Article Text

Abstract
Objective To evaluate the effects of injury prevention programmes on injury incidence in any women’s football code; explore relationships between training components and injury risk; and report injury incidence for women’s football.
Design Systematic review and meta-analysis.
Data sources Nine databases searched in August 2019.
Eligibility criteria Randomised controlled trials evaluating any injury prevention programme (eg, exercise, education, braces) were included. Study inclusion criteria were: ≥20 female football players in each study arm (any age, football code or participation level) and injury incidence reporting.
Results Twelve studies, all in soccer, met inclusion criteria, with nine involving adolescent teams (aged <18 years). All studies (except one) had a high risk of bias. Eleven studies examined exercise-based programmes, with most (9/11) including multiple (≥2) training components (eg, strength, plyometric, balance exercises). Multicomponent exercise programmes reduced overall (any reported) injuries (incidence rate ratio (IRR) 0.73, 95% CI 0.59 to 0.91) and ACL injuries (IRR 0.55, 95% CI 0.32 to 0.92). For exercise-based strategies (single-component and multicomponent), hamstring injuries were also reduced (IRR 0.40, 95% CI 0.17 to 0.95). While exercise-based strategies resulted in less knee, ankle and hip/groin injuries, and the use of multiple training components was associated with greater reductions in overall and knee injuries, further studies would be required to increase the precision of these results. The incidence of overall injuries in women’s football was 3.4 per 1000 exposure hours; with ankle injuries most common.
Conclusion In women’s football, there is low-level evidence that multicomponent, exercise-based programmes reduce overall and ACL injuries by 27% and 45%, respectively.
PROSPERO registration number CRD42018093527.
- injury prevention
- sporting injuries
- injury risk reduction
- anterior cruciate ligament
- women in sport
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Women’s professional, semi-professional and community football is one of the fastest growing sports worldwide.1–3 However, the known physiological, psychological and social benefits of sports participation4 5 can be offset by the risk of injury. In football codes, lower-limb injury (eg, knee, ankle, hip/groin, hamstring) occur frequently,6 7 with previous injury the largest risk factor for sustaining an injury.8–11 Injury, fear of injury, lack of physical skills or strength are barriers to sport and physical activity participation in adolescent girls,12 hence the need to know whether programmes that aim to reduce injury in women’s football are effective or not.
When accounting for football exposure, women have a different injury risk profile than men. The risk of serious knee injury (such as ACL rupture) is at least double in women than in men, regardless of exposure or participation level.13 Women have a higher risk of concussion,14 15 knee16 and ankle injuries than men,17 with men at greater risk of hamstring18 and groin injuries.19 Football codes have a higher incidence of ACL rupture and associated burden,20–23 than do other sports.24
Lower-limb injuries occur due to a dynamic interaction of multiple risk factors,25 some that may be addressed with injury prevention programmes. Many programmes have been investigated (eg, insoles or external joint supports), but mostly exercise-based strategies.26 Exercise-based injury prevention programmes typically focus on improving strength, balance and whole body biomechanics during activities similar to non-contact ACL injury mechanisms (such as changing direction or landing from a jump).27–29 Such programmes include the FIFA 11+,30 31 Prevent injury and Enhance Performance programme (PEP),32 Knäkontroll33 and Footy First.34 These exercise-based programmes include multiple training components, such as agility, balance, mobility, plyometric, running and strength activities. Systematic reviews confirm the efficacy of such programmes to reduce ACL injuries,35 for all athletes and all sports (OR=0.50; 95% CI 0.41 to 0.59), and female athletes specifically (OR=0.33; 95% CI 0.27 to 0.41). No studies have specifically synthesised the literature for female football players, to determine the efficacy of injury prevention programmes on all injuries, and other local injuries (eg, knee, ACL, ankle, hip/groin, hamstring). Determining the sex-specific and sport-specific efficacy of injury prevention programmes will provide patients, clinicians and sporting organisations with context-specific evidence-based recommendations.
Our aim was to systematically review the effect of any type of injury prevention programme on reducing overall injury incidence in women’s football. Secondary aims were to: (1) examine the effect on reducing the incidence of ACL, knee, ankle, hip/groin and hamstring injuries; (2) describe the exercise-based training components (eg, strength, balance) included in each exercise-based programme, and explore the relationship between the number of training components and injury incidence; and (3) report the injury incidence for lower-limb injuries for female football players using control group (ie, non-intervened) data.
Methods
Search strategy and selection criteria
This systematic review is reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines.36 An electronic search of nine online databases (AMED, CINAHL, Cochrane CENTRAL, EMBASE, PEDro, PubMed, Scopus, SPORTDiscus and Web of Science) was performed from inception until August 2019. The searches combined terms related to female football players, injury prevention programmes and randomised controlled trials (online supplementary appendix table 1). Specific selection criteria were: i) randomised controlled trials including any type of injury prevention programme (eg, exercise, education, braces) and a control group that was not exposed to the intervention; ii) ≥20 female football players in each study arm (any age, any football code, any participation level); and iii) reported an outcome relating to injury incidence for any injury.
Supplemental material
Studies including men and women, or studies that included participants who played sports other than football, were included if it was possible to extract the data specific to female football players. Only full-text articles published in English were included, with grey literature excluded. When eligibility could not be confirmed from the reported data, the authors were contacted for additional information. Targeted searching of the reference lists of included articles was also performed to identify any articles not found using the systematic database search strategy.
Study selection, data extraction and quality assessment
Two reviewers (BFM and AGC) independently screened all titles and abstracts of identified reports for eligibility. Full-text manuscripts of potentially relevant articles were retrieved and evaluated against the selection criteria to determine the final list of included articles.
Two reviewers (BFM and AGC) independently extracted data from included articles, with a third reviewer (ABM) consulted to resolve any conflicting results from the data extraction. Data extracted were number of participants (total and per study arm), participant characteristics (age), recruitment sources of participants and the location of the studies, details of the intervention (type, frequency, duration of sessions) and injury outcomes (number of injuries, exposure hours). For the primary aim of the current review, the number of injuries were extracted for reported ‘overall injuries’. While the definition of injury differed between studies (eg, only lower-limb vs whole body, or unclear in their reporting of injuries), overall injuries refers to the total number of injuries reported in the study. The number of injuries in specific lower-limb regions were also extracted to examine ACL, knee (total knee injuries including ACL injuries), ankle, hip/groin and hamstring injuries. The results from the control groups were pooled for the secondary aim to estimate overall injury incidence, as well as for specific lower-limb regions. We did this for all female football players (injury per 1000 exposure hours) for all included studies as well as for the subset of adolescent players (<18 years). For exposure data reported as athletic exposures (ie, one athlete participating in one session), the athletic exposures were converted using the assumption that one athletic exposure equalled two exposure hours, as done previously.37 Estimated exposure hours were calculated if missing data could not be provided by the authors of included studies.
Two reviewers (BEP and ABM) independently extracted data for the secondary aim relating to the exercise-based training components included in each intervention, which were categorised into one of six components (online supplementary appendix table 2). Five components (agility, balance, mobility, plyometric and strength) were adapted from previous work,38 with the addition of a running component (ie, warm-up jogging, high-speed running). Each study was classified as including a component if they described at least one activity pertaining to the component definition. Furthermore, strength and plyometric components were assessed against muscular strength and power training prescription guidelines for adults with intermediate experience39 as well as for adolescents (if average age in the study was <18 years),40 to determine if they met the required criteria. If studies had unclear reporting of the intervention activities, referenced work of the intervention were examined where available.
Two reviewers (ABM and AMB) independently assessed the methodological quality of included studies using the Cochrane Collaboration Risk of Bias Tool, V.1.41 A third reviewer (KMC) was consulted to resolve any discrepancies in scoring. For each included study, the seven domains of the tool were rated as low, unclear or high risk of bias. Cohen’s kappa was calculated to assess the extent of agreement between reviewers for the seven domains, where a kappa of 0.61–0.80 was deemed a substantial level of agreement and ≥0.80 as almost perfect.42 Based on the Cochrane recommendations,41 each study was then rated overall as low (all domains low risk), unclear (all domains low or unclear risk) or high risk of bias (one or more domains high risk). Any discrepancies for study selection, data extraction and quality assessment were initially resolved through discussion and mutual consensus, with a third reviewer consulted if consensus could not be reached.
Quantitative synthesis
Where methodological homogeneity allowed, data were pooled for meta-analysis. To examine the effects of the injury prevention programmes on overall injury rates, the pooled overall injury incidence rate ratio (IRR) and 95% CIs were calculated using random-effects meta-analysis. This analysis was repeated for injuries relating to specific body regions, including ACL, knee, ankle, hip/groin and hamstring injuries. For the meta-analyses in exercise-based programmes, studies that incorporated multiple exercise-based training components in their intervention group were examined as a subgroup, along with an overall pooled estimate for all included studies (including both multiple and single exercise-based training components studies together). Stata V.15.1 (StataCorp, Texas, USA) was used to perform the meta-analyses and calculate the pooled estimates, with forest plots generated to allow a visual representation of each study and the pooled estimate. Between-study statistical heterogeneity was evaluated for each outcome using the standard I2 statistic (ie, the percentage of variability in prevalence estimates that is due to heterogeneity rather than chance, 0%=no inconsistency, 100%=maximal inconsistency),43 with a significance threshold of p<0.05. For the secondary aim, meta-regression plots were generated to examine the relationship between the number of exercise-based training components included in the interventions and the IRR. The number of training components were added together for each study, with a highest possible score of 6 if the intervention included all six training components (1 point for included, 0 points if not, 0.5 points when either strength or plyometric components did not meet specific training prescription guidelines). The meta-regression plots were generated if five or more studies were able to be pooled. Examination of tau squared (τ2) was used to detect a potential ability of the covariate (number of training components) to explain the heterogeneity in the IRR.
The Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach was also used to evaluate the quality of evidence in each meta-analysis.44 As our inclusion criteria meant that all studies were randomised controlled trials, each meta-analysis was considered the highest level of evidence (levels of quality were very low, low, moderate or high); however, this rating was downgraded based on predetermined criteria: i) the risk of bias rating was high for most studies in the meta-analysis (risk of bias); ii) there was greater than low levels of statistical heterogeneity between studies as indicated by an I2 >40% (inconsistency)45; iii) the meta-analysis contained participants from varied football codes or interventions such as exercise and education (indirectness); iv) the clinical course of action would change if the upper versus lower CIs represented the truth46; v) there were large CIs around the pooled estimate of the IRR as indicated by the upper and lower CIs having >0.50 difference (imprecision)45; vi) the majority of studies were commercially funded; or vii) there was asymmetry of a funnel plot if >12 trials were included in the meta-analysis (publication bias).47 48
Results
Search results
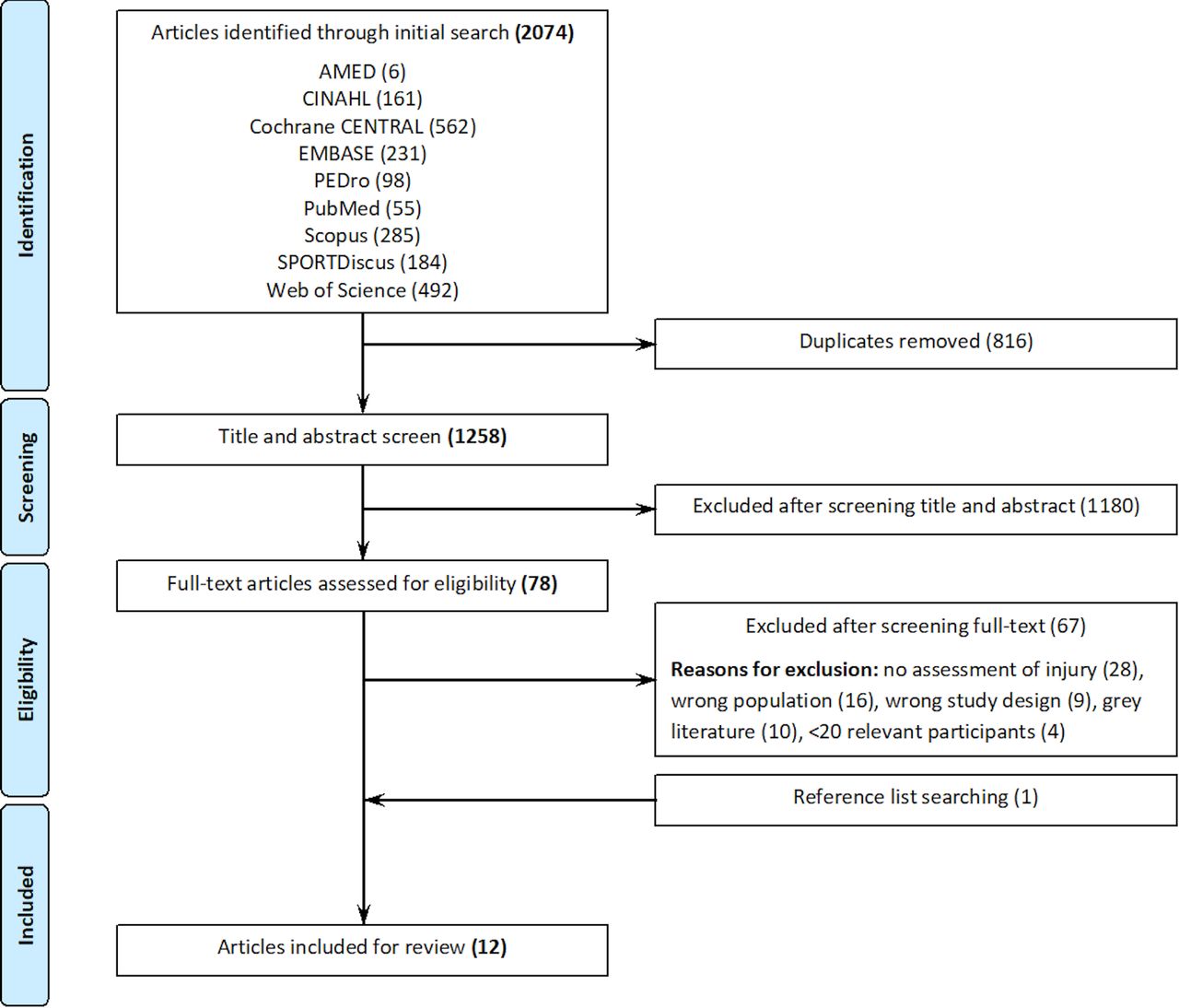
From an initial yield of 2074 articles, 12 studies were included in this review (figure 1).49–60 All studies examined soccer, with no studies identified that included other football codes.

Flow chart of study selection.
Quality assessment
The risk of bias study ratings are presented in table 1, and individual domain ratings for each study are reported in online supplementary appendix table 3. All studies, except one,50 received an overall rating of high risk of bias. Cohen’s kappa was 0.72 (95%CI 0.59 to 0.85), indicating substantial agreement between reviewers.
Study characteristics
Study characteristics
Sample size of included studies ranged from 43 to 4564 analysed participants (table 1). Seven studies were conducted in Europe,51 55–60 and five studies in North America.49 50 52–54 Most studies (9/12) involved adolescent teams (<18 years), with six studies in club-based teams (under 9–18)50 55 57–60 and three in schools.49 53 54 One study was in college teams (average age of 19.88).52 Four studies included female athletes from sports other than football49 54 or included male and female football players together.50 55 The remaining two studies were in national divisions and therefore included older participants.51 56 Intervention adherence data as well as the education and resources provided to the teams are reported for each study in online supplementary appendix table 4.
Intervention components
Neuromuscular exercise-based training (with multiple training components) was the most common intervention used in 9/12 studies.49 50 52–55 57–59 Two other studies in the review included only one exercise-based training component (one was a home-based balance training programme,56 and one an eccentric hamstring strengthening programme).51 The final study included in the review examined the effect of a lighter, smaller football on injury rate.60 As this was the only study with an intervention that was not exercise-based, it was not included in the meta-analyses. This study found a non-significant 22% greater risk of injury in the control group using the standard ball size compared with the intervention group who used the lighter and smaller ball.60
Regarding intervention components, the most common exercise-based training component was strength (10/11 studies), while agility and mobility exercises were used the least (5/11 studies; table 2). With respect to meeting training prescription guidelines, only 30% (3/10) met the guidelines for strength, and 67% (6/9) met the guidelines for plyometric/power training.
Intervention components for exercise-based injury prevention programmes
Effect of intervention on injury
Table 3 presents the reported exposure hours and number of injuries for all studies (study by Zebis et al 60 not included in the meta-analyses as it was not exercise-based). This includes overall reported injuries (primary aim) as well as specific lower-limb regions for ACL, knee, ankle, hip/groin and hamstring injuries (secondary aim). The GRADE rating of the evidence is presented in online supplementary appendix table 5 for each meta-analysis of exercise-based injury prevention programmes.
Exposure and injury data for all injury prevention programmes
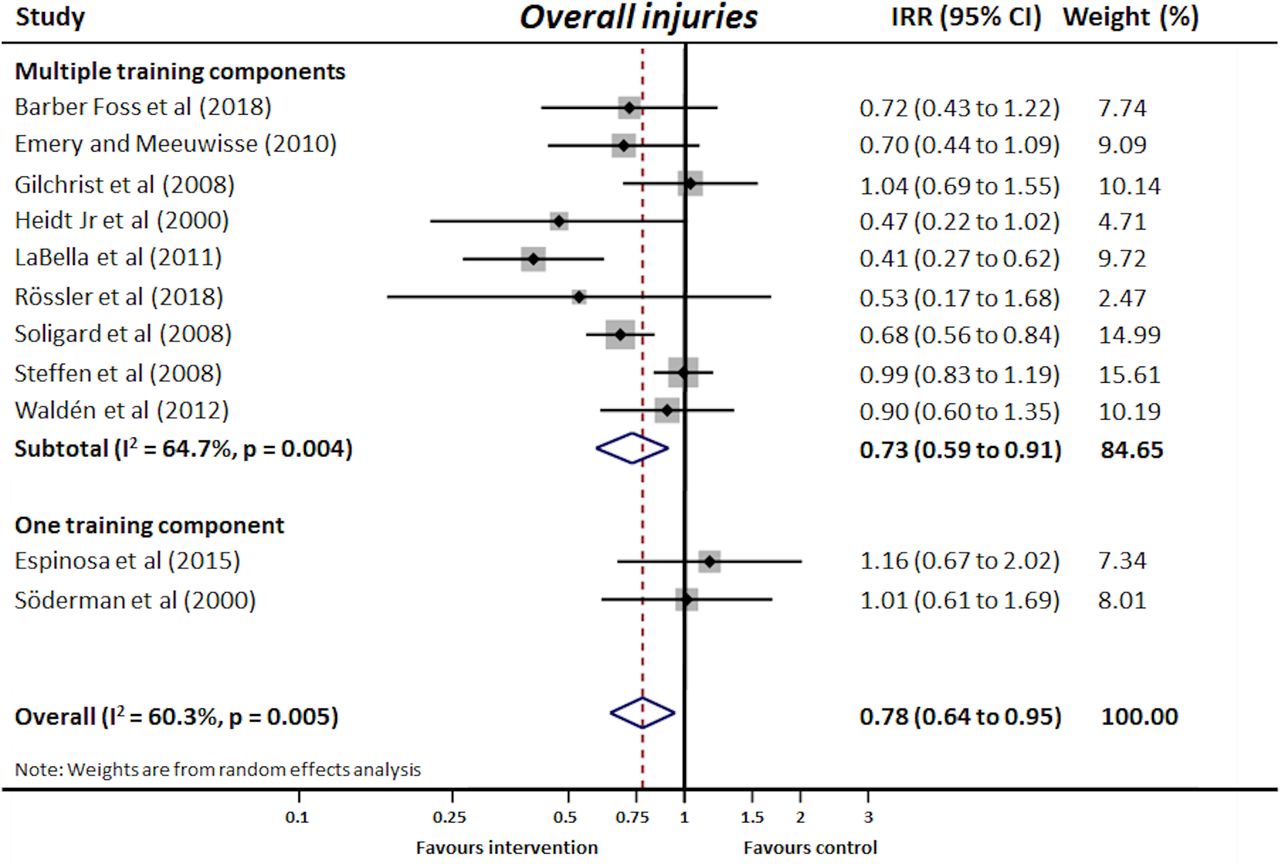
For overall injury (figure 2), we found low-level evidence (online supplementary appendix table 5) that there was a significant overall reduction of 22% in the intervention groups compared with the control groups for exercise-based programmes (total of 11 773 participants; IRR 0.78, 95% CI 0.64 to 0.95). For studies that included multiple training components, a significant reduction of 27% was observed (IRR 0.73, 95% CI 0.59 to 0.91), while also being rated as low.

Meta-analysis examining the effectiveness of reducing overall injury for the exercise-based intervention groups compared with control groups. Note: the size of the boxes around each diamond are proportional to the weight of each study, and the horizontal lines represent the 95% CI. The open diamond represents the pooled overall injury incidence rate ratio (IRR) and its width represents its 95% CI. The studies by Espinosa et al 51 and Söderman et al 56 were separated due to only including one exercise-based training component. Studies by Gilchrist et al 52 and Waldén et al 59 only reported knee injuries, and thus the values for overall injuries are taken from knee injuries.
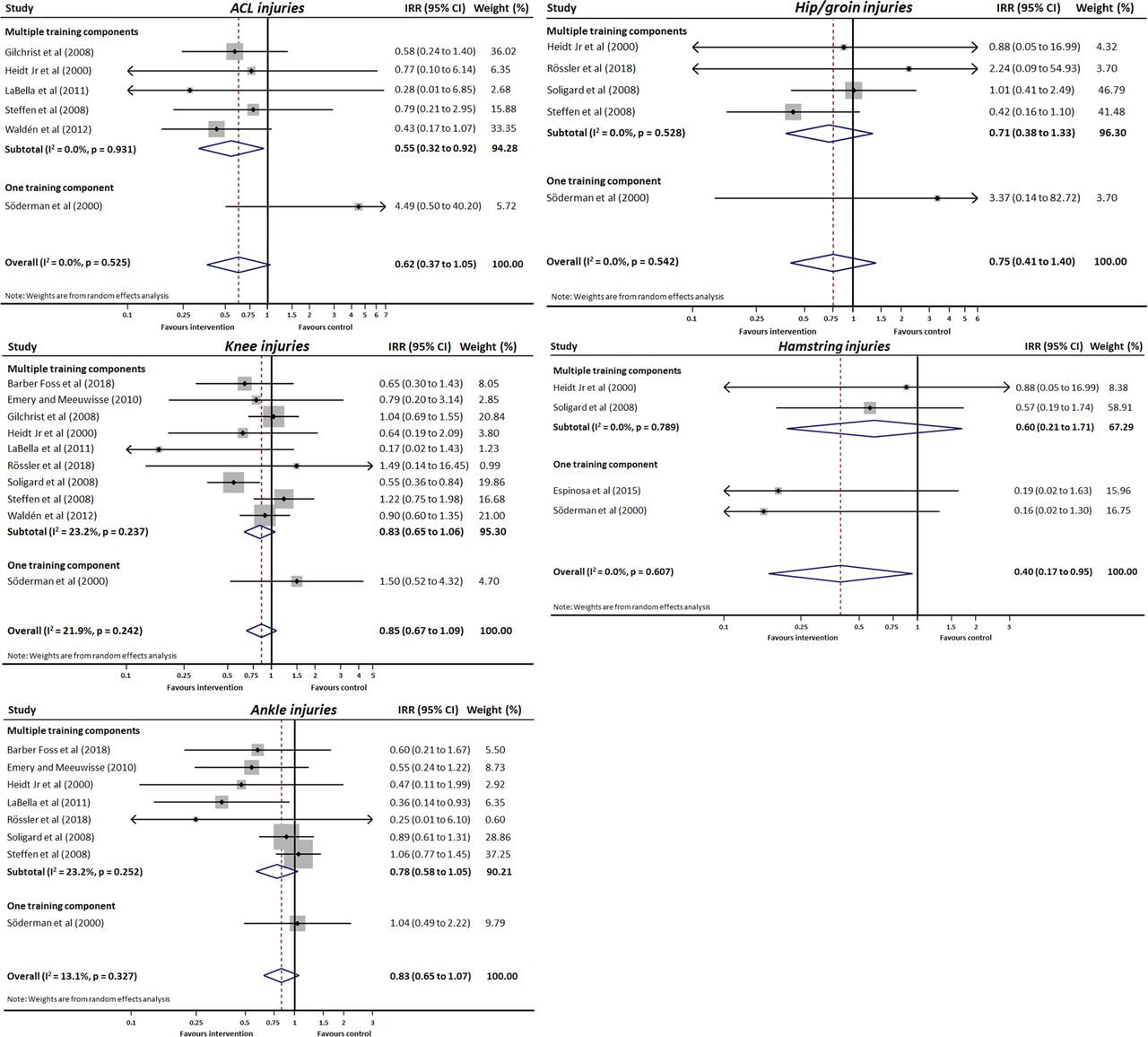
For ACL injuries (figure 3), there was a significant reduction of 45% (IRR 0.55, 95% CI 0.32 to 0.92) when examining multiple training component studies. However, when the one study that examined only balance training by Söderman et al 56 was included, this reduction was not significant at 38% (IRR 0.62, 95% CI 0.37 to 1.05). The level of evidence for the ACL meta-analyses was rated as low (online supplementary appendix table 5).

{kind=link}
{kind=link}
{kind=link}
Meta-analysis examining the effectiveness of reducing ACL, knee, ankle, hip/groin and hamstring injuries for the exercise-based intervention groups compared with control groups. Note: the size of the boxes around each diamond are proportional to the weight of each study, and the horizontal lines represent the 95% CI. The open diamond represents the pooled overall injury incidence rate ratio (IRR) and its width represents its 95% CI. For ACL injuries, the studies by Barber Foss et al 49 and Rössler et al 55 were unable to be included in the meta-analysis as both the intervention and control groups reported no ACL injuries.104 For all meta-analyses, studies reporting no injuries in one group (either intervention or control) had a fixed correction applied to both groups of 0.5 as suggested by the Cochrane Handbook for Systematic Reviews of Interventions.104
The reduction in knee injuries for the intervention groups compared with the control groups was not significant (figure 3), with the level of evidence for the knee injury meta-analyses rated as low (online supplementary appendix table 5). The overall reduction was 15% with all included studies (IRR 0.85, 95% CI 0.67 to 1.09), and 17% with only multiple training component studies (IRR 0.83, 95% CI 0.65 to 1.06).
The reduction in ankle injuries for the intervention groups compared with the control groups was not significant (figure 3), with the level of evidence for these meta-analyses rated as low (online supplementary appendix table 5). The overall reduction was 17% when all studies were included (IRR 0.83, 95% CI 0.65 to 1.07), and 22% with only multiple training component studies (IRR 0.78, 95% CI 0.58 to 1.05).
There was low-level evidence (online supplementary appendix table 5) for a non-significant reduction in hip/groin injuries (figure 3). The overall reduction was 25% when all studies were included (IRR 0.75, 95% CI 0.41 to 1.40), and 29% with only multiple training component studies (IRR 0.71, 95% CI 0.38 to 1.33).
Hamstring injuries had a significant reduction when all studies were included (figure 3) with a low level of evidence rating (online supplementary appendix table 5). There was a non-significant reduction when examining the two multiple training component studies (also rated as low; IRR 0.60, 95% CI 0.21 to 1.71). The reduction for hamstring injuries when all studies were included was significant at 60% (IRR 0.40, 95% CI 0.17 to 0.95).
Relationship between training components and injury reduction
The results of the meta-regression plots are shown in online supplementary appendix figure 6. There were no significant associations (p>0.05) found between the number of exercise-based training components included in the intervention and the IRR for all injuries (hamstring injuries were not examined due to the low number of studies reporting hamstring injuries). There appeared to be a negative relationship (eg, more training components reduced injury risk) for overall and knee injuries, however these relationships were non-significant (p=0.123 and 0.116). This was supported by a reduction in τ2 for the overall and knee injury analyses. For ACL injury, the study by Söderman et al 56 that only examined balance training strongly influenced the meta regression results (online supplementary appendix table 6). Removing this outlier, there was no association between the number of training components and the IRR for ACL, ankle and hip/groin injuries (p=0.441–0.954).
Injury incidence in women’s football
Injury incidence data were reported for the non-intervention groups of included studies (online supplementary appendix table 7). Sample size and exposure hours for these groups are reported in table 3. Many included studies did not separate training and match injuries, and hence the injury incidence data reported here are both training and match injuries combined. The incidence of overall injury in women’s football is reported as 3.42 per 1000 exposure hours (95% CI 3.19 to 3.67). The highest injury rate per lower-limb region was ankle injuries (0.97 per 1000 exposure hours, 95% CI 0.85 to 1.11), followed by knee (0.57, 95% CI 0.51 to 0.64), hamstring (0.22, 95% CI 0.15 to 0.32), hip/groin (0.15, 95% CI 0.10 to 0.21) and ACL injuries (0.12, 95% CI 0.09 to 0.16). Injury incidence rates were mostly unchanged when just examining adolescent teams (<18 years), except for hamstring injuries with reduced incidence to 0.14 per 1000 exposure hours (95% CI 0.08 to 0.23).
Discussion
For female football (soccer) players, injury prevention programmes incorporating multiple exercise-based components can reduce overall injury rates (27%) and ACL injury rates (45%). Reduction rates were not as successful (22% and 38%, respectively) when including single-component programmes. Nine out of the 11 exercise-based interventions included more than one training component,49 50 52–55 57–59 while one study included eccentric hamstring strengthening only,51 and another balance training only.56 When examining both single-component and multicomponent injury prevention programmes, exercise-based programmes can reduce hamstring injuries by 60%. Greater reductions in overall and knee injuries were observed with a larger number of training components included in the intervention, but further studies would be required to increase the precision of these results. The incidence of overall injuries in women’s football was 3.42 per 1000 exposure hours, with ankle injuries most common.
Effectiveness of injury prevention programmes on overall injuries in women’s football
Overall injuries among female football players (n=11 773) were reduced (22%) with exercise-based injury prevention programmes (for single-component and multicomponent) and reduced by 27% when only examining multicomponent programmes. This 22%–27% reduction is lower than previously reported overall injury reduction rates of 27%–40% among male football players (using the FIFA 11/FIFA 11+).61 The lower injury prevention effectiveness in female compared with male football players may reflect different responses to exercise-based training programmes in women and men.62 Additionally, the lower injury reduction rate in our current review may relate to the heterogeneity between injury prevention programmes (compared with the previous review of the FIFA 11/FIFA 11+),61 with some targeting particular injuries (eg, hamstring or ACL injuries) and some designed for other sports (eg, basketball) that may not be specific to the female football player. Designing an injury prevention programme specific to the athlete and the sport may facilitate greater buy-in and adherence from coaches and players, and increase the programme’s effectiveness.63–65 Adherence is not known to differ between men and women, nor between football players and other female athletes, and future research should evaluate sex differences in response to different types of training, adherence and strategies to improve implementation and exercise fidelity in a female football context.66
Effectiveness of injury prevention programmes on ACL injuries in women’s football
Multicomponent, exercise-based injury prevention programmes led to a 45% reduction in ACL injuries (IRR 0.55, 95% CI 0.32 to 0.92), highlighting the effectiveness of such programmes in women’s football. These results are consistent with ACL injury reduction rates of 41%–59% in all athletes (men and women), and the 39%–60% reduction reported for ACL injuries across various female sporting populations.35 38 67–70 Despite the effectiveness of exercise-based ACL prevention programmes in women’s football, they have less impact if they are not used, implemented correctly or sustained over time.71–73 The ‘real-world’ effect of injury prevention programmes may be reduced to as low as 13%.74 Future studies should include planning and strategies to address known competency, organisational and leadership barriers to implementation,75 and improve monitoring and reporting methods.66
Effectiveness of injury prevention programmes on knee, ankle and hip/groin injuries in women’s football
Knee, ankle and hip/groin injuries were reduced in female football players (knee 15%–17%; ankle 17%–22%; hip/groin 25%–29%), but additional studies are needed to improve the precision of these results. These injury reduction rates were lower than those reported previously in male soccer players (knee 32%–58%; ankle 30%–60%; hip/groin 47%),76–78 but the reductions of 15%, 17% and 25% for knee, ankle and hip/groin injuries in multicomponent programmes respectively, may be meaningful in the context of sport, where any additional increase in player availability (particularly to higher ranked players) is important for team success.79 80
The current findings should be interpreted with caution considering the low level of evidence, and knowing that the definitions of injuries, particularly of the hip/groin varied considerably—three reported ‘groin’ injuries,55 56 58 one specifically reported ‘hip/groin’,57 and data were extracted for hip flexor and groin strains in one study.53 As with overall injuries, it is difficult to compare our smaller reduction rates with previous studies due to the many confounding factors (eg, injury definitions, intervention length, adherence) other than sex.
Effectiveness of injury prevention programmes on hamstring injuries in women’s football
Hamstring injuries were reduced by 40%–60% from all studies, comparable to rates in male collegiate (63%),77 and amateur (48%)81 soccer players using the FIFA 11+. The single-component injury prevention programmes, including progressive eccentric hamstring strengthening exercises (81% reduction),51 or balance training (84% reduction),56 were more effective than multiple training component programmes.53 57 The high hamstring injury reduction rates with eccentric exercise51 would be expected, given the significant reductions (45%–77%) observed when an eccentric hamstring exercise is adhered to.65 Since postexercise muscle soreness82 83 might affect adherence, rescheduling the eccentric exercise component to after training84 may assist with adherence and hamstring injury reduction. Interestingly, the balance-only training resulted in large significant reduction in hamstring injuries.56 While multicomponent prevention programmes include hamstring strengthening exercises, only two multi-component studies53 57 reported hamstring injury rates, and further investigation is required.
Influence of included training components and clinical implications
The exercise-based injury prevention programmes (single-component and multi-component) were most effective in reducing ACL injuries (38% reduction), when compared with overall injuries, knee, ankle and hip/groin injuries (22%, 15%, 17% and 25% reduction, respectively). Given the high short-term and long-term burden of ACL injuries,20 23 85 ACL prevention programmes often include neuromuscular exercises focusing on lower-limb alignment during activities specific to ACL injury mechanisms, aligning with current clinical practice guidelines.28 29 86 87 While these activities may reduce all lower-limb musculoskeletal injuries, increased training specificity may be needed to further reduce knee, ankle and hip/groin injuries. For example, targeted progressive hip adductor strengthening to reduce groin injuries,88 89 load management strategies for chronic soft tissues or joint conditions90 or football skills to address sport-specific injury mechanisms and technical skills which may contribute to injury.28
The number of included training components was associated with greater injury risk reduction for overall and knee injuries, but these relationships were imprecise. This association was supported by a reduction in τ2 values, and consistent with the systematic review for ACL injuries in female athletes of various sports.38 Our findings may reflect low statistical power due to the small number of studies (especially for analysis of body regions), and/or the high variability between studies for each training component. Further research is needed to determine the optimal combination of training components in injury prevention programmes in women’s football.
Other injury prevention programmes
Other than exercise-based strategies, this review identified only one RCT examining a different injury reduction strategy; a smaller and lighter football, with a non-significant injury reduction in adolescent soccer players.60 Other strategies such as training load, well-being monitoring, sleep or nutrition have yet to be investigated with the rigour of a full-scale RCT, and may warrant further investigation in women’s football. The education and support provided to coaching staff and players in the included studies in this review is reported in online supplementary appendix table 4. Improving coach self-efficacy through education and training for coaches of female teams should be a priority in women’s football given the potential to improve adherence to injury prevention programmes.91 Furthermore, many coaches may lack sex-specific experience due to the rapid increase in participation and volunteer nature of women’s sub-elite football.
Incidence of injuries in women’s football
The overall (3.42 per 1000 exposure hours) and ACL, knee, ankle, hip/groin and hamstring injury incidence rates in women’s football extend current data, which is mostly limited to ACL injury rates in senior elite men’s football.19 92 93 The average incidence of knee injury (0.57 per 1000 exposure hours) for predominantly female youth players in the current study is similar to previous reports in male senior elite-level (0.47–0.54 per 1000 hours),94 95 and male collegiate-level (estimated at 0.47–0.59 per 1000 hours)96 97 soccer players. The incidence of ACL injury of 0.12 per 1000 exposure hours for predominately youth players in the current study is higher than senior elite-level (0.06–0.11)92 94 95 and collegiate-level (0.06–0.09)96 98 99 female football players. Consistent with previous studies,100 the higher ACL injury rates in female than male youth players, reinforces the need for investment of resources towards effective injury risk reduction strategies into female youth and subelite programmes. Targeting developing players and player programmes is a priority, to ensure these players are provided the best opportunities to progress to senior football with optimal well-being and performance.
Limitations
The current study has inherent limitations due to the low-level of evidence, inconsistent definitions and reporting of injury and exposure hours. Additionally, our search strategy did not include any medical subject headings, which may have limited our search results. Large CIs indicate uncertainty in results in some analyses. This is largely due to studies not reporting all injury types and being excluded from meta-analyses, or those studies having a low injury incidence.53–56 Eleven studies were included for the overall injuries meta-analysis, however two studies52 59 only assessed knee injuries, which were extrapolated in the current review to overall injuries. This process resulted in a conservative (but already significant) estimate of the injury reduction effect for overall injuries. A sensitivity analysis removing these two studies revealed the intervention effect to be greater for overall injury risk. The definition of overall injuries was also inconsistent or unclear and could refer to only lower-limb injuries or whole body (including upper body, head, neck), which could underestimate the IRR for overall injuries, if upper limb injuries were not recorded. This review did not examine upper limb injuries, with only three of the included studies reporting upper limb injuries separately.55 58 60 Due to inconsistent reporting in the included studies, injuries and re-injuries were pooled together for this review as only a few studies separated re-injuries in their reporting. Intervention bias may be evident as many studies were designed with the primary aim to reduce ACL injuries. In addition, some athletes may have been exposed to additional interventions (exercise-based or education-based) outside of the study protocols, as part of their normal routine, but monitoring of such additional interventions was not recorded or feasible in many studies.
The meta-regressions examining the relationship between the number of included training components and injury risk reduction was limited, as it did not factor in many other influences (such as length of time of each component or adherence to each component) and contained a limited amount of studies. Further studies are needed to find the optimal dosage of exercise-based injury prevention programmes, with clear reporting on training dose (duration and frequency) and adherence. Our reporting of injury incidence does not reflect consensus statements that suggest reporting training and match injuries separately.101 However, we were unable to separate training and match injuries due to many included studies not reporting training and match injuries independent of each other.49–51 54 Also, our a priori decision to convert one athletic exposure to two exposure hours (based on previous research)37 may have resulted in an underestimation of our injury incidence data if the true session length of each exposure was <2 hours. Four included studies in the review reported athletic exposures (school/college teams in the USA),49 52–54 and using a shorter duration for each athletic exposure (60 or 90 min) in these studies would have resulted in higher injury incidence results. Finally, while 11/12 studies were rated as a high risk of bias (table 1), the Cochrane Collaboration Risk of Bias Tool V.1 has inherent limitations to assess RCTs evaluating injury prevention programmes, given the inability for participants (players, coaches and programme deliverers) to be blinded (online supplementary appendix table 3). If this domain was removed, five studies would be upgraded to an unclear risk of bias.
Future directions
Future research should explore the sex-specific reasons for the smaller injury reduction rates seen in this review, compared with those previously reported for men’s soccer. Understanding aspects of the injury prevention programmes, such as the impact of sport specificity and the relative effectiveness of components, may enhance injury prevention efforts. The influence of sex-specific player and staff support, education, adherence and response to injury prevention programmes should be explored. There is also an urgent need for further research across all football codes (ie, no rugby, Gaelic, American or Australian football forms could be included) to understand the implications of different codes on injury risk, and on reduction strategies.15 93 Given the increasing professionalism of all women’s football codes, and evolving athlete physical characteristics and injury profiles, injury surveillance should also extend to all injury types. Future injury prevention programmes should consider the context-specific playing group (ie, sex, age, level of competition, injury profile), staffing, training format and facilities28 102 103 to inform content, and optimise adherence and implementation strategies. High-quality RCTs are also urgently needed, with improved methods of adherence monitoring, strategies to address female football-specific barriers and drivers of implementation, following implementation science and behaviour change theories.66 75
Conclusion
Low-quality evidence suggests that multicomponent exercise-based injury prevention programmes reduced overall and ACL injuries by 27% and 45%, respectively. Reductions of 17%, 22% and 29% were observed for knee, ankle and hip/groin injuries, but these imprecise findings reflect heterogeneity and/or lack of statistical power. Exercise-based strategies (both single-component and multicomponent) reduced hamstring injuries by 60%. A larger number of included training components was associated with greater injury risk reduction for overall and knee injuries, but further studies are required to increase the precision of these findings. Given the high burden of overall and specifically ACL injuries, the challenge now is to implement these programmes into women’s soccer, with best evidence suggesting multicomponent exercise-based injury prevention programmes can reduce injury risk.
What is already known?
Women’s football is one of the fastest growing sports worldwide, at all levels.
Injury risk differs between male and female athletes.
Injury prevention programmes can reduce ACL injuries in female athletes across a variety of sports (eg, handball, basketball).
Injury prevention programmes can reduce overall injuries in men’s football.
What are the new findings?
In women’s football (soccer), multicomponent exercise-based injury prevention programmes reduce overall injuries by 27% and ACL injuries by 45%.
There appears to be greater reductions in overall and knee injuries with a larger number of training components included in the intervention.
References
Footnotes
Twitter @kaymcrossley, @Knee_Howells, @agculvenor, @AndreaBruder, @AndreaBMosler, @MentiplayB
Contributors KMC conceived and designed the study. BFM, ABM, AMB, BEP and AGC conducted the search, quality appraisal and data extraction. All authors contributed to interpretation of data and analysis. BFM, KMC, BEP and AGC drafted the manuscript with input from ABM and AMB. All authors have read and approved the final manuscript.
Funding Support for this study was provided by an Australian Football League (AFL) Research Board Grant. BEP is supported by a National Health and Medical Research Council (NHMRC) postgraduate scholarship (no. 1114296). AGC is supported by an NHMRC Early Career Fellowship (no. 1121173). ABM is supported by an NHMRC Early Career Fellowship (No. 1156674).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.