Article Text

Abstract
Objective To examine the effect of gender affirming hormones on athletic performance among transwomen and transmen.
Methods We reviewed fitness test results and medical records of 29 transmen and 46 transwomen who started gender affirming hormones while in the United States Air Force. We compared pre- and post-hormone fitness test results of the transwomen and transmen with the average performance of all women and men under the age of 30 in the Air Force between 2004 and 2014. We also measured the rate of hormone associated changes in body composition and athletic performance.
Results Participants were 26.2 years old (SD 5.5). Prior to gender affirming hormones, transwomen performed 31% more push-ups and 15% more sit-ups in 1 min and ran 1.5 miles 21% faster than their female counterparts. After 2 years of taking feminising hormones, the push-up and sit-up differences disappeared but transwomen were still 12% faster. Prior to gender affirming hormones, transmen performed 43% fewer push-ups and ran 1.5 miles 15% slower than their male counterparts. After 1 year of taking masculinising hormones, there was no longer a difference in push-ups or run times, and the number of sit-ups performed in 1 min by transmen exceeded the average performance of their male counterparts.
Summary The 15–31% athletic advantage that transwomen displayed over their female counterparts prior to starting gender affirming hormones declined with feminising therapy. However, transwomen still had a 9% faster mean run speed after the 1 year period of testosterone suppression that is recommended by World Athletics for inclusion in women’s events.
- gender
- steroids
- body weight
- physical fitness
- treatment
Data availability statement
A de-identified copy of the data is available from the corresponding author upon reasonable request.
Statistics from Altmetric.com
Background
Most competitive sports segregate male and female athletes due to biologic differences between the sexes. Because exposure to testosterone in males leads to physiologic advantages in strength and endurance, female sports need to be a protected category to ensure fairness in competition.1 Questions arise then as to which category a transgender athlete competes in and how society balances benefits to the athlete of sports participation in their experienced gender with perceptions of fairness to other athletes.2–5 Supraphysiologic doses of androgens have a positive effect on athletic performance.6 7 However, gender affirming hormones have an unknown effect on athletic performance among transgender individuals during gender transition, making it difficult to develop guidelines for transgender inclusion in sports. Several guidelines for inclusion of transgender athletes in elite international or professional sports exist but they are based on limited research.8 9 The World Athletics (IAAF) and the International Olympic Committee (IOC) created guidelines requiring female athletes to demonstrate suppression of testosterone levels to less than 5 –10 nmol/L for at least 12 months prior to competing in women’s events. However, athletes have challenged the section of these guidelines applying to women with disorders of sexual development and other causes of hyperandrogenism, citing a lack of supporting evidence, which calls these guidelines into question.10 11
Gender affirming administration of testosterone in transmen decreases adiposity, and increases muscle mass, thigh muscle volume, haemoglobin, grip strength and thigh strength.9 12–14 Gender affirming blockage of testosterone and administration of oestrogen in transwomen (oestrogen) has the opposite effect, but transwomen retain an advantage in muscle mass, volume, and strength over female controls after 1 year on oestrogen.9 14–17 Most changes in body composition occur within the first year on testosterone or oestrogen, with slower changes after that time.9 16 18–20
How do these body composition changes affect athletic performance? A retrospective review of self-reported run times among eight transwomen runners found an overall decline in times collected months to years before and after starting oestrogen but not in the runners’ performance relative to runners of the same age and gender. No other studies have examined the effect of testosterone or oestrogen on athletic performance.21
We conducted this study to examine the effect of gender affirming hormones on body composition and athletic performance among transgender individuals to help improve future guidelines for transgender inclusion in sporting competition.
Methods
Study population
This was a retrospective review of medical records and fitness tests results from 222 self-identified military personnel who filed a request to begin gender transition or continue testosterone or oestrogen while serving in the United States Air Force (Air Force).
Patient involvement
The idea for this study arose from our discussions with servicemembers seen in the Air Force Transgender Clinic about the effect of testosterone or oestrogen on body composition and athletic performance on the Air Force physical fitness assessment. We did not know how to advise them based on the medical literature. We conducted this study to address this concern.
Demographic variables
We recorded the servicemember’s age, service branch, military rank, gender assigned at birth, date testosterone or oestrogen started, type of testosterone or oestrogen used and days between starting testosterone or oestrogen and the first serum hormone level in the adult range recorded in the military electronic medical record. For transwomen, we also recorded the days between starting oestrogen and the first laboratory test indicating suppression of endogenous testosterone. We had incomplete records of testosterone or oestrogen obtained outside the military healthcare system.
Outcome measures
The Air Force requires servicemembers to participate in a physical fitness assessment every 12 months, including measurement of height, weight, waist circumference, number of push-ups and sit-ups performed in 1 min each, and time required to run 1.5 miles. The Air Force uses these tests to assess suitability for promotion, inclusion in specialised programmes and retention in the military service. The Air Force requires servicemembers to participate in all events unless a medical provider grants them a waiver for participation in a specific event secondary to a medical condition. Servicemembers with a waiver for a portion of the assessment must retake the assessment every 6 months. Enlisted servicemembers engage in regular group exercise. However, the type and intensity of training vary by occupation. The Air Force requires servicemembers who fail to meet physical fitness standards to attend additional physical training sessions outside of normal work hours until they can meet the fitness requirements or leave military service.
We assessed pretreatment fitness using the most recent score from each event on the physical fitness assessment prior to starting testosterone or oestrogen. We assessed post-treatment fitness using all fitness test scores occurring in the first 30 months after starting testosterone or oestrogen. We also recorded the time elapsed between starting testosterone or oestrogen and the occurrence of each event. The primary outcome for this study was change in fitness assessment score between the pre-hormone assessment and post-hormone assessment.
We used the results of the Air Force fitness tests performed by men (>2.3 million) and women (>567 000) under the age of 30 between 2004 and 2014 as a proxy for average performance among men (CM) and women (CW) in the Air Force.22 We used the results of all fitness tests performed by men (>3.5 million) and women (>777 000) in the Air Force between 2004 and 2014 as a proxy for height and weight among men (CM) and women (CW) in the Air Force.22
Statistical analysis
We used generalised linear mixed models with a first order autoregressive repeated covariance type in SPSS V.24 to assess the association of hormonal therapy with changes in physical fitness assessment scores. We selected this analysis method to account for correlation between repeated measures, variable number of follow-up assessments, variable follow-up times and missing data points for each participant. From this analysis we obtained an estimated mean of push-ups performed in 1 min, sit-ups performed in 1 min and 1.5 mile run times for transmen and transwomen before testosterone or oestrogen, between 0 and 1 years on testosterone or oestrogen, 1–2 years on testosterone or oestrogen and over 2 years on testosterone or oestrogen. We then compared these results with the average performance of CM and CW.
We conducted a multivariable assessment of the association between months on gender affirming hormones and changes from pre-testosterone or oestrogen fitness after adjusting for pre-testosterone or oestrogen performance and age at initiation of testosterone or oestrogen. Figure 1 is a directed acyclic graph representing the conceptual model underlying our multivariable model. Our null hypothesis for this model is that testosterone and oestrogen are not associated with a subsequent change in athletic performance for any length of testosterone or oestrogen use or pre-testosterone or oestrogen athletic performance. We performed analyses separately for transmen and transwomen.

Directed acyclic graph of our multivariable model. Pre-hormone score: the results of the most recent physical fitness assessment prior to starting gender affirming therapy. Age: age in years when starting gender affirming hormone therapy. Training intensity: type and amount of exercise performed by the servicemember. Physiologic effect of training: effect of training performed on the servicemember’s strength and endurance. Time elapsed: time interval (months) between starting gender affirming hormone therapy and the assessment of physical performance. Post-hormone change in score: change in push-ups, sit-ups and run times between the pre-hormone assessment and the current assessment (primary study outcome).
Results
Research participant characteristics
Two hundred and twenty-two servicemembers self-identified as transgender in 2016–2018 and filed a request to begin or continue gender affirming care while serving in the Air Force. We excluded 147 of these participants for the following reasons: 28 had not started testosterone or oestrogen, 3 were on testosterone or oestrogen but did not have a start date available, 99 did not have pre-testosterone or oestrogen physical assessment scores available and 16 did not have any post-testosterone or oestrogen physical assessment scores available. We included the remaining 29 transmen and 46 transwomen in our study. (table 1) The mean age of our sample was 26.2 years (SD 5.5) with a median age of 25 years (range 19–46). The majority (78.3%) of our participants were <age 30 when they began testosterone or oestrogen. Among CM, mean height was 178.2 cm (6.8) and weight was 83.5 kg (12.0). Among CW, mean height was 164.4 cm (6.4) and weight was 65.7 kg (9.8).
Pretreatment demographics and body composition
The baseline physical fitness assessment occurred an average of 144.4±101.4 days before starting testosterone or oestrogen. We followed participants for an average of 394.0±288.2 days after they started testosterone or oestrogen. Participants had an average of 2.2±0.9 assessments after starting testosterone or oestrogen (median 2, range 1–4). Among transmen, two participants were medically excused from the push-up assessment during the follow-up period, and 11 were excused from the run. Among transwomen, two were excused from the push-up assessment, one from the sit-up assessment, and four from the run. Details of the testosterone or oestrogen prescribed and time to first therapeutic hormone levels are listed in table 2.
Gender affirming hormones prescribed
Effect of gender affirming hormones on body composition and athletic performance
Tables 3–5 and figure 2 provide a summary of changes in patient outcomes while on testosterone or oestrogen. In multivariable analyses, including baseline performance, age at initiation of testosterone or oestrogen, and months on testosterone or oestrogen, we rejected the null hypothesis. In our analyses, a higher baseline score was associated with a greater decline (or smaller increase) in score at follow-up for all outcomes except for 1.5 mile run time among transwomen, where baseline run time had no effect on the changes observed at follow-up (data not shown). Age at initiation of testosterone or oestrogen had no significant effect on outcomes (data not shown). For transwomen, time on oestrogen was associated with an increase in weight (table 3) and a decline in athletic performance (table 4 and figure 2). For transmen, time on testosterone had no effect on body composition (table 3) but was associated with an improvement in athletic performance (table 5 and figure 2). Prior to treatment, transwomen were heavier than CW (mean difference 11.0 kg, 95% CI 7.6 to 14.4) and lighter than CM (−6.8 kg, −10.2 to −3.4). Transmen were lighter than CM (−14.0 kg, −17.5 to −10.5) and heavier than CW (3.8 kg, 0.3 to 7.3). Both transwomen and transmen maintained these differences over the first 2.5 years on testosterone or oestrogen (data not shown).
Effect of gender affirming hormones on weight and waist circumference
Effect of gender affirming hormones on athletic performance among transwomen
Effect of gender affirming hormones on athletic performance among transmen
{kind=link}
{kind=link}
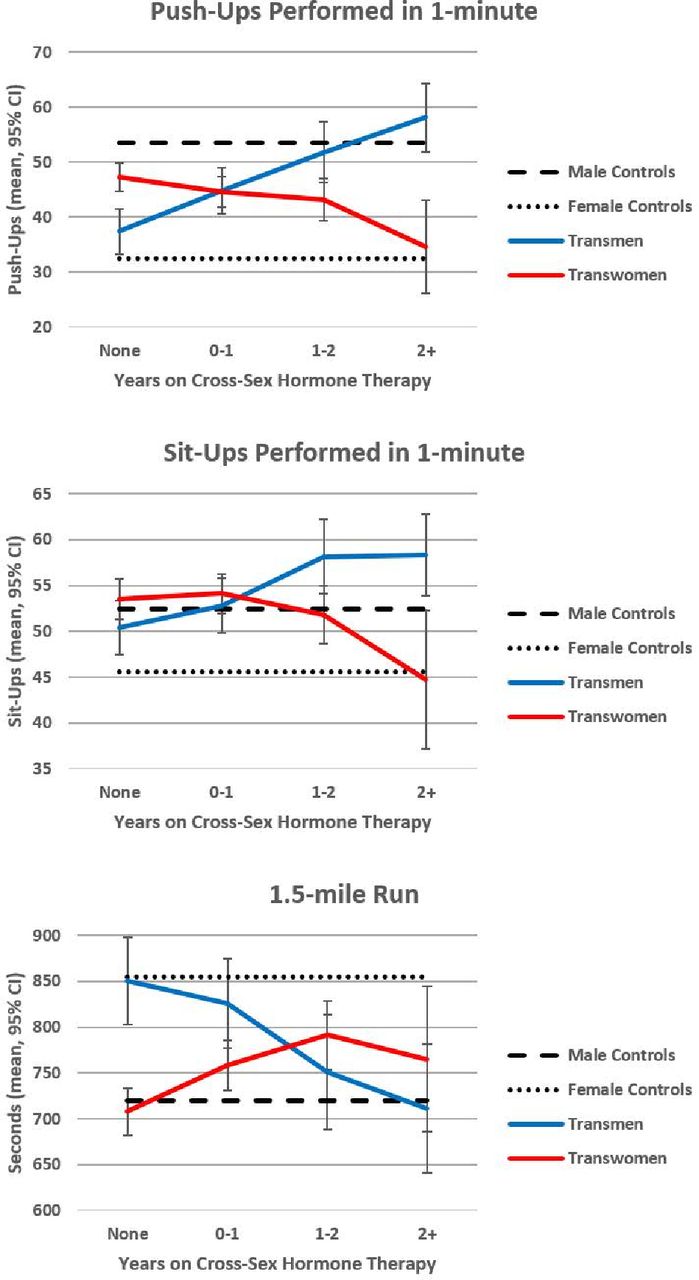
Gender affirming therapy and athletic performance. Male controls line represents the average performance on over 2.3 million Air Force physical fitness tests performed by males under the age of 30 between 2004 and 2014.22 Female controls line represents the average performance on over 567 000 Air Force physical fitness tests performed by females under the age of 30 between 2004 and 2014.22
Athletic performance among transgender servicemembers
Prior to oestrogen, transwomen performed fewer push-ups in 1 min than CM and this gap increased with oestrogen. Transwomen performed more push-ups than CW prior to oestrogen but this difference disappeared after 2 years on oestrogen (table 4 and figure 2). Prior to oestrogen there was no difference in sit-ups performed in 1 min among transwomen compared with CM but there was a difference with CW. After 2 years on oestrogen, transwomen performed fewer sit-ups than CM, but the difference with CW had disappeared (table 4 and figure 2). Run times among transwomen were similar to times among CM and faster than times among CW prior to oestrogen. Run times worsened among transwomen after starting oestrogen and became slower than times in CM but remained faster than CW at all time points (table 4 and figure 2).
Transmen performed more push-ups in 1 min than CW prior to testosterone and this gap increased with testosterone. Transmen performed fewer push-ups than CM prior to testosterone but this gap closed after 1 year on testosterone (table 5, figure 2). Transmen consistently performed more sit-ups than CW before and after testosterone. Transmen and CM completed a similar number of sit-ups in 1 min prior to starting testosterone, and transmen performance exceeded that of CM after 1 year on testosterone. There was no difference in 1.5 mile run times between transmen and CW prior to testosterone, but transmen were faster after 1 year on testosterone. Transmen were slower than CM prior to testosterone but had closed the time gap after 1 year (table 5 and figure 2).
Discussion
In this study, we assessed the effects of gender affirming hormones on transgender individuals over time by means of a standardised test in a non-laboratory setting. Athletic performance improved among transmen and declined among transwomen. Among transwomen, competitive advantages from the effects of prior testosterone exposure continued beyond the 12 month standard currently proposed for inclusion in women’s elite competition.10 This finding suggests that governing bodies for sporting competition should require more than 1 year of testosterone suppression prior to competition when creating guidelines for inclusion of transwomen in women’s elite athletics.
Study findings and prior research
Like previous studies, our study showed an association between testosterone and increased strength among transgender men.13 17 We confirmed the decrease in strength associated with oestrogen in transgender women that was found in some studies,14–16 but not others.17 Unlike several of these previous studies, our measures of muscular strength assessed repeated submaximal efforts (push-ups and sit-ups) over a 1 min period as opposed to a single maximal effort. Our results capture differences in both endurance and strength rather than just strength and probably have more relevance to sports that require sustained effort over time rather than single explosive efforts like power lifting. Our assessments of muscular strength are also confounded by differences in weight between our transgender participants and reference populations. For example, as a group, transwomen weigh more than CW. Thus transwomen will have a higher power output than CW when performing an equivalent number of push-ups. Therefore, our study may underestimate the advantage in strength that transwomen have over CW. Further studies are needed to determine if the changes we saw in our study also apply to measures of explosive strength. Participants’ exercise intentions or training habits were unknown, making it difficult to determine the aetiology of the pretreatment differences in push-up performance between transgender servicemembers and all servicemembers under the age of 30 in the Air Force. It is possible that transmen performed exercises to increase upper body muscle mass in order to give them a more masculine appearance and decrease their gender dysphoria while also improving push-up performance relative to CW. Gender dysphoria could stimulate the opposite behaviour in transwomen, decreasing push-up performance and explaining why transwomen performed fewer push-ups than CM prior to starting oestrogen. Differences in exercise habits could also influence the relationship between athletic performance and testosterone or oestrogen examined in this study. However, without the information on strength training it is impossible to make any definitive determinations.
Transmen also performed more sit-ups in 1 min than CW prior to starting testosterone. This difference in sit-up performance may also reflect a behavioural response to gender dysphoria among transmen. There was no difference between transmen and CM in sit-up performance. Unlike the increased size of upper body musculature associated with push-ups, a flat and toned appearing abdomen is seen as a positive attribute for achieving an ideal masculine or feminine appearance, making it less likely that transwomen would avoid this exercise type at a greater rate than CM.
In addition, we demonstrated a worsening of run times associated with oestrogen among transwomen that was seen in a previous study using a smaller sample and self-reported data.21 Testosterone exposure is associated with an increase in muscle volume and blood haemoglobin content, producing most of the ergogenic effects.1 The improvement in run times seen among transmen with exposure to testosterone and the decline among transwomen undergoing testosterone blockade demonstrates this ergogenic effect of testosterone. However, exposure to testosterone during puberty results in sex differences in height, pelvic architecture and leg bones in the lower limbs that confer an athletic advantage to males after puberty.1 These anatomical differences do not respond to changes in testosterone exposure among post-pubertal adults. These pretreatment anatomical differences may explain why transwomen retained an advantage in 1.5 mile run times over CW after beginning oestrogen as an adult, while push-up and sit-up performance, which are less influenced by differences in skeletal architecture, declined to the level of CW after 2 years on oestrogen. It is possible that these results could be different among transwomen who begin gender affirming hormone therapy shortly after the onset of puberty and never experienced the ergogenic benefits of testosterone exposure. Further research is required to determine if the effects of testosterone or oestrogen on athletic performance vary by level of pubertal development at the time of initiating testosterone or oestrogen and if guidelines for transgender inclusion in sports need to account for the athlete’s pubertal stage when testosterone or oestrogen began.
Study limitations and future directions
The strengths of this study include a larger sample size than previous studies, a longer follow-up period and a focus on performance on a standardised fitness test rather than isolated muscle strength. This study has limitations as well. The lack of a longitudinal control group not on testosterone or oestrogen makes changes in performance due to the passage of time a potential confounding factor. The high variability in time between baseline assessment and starting testosterone or oestrogen could also confound our assessment of the effect of time on testosterone or oestrogen. However, the uniformity of the data showing improvement in performance scores in transmen and the decline in transwomen makes it unlikely that the changes in performance are random or can be attributed to changes over time alone. The conceptual model for our multivariable analysis could be wrong and incorrectly estimate the relationship of testosterone or oestrogen with changes in athletic performance. Finally, testosterone and oestrogen protocols were not standardised for our participants. Variations in hormonal exposure between patients could confound our measurement of the effects of testosterone or oestrogen on athletic performance and body composition. Most participants had documentation of therapeutic hormone levels and suppression of testosterone, suggesting dosing at physiologic levels, although the time between starting testosterone or oestrogen and documentation of physiologic levels varied widely between participants. We do not know to what extent this variability represents differences in medication dosing or inadequate access to medical records from outside the military healthcare system. Future studies should address these limitations. Development of evidence based guidelines for transgender inclusion in elite athletic competition by governing bodies for athletics, such as the IOC and World Athletics, requires further research to define the timing of changes associated with testosterone or oestrogen.
Conclusion
In this study, we confirmed that use of gender affirming hormones are associated with changes in athletic performance and demonstrated that the pretreatment differences between transgender and cis gender women persist beyond the 12 month time requirement currently being proposed for athletic competition by the World Athletics and the IOC.10 This study suggests that more than 12 months of testosterone suppression may be needed to ensure that transgender women do not have an unfair competitive advantage when participating in elite level athletic competition.
What are the new findings?
Transwomen retain an advantage in upper body strength (push-ups) over female controls for 1–2 years after starting gender affirming hormones.
Transwomen retain an advantage in endurance (1.5 mile run) over female controls for over 2 years after starting gender affirming hormones.
Transwomen are currently mandated to have 1 year of testosterone suppression before being permitted to compete at the elite level. This may be too short if the aim is a level playing field.
Data availability statement
A de-identified copy of the data is available from the corresponding author upon reasonable request.
Ethics statements
Ethics approval
This study was approved by the 59th Medical Wing institutional review board.
Acknowledgments
The authors thank the Medical Writing Center at Children’s Mercy Kansas City for editing this manuscript for style and clarity.
References
Footnotes
Contributors All authors listed on this manuscript have contributed to the following tasks: substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data; drafting the work or revising it critically for important intellectual content; final approval of the version published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed are solely those of the authors and do not reflect the official policy or position of the US Army, US Navy, US Air Force, the Department of Defense or the US Government.
Competing interests TAR receives research funding for an unrelated project as part of the Merck Pharmaceuticals Investigator Directed Research Programme. JS is on active duty with the United States Air Force. DA is an employee of the United States Department of Defense.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.