Article Text

Abstract
Objective To investigate the aetiology and incidence of sudden cardiac arrest and death (SCA/D) in US competitive athletes.
Methods Prospective surveillance was conducted from 1 July 2014 to 30 June 2018 through the National Center for Catastrophic Sports Injury Research in collaboration with national sports organisations. Autopsy reports, death certificates, and medical records were reviewed by an expert panel to determine aetiology. Athlete participation statistics from the National Federation of State High School Associations and the National Collegiate Athletic Association (NCAA) were used to calculate incidence rates per athlete-years (AY). Comparisons of incidence rates were calculated using incidence rate ratios (IRR) with 95% CIs.
Results 331 cases of confirmed SCA/D (158 survivors; 173 fatalities) were identified; 15.4% in middle school, 61.6% in high school and 16.6% in college and professional athletes. Average age was 16.7 (11–29) years, and the majority were in male (83.7%), basketball (28.7%) or American football (25.4%) athletes. Common causes included hypertrophic cardiomyopathy (20.6%), idiopathic left ventricular hypertrophy (13.4%), coronary artery anomalies (12.0%) and autopsy-negative sudden unexplained death (9.6%). Coronary anomalies were more common in middle school athletes (28%), while cardiomyopathies (hypertrophic, arrhythmogenic, dilated, non-compaction or restricted) accounted for 47% of cases in college and professional athletes. Incidence was higher in male versus female athletes at the high school (1:43 932 AY (95% CI 1:38 101 to 1:50 907) vs 1:203 786 AY (95% CI 1:145 251 to 1:293 794); IRR 4.6 (95% CI 3.1 to 7.2)) and NCAA (1:34 906 AY (95% CI 1:25 385 to 1:49 173) vs 1:123 278 AY (95% CI 1:66 078 to 1:249 853); IRR 3.5 (95% CI 1.5 to 9.5)) levels. African American male NCAA Division I basketball players had the highest annual incidence rate of SCA/D (1:2087 AY (95% CI 1:1073 to 1:4 450)).
Conclusions Cardiomyopathies account for nearly half of SCA/D cases in college and professional athletes, while coronary artery anomalies play a more prominent role than expected in middle school athletes. Over half of SCA cases in athletes result in sudden death, calling for improved prevention strategies.
- cardiovascular
- cardiology
- death
- prevention
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The leading cause of sport-related death in competitive athletes is sudden cardiac arrest (SCA).1 2 However, studies to determine the precise incidence and aetiology of SCA in athletes have shown considerable variance. Early studies cite the incidence of sudden cardiac death (SCD) as approximately 1:200 000 athletes per year (AY) in the USA, with hypertrophic cardiomyopathy (HCM) representing one-third of cases.3–5 In contrast, more recent studies have estimated the incidence of SCD to be in the range of 1:50 000 AY to 1:80 000 AY, with higher rates among males, African-American athletes, and male basketball athletes.1 6–8 In addition, several studies suggests that structurally normal hearts and presumed primary electrical disorders, also called autopsy-negative sudden unexplained death (AN-SUD), play a larger role in SCA and death (SCA/D) in athletes than previously demonstrated.1 7 9–11
Retrospective study designs and reliance on media reports and catastrophic insurance claims has led to underestimates of the true incidence of major cardiovascular events in athletes due to incomplete case identification.8 12 13 The lack of a mandatory reporting system and defined athlete cohort has made it challenging to study an adequately sized population to determine a precise incidence. SCA with survival is also an important factor to consider, as studies investigating only deaths will exclude a critical proportion of relevant cases that were successfully resuscitated. Indeed, survival from SCA is increasing with improved emergency response programmes and access to automated external defibrillators (AED).14
A better understanding of the epidemiology of SCA/D in young athletes is needed to inform more effective and targeted prevention strategies. The purpose of this study was to determine the aetiology and incidence of SCA/D in USA competitive athletes through a comprehensive, prospective surveillance in collaboration with national centres.
Methods
This study is a continuation of previously reported aetiology data on SCA/D in US competitive athletes from 1 July 2014 to 30 June 2016.11 This study includes a 4-year dataset beginning 1 July 2014 to 30 June 2018 which allows a more robust representation of aetiology and up-to-date calculations of SCA/D incidence. This study was conducted in collaboration with the National Center for Catastrophic Sports Injury Research (NCCSIR), the University of Washington (UW) Medicine Center for Sports Cardiology, the National Collegiate Athletic Association (NCAA), the National Federation of State High School Associations (NFHS) and Parent Heart Watch.
Prospective surveillance
Prospective surveillance was executed through systematic search of traditional and social media sources; reporting directly to the NCCSIR or UW Medicine Centre for Sports Cardiology; search of student-athlete deaths on the NCAA Resolutions List; direct communication with the NFHS; and regular review of cases collected in the Parent Heart Watch database. Sources were continuously monitored through active surveillance, and duplicate cases combined across data sources as previously described.11 Attempts were made to collect autopsy reports from public records and medical records through next-of-kin consent.
Comprehensive data acquisition was attempted on the following: demographics, sport participation, SCA/D event details, medical history, autopsy and hospital records, and cardiovascular findings. Information was abstracted from media reports, medical records, autopsy reports, death certificates and direct reporting to the NCCSIR, and confirmed by phone interviews with coroners, medical examiners, family members and team/school athletic trainers and directors, when available. If no medical examiner or medical records were available, media reports and athlete photos were used to determine race. All competitive athletes in the USA are required to undergo a preparticipation evaluation that includes at minimum a history and physical examination. While some college athletes and most professional athletes also undergo a screening ECG, the specific screening protocol used in athletes later suffering SCA/D was unknown.
Inclusion criteria
Competitive athletes at the middle school (ages 11–13), high school including premiere/select level (ages 14–18), college (ages 19–23), semiprofessional and professional levels (ages 24–29) who experienced SCA/D were included. A competitive athlete was defined as an individual at least 11 years of age involved in regular training in an organised individual or team sport with an emphasis on competition and performance. Furthermore, former athletes were included if the cardiac event occurred within 1 year of competitive sports participation in one of the previously described categories. SCD was defined as a sudden unexpected death due to a cardiac cause or a sudden death in a structurally normal heart with no other explanation for death and a history consistent with cardiac-related death. SCA was defined as an unexpected collapse due to a cardiac cause in which cardiopulmonary resuscitation and/or defibrillation was provided in an individual who survived.11
All cases of confirmed SCA/D in a competitive athlete were included regardless of the activity at the time of the event, including those occurring during exercise, within 1 hour of exercise, at rest or during sleep. Cases occurring during exercise in which autopsy or medical records could not be obtained were included as cardiac in nature if the event details supported an abrupt collapse requiring cardiac resuscitation. Cases of possible SCA/D were excluded if participation as a competitive athlete could not be confirmed, a cardiac aetiology could not be determined (including autopsy negative cases) when occurring during rest or sleep, or a non-cardiac diagnosis was identified.
Aetiology panel adjudication
Provided the high variability in postmortem examinations in the USA, all records for cases of SCA/D were examined by a multidisciplinary study panel including experts in cardiovascular pathology, sports medicine and sports cardiology to determine the underlying cause based on published criteria.1 7 11 15 The Mayo Clinic nomograms for predicted mean heart weight based on age, sex and body weight were used as a component of the pathological guidelines.16 17 If the adjudicated diagnosis differed from the cause of death listed on the autopsy report, the adjudicated diagnosis was used for analysis in this study.
Incidence calculations
Athlete population statistics were retrieved from the NFHS and NCAA in which participation data is provided per sport. Participation data for middle school athletics, the National Association of Intercollegiate Athletics, junior/community colleges, semiprofessional and professional levels was not available, and therefore, incidence rates could not be calculated at these levels. Race participation data were available for NCAA athletes; however, race statistics are not reported by the NFHS. All incidence rates are reported per athlete-years (AY) of participation. At the high school level, some athletes play multiple sports but should account for only one AY of participation. In calculating the overall incidence at the high school level, a conversion factor of 2.35 was applied to account for multisport athletes as used in prior studies.4 7 18 19 A conversion factor was not used for calculation of sport-specific incidence rates in high school athletes as the actual participation statistics were available. Sport-specific incidence was calculated for sports in which five or more SCA/D events occurred during the study period. Incidence was further subdivided by race and NCAA division at the collegiate level. The relative risk of SCA/D in male college athletes by sport and race was compared with the risk in male high school athletes.
Because case capture and reporting mechanisms vary per state within the USA, we also conducted an exploratory analysis of the incidence of SCA/D in male high school athletes. State-specific participation statistics for high school athletes was obtained for each state based on NFHS data. We chose to calculate the incidence of SCA/D in male high school athletes in states with five or more SCA/D cases as incidence rates with fewer than five events may be unreliable. A similar analysis could not be conducted for female high school athletes due to the low number of SCA/D cases.
Statistical analysis
Summary statistics and frequencies were calculated for all cases. Comparisons of incidence rates for cases of SCA and SCD stratified by race, sex and sport were calculated using incidence rate ratios (IRR) with 95% CIs through the EpiR package in RStudio. IRRs and CIs were calculated using exact methods suitable for rare events. Statistical calculations were performed using RStudio (V.1.1.463, R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
This research was done without patient or public involvement in the study design, data analysis, writing or editing.
Results
A total of 331 cases of confirmed SCA/D were identified in middle school, high school, collegiate and professional athletes across the USA during the 4-year study period. One hundred and fifty-eight (47.7%) were cases of SCA with survival and 173 (52.3%) were cases of SCD. Demographic information for all cases is presented in table 1. Notably, the majority of cases were observed in males (83.7%), high school athletes (61.6%) and during exercise (74.0%). Over half of all cases occurred in either basketball (95, 28.7%) or American football (84, 25.4%) athletes (table 2).
Demographic information for cases of sudden cardiac arrest and death in competitive athletes: 1 July 2014–30 June 2018 (n=331)
Sport information for cases of sudden cardiac arrest and death in competitive athletes: 1 July 2014–30 June 2018 (n=331)
Aetiology
An aetiology could be determined in 209 (63.1% of all confirmed SCA/D) cases (141 deaths and 68 survivors). Information contributing to an adjudicated diagnosis included autopsy reports, cause of death reporting from the medical examiner, death certificates, verbal diagnosis from next-of-kin or a stated diagnosis in a media report (figure 1).
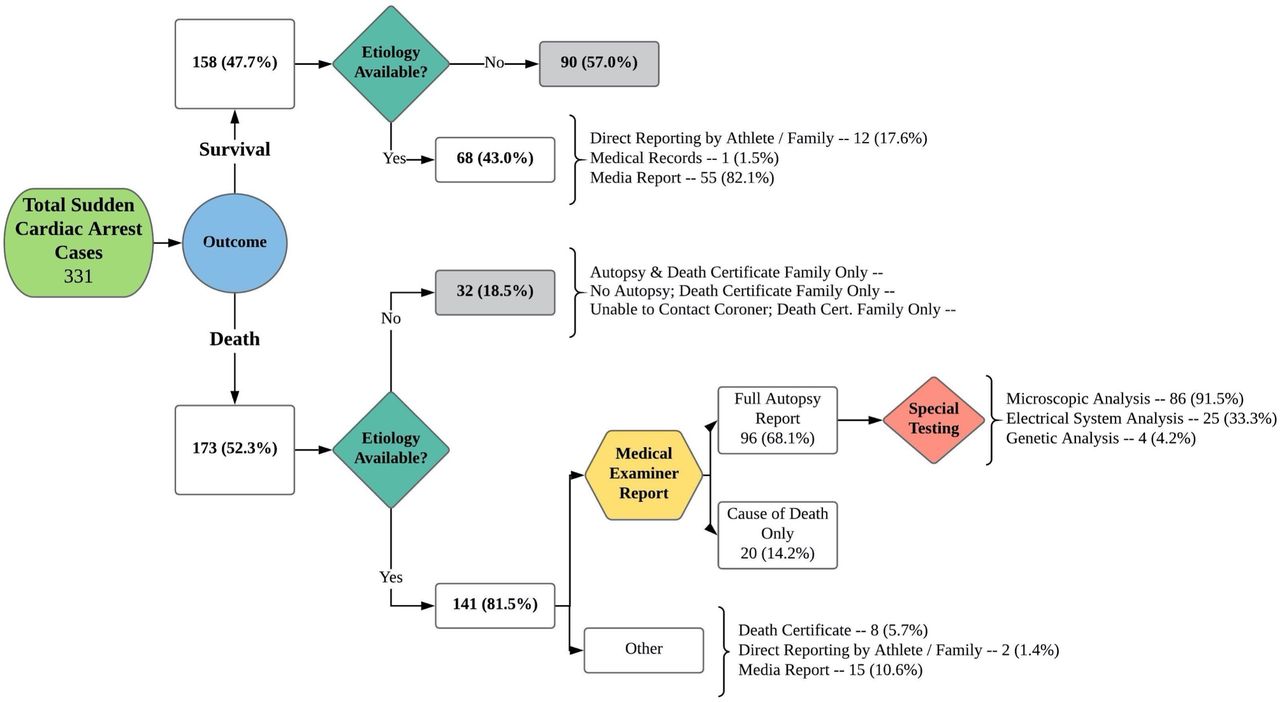
Aetiology acquisition for cases of sudden cardiac arrest and death in competitive athletes: 1 July 2014–30 June 2018 (n=331).
Information regarding the cause of death was available in 141 of 173 (81.5%) SCD cases. A medical examiner report was available in 116 (67.1%) cases, including 96 full autopsy reports and 20 cause of death reports. Eighty-six (91.5%) of the available autopsy reports included microscopic examination and 4 (4.2%) genetic analysis. In 17 of 96 (17.7%) cases with full autopsy reports the adjudicated diagnosis differed from the cause of death stated in the autopsy report, including five cases determined to be AN-SUD. Information regarding the cause of SCA was available in 68 of 158 (43.0%) of survivors; however, medical records could be attained for review in only one case.
The most common cause of SCA/D was HCM (n=43, 20.6%), followed by idiopathic left ventricular hypertrophy (n=28, 13.4%), coronary artery anomalies (n=25, 12.0%) and AN-SUD (n=20, 9.6%) (figure 2). Aetiology differed by age level (table 3). Coronary artery anomalies were the most common cause of SCA/D in middle school athletes (28%) but represented only 12% of cases in high school athletes and 3% of cases in college and professional athletes. Cardiomyopathies (hypertrophic, arrhythmogenic, dilated, non-compaction or restricted) accounted for 47% of cases in college and professional athletes, but represented only 28% of cases in high school athletes and 27% in middle school athletes.

Aetiology of sudden cardiac arrest and death (n=209).
Aetiology of sudden cardiac arrest and death by level of competition (n=209)
Incidence
During our study period, the total number of participating high school and NCAA athletes was 13 437 949 AY and 1 979 937 AY, respectively. The overall average annual incidence rate of SCA/D at the high school and NCAA levels was 1:65 872 AY (95% CI 1:57 691 to 1:75 538) and 1:50 768 AY (95% CI 1:37 960 to 1:69 285), respectively. The incidence rate of SCA/D was higher in male vs female athletes at both the high school (1:43 932 AY (95% CI 1:38 101 to 1:50 907) vs 1:203 786 AY (95% CI 1:145 251 to 1:293 794); IRR 4.6 (95% CI 3.1 to 7.2)) and NCAA (1:34 906 AY (95% CI 1:25 385 to 1:49 173) vs 1:123 278 AY (95% CI 1:66 078 to 1:249 853); IRR 3.5 (95% CI 1.5 to 9.5)) levels.
Among the sports analysed at the high school level with five or more cases in male athletes, ice hockey (1:23 550 AY; 95% CI 1:12 110 to 1:50 207), basketball (1:39 811 AY; 95% CI 1:31 076 to 1:51 761) and football (1:82 587 AY; 95% CI 1:64 189 to 1:107 900) had the highest incidence rates of SCA/D (figure 3). In female high school athletes, only soccer (n=6) had greater than five cases with an incidence rate of 1:256 005 AY (95% CI 1:131 641 to 1:545 783).

Incidence rates of sudden cardiac arrest and death in high school athletes. AY, athlete-years.
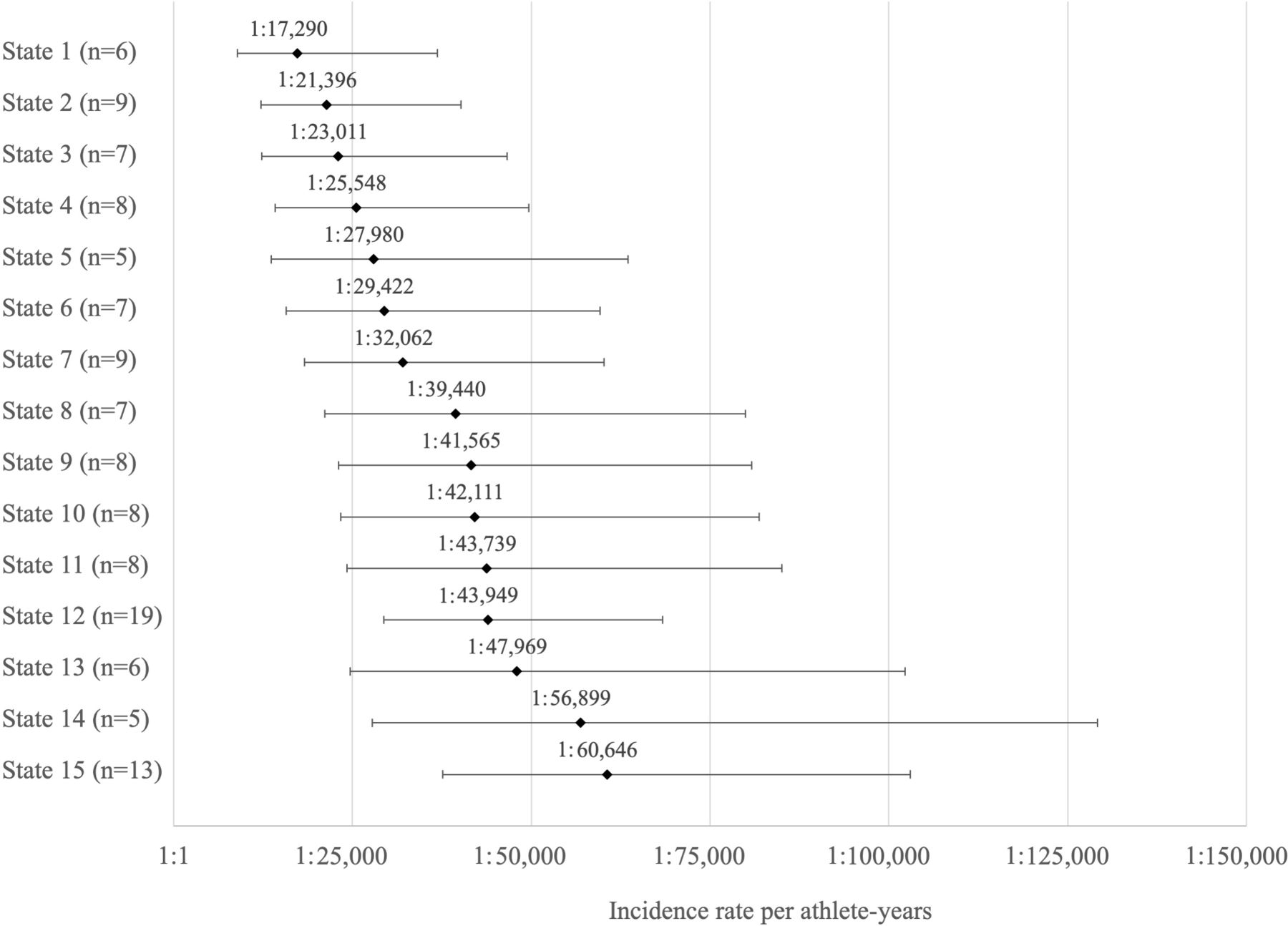
The incidence of SCA/D in male high school athletes was also analysed in states with five or more SCA/D cases (figure 4). Three states had an incidence less than 1:25 000 AY (range 1:17 290–1:23 011); 10 states had an incidence between 1:25 000 and 1:50 000 AY (range 1:25:548 – 1:47 969); and two states had an incidence between 1:50 000 AY and 1:100 000 AY (range 1:56 899–1:60 646). Incidence rates for 25 states were not included as each had less than five cases reported during the study period. In nine states, no case of SCA/D in a high school male athlete was reported or identified during the 4-year study period.
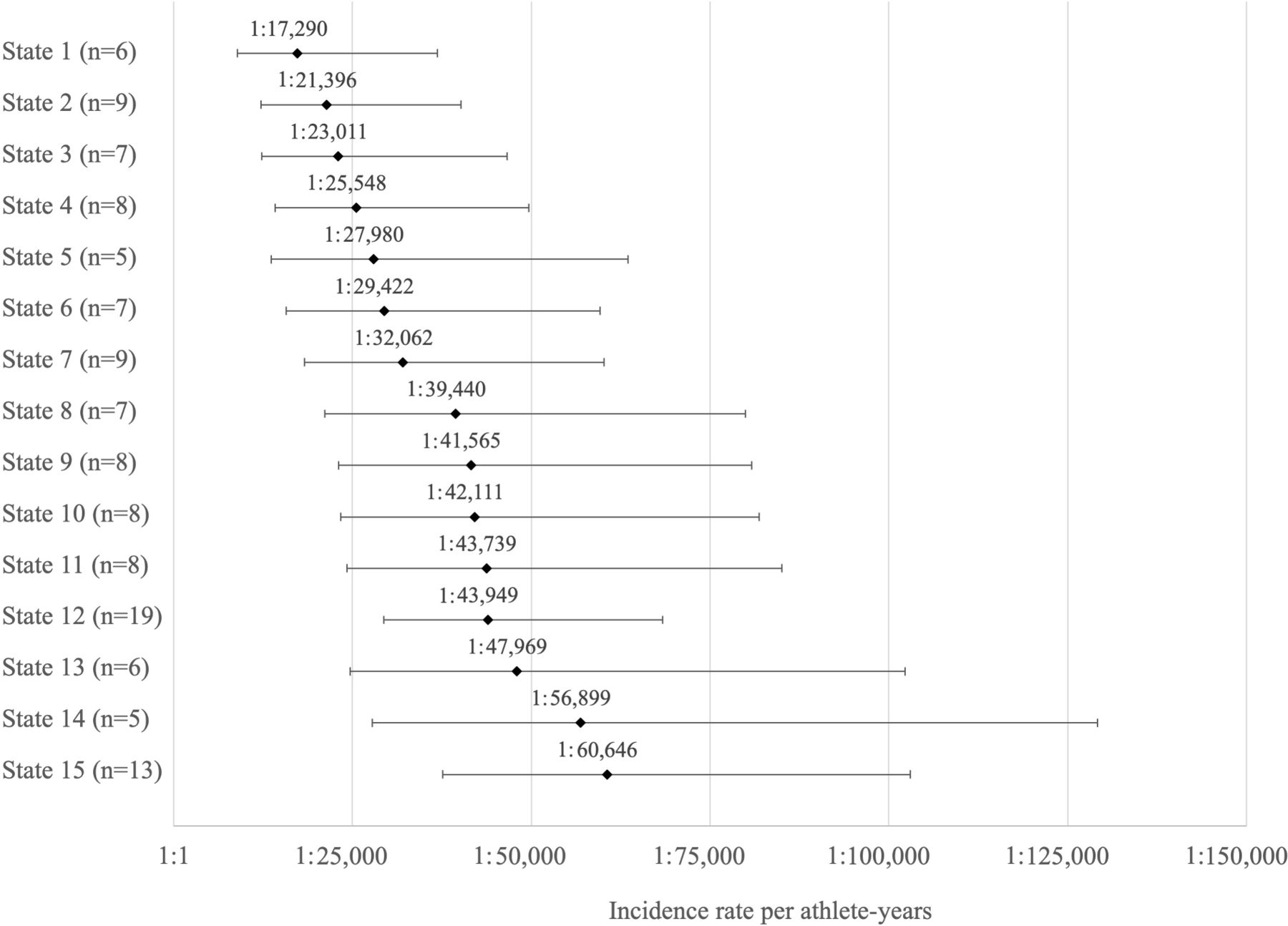
Incidence rates of sudden cardiac arrest and death in high school male athletes in states with five or more cases.
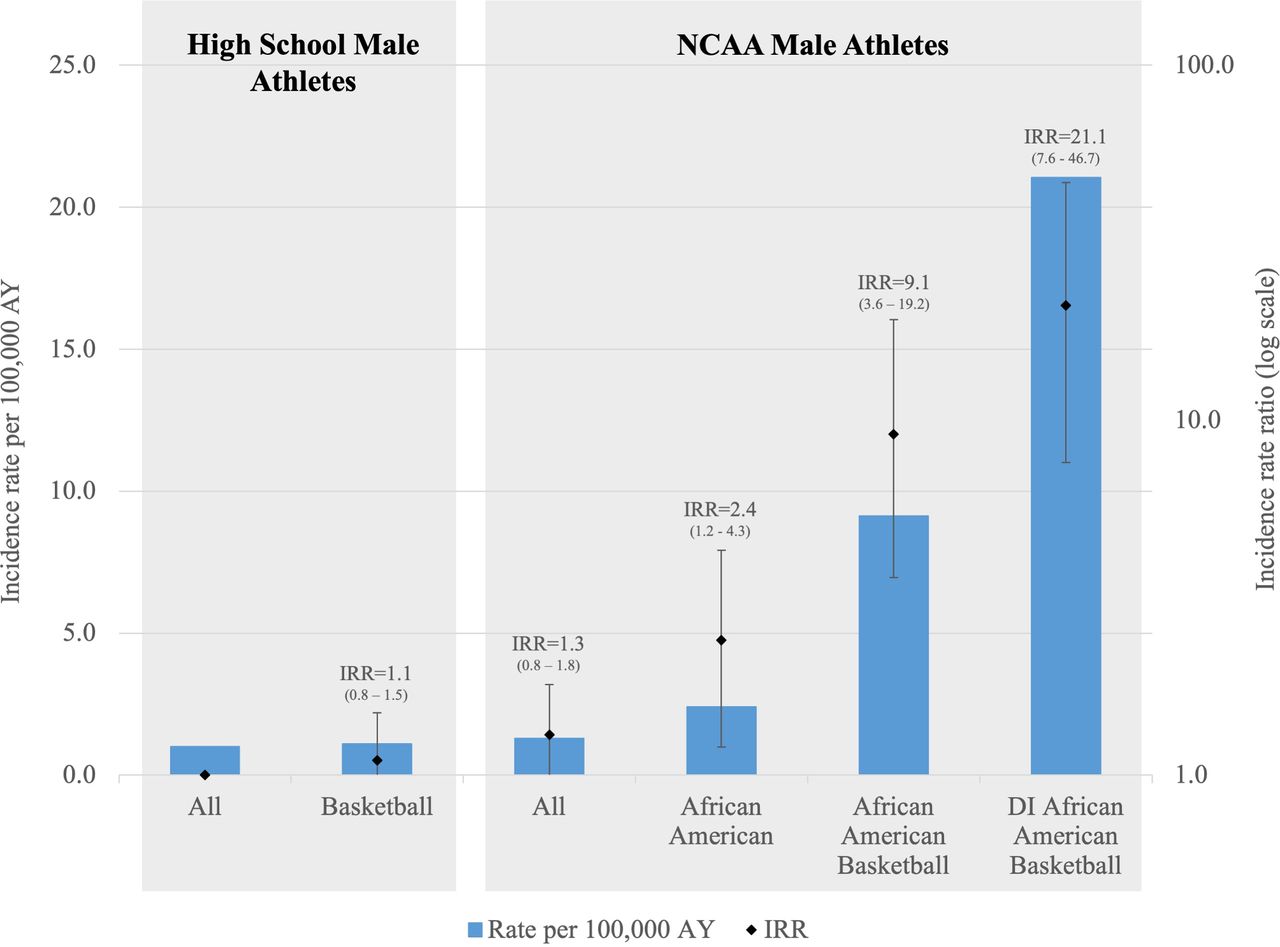
In NCAA athletes, the incidence rate appeared higher in African American (1:18 413 AY; 95% CI 1:11 226 to 1:31 921) vs Caucasian (1:38 641 AY; 95% CI 1:25 554 to 1:60 802) male athletes (IRR 2.1; 95% CI 0.9 to 4.6), although this difference was not statistically significant (figure 5). Basketball players had the highest incidence among both African-American (1:4810 AY; 95% CI 1:2578 to 1:9 748) and Caucasian (1:15 098 AY; 95% CI 1:5420 to 1:48 808) male athletes (IRR 3.1, 95% CI 0.6 to 31.0) . African-American male NCAA Division I basketball players had the highest annual risk of SCA/D (1:2087 AY; 95% CI 1:1073 to 1:4 450). In addition, 85.7% of African American male basketball cases were at the Division I level. The IRR of SCA/D in an NCAA Division I African-American male college basketball athlete compared with a high school male athlete was 21.3 (95% CI 7.6 to 46.7) times higher (figure 6).
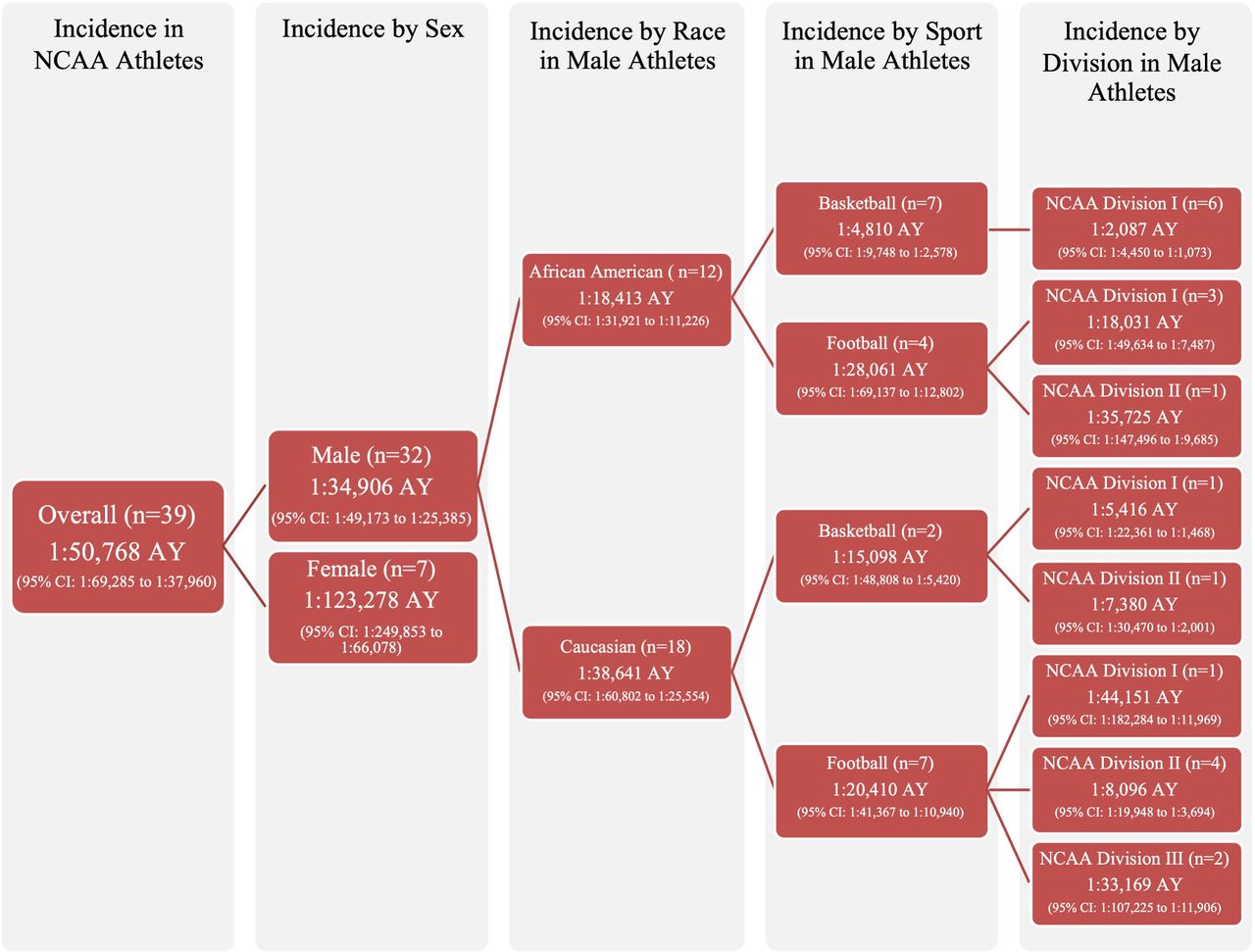
Incidence rates of sudden cardiac arrest and death in NCAA athletes. AY, athlete-years; NCAA, National Collegiate Athletic Association.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidence rate ratios (IRR) of sudden cardiac arrest and death in select athlete populations compared with all high school male athletes. DI, division I, NCAA, National Collegiate Athletic Association.
Discussion
This study provides a contemporary update of the aetiology and incidence of SCA/D in US competitive athletes. In the absence of a mandatory reporting system, a prospective surveillance approach with collaborative efforts among national centres, as described herein, is the most effective strategy at present to monitor SCA/D in US athletes in order to inform prevention strategies.
While records to determine an aetiology were absent in 37% of cases, our study provides important insights into the causes of SCA/D in US athletes using the most complete data possible. HCM was the most common identified disorder across all age levels, accounting for approximately one in five cases, consistent with several prior studies.11 20–22 AN-SUD is the most common finding reported in select populations of SCD in athletes. AN-SUD accounted for 25% of SCD in NCAA athletes and 42% of sports-related sudden death cases referred to a cardiac pathology centre in the UK.1 9 We found AN-SUD represented 1 in 10 (10%) cases in this study. This difference may be related to the inclusion of SCA with survival in 48% of our cases, thus reducing the proportion of AN-SUD in our total cohort.
Our analysis provides important evidence that the causes of SCA/D vary by age. Anomalous coronary arteries accounted for nearly one-third of cases in middle school athletes. Coronary artery anomalies do not typically demonstrate ECG abnormalities but may present with symptoms of exertional chest pain or syncope, suggesting that evaluation of exercise-related symptoms in this age group must exclude anomalous coronary pathology.23 24 Anomalous coronary artery origin can be identified by echocardiography in approximately 90% of cases, but cardiac MRI or CT provide a more detailed assessment of coronary anatomy and should be considered when clinical suspicion remains and the echocardiogram is non-diagnostic. In contrast, cardiomyopathies such as HCM and arrhythmogenic cardiomyopathy represented nearly half of SCA/D cases in college and professional athletes. Other reports have also found HCM and arrhythmogenic cardiomyopathy are the most common causes of exercise-related SCD in athletes.21 22 Cardiomyopathies readily demonstrate abnormalities on a resting ECG.25 Notably, 71% of cases with an established pathological aetiology in college and professional athletes in this cohort were caused by disorders typically associated with ECG abnormalities.25
Our data also support that the incidence of SCA/D varies substantially across athlete sex, race, level of competition and sport. This study demonstrates a higher incidence of SCA/D in male, African-American and college athletes. Two sports, basketball and football, represented over half of call cases. Similar to prior studies, male college basketball players demonstrate the highest risk.1 11 26 Male, African-American, NCAA division I basketball players had an alarming incidence rate of 1:2087 AY. If translated over a 4-year college career, approximately 1 in 500 male, African-American NCAA division I basketball players would suffer a life-threatening cardiovascular event. Indeed, this risk was 21.1 times higher than the average risk in a male high school athlete, although the IRR demonstrated a wide 95% CI (7.6 to 46.7). Similarly, in a prospective cohort of elite adolescent soccer players, the risk of SCA/D was approximately seven times higher in black (1: 3908) vs white (1: 25 880) athletes.27
This study provides a breakdown of the incidence of SCA/D in male high school athletes by states with five or more cases. There were not enough cases to conduct a similar analysis in female high school athletes. It is well recognised that case identification varies considerably by competition level and that media reports remain the largest contributor to case identification at the high school level.11 In NCAA athletes, only 44% of SCD cases in division III athletes and 61% of cases in division II athletes were identified by a systematic search of media reports, compared with 87% of SCD cases in division I athletes.1 Thus, it is likely that all estimates of SCA/D in high school athletes, including in this report, are underestimates and suffer from incomplete case capture. Accepting that media reporting of high school cases is inconsistent and that awareness of reporting mechanisms to the NCCSIR also may vary, we conducted incidence calculations based on state participation (denominator) data provided by the NFHS. Importantly, 13 states had an incidence of SCA/D in male high school athletes greater than 1:50 000 AY. While the small sample size and wide 95% CIs limit definitive conclusions, these results suggest that the risk of SCA/D in male high school athletes may be underestimated in prior studies. More research is needed to determine factors to improve case capture and reporting mechanisms across states.
Our findings provide important insights to guide cardiovascular screening programmes. To date, the existing minimum standard of a preparticipation history and physical examination has shown to inadequately identify at risk athletes with disorders known to cause SCA/D.28–32 There remains controversy, however, on the optimal screening tool for athletes across all groups. Screening programmes must consider the risk of the targeted athlete population as well as the sports cardiology resources and physician expertise available to conduct more advanced screening.28 Effective strategies for cardiovascular screening in athletes also must account for the aetiologies most likely to place the athlete at higher risk of SCA/D.28 Our data support that ECG screening may be most effective in detecting disorders associated with SCA/D in targeted higher-risk athlete groups. Specifically, nearly three-quarters of cases in college and professional athletes would readily display ECG abnormalities.25 For male African-American college basketball players with the highest risk of SCA/D, more intensive screening programmes must become standard.
Ideally, a practiced emergency action plan would be in place for all sports at all levels with access to an athletic trainer and an AED at all practices and competitions.33 However, 52% of SCA cases in this cohort resulted in sudden death. More research is needed to detail the gaps in emergency planning or delays in the recognition of SCA in order to improve outcomes. In addition, a coordinated emergency response may not be an option when events occur outside of organised practice and training. Thus, a multimodal approach that includes primary prevention through informed and targeted screening programmes alongside a comprehensive emergency action plan will be the best way to reduce the greatest number of catastrophic events in athletes.
Limitations
This study is limited by a number of factors, notably the lack of a mandatory reporting system within the USA and difficulty in acquiring records to evaluate aetiology. Although the prospective study design used all available resources for case identification, additional cases of SCA/D within the study population likely went undetected and would have impacted both the aetiology assessment and incidence calculations. Thus, under-reporting or incomplete case identification may have underestimated the overall incidence of SCA/D, and the reported incidences in this study represent minimum figures. Conclusions based on state and sport subgroups should be made with caution due to small case numbers; a limitation that could be addressed through a longer study duration with additional mechanisms to ensure case capture. The quality and depth of autopsy reports also varied widely among medical examiners and access to autopsy reports was subject to state regulations. Given the high variability in postmortem examinations throughout the USA, assessment by a multidisciplinary panel using standardised criteria for athletes was essential for making comparisons and identifying specific causes in this study. Furthermore, information for SCD cases was more readily available in comparison to survivors, as SCA with survival accounted for 47.7% of total cases but only 32.5% of available aetiologies. Additional research and a larger dataset are needed to explore survival rates based on aetiology, demographics, sport type and sport level.
Conclusion
The aetiology of SCA/D in competitive athletes involves a heterogeneous grouping of structural, electrical and acquired cardiac disorders. Cardiomyopathies represent nearly half of all cases in college and professional athletes, whereas coronary artery anomalies are more common in younger middle school athletes. The majority of causes of SCA/D in athletes have recognisable changes on a resting ECG. The incidence of SCA/D varies based on sex, race, participation level, and sport, with male, African-American and basketball athletes demonstrating higher risk. This study also suggests that the incidence in male high school athletes may rival the risk in male college athletes—a finding which requires validation in longer duration studies. These results provide important information about SCA/D in athletes to inform the development of more effective prevention strategies. Improved emergency planning and universal access to AEDs during sport is likely to save lives.
Key messages
What are the findings?
The leading cause of sudden cardiac arrest and death (SCA/D) varies by age: anomalous coronary arteries accounted for 28% of cases in middle school athletes, while cardiomyopathies (hypertrophic, arrhythmogenic, dilated, non-compaction or restricted) accounted for 47% of cases in college and professional athletes.
African-American male National Collegiate Athletic Association Division I basketball players had a greater incidence rate of SCA/D (1:2087 AY) which was 21.1 times higher than the average risk in a male high school athlete.
Seventy-one percent of disorders causing SCA/D in college and professional athletes are associated with ECG abnormalities.
How might it impact on clinical practice in the future?
Effective strategies for cardiovascular screening must account for the aetiologies most likely to cause SCA/D in a specific athlete population.
The evaluation of exercise-related chest pain or syncope in middle school aged athletes must exclude anomalous coronary pathology.
ECG screening to detect disorders associated with SCA/D should be considered in college and professional athletes and targeted higher-risk athlete groups.
Secondary prevention through emergency response planning and access to automated external defibrillators has the potential to reduce fatalities from SCA in athletes.
References
Footnotes
Twitter @DaveMSiebert, @DrKimHarmon, @DreznerJon
Contributors All authors were involved in data collection, analysis, writing and revision of the manuscript. All authors have approved the final version submitted.
Funding Supported by the National Center for Catastrophic Sports Injury Research (University of North Carolina at Chapel Hill), funded in part by the National Collegiate Athletic Association, the National Federation of State High School Associations, the American Football Coaches Association, the National Athletic Trainers’ Association, the National Operating Committee on Standards for Athletic Equipment, and the American Medical Society for Sports Medicine. DFP also received the Alpha Omega Alpha Carolyn L. Kuckein Student Research Fellowship for her work on this study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study was approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill with an IRB nauthorisation agreement with the University of Washington Human Subjects Division.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.