Article Text

Abstract
Objective The aim of this systematic review was to investigate the effect of exercise-based programmes in the prevention of non-contact musculoskeletal injuries among football players in comparison to a control group.
Design Systematic review and meta-analysis of randomised controlled trials.
Data sources MEDLINE, EMBASE, CENTRAL, CINAHL, PEDro and SPORTDiscus databases were searched from the earliest record to January 2021.
Eligibility criteria Studies were eligible if they (1) included football players aged 13 years or older, (2) used exercise-based programmes as intervention, (3) presented the number of non-contact musculoskeletal injuries (ie, defined as any acute sudden onset musculoskeletal injury that occurred without physical contact) and exposure hours for each group, and (4) had a control group (eg, usual training, minimal intervention, education). All types of exercise-based prevention programmes were eligible for inclusion. Risk of bias for each included study and overall quality of evidence for the meta-analysis were assessed.
Results Ten original randomised controlled trials with 13 355 football players and 1 062 711 hours of exposure were selected. Pooled injury risk ratio showed very low-quality evidence that exercise-based prevention programmes reduced the risk of non-contact musculoskeletal injuries by 23% (0.77 (95% CI 0.61 to 0.97)) compared with a control group.
Conclusion Exercise-based prevention programmes may reduce the risk of non-contact musculoskeletal injuries by 23% among football players. Future high-quality trials are still needed to clarify the role of exercise-based programmes in preventing non-contact musculoskeletal injuries among football players.
PROSPERO registration number CRD42020173017.
- soccer
- exercise
- sporting injuries
- football
- injury prevention
Statistics from Altmetric.com
Introduction
Football (soccer) is one of the most popular sports worldwide. It is estimated that more than 250 million men and women, from children to elderly, with different socioeconomic backgrounds and levels of expertise, play football.1 2 Besides the well-known health benefits of sports participation,3–6 there is an increased risk of musculoskeletal injuries. Injury rate among professional and amateur players may vary. Previous research has shown that injury rates among amateurs and professionals are 9.6 and 8.1 per 1000 hours of exposure, respectively,7 8 and up to half of these injuries are muscle injuries.9
Although football is a sport with frequent physical contact, occurrence of non-contact musculoskeletal injuries, such as hamstring strain and anterior cruciate ligament (ACL) rupture, is common.10 There is evidence showing that more than 90% of all muscle injuries and 51%–64% of joint/ligament injuries (ie, ACL) in football occur in non-contact situations.11–13 Lower limb injuries are the most common type of injury in football and most of these (66%) are non-contact injuries and, therefore, preventable.14 Recovery from non-contact injury depends on the type and severity of injury but often requires athletes to take time off from sports. For instance, an acute hamstring strain (grade I or II) may take up to 8 weeks of rehabilitation,15 while time loss following an ACL injury is ~7.5 months.12
Sport injuries can affect the athlete’s physical and mental health and, consequently, impact team’s performance.16–19 Professional teams lose approximately £45 million (~US$55 million) per season due to injuries from 2012 to 2017.20 To reduce absence from training and competition, interventions to reduce injuries among football players have been developed.21 22 One of the available intervention programmes for football players is the general (ie, targeting multiple body parts) exercise-based programme FIFA 11+.23 This general programme has been shown to reduce overall injury rate by 39%.22 Focused programmes, comprised of exercises targeting a specific muscle group (eg, the Nordic Hamstring Exercise (NHE)), may provide extra protection for the targeted tissue21 as it is shown to reduce the risk of hamstring injury by 46% among amateur football players.24 Despite the burden of non-contact musculoskeletal injuries to athletes and their teams, the efficacy of focused and general exercise-based programmes to prevent non-contact musculoskeletal injuries and the overall incidence rate of such injuries remains unclear.
Previous systematic reviews investigating exercise-based programmes to prevent injuries in football players combined data from all types of injuries and/or interventions.22 25–28 Given that the injury profile and incidence vary across teams and leagues,29 30 it would be informative to estimate the efficacy of exercise-based programmes, including focused and general exercise programmes, specifically for preventing non-contact musculoskeletal injuries. In addition, informing injury incidence of non-contact injuries would contribute to the development of future interventions. This information may be incorporated in pre-season and during-season training plans.
To the best of our knowledge, there is no systematic review assessing the efficacy of exercise-based programmes in the prevention of non-contact musculoskeletal injuries among football players. The primary aim of this systematic review and meta-analysis was to evaluate the effects of exercise-based programmes in the prevention of non-contact musculoskeletal injuries among football players in comparison with a control group. In addition, we aimed to (1) investigate whether there are differences in the estimates between focused and general exercises on the prevention of specific non-contact injuries, and (2) report the injury incidence of non-contact injuries using data from control groups.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were followed for reporting of this review.31 The protocol for this review was prospectively registered in the PROSPERO database (CRD42020173017).32
Search strategy and inclusion criteria
The search for relevant studies was performed in six databases (MEDLINE, EMBASE, CENTRAL, CINAHL, PEDro and SPORTDiscus) from the earliest record to 10 March 2020 and updated on 14 January 2021. Clinical trial registries, such as clinicaltrials.gov, the International Standard Randomised Controlled Trial Number Register (IRSCTN) and the Australian–New Zealand Clinical Trials Registry (ANZCTR), were also searched for potential ongoing or unpublished trials. The search strategy used a combination of terms related to football, soccer, prevention and randomised controlled trial (online supplemental table 1). The reference list of previous systematic reviews in the topic was checked to find potential studies that could also be used in this review. There was no restriction regarding language of publication.
Supplemental material
Only randomised controlled trials investigating the efficacy of exercise-based programmes compared with a control group for preventing non-contact musculoskeletal injuries in football players were included. An exercise-based prevention programme was defined as any exercise therapy that was performed in order to develop or improve function, skills or physical fitness. Control group was defined as usual training/warm-up, minimal intervention, education or not exposed to the intervention. Non-contact musculoskeletal injuries were the primary outcome in this review and was defined as any acute sudden onset musculoskeletal injury that occurred without physical contact by another player or object on the field.33 Studies were eligible if they (1) included football players aged 13 years or older, (2) used exercise-based programmes as intervention, (3) presented number of non-contact injuries and exposure hours for each group, and (4) had a control group. All types of exercise-based prevention programmes were eligible for inclusion. Studies reporting overall injuries were included if it was possible to extract the data specific to non-contact injuries. When information about the injuries was unclear, we contacted the authors via email to confirm or clarify the number of non-contact injuries. A total of three attempts to contact the authors were made. If missing or unclear data could not be provided by the authors of included studies, they were excluded.
Study selection and data extraction
Two independent reviewers (VNL and BABR) applied the inclusion criteria and screened all titles and abstracts. Full texts were evaluated for potential inclusion and disagreements were resolved by consensus. If consensus was not reached, a third reviewer (RZP) was consulted.
Two independent reviewers (VNL and IRL) performed the data extraction of included studies using a standardised data extraction form. In case of disagreement, a third reviewer (RZP) arbitrated the decision. We extracted the following information from each eligible study: country, participants’ characteristics (ie, age, sex and skill level), sample size (total and per group), characteristics of the intervention (focused or general exercises), number of non-contact injuries and exposure hours for each group, and study length. Interventions were categorised as general when the exercises targeted many body segments and joints, with no priority to train or protect a specific muscle group or joint. Focused interventions were defined as a set of exercises chosen to train and protect a specific muscle or joint. When exposure information was reported as ‘athletic exposure’ (ie, one athlete participating in one training or game), we converted the data using the assumption that one athletic exposure was equivalent to 2 hours of exposure.28
Quality assessment
The PEDro scale was used to assess the risk of bias of the included clinical trials.34 35 All studies included in this review were listed in the PEDro database36; therefore, these assessments were adopted.35 Given the nature of the intervention assessed in this review, we adapted the scale and did not consider the items participant and therapist blinding, as it is not possible to blind participant and therapists in trials testing efficacy of exercise prevention programmes. Risk of bias of trials were confirmed by a reviewer (RZP) with 5 years of experience in rating trials using the PEDro scale.
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was used to assess the overall quality of the evidence.37 38 The GRADE tool is a systematic and explicit approach that allows judgements to be made about strength of evidence resulting from systematic reviews. Briefly, the GRADE classification was initially regarded as ‘high’ but downgraded by one level for each of the following domains we considered: (1) risk of bias (downgraded by one level when more than 25% of participants included in the meta-analysis were from studies with ‘high risk of bias’ (ie, when the study did not meet one or more of the following items: random allocation, allocation concealment, assessor blinding, complete outcome follow-up data and intention-to-treat analysis)); (2) inconsistency (downgraded by one level considering: the proportion of the observed variance may be substantial (I2>50%), visual inspection for minimal or no overlap of CIs, and χ2 test (p value <0.05); (3) indirectness (downgraded by one level if meta-analysis included participants with heterogeneous characteristics with regard to sex, age and level of sport (eg, men, women, youth, adults, amateur, professionals)); (4) imprecision (downgraded by one level when the clinical course of action differed considering the upper and lower CI as the true estimate, or the difference between upper and lower CI around the pooled estimate of the injury risk ratio (IRR) was >0.5)28; and (5) publication bias (assessed funnel plot asymmetry by visual inspection and quantified using the Egger test (p value <0.1), if there were at least 10 studies in the meta-analysis).
The following categories were used to define the quality of evidence: high quality (ie, further research is unlikely to change our confidence in the estimate); moderate quality (ie, further research is likely to have an important impact on our confidence in the estimate and might change the estimate); low quality (ie, further research is likely to have an important impact on our confidence in the estimate and is likely to change the estimate); and very low quality (ie, we are uncertain about the estimate).37 38
Statistical analysis
Number of non-contact injuries and exposure hours were used to calculate the injury incidence rate per 1000 hours and the IRR. The inverse variance random-effect model was used to compute the pooled IRR and 95% CIs. As previously planned in our protocol, the available evidence allowed us to perform a subgroup analysis stratifying by intervention specificity (general vs focused exercises). Given that focused interventions targeted the hamstring muscles, subgroup analysis was restricted to non-contact hamstring injury. Heterogeneity between studies (ie, how much the effect size varies across studies) was estimated based on the proportion of the variation in point estimates due to between-study differences (I2). Number needed to treat (NNT) analysis was performed by a mathematical formula.39 Meta-analyses were calculated using RevMan software, V.5.3.
Deviation from protocol
Post hoc sensitivity analyses were performed to investigate the effect of exercise-based programmes in the prevention of non-contact musculoskeletal injuries when (1) including only male or female participants, and (2) including only youth or adult participants. In addition, we decided to replace the terms unimodal and multimodal exercise programmes described in the registered protocol with the terms focused and general exercise programmes. Although the most appropriate terms to refer to these types of exercises may be open to question, the terms focused and general exercise programmes were considered more suitable for this review.
Results
Included studies
The search strategy identified 7512 studies. After removal of duplicates, 4366 studies remained. Title and abstract screening identified 53 potentially eligible studies, and 10 original randomised controlled trials met the criteria to be included in this review (figure 1). In this review, a total of three studies were excluded due to lack of clear information.
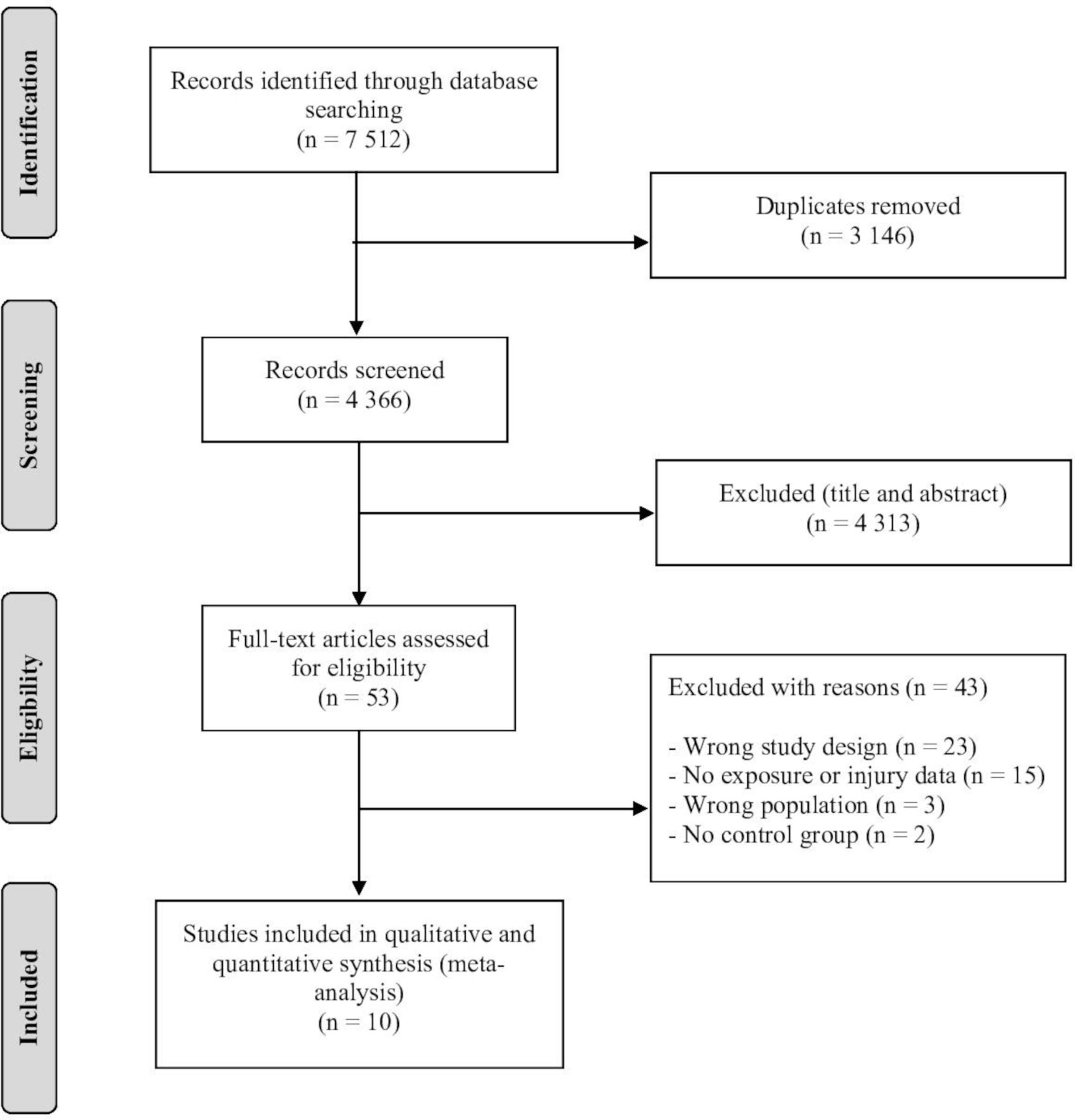
Flow chart of the included studies.
The included studies were conducted in the USA,33 40 Norway,23 41 the Netherlands,24 42 Germany,43 Japan,44 Nigeria45 and Sweden.46 Six studies included only male football players24 40 42–45 and four included only female football players,23 33 41 46 and the total sample sizes for intervention and control groups were 6900 and 6455, respectively. One study used veteran players,43 two used adult players24 42 and seven used youth players (eg, high school or collegiate).23 33 40 41 44–46 All studies included amateur players. Three studies used a focused exercise programme,24 42 44 while seven used a general intervention.23 33 40 41 43 45 46 The intervention period ranged from 12 weeks to 9 months (table 1).
Characteristics of the included studies
Three ongoing trials were identified in clinical registries: one from Sweden and two from Saudi Arabia. The status for all registered trials is ‘Not yet recruiting’ (online supplemental table 2).
Study characteristics
Four studies used the FIFA 11+ warm up and strengthening programme,23 40 43 45 two studies used the Nordic Hamstring Exercise,24 44 one study used the FIFA 11 programme,41 one study used the Prevention Injury and Enhance Performance programme,33 one study used the Bounding Exercise Programme42 and one study used a neuromuscular training programme (Knäkontroll).46 Focused prevention programmes consisted of exercises for the quadriceps or hamstring muscles, while general programmes involved agility, balance, mobility, plyometrics, running and strength exercises for the lower limb. All interventions were applied at least twice a week to every training session. A total of 545 non-contact injuries and 1 062 711 hours of exposure were computed.
Outcomes of the included studies were overall injuries,41 43 45 overall lower limb injuries,23 overall hamstring injuries,24 42 44 overall knee injuries,46 overall ACL injuries40 and non-contact ACL injuries.33 Regarding comparators, control groups were instructed to perform their usual warm-up exercises23 33 41 and/or training routines.24 42 43 45 46 Two studies did not provide information on control groups.40 44
Quality assessment
Overall risk of bias of individual included studies is shown in online supplemental table 3. All studies had random allocation, 30% had concealed allocation, 40% blinded the assessors, 50% had complete outcome follow-up data and 70% had intention-to-treat analysis. Due to the nature of the interventions, none of the included studies were blinded for participants and therapists.
Effect of exercise-based prevention programmes on non-contact musculoskeletal injuries
The results of meta-analysis pooling data from 10 trials showed very low-quality evidence (ie, downgraded one level due to risk of bias, one level due to indirectness and one level due to publication bias (online supplemental figure 1) that exercise-based prevention programmes reduce, on average, the risk of non-contact musculoskeletal injuries by 23% (IRR 0.77; 95% CI 0.61 to 0.97; n=13 355; I2=30%) compared with the control group (figure 2A).
Supplemental material

{kind=link}
{kind=link}
Meta-analysis investigating the effect of exercise-based prevention programmes compared with a control group in reducing (A) overall non-contact injuries and (B) non-contact hamstring injuries in football players. The size of the blue boxes is proportional to the weight of each study in the analysis.
There is low-quality evidence (ie, downgraded one level due to risk of bias and one level due to imprecision) that focused programmes reduce the risk of non-contact hamstring injuries by 35% (IRR 0.65; 95% CI 0.44 to 0.97; n=1238; I2=0%) compared with the control group. There is very low-quality evidence (ie, downgraded one level due risk of bias, one level due to inconsistency, one level due to indirectness and one level due to imprecision) that general programmes were not more effective than control group (IRR 0.63; 95% CI 0.19 to 2.12; n=2573; I2=51%). Focused programmes were not different from general interventions for the prevention of non-contact hamstring injuries (p value=0.95) (figure 2B). Detailed information regarding the quality of evidence (GRADE) is shown in table 2. The NNT value was 148 for overall intervention programmes and 31 for focused programmes. The NNT values for men and women were 118 and 181, respectively, for overall intervention programmes.
Summary of findings and quality of evidence (GRADE)
Sensitivity analysis
The pooled effect restricted to studies with male athletes showed an IRR of 0.68 ((95% CI 0.48 to 0.96); n=3444; I2=20%) favouring exercise-based prevention programmes over control, while for studies with female athletes the IRR was 0.85 ((95% CI 0.63 to 1.16); n=9911; I2=38%) (online supplemental figure 2). The IRR for studies with youth and adult participants were 0.75 ((95% CI 0.54 to 1.02); n=12 111; I2=36%) and 0.77 ((95% CI 0.51 to 1.16); n=1244; I2=39%), respectively (online supplemental figure 3).
Incidence of non-contact injuries
The incidence rate of non-contact injuries in this review (for control groups only) was 0.54 (95% CI 0.47 to 0.60) per 1000 hours of exposure (table 3). When considering studies with overall non-contact injuries as outcome,41 43 45 the injury incidence rate was 0.96 (95% CI 0.79 to 1.13) per 1000 hours of exposure. The average incidence rate of non-contact injuries for male (age range 16.3–43.1 years)24 40 42–45 and female (age range 14.1–19.9)23 33 41 46 participants were 0.57 (95% CI 0.46 to 0.68) and 0.52 (95% CI 0.44 to 0.59) per 1000 hours of exposure, respectively. Among youth and adult participants, the incidence rates were 0.43 (95% CI 0.37 to 0.49) and 1.49 (95% CI 1.16 to 1.82) per 1000 hours of exposure, respectively. The average incidence rates of non-contact injuries to the hamstring23 24 42–45 and ACL40 41 were 0.41 (95% CI 0.32 to 0.50) and 0.87 (95% CI 0.70 to 1.05) per 1000 hours of exposure, respectively. Detailed information is shown in table 3.
Injury and exposure data of the included studies
Discussion
Statement of principal findings
This systematic review shows that exercise-based prevention programmes may be effective in reducing the risk of non-contact musculoskeletal injuries by 23% (95% CI 3% to 39%) among football players when compared with a control group. This result is based on very low-quality evidence and more high-quality studies in this area are needed to clarify the role of exercise-based programmes in preventing non-contact musculoskeletal injuries. Hamstring-focused programmes did not reduce hamstring injury any more than general programmes. The incidence rate of overall non-contact injuries, for control groups only, was 0.96 per 1000 hours of exposure.
Strengths and limitations of the review and the available evidence
The strengths of this systematic review include the use of a prespecified protocol with no language and date restriction criteria, the inclusion of only randomised controlled trials, the assessment of risk of bias and overall quality of the evidence. On the other hand, this review has limitations that should be considered. Although most of the included studies (80%, n=8) used the consensus statement proposed by Fuller et al 47 to define injuries, 60% (n=6) focused on specific type of injuries (hamstring, knee or ACL) and did not report other non-contact injuries. This may have influenced the pooled estimated found in this review. Future studies should investigate and report data for all non-contact injuries to allow estimates to be calculated for overall and specific types of non-contact injuries. We only included lower limb non-contact injuries, and most of participants were women and young amateur athletes, which limits the generalisability of our findings. Nevertheless, the majority of injuries in football affect the lower extremities, and there are more amateur than professional players worldwide (265 million vs 200 000).48 Finally, we used visual inspection and statistical test for asymmetry of funnel plots to assess publication bias. These approaches are prone to error and their results should be interpreted with caution.
A limitation of the available evidence is the high risk of bias (4 of the 10 studies) and small number of studies included in the meta-analysis. Despite the advance in football prevention strategies, there is still a lack of randomised trials investigating non-contact musculoskeletal injuries, especially among high-risk populations (eg, elite youth female players).49 Ninety per cent (n=9) of the included studies did not report non-contact injuries in training and matches separately; therefore, we were not able to report injury incidence separately for training and matches. Finally, our search strategy identified three ongoing trials that might change our current estimates and should be considered for future reviews.
Comparison with previous reviews on injury risk reduction
Our results showed an estimated risk reduction of 23% in the prevention of non-contact musculoskeletal injuries favouring exercise-based programmes over control, but the true effect could vary largely from 3% to 39%. This estimate is lower than a previous systematic review showing a 37% risk reduction for exercise-based programmes on prevention of sport injuries.50 The diversity of interventions, sports and participation level may help to explain the higher heterogeneity (I2=70%; p<0.001) of this previous review in comparison to our results. In football, specifically, there is evidence that exercise-based prevention programmes reduced overall injuries by 22% and 25% among women and recreational/subelite athletes, respectively.22 28 These results combined evidence from overall injuries and different interventions, which might be related to the significant heterogeneity (I2=60.3% and 68.9%).22 28 Our review presents low heterogeneity probably due to inclusion of specific football injuries (ie, non-contact). Our results could be interpreted as promising, but future high-quality studies are needed to determine whether the results are clinically relevant to be applied in the sport settings. For instance, the NNT analysis indicated that at least 148 football athletes are needed to be exposed to intervention to prevent one non-contact musculoskeletal injury, which is considerably higher than previously pooled NNT estimates on non-contact injury (NNT=89).51
Interestingly, our sensitivity results for gender showed that exercise-based prevention programmes were not more effective to prevent non-contact injuries compared with control in female athletes. The four trials included in the sensitivity analysis were conducted with female amateur athletes and three of these trials were considered to be of high risk of bias (ie, no concealed allocation, no assessor blinding, no adequate follow-up, or no intention-to-treat analysis). Our results contrast with a previous review showing that exercise-based prevention programmes reduce overall injuries by 22% in female football players.28 In addition, there is evidence that a subgroup of female athletes, that is, elite youth female athletes, are at a higher risk of injury.49 More high-quality studies are needed, especially with high-risk subgroups (eg, youth elite female athletes), to strengthen our findings and to provide information on how health and football policy makers can adopt and optimise exercise-based prevention programmes across all ages and skill levels (ie, amateurs vs professionals and youth vs adult players).
The pooled effect calculated in the sensitivity analyses showed considerable overlap of 95% CI, which means that the available studies do not clearly show differences according to sex and age.
General versus focused exercise programmes
Our subgroup analysis did not reveal significant difference between focused and general interventions (substantial overlap between both estimates). Our analysis for the subgroup of focused intervention included three studies focusing on hamstring exercises (ie, Nordic Hamstring Exercise and Bounding Exercise Programme)24 42 44 and showed low-quality evidence that the focused interventions may reduce the risk of non-contact injuries, in this case hamstring injuries, by 35% (95% CI 3% to 56%) when compared with the control group. A previous systematic review has shown that injury prevention programmes that include Nordic Hamstring Exercise decreased the risk of hamstring injuries by 51% when compared with the control group.21 This estimate is higher than the estimate found in our review and might be due to differences in study designs, mechanism of injury and participants. We included only randomised controlled trials, non-contact injuries and both sexes, while previous reviews included both randomised and prospective cohort studies,21 overall injuries (ie, contact and non-contact)21 28 and only women.28 The pooled NNT estimates for focused programmes showed that 31 athletes would need to participate in the intervention to prevent one non-contact hamstring injury, which is slightly higher than previous individual evidence of specific exercise (ie, eccentric training) on hamstring injuries (NNT=13).52
Given that NNT is highly dependent on the incidence of an outcome, and not only on the efficacy of an intervention, the NNT values in this review should be interpreted with caution. Considering that incidence may vary according to type of injury, characteristics of participants and sport, comparisons of NNT should be done between similar outcomes, participants and sports.
Incidence of non-contact injuries in football
The incidence of non-contact injuries in this review (0.54 per 1000 hours) is higher than those observed for overall injuries in amateur players (0.49 per 1000 hours),53 and lower than observed for non-contact (7.4 per 1000 hours)54 and overall (8.1 per 1000 hours)7 injuries in professional football players. None of the studies in this review included professional players, which may explain these differences. We would argue that professionals play at the highest level and, therefore, are more susceptible to injuries than amateur players. The highest incidence in our study was for non-contact ACL injuries (0.87 per 1000 hours), which is lower than previous findings showing an incidence rate of ~1.5 per 1000 hours across a seven-season study with professional players.9 Among a total of 4483 injuries observed, 18% (n=828) were ligament-related injuries (eg, sprain/ligament injury).9 Since the majority of ligament injuries (ie, 64%) occurs in non-contact situations,11 more high-quality randomised trials should be conducted to investigate the efficacy of exercise-based programmes in preventing non-contact ACL injuries among amateur and professional football players. It is important to mention that only 55% of athletes who undergo ACL reconstruction return to competitive pre-injury level,55 which may cause some athletes to not progress on to professional level when suffering an ACL injury at lower levels of competition.
Although this review reported injury incidence for overall non-contact injuries from control group data, many of the included trials reported only a subset of non-contact injuries (eg, hamstring or ACL); thus, the injury incidence rates do not reflect the true rate of overall non-contact injuries. It is possible that non-contact injuries which were actually sustained during the exposure time included in this review were not recorded. Even for overall non-contact injuries, there is an inherent limitation of incidence rates due to differences in reporting systems, injury definition and athletes’ perception.
Implications for clinicians
Given that football is the most popular recreational and amateur sport worldwide and provides important health benefits,56 57 well-documented strategies to reduce injuries among football players, especially amateurs, is of utmost importance to sports and public health. Based on the findings of our review and the available evidence,13 21 54 we recommend that exercise-based programmes should be implemented in amateur football to reduce non-contact musculoskeletal injuries. Although this recommendation is based on very low-quality evidence, we should not diminish the merits of exercise-based programmes in preventing sports injuries. The very low-quality evidence strengthens the need for more high-quality research on this topic. Regarding specificity of exercise-based programmes (ie, general or focused), our findings suggest that there might be a role for focused interventions, such as hamstring-specific exercises (ie, eccentric), when the aim is to prevent non-contact hamstring injuries, which is the most prevalent non-contact injury in football.10 11 Since athletes with history of hamstring injury are 2.7 times more likely to re-injury,58 we would argue that it might be feasible to incorporate hamstring-focused exercises to exercise-based prevention programmes for preventing occurrence and recurrence of this type of injury. Based on the available evidence on the efficacy of general exercises for reducing the risk of overall non-contact musculoskeletal injuries,22 28 our view is that exercise-based prevention programmes with general exercises (eg, eccentric strengthening, plyometrics, running, agility and neuromuscular training) would be more feasible to implement for amateur football players because exercises are often easy to perform and may require less supervision. Interestingly, adherence to general and focused exercises may vary. Previous research has shown that adherence to general exercises is up to 85%,59 while adherence to focused exercise (ie, Nordic Hamstring Exercise) is 69% among amateur football players.60 Clinicians should consider using, in addition to athletes’ preferences for exercises, the top strategies to maximise player adherence to injury prevention programmes: education, trust and communication, and coach attendance at sessions.61
Conclusion
Exercise-based prevention programmes reduce non-contact musculoskeletal injuries by 23% (95% CI 3% to 39%) in amateur football players. Despite this evidence being rated as very low quality and considering the burden that an injury may have on athletes’ health, exercise-based prevention programmes should be implemented in football settings. Given the number of ongoing trials, the estimate of effect found in this review is likely to change once the results of these trials become available. At present, it is still unclear whether focused or general programmes provide greater reduction in overall non-contact musculoskeletal injuries. Further research investigating the efficacy of these programmes in amateur and professional settings are warranted to provide a more directive clinical recommendation.
What is already known?
More than 90% of all muscle injuries and 51%–64% of joint/ligament injuries (ie, ACL) in football (soccer) occur in non-contact situations.
Exercise-based prevention programmes reduce the overall injury rate.
There is no systematic review assessing the efficacy of exercise-based programmes in the prevention of non-contact musculoskeletal injuries among football players.
What are the new findings?
Exercise-based prevention programmes reduce, on average, the risk of non-contact musculoskeletal injuries by 23%.
Focused exercise-programmes reduce the risk of non-contact hamstring injuries by 35%.
The injury incidence rate of overall non-contact injuries (for control group only) was 0.96 per 1000 hours of exposure.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge the Coordination for the Improvement of Higher Education Personnel (CAPES) – Finance code 001, and the corresponding authors of included studies for their help in data acquisition. STF and RZP are fellowship recipients from the National Council for Scientific and Technological Development (CNPq).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @itolemes, @Rafael_Z_Pinto, @Evertverhagen, @cs_bolling
Contributors IRL, RZP, VNL, BABR and TRS conceived and designed the study. IRL and VNL conducted the search. IRL, VNL and BABR performed the screening, study selection and data extraction. IRL, RZP, STF and TRS analysed and interpreted the data. IRL, RZP and TRS drafted the manuscript with input from STF, EV, CB and CFA. All authors have read and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.