Article Text

Abstract
Objective To systematically review risk factors for hamstring strain injury (HSI).
Design Systematic review update.
Data sources Database searches: (1) inception to 2011 (original), and (2) 2011 to December 2018 (update). Citation tracking, manual reference and ahead of press searches.
Eligibility criteria for selecting studies Studies presenting prospective data evaluating factors associated with the risk of index and/or recurrent HSI.
Method Search result screening and risk of bias assessment. A best evidence synthesis for each factor and meta-analysis, where possible, to determine the association with risk of HSI.
Results The 78 studies captured 8,319 total HSIs, including 967 recurrences, in 71,324 athletes. Older age (standardised mean difference=1.6, p=0.002), any history of HSI (risk ratio (RR)=2.7, p<0.001), a recent HSI (RR=4.8, p<0.001), previous anterior cruciate ligament (ACL) injury (RR=1.7, p=0.002) and previous calf strain injury (RR=1.5, p<0.001) were significant risk factors for HSI. From the best evidence synthesis, factors relating to sports performance and match play, running and hamstring strength were most consistently associated with HSI risk. The risk of recurrent HSI is best evaluated using clinical data and not the MRI characteristics of the index injury.
Summary/conclusion Older age and a history of HSI are the strongest risk factors for HSI. Future research may be directed towards exploring the interaction of risk factors and how these relationships fluctuate over time given the occurrence of index and recurrent HSI in sport is multifactorial.
- Hamstring
- posterior thigh
- biceps femoris
- muscle strain
- injury
- sport
- risk factors
Statistics from Altmetric.com
Introduction
The hamstrings are involved in a host of athletic motions that include running,1–3 jumping4 and kicking.5 6 Hamstring function is important to the performance of most sport-related activities, particularly when fast running is required.2 4–7 Injuries to the hamstring muscles compromise individual performance and team success in many sports.8–13 Awareness of risk factors for hamstring strain injury (HSI) is an important component of athlete load management, injury prevention and return to play decision-making post injury.14 15 Previous reviews of risk factors for injury have identified that older age and a history of HSI are commonly associated with a greater risk of future HSI.16–18
Prospective studies continue to examine a range of modifiable and non-modifiable factors to determine which are most associated with HSI.19–21 Hamstring strength can now be measured using novel field-based procedures,22 such as the Nordic hamstring exercise (NHE) test.23–25 The relationship between hamstring strength measured by these devices and HSI risk is not known.16 26 In a 2018 systematic review, isokinetic strength testing did not accurately predict risk of HSI.26 Whether an athlete’s training load, including various measures of running workload and match exposure, increase HSI risk is of interest.27–30
Given the significant body of new research, we updated our 2013 systematic review16 of risk factors for sport-related index and recurrent HSI.31 32.
Method
Search strategy and selection of studies
A systematic search was carried out using Medline, CINAHL, Embase, AMED, AUSPORT, SportDiscus, PEDro and the Cochrane Library from 2011 to December 2018. Previous searches from the original systematic review captured studies published from database inception to 2011.16 The studies included in the original review were included in this update. An identical search method was used, including databases searched.16 Keywords derived from the research question were used to structure the search and were mapped to medical subject headings where possible (online supplementary appendix 1). Citation tracking and manual reference list scanning were carried out. Ahead of press searching was performed using key sports medicine journals identified from database searches (British Journal of Sports Medicine, Scandinavian Journal of Medicine and Science in Sports, American Journal of Sports Medicine, Sports Medicine). Acquired references were imported and duplicates were removed (EndNote V.X3 software, Thomas Reuters, New York; USA). All reviewers (BG, MNB, NvD, TP) took part in applying selection criteria to prospective studies. Consensus was reached by discussion where required.
Supplemental material
Study selection criteria
Participants/injury
Included studies investigated index (ie, a first-time injury within the surveillance period) and/or recurrent HSIs (ie, a second HSI following an index HSI)31 32 in athletic populations during sport-related activities. All studies presented discrete data for HSI. Only HSIs were examined; studies examining tendinopathy, non-specific thigh injuries, hamstring origin avulsions and contusion-type pathologies were excluded.
Risk factors for HSI
Studies were required to present discrete data for one or more risk factors and their association with HSI. Intrinsic (eg, age, injury history, physical qualities) and extrinsic (eg, environment, stage of the season, competition schedule) factors were included. Studies reporting data that were not directly examined in relation to injury risk or the occurrence of HSI were excluded.
Study type
Systematic reviews and studies involving the analysis of prospectively collected data on non-modifiable factors were included. Intervention studies were excluded to limit potential confounding. All included studies involved human participants, were published in English and full-text versions were available. Conference abstracts and unpublished data were excluded.
Data collection and analysis
Risk of bias assessment
Three reviewers (BG, MNB, NvD) used a modified version of the Quality in Prognosis Studies (QUIPS) tool to assess the risk of bias of all studies that were not systematic reviews. Risk of bias assessment using the QUIPS has been previously described33 34 and has been utilised in recent HSI-related systematic reviews.26 35 36 The QUIPS permits a systematic approach to best evidence synthesis described in detail later. Two of three reviewers were allocated to each study (BG, MNB, NvD). Discrepancies between authors in QUIPS scoring were reassessed and resolved by a third reviewer to reach consensus.
Six areas of assessment determined the overall risk of bias for each study: study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis and reporting (online supplementary appendix 1). Each area has specific criteria that all studies are appraised against to identify whether it is a potential source of bias. Criteria are given a score of either ‘yes’ or ‘no’, and if for a single category there are less than 75% of ‘yes’ responses, it is deemed to be a ‘high risk’ of bias for that area of study design. ‘Low risk’ for an area is reached by scoring a ‘yes’ for 75% or more of the criteria for that single category. A study is then given an overall risk of bias according to the scores of each area. To be deemed as a ‘low risk of bias’ study, it must score a ‘yes’ for at least five categories. It must have also scored a ‘yes’ for the area relating to outcome measurement (item 4). Studies are otherwise classed as ‘high risk of bias’.
Data extraction
Data were extracted with a focus on factors evaluated for their association with index and/or recurrent HSI. Raw data were extracted according to outcome measurement and the results reported. Reviewers extracted data relating to the key results, athletic population, length of tracking, and methods of HSI diagnosis and injury classification.
Data analysis and best evidence synthesis
Non-blinded reviewers (BG, TP) extracted data independently, including mean values, medians, standard deviations (SDs), risk ratios (RRs), odds ratios (ORs) and hazard ratios (HRs). For continuous data, the difference in the injured and uninjured group means were divided by the pooled SD to calculate standardised mean differences (SMDs) and their accompanying 95% confidence intervals (CIs).37 The SMD indicates the magnitude of difference between injured and non-injured groups for a continuous variable. Where appropriate the RRs were recalculated from raw data provided. The reported ratios and the 95% CI were used when the studies did not provide adequate frequency data. Comprehensive meta-analysis V.2.0 (Biostat, Englewood, New Jersey, USA) was used to perform meta-analyses from data provided in individual studies for the potential risk factors for HSI. A random effects model was used to better account for potential methodological or statistical heterogeneity. Compared to a fixed effects approach, a random effects model reduces the likelihood of a type two error by making it more difficult for a result to be determined as statistically significant. The random effects model offers more accurate and statistically safer information by generating wider CIs around pooled effect sizes.37 Heterogeneity was assessed using the I2 statistic.38 Effect sizes were interpreted as small (0 to 0.20), moderate (0.21 to 0.5) or large (≥0.80). Statistical significance was set at p<0.05.39
A best evidence synthesis was used to identify the level of evidence (LOE) and strength of association between each factor and HSI risk. The best evidence synthesis provided another source of information in conjunction with findings from the meta-analyses. It was used to clarify the relationship with HSI when heterogeneity or a paucity of raw data did not permit a meta-analysis to be performed.26 35 36 For each risk factor analysed the LOE is determined according to set criteria that includes information from the risk of bias assessment.40 41 Listed below are the four hierarchical levels of evidence:
Strong evidence: Consistent results in two or more low risk of bias studies, with generally consistent findings in ≥75% of studies.
Moderate evidence: One low risk of bias study and one or more high risk of bias studies provide consistent findings, or consistent findings reported in two or more high risk of bias studies with consistent results in≥75% studies.
Limited evidence: Single study findings from either a high risk or low risk of bias study.
Conflicting evidence: Multiple studies (of either high risk or low risk of bias) that do not provide consistent results, with consistent results in<75% studies.
Results
Search results
Initial searches yielded 2759 articles and there were an additional 42 articles from other sources (citation tracking, ahead of press searches, manual reference checking). This yield was reduced to 1685 following removal of duplicates. Screening of the titles and abstracts resulted in selection of 138 articles for analysis in full-text form, and 44 of these articles were determined to meet the requirements for inclusion. Once combined with the yield from the original systematic review,16 a final total of 78 studies were included (figure 1).

Flow diagram demonstrating study selection for the analysis of risk factors for index and recurrent hamstring strain injury.
Description of the included studies
The most represented athletic populations were: football (n=26), Australian Football (n=21), and track and field (n=8); in predominantly male cohorts from the elite level of competition (elite: 61%, amateur: 23%, mixed: 16%), aged 16–37 years. Study populations originated from the United Kingdom (UK), Australia, France, ‘Europe’, Norway, Iceland, Belgium, Brazil, Qatar, Japan, the United States of America (USA) and the Netherlands. Across all studies 8,319 total HSIs, including 967 confirmed recurrences, were captured among 71, 324 subjects (online supplementary table 1).
Supplemental material
Overview of results of risk of bias assessment (QUIPS)
A low risk of bias was found for 28 studies (40%).12 20 23–25 27 28 42–62 A high risk of bias was identified in 42 studies (60%)19 21 22 29 30 63–99(table 1). Authors reached full agreement on risk of bias assessment (BG, MNB, NvD). The most common potential source of bias was ‘study confounding variables’ (item 5: 64.3%), which was related to whether potential confounders were defined, identified and accounted for in the study design and analysis. Other sources of bias included study attrition (item 2: 35.7%), study participation (item 1: 31.4%), outcome measurement (item 4: 28.4%), prognostic factor measurement (item 3: 25.6%), statistical analysis and reporting (item 6: 18.3%).(table 1) Systematic reviews18 26 100–105 were not subject to the QUIPS tool.
Risk of bias assessment
Overview of results from meta-analyses
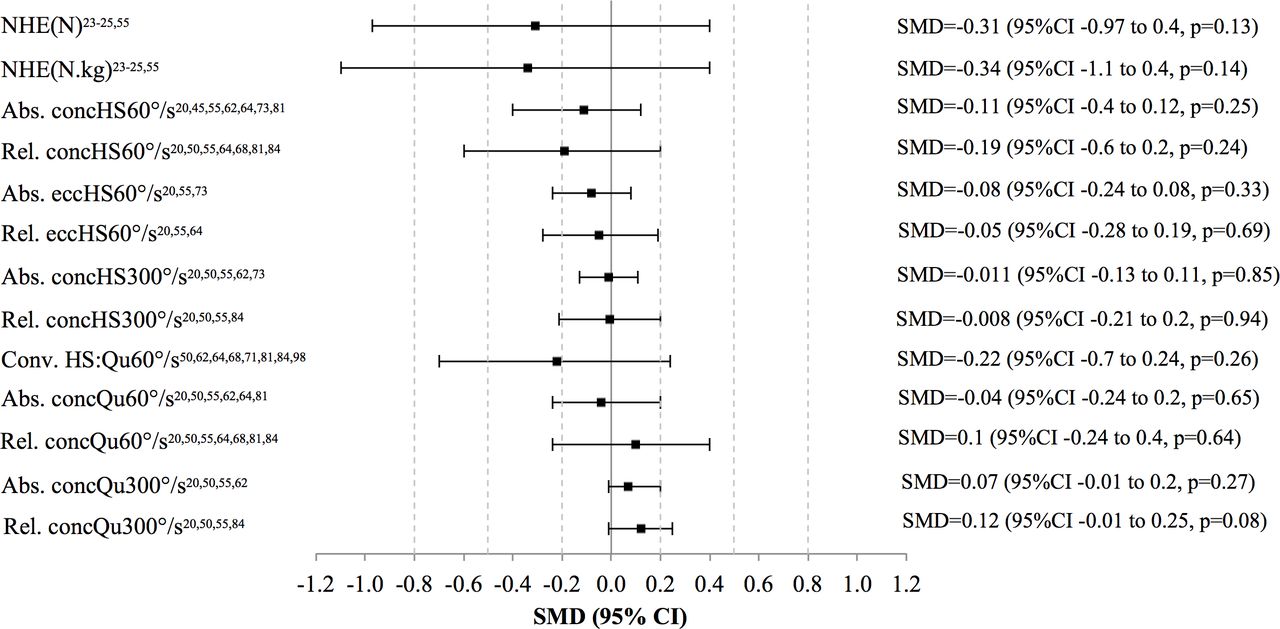
Twenty-one potential risk factors were evaluated using meta-analysis. From these results, the strongest risk factors for HSI were older age (figure 2), history of HSI, previous anterior cruciate ligament (ACL) injury and previous calf strain injury (figure 3). None of the 13 strength-related variables were significantly associated with risk of HSI (figure 4).

Meta-analysis for age, height, weight and body mass index. SMD, standardised mean difference.
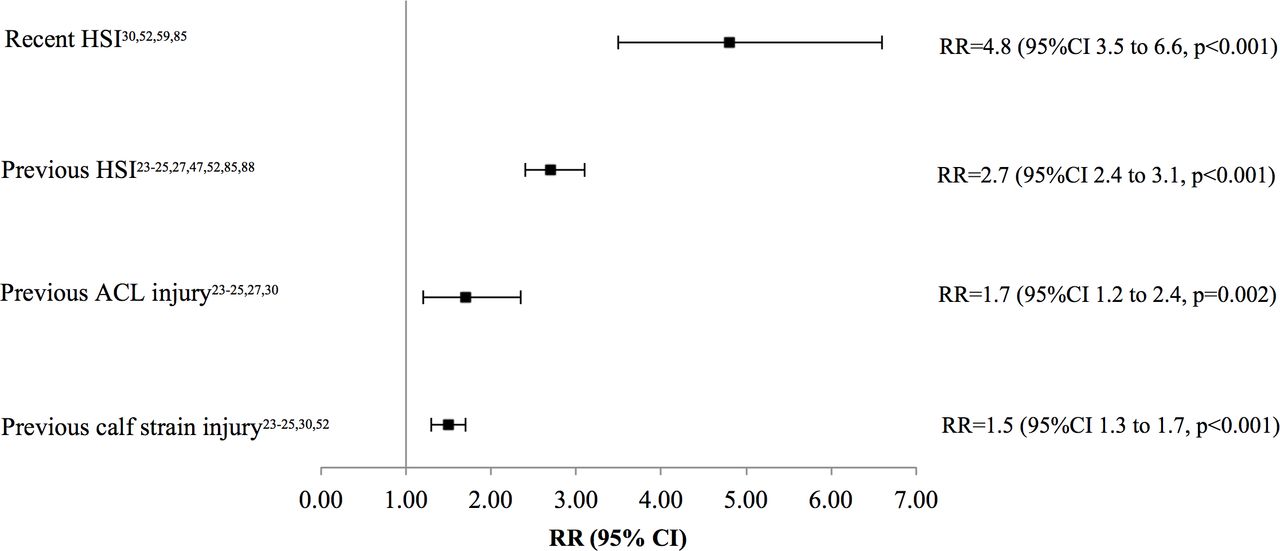
Meta-analysis for injury history: hamstring strain injury (HSI), ACL injury and calf strain injury. RR, risk ratio.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis for strength testing: Nordic hamstring exercise (NHE) and isokinetic variables. Abs., absolute; conc, concentric; Conv., conventional ratio; ecc, eccentric; HS, hamstrings; Qu, quadriceps; Rel., relative; SMD, standardised mean difference.
Overview of results from the best evidence synthesis
The best evidence synthesis included 179 factors and their association with index (129 factors) and/or recurrent (50 factors) HSI. Forty-nine factors demonstrated evidence for an association with increased risk of HSI (index: 41, recurrent: 8). One hundred and twelve factors demonstrated evidence for no association with increased risk of HSI (index: 73, recurrent: 39). Eighteen showed conflicting evidence of an unknown association with HSI (index: 15, recurrent: 3) (online supplementary appendix 2: tables 2-5).
Supplemental material
Risk factor evaluation according to key areas of risk
Non-modifiable factors
Older age was associated with a greater risk of HSI from meta-analysis of 19 studies (SMD=1.6, 95% CI 0.6 to 2.6, p=0.002).20 21 23–25 27 42 45 46 50 55–57 60 61 71 73 90 95 (figure 2). A history of HSI (RR=2.7, p<0.001),23–25 27 47 52 85 88 ACL injury (RR=1.7, p=0.002),23–25 27 30 knee injury (LOE: moderate),46 95 calf strain injury (RR=1.5, p<0.001)23–25 30 52 and ankle ligament injury (LOE: limited)51 increased the risk of HSI; if the previous HSI occurred within the same season the risk was even greater (ie, recent history: RR=4.8, p<0.001)30 52 59 85 (figure 3, online supplementary appendix 2: table 2). A history of quadriceps strain injury23–25 49 and previous chronic groin pathology/‘osteitis pubis’23–25 95 did not increase the risk of HSI (LOE: strong) (online supplementary appendix 2: table 3).
Architecture and structure
Athlete (weight, body mass index) and muscle (biceps femoris;24 gluteus maximus, gluteus medius)74 size did not increase the risk of HSI (figure 2, online supplementary appendix 2: table 3), but biceps femoris fascicle length24 and hamstring muscle-tendon unit stiffness60 were associated with risk of index HSI (LOE: limited) (online supplementary appendix 2: table 2).
Strength
Reduced hamstring strength qualities, strength endurance (index: single leg hamstring bridge;46 recurrent: eccentric leg curl21) and strength (hand held dynamometry; index: eccentric,22 isometric;22 recurrent: isometric44), were associated with an increased risk of HSI (LOE: limited) (online supplementary appendix 2: tables 2 and 5). Eccentric hamstring strength during the NHE was not associated with risk of HSI from the meta-analysis (SMDabsolute=−0.31, 95% CI −0.97 to 0.4, p=0.13; SMDrelative=−0.34, 95% CI −1.1 to 0.4, p=0.14);23–25 55 the best evidence synthesis identified conflicting evidence of an unknown association (figure 4, online supplementary appendix 2: table 4). In 11 meta-analyses isokinetic testing was unrelated to HSI risk (figure 4).
Power and ballistic function
Reduced single leg hop for distance22 and the percentage difference between non-countermovement jump and countermovement jump94 were associated with risk of index HSI (LOE: limited) (online supplementary appendix 2: table 2). Other countermovement jump measures were not associated with index HSI, such as height (LOE: strong)42 50 78 84 94 and power output (LOE: moderate)42 78 (online supplementary appendix 2: table 3).
Flexibility, mobility and range of motion
No factor related to flexibility, mobility and range of motion showed a clear relationship with risk of index HSI, including common hamstring tests: passive knee extension (LOE: strong),42 45 56 89 91 active knee extension (LOE: strong),47 56 75 76 89 91 passive straight leg raise (LOE: strong)50 61 75 89 96 and slump (LOE: moderate)47 75 76 (online supplementary appendix 2: table 3). A greater active knee extension deficit just after return to play increased the risk of recurrent HSI (LOE: limited)44 (online supplementary appendix 2: table 5). The relationships between reduced hip extension (modified Thomas test)47 75 76 91 and ankle dorsiflexion (lunge)46 47 56 75 76 and risk of index HSI were conflicting (online supplementary appendix 2: table 4).
Electromyography and motor control
Reduced trunk muscle (cluster of: internal oblique, external oblique, thoracic erector spinae, lumbar erector spinae) electromyographic (EMG) activity during the backswing phase of sprinting (LOE: limited)90 and increased gluteus medius EMG activity during running (12 km/hour, 15 km/hour) (LOE: limited)74 were associated with risk of index HSI (online supplementary appendix 2: table 2). There were conflicting findings for gluteus maximus EMG activity while sprinting and running at a range of submaximal speeds74 90 (online supplementary appendix 2: table 4). Trunk and hamstring motor control were associated with index HSI in three studies: muscle recruitment pattern during prone hip extension (LOE: limited),91 dominance of biceps femoris recruitment during a fatiguing eccentric leg curl (LOE: limited)21 and hamstring movement discrimination (LOE: limited)68 (online supplementary appendix 2: table 2).
Running-based measurements
Increases in high-speed running exposure were associated with a greater risk of index HSI27 28 (online supplementary appendix 2: table 2). Sprinting kinematics were also associated with index HSI risk in cases of increased thoracic side-bending during front swing (LOE: limited)92 and increased anterior pelvic tilt during backswing (LOE: limited)92 (online supplementary appendix 2: table 2). Aerobic (VO2 max) (LOE: moderate),42 84 intermittent running (YoYo) (LOE: moderate),50 94 sprinting (40 m sprint characteristics) (LOE: moderate)45 84 and agility (LOE: limited)50 test results were not associated with risk of index HSI (online supplementary appendix 2: table 3).
Sports performance and match play
Playing position impacted the risk of index HSI in football (LOE: strong),19 20 45 49 55–57 71 94 97 American football (LOE: moderate),62 72 rugby (LOE: moderate),12 67 Gaelic football (LOE: limited)88 and cricket (LOE: limited)85 (online supplementary appendix 2: table 2). Positions that can have larger running demands resulted in a greater risk of index HSI in football (midfielders, defenders and forwards vs goalkeepers),49 56 American football (receivers, defensive backs, running backs vs linemen)72 and cricket (fast bowlers vs spin bowlers).85 Reduced between match recovery and/or increased schedule congestion29 63 69 and the level of competition45 83 97 showed conflicting relationships with HSI risk (online supplementary appendix 2: table 4).
Clinical and imaging examination of the index HSI
Clinical examination findings of the index HSI at baseline (the number of previous HSIs;44 reduced strength endurance)21 and just after return to play (strength; range of motion; tenderness to palpation)44 were associated with greater risk of recurrent HSI (LOE: limited) (online supplementary appendix 2: table 5). None of the MRI findings of the index HSI were clearly associated with greater risk of recurrent HSI whether taken at baseline or return to play, including conflicting evidence of an unknown association for intratendinous injury/intramuscular tendon disruption54 105 (online supplementary appendix 2: table 5).
Environmental factors
International travel prior to a cricket match was associated with HSI (LOE: limited).85 Other environmental factors were unrelated to risk of HSI (online supplementary appendix 2: tables 2 and 3).
Discussion
We investigated 179 potential risk factors in a data set of 8,319 HSIs, including 967 recurrences, in over 71,000 athletes. Older age and previous injury were the strongest risk factors for HSI from meta-analysis. Athletes who have any history of HSI are 2.7 times more likely to sustain a HSI than those without, and they are at an even greater risk if the previous HSI occurred in the same season (≈5 times). The influence of these non-modifiable factors was not consistent across studies, highlighting the potential modulation of risk by other factors such as the physical characteristics of the athlete (eg, strength qualities),22 25 46 106 exposure to load (eg, high-speed27 28 and match29 30 running workload) and mechanical function when performing sport-related activities (eg, running kinematics).92 107 In the best evidence synthesis, factors related to sports performance and match play, running and strength were most consistently associated with HSI.
Modifiable risk factors
Strength and flexibility qualities were the most investigated modifiable risk factors for HSI. While baseline strength deficits were associated with a greater risk of HSI in a number of studies,21 22 44 46 flexibility, mobility and range of motion provided limited value as stand-alone risk factors. Strength and flexibility qualities change over time and fluctuate in response to exposure (ie, fatigue).14 108 It may not be valid to use data from a single occasion of baseline assessment to prospectively evaluate associations with subsequent HSI. Testing procedures may be better implemented as part of ongoing monitoring rather than baseline screening16 and when employed regularly as part of the clinical management of an index HSI to avoid a recurrence.108 109 This could be especially relevant for susceptible athletes, such as those who are older, have a history of HSI and a hamstring strength deficit.24 25 110
Running exposure is another modifiable risk factor for HSI.27 28 The risk of subsequent HSI is elevated in athletes exposed to greater high-speed running loads, especially with sudden increases (ie, within the previous 7–14 days).27 28 These athletes may be predisposed to HSI due to the fatigue and eccentrically induced muscle damage associated with fast running activities.111 Graduated exposure may also be advantageous for resilience to injury mechanisms such as sprinting.112 113 A balance must be found between inducing positive adaptations that are protective against HSI and excessive exposure that increases susceptibility to HSI.113 114
Non-modifiable risk factors
Athletes who are older and have an injury history are often at greater risk of a future injury.10 16 49 52 115 ‘Old’ is difficult to define, as age can influence HSI risk in athletes as young as 24 years.52 Age could impact HSI risk because it correlates with exposure: over time (ie, with older age) athletes are exposed to greater mechanical loads and the likelihood of encountering injury mechanisms increases. Small differences in age likely represent large differences in exposure in elite sport. Age-related physical changes may also predispose older athletes to HSI116 by affecting structural (eg, altered architecture,117 118fibre type populations,119 120cross-sectional area,120 121 stiffness122) and neurological (eg, denervation of high-threshold motor units123–125) qualities.
Previous muscle injury can also result in structural (reduced biceps femoris fascicle length,118 atrophy,126 scar tissue127) and neurological (reduced voluntary activation128) maladaptation within the injured muscle. This may explain reduced hamstring strength129 130 and a shift towards peak knee flexor torque generation at shorter muscle-tendon unit lengths131 following a HSI. Persistent deficits may reduce the ability of the hamstrings to tolerate high degrees of stress and strain, contributing to an elevated risk of recurrence.
A novel finding is that athletes with a history of ACL injury have a 70% increase in risk of HSI, and a previous calf strain injury increases the risk by 50%. The mechanisms responsible for the increased risk following ACL injury are unclear, but reduced proprioception, strength deficits and altered gait could contribute.132–134 Susceptibility to HSI following an ACL reconstruction may also be associated with ongoing hamstring deficits due to the graft used.135 136 Athletes may be more likely to sustain a HSI following a calf strain injury because the hamstrings become less conditioned to tolerate injury mechanisms and high-speed running workloads after a period of reduced exposure.28 This highlights the importance of holistic rehabilitation and greater consideration for the risk of subsequent HSI when athletes return to play from these injuries.
Recurrent HSI
Clinical data about the history of HSI and persistent hamstring deficits best evaluate risk of recurrent HSI. Strength deficits, reduced hamstring flexibility and palpation tenderness at return to play may indicate an increased risk of recurrent HSI. MRI descriptors of the index HSI at baseline and return to play do not accurately predict risk of recurrence.
Implications/future directions
Awareness of risk factors may be useful for athlete management to mitigate HSI risk. The identification of modifiable risk factors is an important component of injury prevention models.137 138 Identifying single risk factors provides some direction for clinicians, but fails to account for the complex and fluctuating interactions between risk factors.139 The interactions between potential risk factors for HSI is accounted for in some investigations,24 140 but further research is needed to fully understand these relationships and how they may influence injury risk.139 Such investigations may be especially important to guide clinical practice since HSIs (index or recurrent) unlikely occur because of any isolated factor.109 110 129
Limitations
As with any systematic review or meta-analysis, the strength of these results relies on the quality of the studies included. A lack of consistency in injury definitions and variable study methods (see online supplementary table 1), as well as limited consideration between injury types (eg, index vs recurrent HSI) and mechanisms (acute vs gradual onset injuries),16–18 are limitations of the included studies. Distinctions between index and recurrent HSI are not always clearly described. Even when this is defined, the classification of a recurrent HSI often relied on participant memory, subject to recall bias. Some recurrences may have been erroneously recorded as an index HSI despite the presence of an injury history. Given the exclusion of intervention studies, data derived from the control groups in these studies are not included here. Another shortcoming of the available evidence is that the sample size and number of HSIs are often too small to meet the methodological requirements when investigating these relationships.141 Publication and language biases are other potential limitations of this review.
Conclusion
Older age, and a history of HSI, ACL injury and calf strain injury were significant risk factors for HSI. Factors related to sports performance and match play, running and hamstring strength are likely important for evaluating the risk profile of athletes, which reflects the multifactorial nature of index and recurrent HSIs.
What is already known
Older age and a history of hamstring strain injury (HSI) are strong risk factors for HSI.
What are the new findings
Older age and injury history (HSI, ACL injury, calf strain injury) are associated with an increased risk of subsequent HSI.
Key areas to evaluate athletes for information about risk of HSI are sports performance and match play, hamstring strength, and running.
Clinical examination findings best evaluate the risk of recurrent HSI.
Future research should consider examining the interactions between risk factors for HSI, along with how these relationships fluctuate over time, such as over the course of a competition season.
References
Footnotes
Twitter @BradyDGreen, @mbourne5, @NicolvanDyk, @DrTaniaPizzari
Correction notice This article has been corrected since it published Online First. The title has been amended.
Contributors All authors made equal contributions to the work. All authors provided permission for the submission and publication of this version of the review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.