Article Text

Abstract
Objective To scope the relationships between rugby union, and health and well-being.
Design Scoping review.
Data sources Published and unpublished reports of any age, identified by searching electronic databases, platforms and reference lists.
Methods A three-step search strategy identified relevant published primary, secondary studies and grey literature, which were screened using a priori inclusion criteria. Data were extracted using a standardised tool, to form (1) a numerical analysis and (2) a thematic summary.
Results and discussion 6658 records were identified, and 198 studies met the inclusion criteria. All forms of rugby union can provide health-enhancing physical activity (PA). ‘Non-contact’ and wheelchair rugby in particular provide a wide range of physical and mental health and well-being benefits. The evidence is either mixed or unclear in relation to ‘contact’ rugby union and its effects on a range of physical health domains. Injury and concussion incidence rates are high for contact rugby union relative to other sports.
Conclusions A wide range of stakeholders as well as existing and potential participants can use this information to make a more informed decision about participating in and promoting rugby union as a health-enhancing activity. Industry and policy-makers can use this review to inform policies and strategies that look to increase participation rates and use rugby union as a vehicle to contribute positively to population health. Further research understanding rugby union’s contribution to PA as well as to muscle-strengthening and balance is indicated, as well as research examining more health and well-being outcomes across more diverse cohorts.
- rugby
- physical activity
- health promotion
- well-being
- injuries
Statistics from Altmetric.com
Introduction
Rugby union is a team-based sport, played in over 120 countries by over 8 million people.1 Multiple forms of the game exist, with different rules as to the number of players on each side (traditionally 15 or 7), and the degree of contact involved (full contact/non-contact e.g. ‘tag’‘touch’). There are also adapted forms of rugby union for athletes with disabilities, such as wheelchair rugby.
As with many team and individual sports, any form of rugby union can involve moderate-to-vigorous physical activity (MVPA),2 which alongside being ‘non-sedentary’ confers a wide range of physical, mental and social well-being benefits.3–6 Indeed, there are widely published health benefits associated with participating in various individual and team sports,7 8 including improved aerobic fitness, cardiovascular function, metabolic fitness and in some cases reduced mortality.9 Sport is also considered an ‘underused yet important’ contributor to physical activity (PA) and health10 in the World Health Organisation’s (WHO) 2019 Global Action Plan for Physical Activity.
Despite global participation in rugby union, there has not been an overarching review of the evidence on the specific relationships between rugby union, and health and well-being. A systematic review of the potential health benefits of different sporting disciplines7 found 69 studies in total, but only 1 focused on rugby union. Scientific efforts to date have focused mainly on the relationship between rugby union participation and injury. However, given that health (as per WHO definition) is not ‘merely the absence of disease or infirmity’,11 there is a need to consider the potential impact of rugby union participation on health and well-being. Existing as well as potential future participants and various other stakeholders (eg, parents, medical professionals, schools, clubs and unions) need to know the likely benefits as well as the risks to make an informed choice about rugby union participation.12
Therefore, and in line with this approach being used in different sports,13 the aim of this scoping review is to inform participation, policy, advocacy and research strategy by:
(1) Identifying the relationships between rugby union and various health and well-being outcomes.
(2) Identifying evidence gaps and key research priorities for rugby union and health and well-being.
Methods
A scoping review was considered the most appropriate methodological approach to address this aim, especially given the iterative nature of researching what is a novel topic. Scoping reviews are a type of review that seek to identify the nature and extent of research evidence for a given topic, in comparison to, for example, systematic reviews that seek to provide an exhaustive appraisal and synthesis of research evidence.14 Scoping reviews are, therefore, characterised as broad in nature, and are often focused on mapping key concepts that underpin research areas, and detailing the range of evidence available for a certain topic.15–17
This scoping review is based on Arksey and O’Malley’s five-stage scoping review process, and informed by Levac et al’s framework, as well as the work of the Joanna Briggs Institute and previously published relevant scoping reviews.13 15–18 The protocol was published in an open-access journal.19 See online supplementary appendix 1 for the completed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-Scoping Review (ScR) checklist.20
Supplemental material
Stage 1: identify the research question(s)
Following a preliminary literature search and discussions between the author groups, the following research questions were developed to reflect the population, context and content of the review.
What is known about the relationships between rugby union, and health and well-being?
What are the evidence gaps in the field?
What are the key research priorities in the field?
Stage 2: identifying relevant studies
The a priori inclusion and exclusion criteria (table 1) were determined based on existing frameworks and discussions within the research group.13 18 Essentially, we wanted this scoping review to include a broad range of studies that included participants of any population involved in rugby union, in any capacity, with studies not limited by factors such as age or language. Owing to the iterative nature of the scoping review, important elements of our methods should be noted.
Inclusion and exclusion criteria
A decision was made to limit studies to those referring to ‘rugby union’ only, and to report on the outcomes by the type of rugby union referred to in the studies (contact/non-contact/wheelchair). Following author group discussion, it was decided that given at a practical level, non-contact forms of rugby union and rugby league are identical and played under the same rules, these would be treated as the same, and as such studies relating to ‘non-contact’ forms of rugby league would be included in the analysis. We did not extend this principle to ‘contact’ forms of rugby league for several reasons. First, our initial limited search returned a volume of material for both rugby league and rugby union that was beyond capacity for this scoping study. Second, in regard to contact forms of rugby league and rugby union, there are inherently different rules, patterns of play and demands between both sports that limit comparability.
In regard to injuries, given the volume of research, and focus in this area, a decision was made to limit injury studies to systematic reviews (as per the published protocol).19 This has allowed us to report review-level evidence on this topic, using previous syntheses conducted by other author teams, as has been done before in different subject areas.21 One potential approach considered was to exclude studies in which the outcome variables are injuries or other acute health problems (as per previously published systematic reviews).7 However, we decided that this approach might overlook a key concern that the author group’s professional experience tells us is critical to stakeholders, and would limit the applicability of this scoping review.
Search strategy
The three-step search strategy (an initial limited search, followed by the identification of key words and index terms, and then further searching of references and citations) using eight research databases is summarised in online supplementary appendix 2. The eight databases searched included: Medline, Embase, PsycINFO, SPORTDiscus, Web of Science Core Collection, Google Scholar, ProQuest Dissertations & Theses Global and WHO—International Clinical Trials Registry Platform.
Supplemental material
Stage 3: study selection
Relevant titles and abstracts identified by the search strategy were evaluated against the eligibility criteria by the lead author (SAG). NKPP subsequently completed the same process on a random sample of 20% of titles and abstracts, using the same inclusion and exclusion criteria, with 97% overall concordance (defined as percentage positive agreement between authors). SAG then reviewed the titles and abstracts of all other studies and sourced the full text for all articles meeting the inclusion criteria. Authors were contacted where full texts were not available.
Stage 4: charting the data
SAG and NKPP designed a data extraction form (see online supplementary appendix 3). SAG and NKPP trialled the data extraction form on 5 randomly selected studies, and independently extracted data from the first 10 studies to determine whether their approach to data extraction was consistent with the research question and purpose. Following this step, SAG extracted data from 90% of included studies and NKPP extracted data from 10% of studies. SAG checked 10% of NKPP’s data extractions for accuracy and vice versa,19 with 96% overall concordance. As per a previously published scoping review in a relevant field, no further cross-checking was performed given the high level of concordance.13 18
Supplemental material
Stage 5: collating, summarising and reporting the results
Data are presented in the following formats:
Numerically, alongside a scoping review flowchart. The data are presented by theme (see description below), period of publication, country of origin and study type.
Thematically, using a descriptive analysis to map key findings and concepts relevant to the research question. SAG used an inductive thematic analysis framework, and based the analysis on Braun and Clarke’s six-phase framework.22 Familiarisation with the data was achieved by manually extracting key data from individual studies. These were then individually categorised according to the primary focus and main outcome measures. These categories were then grouped to form themes, which were subsequently reviewed and refined to include subthemes where appropriate.16 22 23 A visual summary of this process is provided in figure 1. Where a vast number of studies were assigned to a specific theme (as can be seen in online supplementary appendix 4) priority would be given to reporting the results from studies that the authors believe are most relevant to some of the afore-mentioned stakeholders and policy-makers, or where more ‘gold-standard’ outcome measures were used, or where certain patterns were clear from the data. In cases where individual studies are highlighted, we have also tried to highlight any methodological issue(s) associated with them that may impact the real-world applicability of the data.
Supplemental material
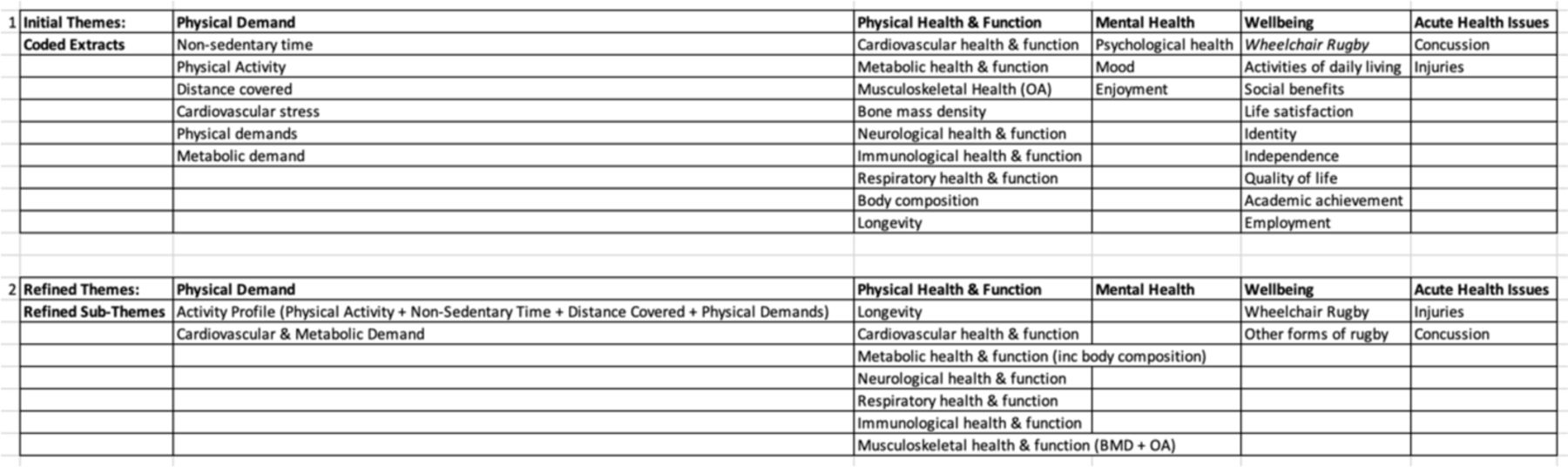
A summary of how themes were generated, based on Braun and Clarke’s six-phase framework. *OA (osteoarthritis)
(Optional) stage 6: consultation
The author group have been involved with the sport of rugby union in many different forms. We authors have played, coached and been responsible for the medical care of professional rugby union players. Similarly, there is extensive experience within the group in not only conducting health and well-being research specific to rugby, but also in sport, physical activity and public health in general. Multiple members of the group are also employed by and advise the board of two of the UK’s national rugby governing bodies (Rugby Football Union and Scottish Rugby Unionn (RFU and SRU)), as well as have roles in advising about physical activity and sport at a governmental level. Given the breadth of knowledge and experience within the group in working with key stakeholders as such, we did not host an external consultation exercise, though we will be involving additional groups in both the dissemination phase of this project, and in future studies (which are currently in the planning process).
Results
Numerical analysis
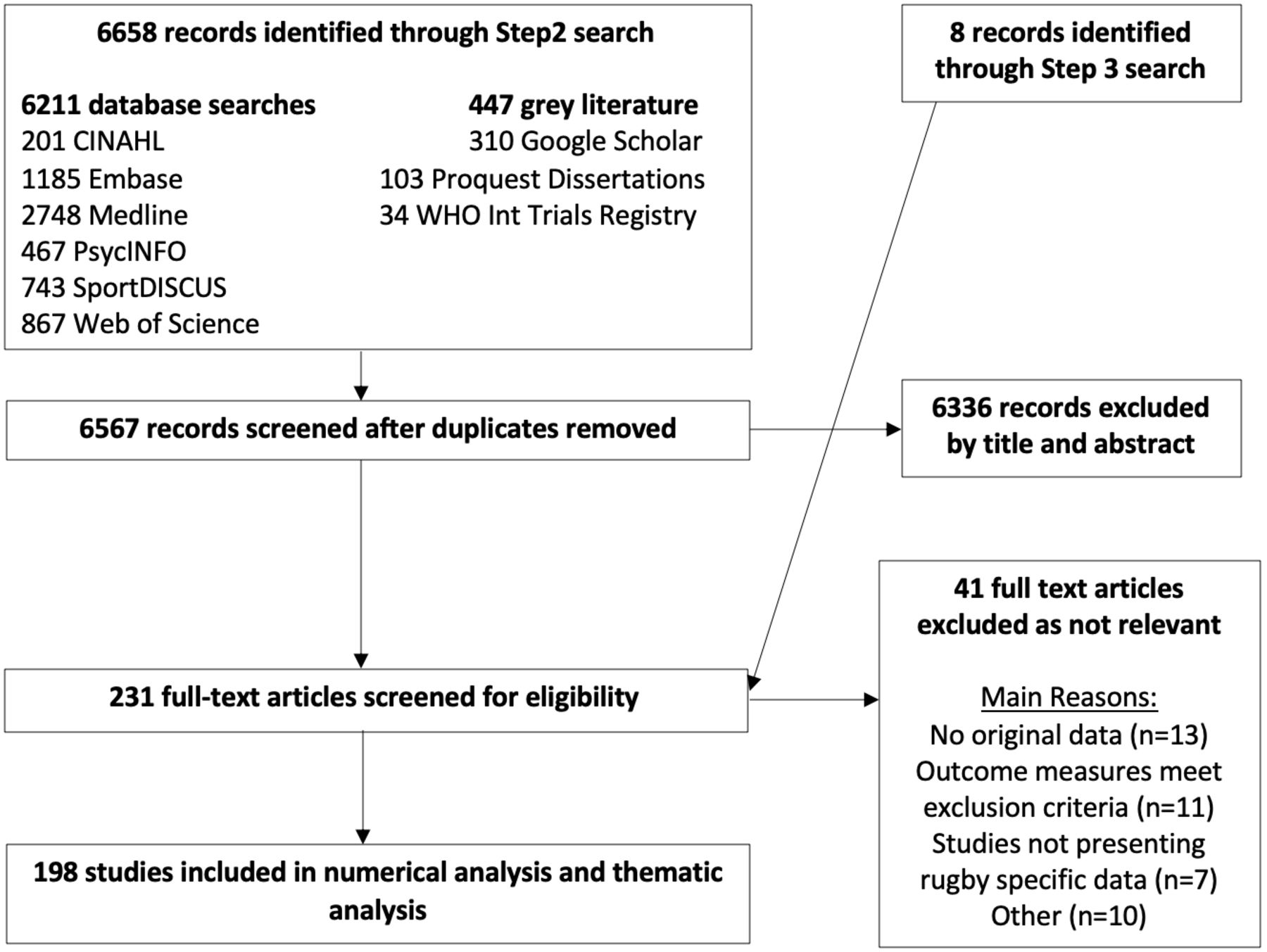
The initial search identified 6658 studies, 6211 of which came from recognised databases and 447 from grey literature. Six thousand five hundred and sixty-seven studies remained after further duplicates were manually removed from the search. Six thousand three hundred and thirty-six studies did not meet the inclusion criteria. Of the 231 identified studies, 41 were deemed irrelevant and removed following full text review (with reasons provided in the flowchart—figure 2). Eight additional studies were included following further searches of references and author consultation. Overall, 198 studies met inclusion criteria and were included in the analysis. The scoping review flowchart details the search and study selection process (figure 2).

Scoping review study selection flowchart.
Chronology and geography of included studies
Figure 3 highlights the substantial chronological increase in the number of related studies, with a rate of increase greater than that seen in the only comparable review in golf and health.13 Geographically, table 2 demonstrates the contribution per continent, and the country in each continent with the largest contribution to the literature. Europe provided the majority of included studies (47%), and the UK was the main contributor within this region (n=41 studies). Australasia (16%), North America (15%) and Africa (11%) were other major contributors. South Africa contributed all of the included studies within the African continent. Asia (7%) and South America (5%) provided a low proportion of the overall included studies, in keeping with the recognition that these are generally considered less established rugby union markets.24 All of the 198 final studies were published in English, despite the sizeable contribution from a diverse range of countries where English would not be considered the native language.

Included studies by year of publication.
Geography of included studies
Type of studies
Table 3 details the type of studies included in the review.
Type of studies included
Themes identified
Studies fell within five broad themes:
Rugby union and physical activity (n=51).
Rugby union, physical health and function (n=95).
Rugby union, mental health and function (n=11).
Rugby union and well-being (n=21).
Systematic reviews of rugby union injuries or acute health issues (n=20).
Thematic analysis
Theme 1: rugby union and physical activity
Fifty-one studies reported on the level/volume/amount of PA conducted while playing rugby union across different levels and formats of the game. The majority of this research was performed in men’s rugby union, with a relative lack of research breadth and depth in women’s rugby union across all formats of the game (70% vs 14% of studies respectively). Most research focused on adult (18 years and older) rugby union, with 12% of studies primarily involving youth athletes.
Contact rugby union (15-a-side (15s), 7-a-side (7s), etc)
Data from one study (with ambiguity over participant number, gender and analysis) suggests that traditional 15s rugby union has a mean metabolic equivalent of task (MET) value of 8.3 (8.1–8.5),2 classifying it as a vigorous form of PA. Various cross-sectional studies also show that training and matches in 15s and 7s (across both men and women’s rugby union) provide a strenuous cardiovascular stimulus,25–28 with 7s matches (which are shorter in duration than 15s matches) providing a more intense cardiovascular stimulus than 15s.29
Non-contact rugby (touch, tag, etc)
Cross-sectional data from a population of 101 male and female 11–14 year olds indicates that touch and tag rugby have MET values of 6.3 (5.6–7.2)2 and 6.0 (4.5–7.5),30 respectively, which correspond to vigorous-intensity PA. A cross-sectional study of 16 male touch rugby players showed that they spent approximately 75% of time at over 80% of maximal heart rate (HRmax) during match play.31
Wheelchair rugby
Wheelchair rugby has a MET value of 3.8–4.3 (dependent on position) according to a cross-sectional study involving 52 male participants32. This would correspond to moderate-intensity PA using able-bodied cut-off scores, though the relative intensity may be different in this population relative to the parameters generally promoted in able-bodied populations. Wheelchair rugby players have also been shown to spend up to half of match play at above 90% of HRmax, which the authors of the paper suggest is sufficient to generate improvements in cardiorespiratory parameters in this population.33
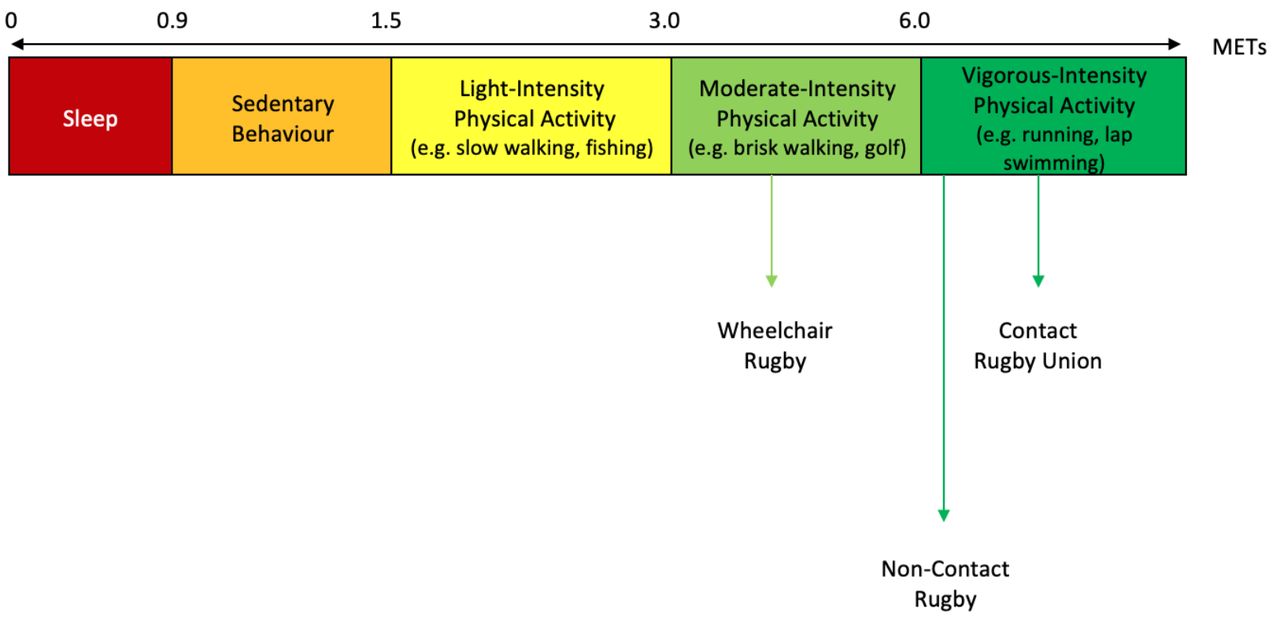
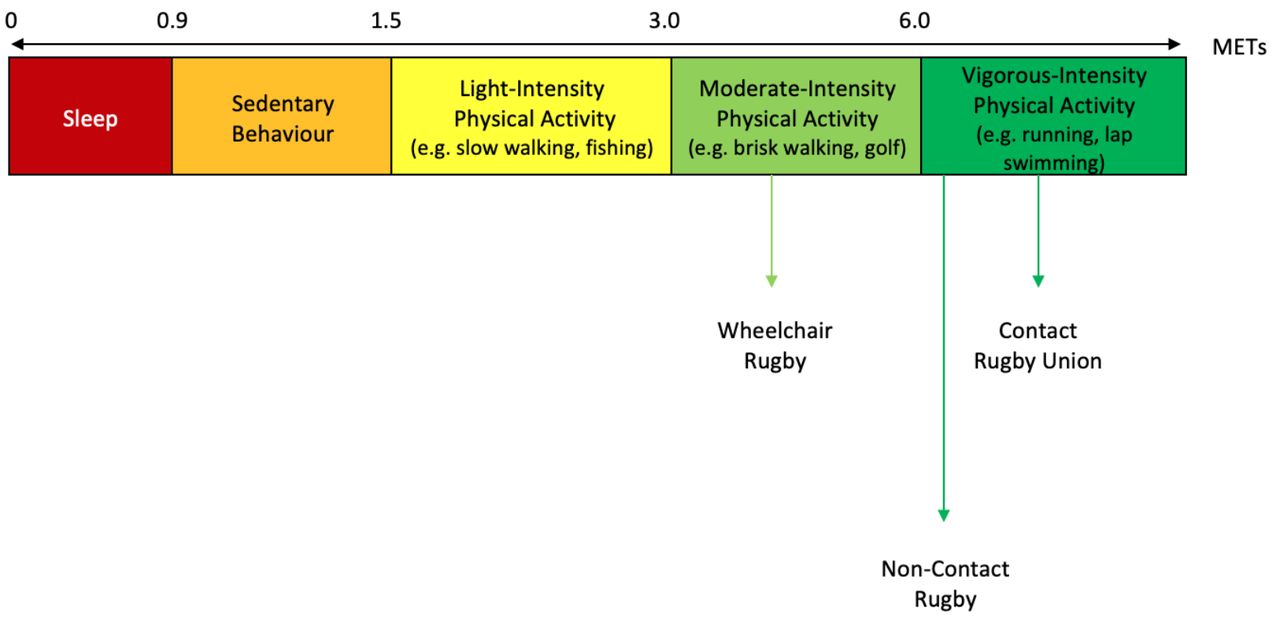
The MET values for the various forms of rugby union are shown below in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MET values attributed to different forms of rugby union. Light-intensity activities are defined as 1.1 METs to 2.9 METs, moderate-intensity activities are defined as 3.0–5.9 METs, and vigorous-intensity activities are defined as 6.0 METs or more. *MET (metabolic equivalent of task)
The majority of studies (n=32) described the movement profile (eg, distance covered, time spent moving) associated with various forms of rugby union, with all showing that rugby union participation results in important contributions to these indices of PA.25 28 34–63 This review did not find any studies that explored an association between rugby union participation and muscle-strengthening and balance improvement. National population surveys, however, typically ‘count’ rugby union as an activity that can provide muscle-strengthening/balance improvement when accrued for period of over 10 min.64–67 There is also non-rugby union-specific evidence that ‘ball sports’ can improve muscle function, bone health and balance.68 69
Theme 2: rugby union, physical health and function
Contact rugby union (15s, 7s, etc)
Cardiovascular health and function
One cross-sectional study comparing a cohort of 259 retired elite rugby union players to the general population (using data from the English Longitudinal Study of Aging (ELSA)), found that the incidence of high blood pressure was significantly lower in former rugby players when adjusted for age.70 This is consistent with another cross-sectional study among 52 retired international rugby union players, that reported a lower frequency of chronic cardiovascular disorders in this cohort relative to controls (matched for both age and social deprivation).71 This evidence base is contrasted somewhat by the results of cross-sectional studies among over 200 veteran rugby union players from 10 countries, that demonstrated a higher incidence of hyperlipidaemia and hypertension compared with the Australian general population.72–74 However, it is not clear whether these cohorts were consistently matched in terms of age and gender, or measures put in place to account for the significantly higher relative body mass index among veteran rugby union players, which might skew the results.73 Similar contrasting findings exist for the effect of rugby union on lipid profile.75–79
Metabolic health and function
The relationship between rugby union and metabolic health and function is similarly unclear. In standardised morbidity ratio analyses of 259 retired elite male players aged over 50 years, diabetes rates were significantly lower compared with ELSA participants.70 Again this is in contrast to the higher metabolic risks reported among the previously mentioned cohort of veteran rugby union players, who had a higher incidence of diabetes relative to an age-matched Australian control group.73
Musculoskeletal health and function
The prevalence of osteoarthritis and rates of joint replacements are significantly higher among both former elite players80 81 and former amateur players82 relative to the general population. Data suggests an association between rugby union participation and increased bone mass density (BMD), especially when compared with both sedentary controls and athletes from other sports.83–90 Both cross-sectional and longitudinal epidemiological studies, however, have shown that increased BMD may be considered as part of the osteoarthritis spectrum,91 and one cross-sectional study reported a significant increase in osteoporosis among a retired elite male cohort.70 One area of particular academic interest is degenerative lesions of the cervical spine (especially among front-row rugby union players).92–96 While all studies reported premature and advanced changes of degenerative disease, these changes did not always manifest themselves clinically or affect activities of daily living.93 95
Neurological health and function
Research on potential neurological sequelae comprised nearly a third of the studies categorised under the ‘physical health’ theme (31%). Overall, there are mixed reports regarding long-term cognitive function and neurological health in retired able-bodied rugby union players. A systematic review on this topic reported normal objective neuropsychological performance in retired rugby union players across most cognitive domains (apart from fine motor control), and also that the evidence is generally both ‘inconclusive and poorly developed’.97 For current players, findings are similarly mixed, with some studies reporting reduced cognitive function and cognitive vulnerability following exposure to rugby union,98–104 while other studies do not.71 105–110
Immunological health and function
Data from a study involving 40 elite male players suggest that they have a more favourable gut microbiota relative to sedentary individuals, which is linked with a wide range of immunological health outcomes.111 However, they may be more susceptible to infection over the course of the professional season due to suppressed immunity and the sustained activation of their inflammatory response.112
Non-contact rugby (touch, tag, etc)
Cardiovascular health and function
Two small observational studies suggest that regular participation in touch rugby over a 10–12-week period has clinically favourable effects on cardiovascular risk factors (including resting heart rate and diastolic blood pressure).113 114 In one randomised control trial (RCT) of active men, the effect sizes across similar domains were greater than those reported in a group whose PA was prescribed as self-paced interval running.115 One RCT in a cohort of thirty-three sedentary men also demonstrated improvements in submaximal VO2 (rate of oxygen consumption) compared with a sedentary control group.116
Metabolic health and function
There is some evidence that suggests that participating in touch rugby improves metabolic risk factors. Using an RCT design in a cohort of 33 middle-aged inactive men, touch rugby was associated with improvements in metabolic risk factors associated with the prevention of type 2 diabetes mellitus, including VO2 at 80% HRmax, glycated haemoglobin levels and total body fat mass.117 These effect sizes were found to be similar to those provided by a continuous cycling training programme.117 Prescribing touch rugby as a mode of PA in a small (n=10) sedentary male Indigenous Australian population also increased engagement in PA and assisted in the acute regulation of glucose disposal.118 Similarly, a varied activity programme that included rugby (alongside other sports, circuit-based aerobics, strength and resistance exercises) also led to an improvement in metabolic and cardiorespiratory fitness among 22 obese children.119
Immunological health and function
Data from a small (n=9) RCT suggest that small-sided touch rugby games stimulate and maintain an acute anti-inflammatory response similar to that provided by stationary cycling, though there are no data to support an association between this and illness or injury risk.120
Wheelchair rugby
Cardiovascular health and function
Data from 14 high-level wheelchair rugby athletes suggest that wheelchair rugby participants have a higher aerobic capacity relative to untrained quadriplegics.121 Regularly participating in upper-body sports activities such as wheelchair rugby has also been associated with long-term reductions in carotid atherosclerosis122 and improved serum lipid profiles75 relative to sedentary controls.
Musculoskeletal health and function
One study investigating the longitudinal effects of wheelchair rugby training on the body composition of 13 subjects with quadriplegia demonstrated that regular participation in wheelchair rugby training increased lean mass, and decreased total body fat mass.88
Neurological health and function
Data from a study comparing 19 physically active wheelchair rugby athletes at the 2015 Parapan American Games to 9 relatively inactive spinal cord injury controls suggest that physically active wheelchair rugby participants exhibit improved dynamic cerebral autoregulation and cognitive function.123
Respiratory health and function
Participation in wheelchair rugby over the course of 12 months has been linked to a reduction of respiratory dysfunction in a cohort of 10 quadriplegic athletes.124 Wheelchair rugby athletes with quadriplegia have also been shown to have enhanced respiratory muscle strength and thoracic mobility relative to sedentary quadriplegic controls (with no significant difference between levels of spinal cord injury between the two groups).125 A small (n=15) group of male subjects with quadriplegia who underwent 12 months of regular wheelchair rugby training also significantly improved their pulmonary function relative to sedentary quadriplegic subjects.126
Theme 3: rugby union, mental health and function
Contact rugby union (15s, 7s, etc)
Two studies investigated symptoms of common mental disorders among retired professional rugby union players.127 128 One cross-sectional study among 295 retired professional rugby union players reported a prevalence rate of 28% for anxiety/depression, which is generally above that reported in the general population worldwide (12%–25%).128 Within a current elite male rugby union playing cohort, one study of 990 players found that when matched for age and gender, the prevalence of symptoms of anxiety/depression seems slightly higher than in other general/occupational populations.129 An observational prospective cohort study in a cohort of 595 professional rugby union players reported incidence rates of symptoms of common mental disorders similar to those of professional athletes from other sports.130
Non-contact Rugby (Touch, Tag etc)
No relevant studies found.
Wheelchair rugby
A cross-sectional study that collected data from 150 males with quadriplegia at various wheelchair rugby tournaments found that practicing wheelchair rugby 2 times or more a week (compared with once a week or less) was significantly associated with lower depressive symptomology and perceived stress.131
Theme 4: rugby union and well-being
The majority (57%) of studies were performed in a wheelchair rugby union setting.
Contact rugby union (15s, 7s, etc)
A qualitative study among 15 veteran male players aged 54–83 years investigating the motivation to continue playing, reported that playing gave participants ‘a sense of nostalgia and pride’, ‘lifelong friendship and belonging’, ‘pure joy and passion’ and helped them be ‘mentally and physically active’.132 ‘Making friends’ was also reported as a main motivation for playing rugby union among amateur male players aged over 35 years.133 A cross-sectional study among 339 female rugby players reported that they played rugby because ‘they enjoy the game, they like the aggressive aspects of the sport, they appreciate the social aspects of the game, and they believe the sport provides them with positive benefits, such as increased fitness, confidence and strength’.134
Three studies investigated academic achievement among adolescent rugby union players.135–137 One observational study in Ireland reported no statistically significant difference to the final Leaving Certificate Score among students who participated in rugby union.136 A retrospective analysis among 30 adolescent South African students found ‘no conclusive evidence’ that rugby union players perform statistically worse in their academic achievement relative to students who had not played rugby union.135
Non-contact Rugby (Touch, Tag etc)
No relevant studies found.
Wheelchair rugby
The data from all relevant studies (n=12) suggest a beneficial effect of wheelchair rugby on numerous proxy measures of well-being including quality-of-life,138 self-esteem,138 139 self-identity,139 functional independence,139 140 autonomy141 and improvements in activities of daily living.139 142 143
Theme 5: rugby union and injuries or acute health issues
We found 20 systematic reviews reporting on concussion and acute health issues associated with rugby union. Four of these directly concerned concussions and the remainder concerned a wide variety of injuries. Over half (55%) of the studies directly reported on male-only cohorts, six on mixed cohorts, one on a female-only cohort and two did not directly specify the cohorts investigated. While there has been a targeted effort to standardise the definition on injuries in rugby union,144 there is still some heterogeneity which potentially distorts the true incidence, and could affect the applicability of the data.
Contact rugby union (15s, 7s, etc)
The overall incidence of injuries in senior men’s professional rugby union matches was 81 per 1000 player match-hours,145 and 46.8 per 1000 player match-hours within senior male amateur rugby union players.146 The incidence of time-loss injury in male adolescent rugby union players was lower than in senior male professional players but higher than in adolescent athletes in other sports.147 Injury incidence rates in elite men’s 7s matches are higher than those reported for 15s at the same level of competition, while injuries are also more severe.148 The injury incidence in women’s 15s and 7s was lower than men’s professional 15s and 7s competitions but similar to men’s youth 15s, with a pooled incidence in women’s 15s of 19.6 per 1000 player match-hours.149
In regard to concussion, the results of one meta-analysis150 revealed an overall incidence in men’s and women’s 15s of 4.73 and 0.55 per 1000 player match-hours, respectively. In men’s 7s, concussion incidence was 3.01 per 1000 player match-hours. The incidence of concussion varied considerably between levels of play, with elite men’s 15s recording a rate of 0.40 concussions per 1000 player match-hours, schoolboy 15s 0.62 concussions per 1000 player match-hours (consistent with data reported elsewhere151), and men’s community or subelite 15s recording a rate of 2.08 concussions per 1000 player match-hours. The concussion risk in rugby union was reported as higher relative to other sports in two systematic reviews;152 153 however, the authors of one suggest that this may be attributable in some degree to continuing efforts to increase awareness and implement strict concussion policies regarding reporting and removal from play.153
Non-contact Rugby (Touch, Tag etc)
No relevant studies found
Wheelchair rugby
We found one systematic review relating to injury profile in wheelchair rugby, which investigated the acute and chronic musculoskeletal injury burden of para sport.154 It reports that wheelchair rugby is one of the ‘highest risk sports’ for upper limb injuries.
Discussion
We aimed to identify the relationships between rugby union and various health and well-being outcomes, as well as identify priorities for further research in the area. This is the first scoping review of rugby union and health and well-being, and as such comparisons are limited. However, the findings of this review are in keeping with the findings of a scoping review on golf and health,13 in that the available evidence suggests rugby union can provide health-enhancing MVPA. Specific risks associated with rugby include musculoskeletal injury and concussion, which appear to be highest in the professional game. This review also supports previously published reviews that associate sport with a range of health and well-being benefits.7 9
Strengths and limitations
This scoping review provides an appropriate broad overview of the research area, but a number of potential limitations may affect its applicability. While we tried modelling the review on the PRISMA-ScR checklist,20 some of the suggested steps were not feasible within the context of this review. Given the vast number of studies identified by the search strategy, and the timeline and capacity of the author group, we were unable to ensure that two of the authors independently screened 100% of the potentially relevant studies and subsequently extract 100% of the data from the included studies. Similarly, while we tried using broad search terms in the search strategy across all databases to capture all relevant studies (especially relating to well-being), we realise that our search terms may have led to us overlooking studies using more subtle psychosocial outcome measures. While we feel that our methods enabled us to find these elsewhere (eg, in the reference lists of other studies), this is something we feel needs raising.
Scoping reviews do not formally assess the methodological quality of individual studies, though we have tried to highlight significant or recurrent methodological issues encountered when critiquing individual or groups of studies. Significant variety exists as to the scientific rigour and methodological quality of individual studies, especially in relation to cross-sectional studies where populations are sometimes poorly defined, and it is not always clear if control groups have been appropriately matched. Similarly, many of the studies have a small sample size, introducing potential error in interpretation. Another limitation that needs considering in regard to injury data is that we did not have the capacity to formally critically appraise the individual studies that make up the systematic reviews, and as such the data should be interpreted in this context.
Despite these limitations, our chosen approach has enabled us to not only address the primary research questions identified in the protocol, but also to summarise the evidence in a format that is useful for policy-makers and other relevant stakeholders.
Conclusions and implications for:
Existing/potential participants
Given the findings that rugby union can provide health-enhancing PA, participants could benefit from a range of associated benefits, including a lower risk of developing type-2 diabetes mellitus, various forms of cancer,3 155 156 stroke and heart disease,3 as well as a lower risk of depression.65 157 158
To enable comparison against national and international guidelines for PA,10 65 154 table 4 summarises how rugby union may relate to the four PA-related domains that comprise these guidelines. Further high-quality research is required to be able to concretely determine rugby union’s exact contributions to these PA domains, however, especially in regard to less ‘traditional’ playing populations across more diverse contexts and countries.
How rugby union may contribute to national and international physical activity (PA) guideline domains
There is evidence to support a positive relationship between both non-contact and wheelchair rugby in particular and physical health outcomes across a wide range of domains. As such, these forms of the game could be actively advocated as health-promoting activities across the general population. The evidence base is generally mixed or less clear for contact forms of rugby union.
Despite relatively fewer studies, the relationship between rugby union and both mental health and well-being is generally positive, especially in non-professional settings. Wheelchair rugby in particular has strong wide-ranging mental health and well-being benefits.
Contact rugby union has high injury and concussion incidence rates relative to other sports across the spectrum of participation.
Industry and policy-makers
Industry and policy-makers can use the findings of this scoping review to inform current as well as future participants (and associated stakeholder groups such as parents and teachers) about the association between rugby union, and health and well-being. Outside of wheelchair rugby (which has a generally strong supporting evidence base), there is stronger (though still limited) evidence to suggest a beneficial association between non-contact forms of rugby union and health and well-being, at a reduced ‘injury cost’ across the spectrum of participation relative to contact forms of the game. From a population health perspective as such, industry and policy-makers could look to further embrace elements of these formats across the playing population to potentially increase participation (especially if current injury rates are deemed as a significant barrier by some stakeholders). While gaps in the research exist that preclude any insight into the potential effect of such a shift, it could be considered a low-risk approach to take given the current climate and conversation around contact/collision sports.
Researchers
This study has identified several gaps in the available literature (box 1). Addressing these research priorities would substantially further understanding of the relationship between rugby union, and health and well-being.
Relevant research priorities identified
To expand understanding of the physical activity (PA) profile of various forms of rugby union, especially in women’s, youth, amateur and veteran cohorts.
To establish the contribution of rugby union to muscle strength, balance and coordination.
To establish the PA profile of other groups involved with the game (eg, referees, coaches, supporters).
To establish current drivers, barriers and effective interventions for rugby union participation across the spectrum of participation (given the evidence for health benefits). This should take into account the views of multiple stakeholders (players, parents, schools, healthcare professionals), especially in non-contact and wheelchair forms of the game.
To establish the short-term and long-term effect of rugby union participation on a range of physical health domains (e.g. neurocognitive health and function), especially in contact rugby union among amateur and women’s players.
To establish the potential effect of various forms of rugby union on mental health and well-being (especially psychosocial) markers, in particular among amateur, women’s and non-contact players.
To establish the injury profile of non-contact and wheelchair rugby, as well as continue with current injury surveillance efforts in women’s and amateur contact rugby union.
To broadly compare the health and well-being outcomes associated with rugby union, to other sports or physical activities.
What is already known?
Scoping reviews provide a useful framework to summarise information on a broad topic.
Rugby union is a worldwide sport with a diverse participant base.
What are the new findings?
All forms of rugby union (contact, non-contact, wheelchair) could be considered as evidence-based ways of providing health-enhancing moderate-to-vigorous physical activity, which is linked to a wide range of health and well-being benefits.
More research is needed as to the relationship between contact rugby union and physical health, but there is strong evidence showing a wide range of physical health benefits for non-contact forms of rugby and wheelchair rugby in particular.
There is a generally positive relationship between most forms of rugby union and both mental health and well-being, especially in wheelchair rugby, though further research is required outside of the wheelchair rugby setting.
Across the spectrum of participation, contact rugby union has high injury and concussion incidence rates relative to other sports, highest at the professional level.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @SteffanGriffin, @nim_perera, @docandrewmurray, @drsimonkemp, @drkeithstokes, @narrowboat_paul
Correction notice This article has been corrected since it published Online First. The second author's name has been corrected.
Contributors SAG proposed the review. SAG, AM, KAS and SK identified the method and identified the framework for the review. SAG, AM, NPP and CH proposed the search strategy. All authors contributed to the development of the research questions and the study design. All authors developed the first and subsequent drafts of the manuscript, then subsequently reviewed and approved the final manuscript.
Funding This project formed part of SAG’s work with the Department of Primary Care and Public Health at Imperial College London, a remunerated post, as well as SAG’s work as a Sports Medicine Training Fellow at the Rugby Football Union. NPP is funded from the Centre for Sport, Exercise and Osteoarthritis Research Versus Arthritis (sports grant number: HFR02510).
Competing interests SAG receives remuneration for clinical work in professional rugby union, and is employed by the Rugby Football Union as a Sports Medicine Training Fellow. AM receives remuneration from Scottish Rugby Union for clinical work. SK is employed by the Rugby Football Union as medical services director. KAS is employed by the Rugby Football Union as medical research lead.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.