which 19 were eligible for inclusion. Thirteen of those reported changes in depressive symptoms and were included in the meta-analysis. Six studies were excluded from the quantitative analyses as they did not report depression symptom scores. Figure 1 shows the flow of studies through the review and reasons for exclusion.
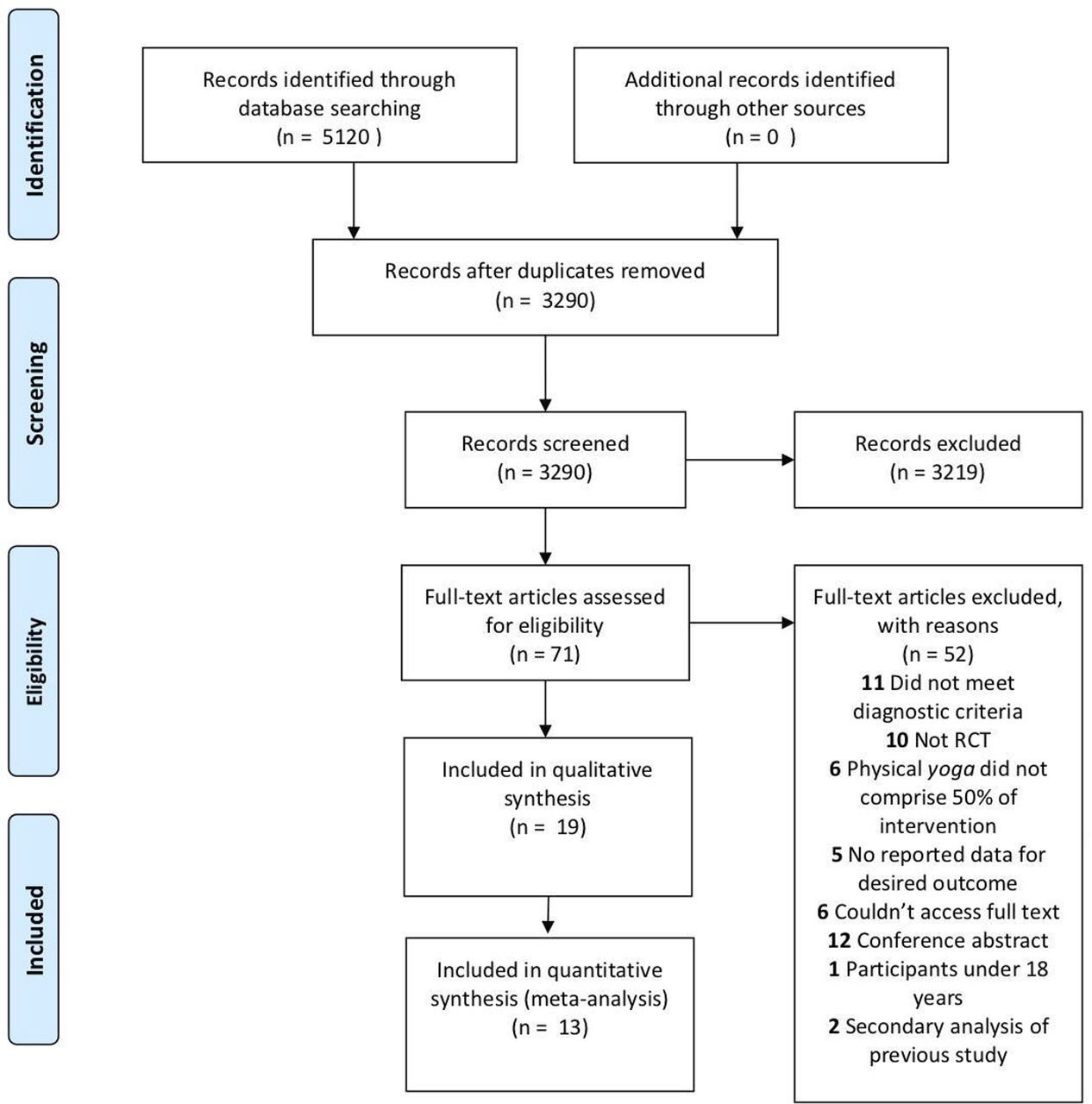
Identification and selection of studies for the review. Adapted from Moher et al. 31 PRISMA, Preferred Reporting Items for Systematic Reviews andMeta-Analyses; RCT, randomised controlled trial.
Characteristics of included trials
Characteristics of participant sample, primary diagnosis, diagnostic criteria, yoga intervention and control group are shown in table 3. Analyses of physical health outcomes were not performed because of insufficient data.
Description of the 19 included trials
Of the 19 included RCTs, 12 originated from the USA,19 39–49 two from India,50 51 two from Japan52 53 and one each from China,54 Germany55 and Sweden.56 Nine trials included patients with a depressive disorder (antenatal=539–41 43 47; bipolar depression=148; major depressive disorder=344 46 55), five included a diagnoses of schizophrenia,19 50–52 57 three with a post-traumatic stress disorder (PTSD) diagnosis,42 45 49 one with diagnosed alcohol dependence56 and one with a range of psychiatric disorders.53 A total of 1080 participants were included across the 19 RCTs; sample sizes of individual studies ranged from 18 to 122 (median=57; mean=57), with 69% of the total sample being women.
Nine studies39–41 43 45–48 55 reported using the Structured Clinical Interview for DSM for diagnostic purposes. One study used the Mini International Neuropsychiatric Interview,44 one used the Clinician Administered PTSD Scale for DSM49 and another used scores above 57 on the PTSD Checklist for DSM.42 One study used the Structured Clinical Interview for the Positive and Negative Syndrome Scale (PANSS),19 two studies used the International Classification of Diseases-10,52 53 two studies used psychiatrist interviews to confirm DSM criteria50 51 and two studies did not specify how the diagnosis was made.54 56 Tools used to measure changes in depression symptoms were the Quick Inventory of Depressive Symptomatology (QIDS SR-16),46–48 Depression Anxiety and Stress Scale (DASS-21),42 Centre for Epidemiologic Studies Depression Scale (CES-D),40 41 58 Hamilton Depression Rating Scale (HAM-D/HDRS),39 55 Beck Depression Inventory (BDI),44 49 Hospital Anxiety and Depression scale (HAD),56 PANSS Depression subscale19 and the Calgary Depression Scale (CDS).54
Interventions
In total, n=578 participants were assigned to yoga and n=502 to control conditions. Seven RCTs utilised attention control groups, including health education,43 46 47 49 yoga education,44 social support40 and bibliotherapy.48 Seven RCTs utilised waitlist control19 39 42 45 50 51 59 and five utilised treatment as usual.41 52 53 55 56 Yoga interventions were on average 2.4 months long (range 1.5–2.5 months) with 1.6 sessions per week (range 1–3 sessions) of a duration of 60 min (range 20–90 min). Types of yoga were hatha,44 46 48 49 52 53 55 vinyasa,39 SVYASA (Swami Vivekananda Yoga Anusandhana Samsthana),50 51 kundalini,42 kripalu45 or were unspecified.19 40 41 43 47 54 56 Seventeen interventions were supervised by yoga practitioners19 39–49 52–56 and two interventions were primarily unsupervised as they were home practices.50 51
Study quality
PEDro scale total scores ranged from 4 to 7, indicating that the studies demonstrated fair to high quality (high=53%, fair=47%) (table 2). Only 21% of trials reported concealed allocation and 37% used an intention to treat analysis.
Publication bias
The funnel plot for the analysis appeared to be roughly symmetrical. Publication bias was tested using Egger’s regression method36 and the Begg–Mazumdar test,37 with a p value<0.05 suggesting the presence of bias. The effect size was not modified by the Duval and Tweedie trim and fill test. Additionally, funnel plots in figure 2 display study specific effect estimates in relation to the SE, assessing the potential presence of publication bias. Heterogeneity was limited (I2=33%, p=0.11).

{kind=link}
{kind=link}
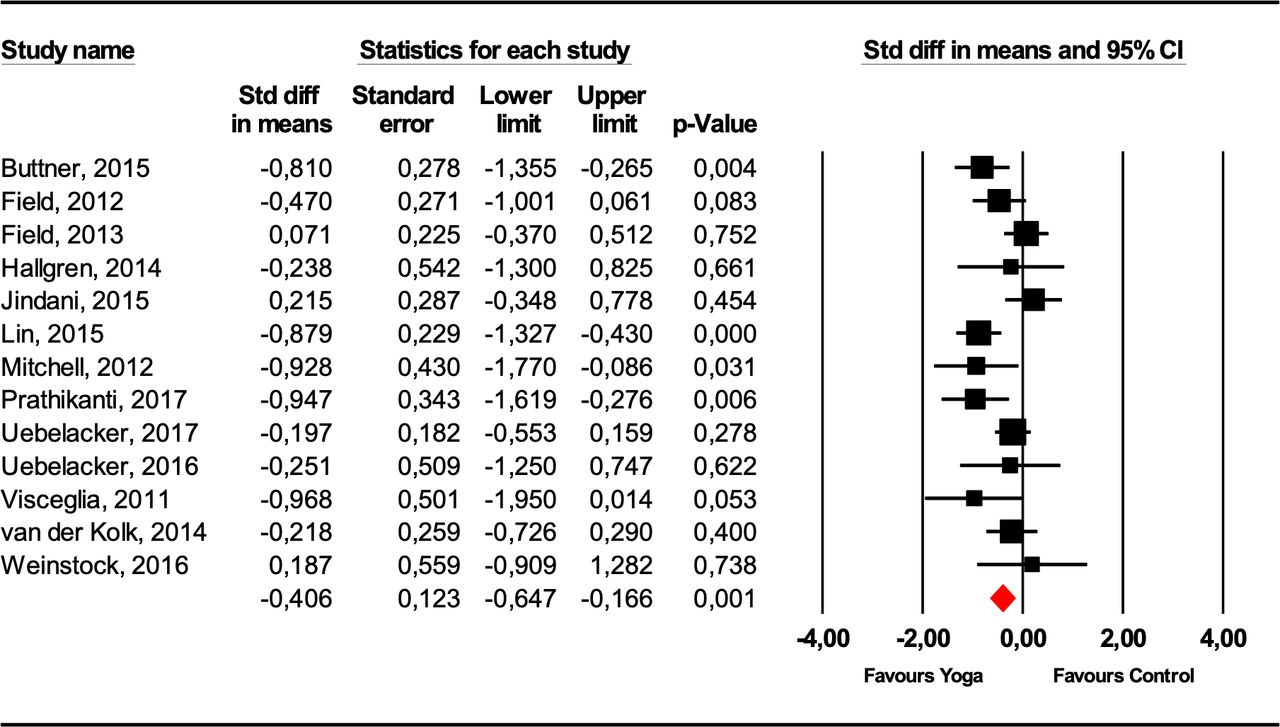
Effects of yoga versus treatment as usual, waitlist control or attention control interventions on depressive symptoms across a range of mental disorders, showing estimates of effect size with 95% CIs and relative weight (% weight) for each trial.
Assessment of overall effect
Primary outcomes: effect of yoga on depressive symptoms in people with a mental disorder
A moderate effect of yoga on depressive symptoms compared with all control groups was found (SMD=−0.41; 95% CI −0.65 to -0.17, p<0.001; heterogeneity: I2=50%; Q=23.86; p=0.02; RCT=13; yoga n=333; control n=299) (figure 2).
Subgroup analyses
Control group
Subgroup analyses based on control groups revealed evidence for a moderate effect of yoga on depressive symptoms compared with waitlist control (n=4, SMD=−0.58; 95% CI −1.03 to −0.12, p<0.05), a small, but not statistically significant, effect compared with treatment as usual (n=2, SMD=−0.39; 95% CI −1.14 to 0.36, p=0.31) and to attention controls (n=8, SMD=−0.21; 95% CI −0.54 to 0.12, p=0.22).
Diagnostic category
Subgroup analyses based on diagnostic groups revealed evidence for a moderate effect of yoga on depressive symptoms in depressive disorders (n=8, SMD=−0.40; 95% CI −0.67 to -0.13, p<0.01), no effect in PTSD (n=2, SMD=−0.01; 95% CI, −0.51 to 0.48, p=0.95), a small, but not statistically significant, effect in alcohol use disorders (n=1, SMD=−0.24; 95% CI −1.40 to 0.92, p=0.69) and a large effect in schizophrenia (n=2, SMD=−0.90; 95% CI −1.44 to −0.35, p<0.01).
Secondary outcomes: effect of yoga on physical health
Insufficient data were available to pool the effects of yoga on physical health outcomes. Seven studies included measures of physical health. One study52 examined cardiometabolic health (fasting blood glucose and total cholesterol) and found no significant differences between the yoga and control groups over the 8 week intervention. Another study by the same authors53 examined physical fitness (strength) by measuring hand grip strength, lower limb muscle endurance and knee flexion strength to body weight ratio. The yoga group had significantly greater improvements across all three measures compared with the treatment as usual group. Lin et al 57 assessed aerobic fitness with a VO2max test and found no significant changes between groups. While not statistically significant, Field et al 40 reported reduced cortisol levels within a single session (acute response) for both yoga and social support groups, and increased cortisol levels from baseline to last session (chronic response). Three studies measured physical health/functioning with self-report questionnaires. Uebelacker et al 46 reported no significant improvements for Short Form Health Survey (SF-20) scores between groups. Buttner et al 39 however used the SF-36 to measure health related quality of life and reported that the yoga group experienced a steeper linear increase in scores compared with the waitlist control. Visceglia et al 19 reported that the yoga group had significant improvements in the physical health domain of the World Health Organization Quality of Life Instrument (WHOQOL-BREF) whereas no improvement was reported for the control group.
Meta-regression
Meta-regression analyses using a mixed effects model revealed that number of sessions per week had a significant effect on depressive symptoms, with higher session frequency leading to a greater improvement in symptoms (β=−0.44; p<0.001; CI −0.66 to −0.21) (Supplementary Table 2). Other intervention variables, such as trial quality, session duration, intervention length, supervision and number of yoga components included (as reported) did not influence depressive symptoms.
Remission rates
Three studies reported remission rates where symptom severity scores returned to below the diagnostic threshold. van der Kolk et al 49 reported that 52% of participants no longer had clinically significant PTSD symptoms compared with 21% in the health education control group; Prathikanti, et al 44 reported that 60% of participants reached remission in the yoga group compared with 10% in the control group; and Uebelacker et al 46 reported no significant difference in remission rates between the groups at the end of the intervention but at the 3 month follow-up, 39% of participants in the yoga group were in remission compared with 24% in the control group.
Adverse events, attendance and dropout rates
Seven studies reported on adverse events.19 44 46–48 53 54 All reported that no adverse events occurred from the intervention. Four studies reported on some form of intervention fidelity (eg, participant fidelity such as attendance or adherence, or instructor fidelity, such as adherence to intervention protocol) (table 4).44 46–48 Dropout rates are reported in table 4. Total dropout rate ranged from 9% to 48%. All but two studies reported dropout rates.19 43
Dropout, attendance and adverse events of the included studies
Discussion
The purpose of this systematic review and meta-analysis was to examine the effects that a predominantly physical yoga practice has on depressive symptoms in people with a diagnosed mental disorder. The results demonstrated that yoga has a moderate effect on reducing depressive symptoms across a range of diagnosed mental disorders, thus suggesting yoga may be a viable transdiagnostic intervention for the management of depressive symptoms in people with mental disorders.
The magnitude of the effect of yoga on depressive symptoms compared with treatment as usual, waitlist and attention control combined (SMD=−0.41) was comparable with findings in previous meta-analyses of yoga for depressive symptoms in people with depressive disorders (Cramer et al,28 SMD=−0.69, 95% CI=−0.99 to 0.39; Gong et al, SMD=−0.59, 95% CI=−0.94 to −0.25). Gong and colleagues60 included six trials in their meta-analysis, of which four were also included in the current review. Cramer and colleagues included nine trials in their meta-analysis, of which four were also included in the current review. The variance in results is likely a reflection of the larger sample size with additional studies of high methodological quality, resulting in a more conservative effect. However, the current review has reported the most precise estimate so far, as indicated by narrower confidence intervals. Subgroup analyses in the reviews of both Gong et al (2015) and Cramer et al (2013) indicated larger effects on depressive symptoms for meditation based yoga interventions compared with physically active yoga interventions. This may partially explain the smaller overall effect seen in the present study, as only physically active yoga interventions were included. While the present review yields a smaller result than physical activity reviews, a moderate effect size indicates that yoga is an efficacious modality of physical activity that should be considered when offering interventions to psychiatric populations, particularly considering the importance of preference and enjoyment for long term adherence and behaviour change.61 Determining the benefits of mindful exercise, such as yoga, against conventional exercise should be explored further. Preliminary data suggest that combining mindfulness with conventional exercise is effective for reducing depressive symptoms.62 There is strong evidence to support that both mindfulness21 and aerobic and/or resistance exercise14 63 independently reduce depressive symptoms. Exploring whether the effects are strengthened when these are combined, or whether movement allows for greater engagement in mindfulness for novices, is a novel and integral topic. Identifying the mechanisms by which yoga may reduce depressive symptoms is of clinical importance yet is beyond the scope of this review. Nonetheless, a recent comprehensive review64 of the potential mechanisms by which physical activity may reduce depressive symptoms identified a range of biopsychosocial pathways which are likely to have broad relevance to understanding the mechanisms of yoga.
Extrapolating an effective, and even optimal 'dose' of yoga to facilitate clinically significant change would help inform clinical practice. Further exploration of yoga in comparison with conventional or purposefully non-mindful exercise may help determine effective components of yoga practice. In order to explore a dose–response relationship between yoga practice and the longevity of its benefits, future research should consider collecting follow-up data at varying time points post-intervention. Only six included articles reported follow-up data, with time points ranging from 12 weeks (2 weeks post intervention),46 16 weeks (8 weeks post intervention),51 52 18 weeks (6 weeks post intervention),53 6 months (14 weeks post intervention)46 56 and 18 months (15 months post intervention).54 Therefore, conclusions about the potential long term effects of yoga on depressive symptoms were unable to be made.
We found that the number of sessions per week moderated the effect of yoga on depressive symptoms. This is an important finding and should be considered in the design of future yoga interventions targeted at depressive symptoms in people with mental disorders. Interventions should aim to increase the frequency of their sessions per week, as opposed to the duration of each session or the overall duration of the intervention. Further investigation into the duration of effects, and whether particular types of yoga elicit better effects, would be a valuable research question to explore.
Structured exercise in depression and schizophrenia has been shown to have better outcomes when delivered by a qualified health professional.65 66 However, the impact of qualification in yoga practice and outcomes is unclear. The qualification of yoga practitioners who delivered the interventions in the included RCTs was not reported. Currently, yoga teacher training and education courses are not regulated or standardised, nor accredited within any institutes of higher education.67 This may have implications when dealing with clinical populations who have chronic and complex conditions that require indepth understanding of pathology and psychopathology as well as contraindications and safe prescription of exercise. Furthermore, additional training and upskilling in mental health first aid should be considered for any exercise professional or yoga practitioner delivering interventions for this population. Future research should report the qualification level and type, as well as the experience of the yoga practitioner delivering the intervention, and further analyses should explore the effect this has on intervention outcomes/effectiveness.
Along with efficacy, this review also demonstrated the feasibility of yoga for people with mental disorders. Attendance and dropout did not differ significantly from control groups, with some studies reporting better adherence to yoga than control condition.46 50 51 A common barrier included ‘difficulties making it to classes’,48 thus having yoga services available within inpatient and outpatient mental health facilitates may address this barrier and is likely to have positive effects on symptoms of depression, as well as increasing physical activity levels and promoting greater physical health.
Limitations
The present review included a range of yoga interventions but due to the relatively small number of trials identified and the poorly defined interventions, it was not possible to conduct separate analyses based on the type and intensity of the interventions. Results from the control and diagnostic category subgroup analyses must also be interpreted with caution because of the small number of studies included. This review did not look at comparisons with true active bona fide interventions and only a small number of studies were available for each kind of control group, thus limiting the comparability of yoga against other interventions for depressive symptoms.
This review has limitations that relate to the primary trials included, such as non-standardised reporting of intervention protocols, lack of intervention description (eg, type of yoga and components of yoga prescribed), poor methodological quality (eg, inadequate blinding of assessors, inadequate follow-up, lack of intention to treat analysis), mix of interviewer rated and self-report outcome measures, and lack of reporting intervention adherence and adverse events. More high quality studies with sufficient sample sizes based on predetermined power analyses are required.
It is essential that future yoga research is reported in a standardised manner whereby the components of yoga can be clearly determined; mindfulness, meditation and physical activity. For further understanding of the mechanism by which yoga has an effect on mental and physical health, intervention variables such as type of yoga, intensity, environment, instructor qualification, specific postures, cueing, philosophical focuses, mindfulness techniques and breathing techniques should be adequately reported. Additionally, the question of longevity of the effects of yoga following intervention cessation requires further investigation; future studies should include long term follow-up. The effects of yoga may be moderated by participant specific factors, such as comorbidities and time since diagnosis, and therefore these factors warrant reporting and investigation in future studies.
Meaningful measures of physical health should be measured so that yoga intervention data can be compared with other modalities of physical activity and independently examined with regard to its physical health benefits, particularly among individuals with a mental disorder.
Conclusion
This review found evidence of a positive effect of yoga beyond usual care for reducing depressive symptoms in people with a range of mental disorders. There was a dose–response relationship between the number of yoga sessions per week and improvements in depressive symptoms. Consideration of yoga as an evidence based exercise modality alongside conventional forms of exercise is warranted given the positive results of this review. Yoga may provide an additional or alternative strategy to engage people experiencing depression in meaningful physical activity.
What is already known?
There is an urgent need to improve physical and mental health for people with diagnosed mental disorders. This is a priority for clinicians, healthcare services, researchers and policy makers.
There is evidence to support exercise and mindfulness as singular therapies for improving depressive symptoms.
What are the new findings?
Physically active yoga has a moderate positive effect on improving depressive symptoms in people with a range of mental disorders.
Session frequency per week significantly influences the magnitude of depressive symptom reduction.
Supplemental material
Supplemental material
Ethics statements
References
Footnotes
Twitter @theyogidoc_, @simon_rosenbaum
Contributors JB and SR conceived the study. OL screened papers. FS, BS and JF assisted with data analysis. All authors contributed to data interpretation and drafting of the manuscript and approved the final version.
Funding Simon Rosenbaum is funded by an NHMRC Fellowship APP1123336. Brendon Stubbs is supported by a Clinical Lectureship (ICA-CL-2017-03-001) jointly funded by Health Education England (HEE) and the National Institute for Health Research (NIHR). Brendon Stubbs is part funded by the NIHR Biomedical Research Centre at South London and Maudsley NHS Foundation Trust. The views expressed are those of the author(s) and not necessarily those of the (partner organisation), the NHS, the NIHR or the Department of Health and Social Care. Joseph Firth is supported by a University of Manchester Presidential Fellowship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.